
Students in Dormitories Were Not Major Drivers of the Pandemic during Winter Term 2020/2021: A Cohort Study with RT-PCR and Antibody Surveillance in a German University City

 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
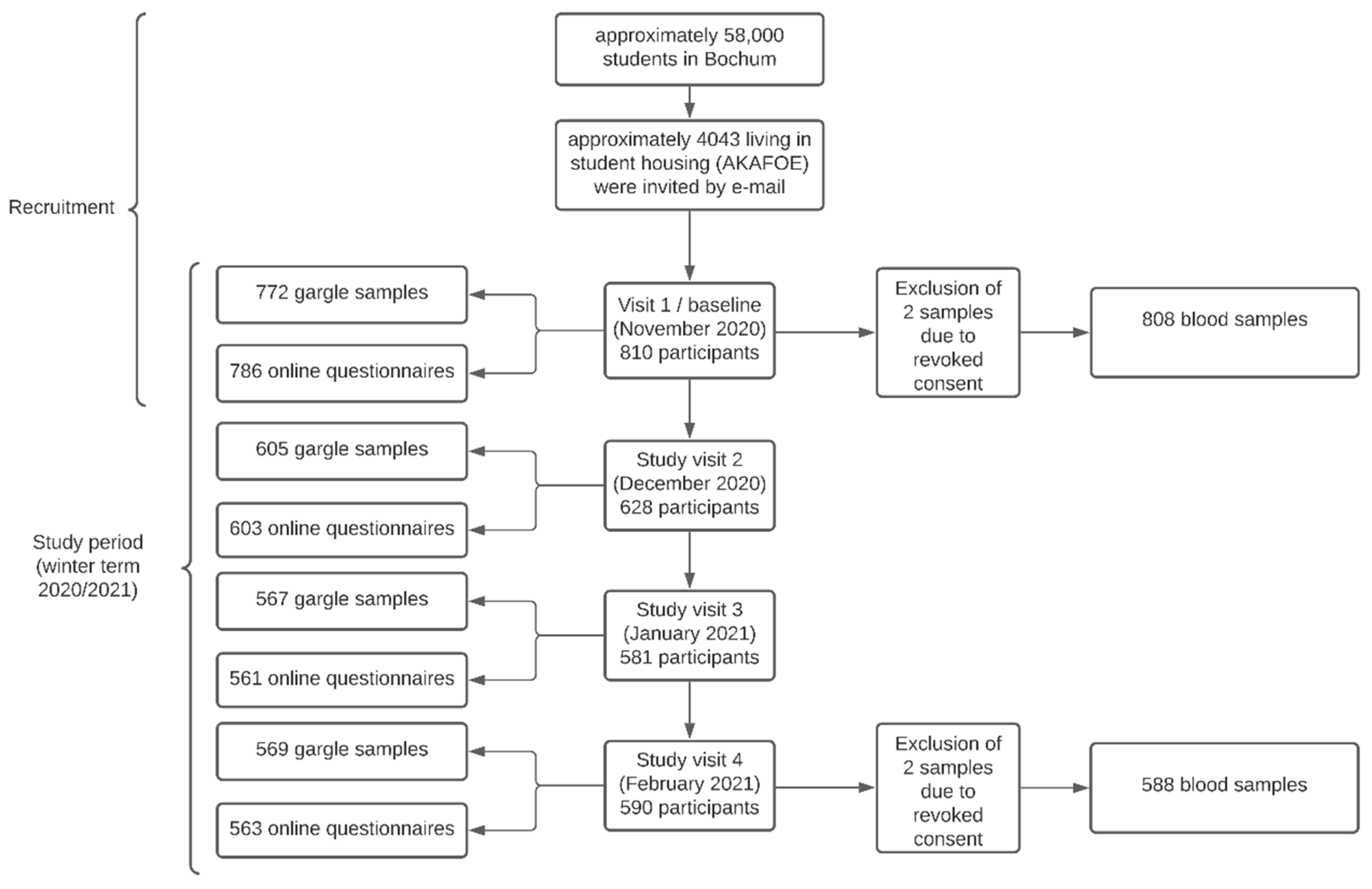
2.1. Study Design
2.2. Detection of Anti-SARS-CoV-2 Antibodies
2.3. SARS-CoV-2 Detection by RT-PCR
2.4. Data Management and Statistical Analysis
3. Results
3.1. Study Population
3.2. Cross-Sectional Prevalence of Infection with SARS-CoV-2 at Baseline
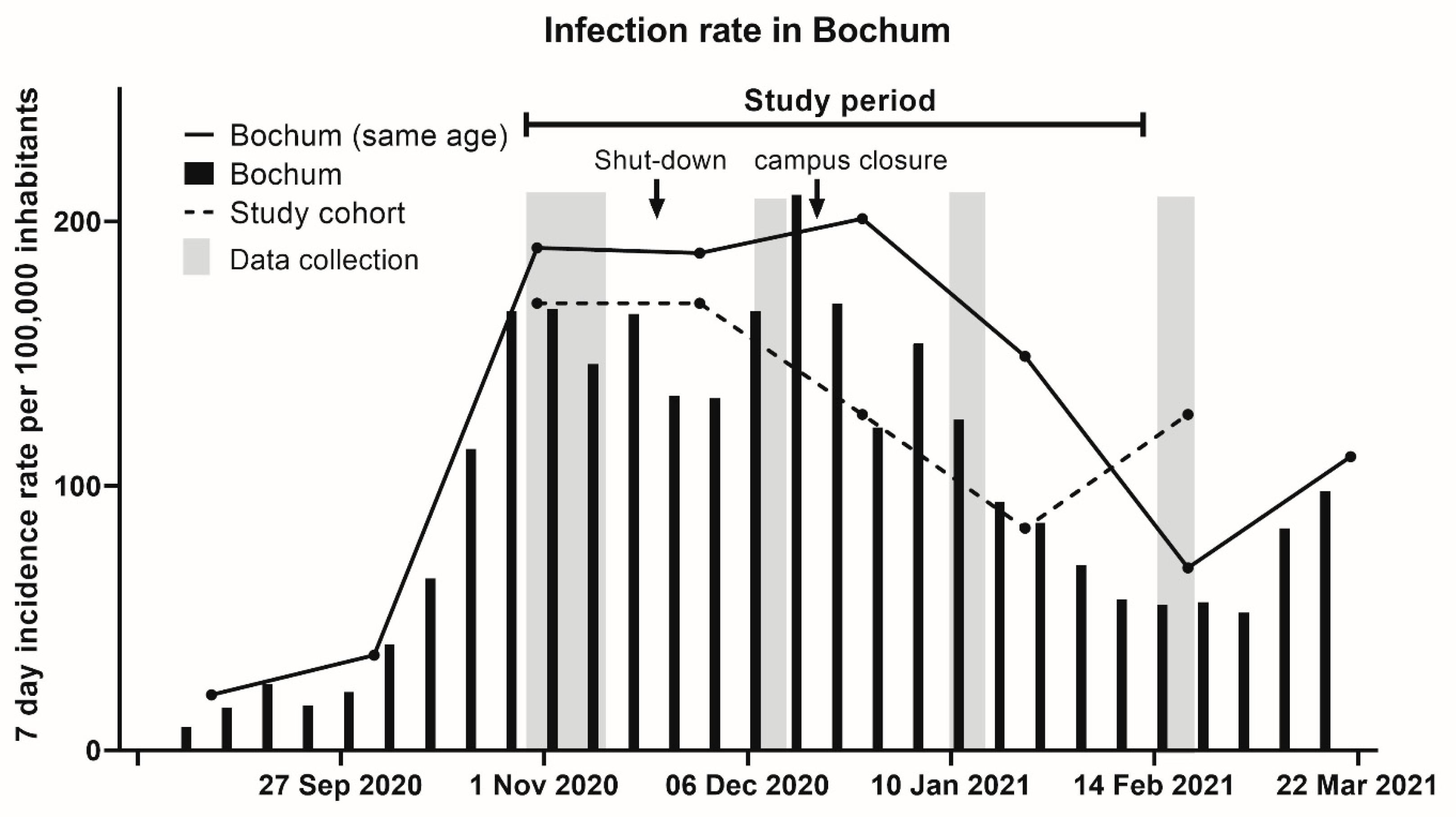
3.3. SARS-CoV-2 Incidence Rates in Bochum, Germany during the Study Period
3.4. Incidence of SARS-CoV-2 Infections within the Study Period
3.5. RT-PCR Results and Gargle Sample as a Surveillance Tool
3.6. Impact of the Housing Situation on Infection Risk and Risk Factor Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef]
- Schilling, J.L.A.; Schumacher, D.; Ullrich, A. al DMe. Krankheitsschwere der ersten COVID-19-Welle in Deutschland basierend auf den Meldungen gemäß Infektionsschutzgesetz. J. Health Monit. 2020, 11, 1–20. [Google Scholar] [CrossRef]
- Böhmer, M.M.; Buchholz, U.; Corman, V.M.; Hoch, M.; Katz, K.; Marosevic, D.V.; Böhm, S.; Woudenberg, T.; Ackermann, N.; Konrad, R.; et al. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: A case series. Lancet Infect. Dis. 2020, 20, 920–928. [Google Scholar] [CrossRef]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dorner, L.; Parker, M.; Bonsall, D.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganyani, T.; Kremer, C.; Chen, D.; Torneri, A.; Faes, C.; Wallinga, J.; Hens, N. Estimating the generation interval for coronavirus disease (COVID-19) based on symptom onset data, March 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Levinson, M.; Cevik, M.; Lipsitch, M. Reopening Primary Schools during the Pandemic. N. Engl. J. Med. 2020, 383, 981–985. [Google Scholar] [CrossRef]
- Hyde, Z. COVID-19, children and schools: Overlooked and at risk. Med. J. Aust. 2020, 213, 444. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMichael, T.M.; Clark, S.; Pogosjans, S.; Kay, M.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; Ferro, J.; Brostrom-Smith, C.; et al. COVID-19 in a Long-Term Care Facility—King County, Washington, February 27–March 9, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 339–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyal, J.W.; Grant, M.P.; Broadwater, K.; Bjork, A.; Waltenburg, M.A.; Gibbins, J.D.; Hale, C.; Silver, M.; Fischer, M.; Steinberg, J.; et al. COVID-19 Among Workers in Meat and Poultry Processing Facilities―19 States, April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef]
- Mosites, E.; Parker, E.M.; Clarke, K.E.N.; Gaeta, J.M.; Baggett, T.P.; Imbert, E.; Sankaran, M.; Scarborough, A.; Huster, K.; Hanson, M.; et al. Assessment of SARS-CoV-2 Infection Prevalence in Homeless Shelters—Four, U.S. Cities, March 27–April 15, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 521–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A Review of Viral, Host, and Environmental Factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; Sultana, M.S.; Hossain, S.; Hasan, M.T.; Ahmed, H.U.; Sikder, M.T. The impact of COVID-19 pandemic on mental health & wellbeing among home-quarantined Bangladeshi students: A cross-sectional pilot study. J. Affect. Disord. 2020, 277, 121–128. [Google Scholar] [CrossRef]
- Radu, M.C.; Schnakovszky, C.; Herghelegiu, E.; Ciubotariu, V.A.; Cristea, I. The Impact of the COVID-19 Pandemic on the Quality of Educational Process: A Student Survey. Int. J. Environ. Res. Public Health 2020, 17, 7770. [Google Scholar] [CrossRef] [PubMed]
- WHO. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection Using Rapid Immunoassays: Interim Guidance; 11 September 2020 (Geneva: World Health Organization). Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 2 May 2021).
- WHO. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases: Interim Guidance; WHO Headquarters, WHO Worldwide: 19 March 2020. Available online: https://www.who.int/publications/i/item/10665-331501 (accessed on 2 May 2021).
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, S.; Davidson, R.S.; Gunson, R.N. Comparison of gargle samples and throat swab samples for the detection of respiratory pathogens. J. Virol. Methods 2017, 248, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Adachi, E.; Yamayoshi, S.; Koga, M.; Iwatsuki-Horimoto, K.; Kawaoka, Y.; Yotsuyanagi, H. Gargle Lavage as a Safe and Sensitive Alternative to Swab Samples to Diagnose COVID-19: A Case Report in Japan. Clin. Infect. Dis. 2020, 71, 893–894. [Google Scholar] [CrossRef] [Green Version]
- Malecki, M.; Lusebrink, J.; Teves, S.; Wendel, A.F. Pharynx gargle samples are suitable for SARS-CoV-2 diagnostic use and save personal protective equipment and swabs. Infect. Control Hosp. Epidemiol. 2020, 1–2. [Google Scholar] [CrossRef]
- Mittal, A.; Gupta, A.; Kumar, S.; Surjit, M.; Singh, B.; Soneja, M.; Soni, K.D.; Khan, A.R.; Singh, K.; Naik, S.; et al. Gargle lavage as a viable alternative to swab for detection of SARS-CoV-2. Indian J. Med. Res. 2020, 152, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.-L.; Jiang, Q.; Ye, F.; Li, S.-Q.; Hong, C.; Chen, L.-Y.; Li, S.-Y. Effect of Throat Washings on Detection of 2019 Novel Coronavirus. Clin. Infect. Dis. 2020, 71, 1980–1981. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Krause, R.; Lamprecht, B.; Berghold, A.; Hanson, B.; Stelzl, E.; Stoiber, H.; Zuber, J.; Heinen, R.; Köhler, A.; et al. Prevalence of RT-qPCR-detected SARS-CoV-2 infection at schools: First results from the Austrian School-SARS-CoV-2 prospective cohort study. Lancet Reg. Health Eur. 2021, 5, 100086. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Zimmer, G.; Agoritsas, T.; Stirnemann, J.; Spechbach, H.; et al. Validation of a commercially available SARS-CoV-2 serological Immunoassay. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Public Health England. Guidance: Investigation of Novel SARS-CoV-2 Variants of Concern. Technical Breefing Document on Novel SARS-CoV-2 Variant. Available online: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201 (accessed on 21 December 2020).
- Walker, A.; Houwaart, T.; Wienemann, T.; Vasconcelos, M.K.; Strelow, D.; Senff, T.; Hülse, L.; Adams, O.; Andree, M.; Hauka, S.; et al. Genetic structure of SARS-CoV-2 reflects clonal superspreading and multiple independent introduction events, North-Rhine Westphalia, Germany, February and March 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- 2020. Available online: https://duvatools.bochum.de/asw/asw.exe?aw=/Bevoelkerungspyramide_2020_tbl.ini (accessed on 2 May 2021).
- 2021. Available online: https://survstat.rki.de/Content/Query/Create.aspx (accessed on 2 May 2021).
- Berghoff, H. Studentisches Wohnen 2003 und 2018: Wo Studierende Unterkommen—Gerstern und Heute. 2019. Available online: https://www.che.de/wp-content/uploads/upload/Im_Blickpunkt_Studentisches_Wohnen_2003_und_2018.pdf (accessed on 2 May 2021).
- RKI. Nationale Teststrategie—Wer Wird in Deutschland auf das Vorliegen Einer SARS-CoV-2 Infektion Getestet? 2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Teststrategie/Nat-Teststrat.html (accessed on 2 May 2021).
- RKI. Serologische Untersuchungen von Blutspenden auf Antikörper Gegen SARS-CoV-2 (SeBluCo-Studie). 2021. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/SeBluCo_Zwischenbericht.html (accessed on 2 May 2021).
- Mourad, A.; Turner, N.A.; Baker, A.W.; Okeke, N.L.; Narayanasamy, S.; Rolfe, R.; Engemann, J.J.; Cox, G.M.; Stout, J.E. Social Disadvantage, Politics, and Severe Acute Respiratory Syndrome Coronavirus 2 Trends: A County-level Analysis of United States Data. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Plümper, T.; Neumayer, E. The pandemic predominantly hits poor neighbourhoods? SARS-CoV-2 infections and COVID-19 fatalities in German districts. Eur. J. Public Health 2020, 30, 1176–1180. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | All Participants n = 810 | Attended Final Visit n = 590 |
|---|---|---|
| Personal information | ||
| Age [years] | 23.7 (±3.4) [810] | 23.5 (±3.2) [590] |
| Females | 377 (46.5%) [810] | 283 (48.0%) [590] |
| BMI [kg/m2] | 23.3 (±3.8) [771] | 23.2 (±3.68) [574] |
| Living conditions | ||
| Single apartment | 299 (39.4%) [779] | 198 (34.6%) [572] |
| Shared apartment | 480 (61.6%) [779] | 374 (65.3%) [572] |
| No. of roommates, | 3.2 (±2.2) [478] | 3.0 (±1.9) [372] |
| mean (SD) (n = 478) | min. 0, max. 14 | min. 0, max. 14 |
| Health information | ||
| Nicotine consumption | 113 (14.7%) [767] | 73 (12.9%) [565] |
| Alcohol consumption | 369 (48.1%) [767] | 297 (52.7%) [564] |
| Chronic disease | 112 (14.3%) [782] | 82 (14.3%) [573] |
| Bronchial asthma | 36 | 30 |
| Metabolic disease | 23 | 16 |
| Psychiatric | 17 | 12 |
| Regular medication | 213 (27.4%) [778] | 165 (28.8%) [574] |
| Contraceptives | 126 | 103 |
| Thyroid drugs | 31 | 24 |
| Antidepressants | 20 | 13 |
| Analgesics | 17 | 12 |
| Regular sports activities | 500 (64.5%) [775] | 378 (66.3%) [570] |
| Country of birth | ||
| Germany | 572 (73.1%) [783] | 456 (79.0%) [577] |
| Iran | 37 (4.7%) [783] | 17 (3.0%) [577] |
| Russia | 30 (3.8%) [783] | 21 (3.6%) [577] |
| Italy | 12 (1.5%) [783] | 8 (1.4%) [577] |
| Other | 132 (16.9%) [783] | 75 (13.0%) [577] |
| Have You Ever Been Tested Positive for SARS-CoV-2 Infection? | Anti-SARS-CoV-2 Antibody Status | |
|---|---|---|
| Positive | Negative | |
| Total number | 23 | 785 |
| Yes | 7 (30.4%) | 2 † (0.25%) |
| No | 15 (65.2%) | 760 (96.7%) |
| No answer | 1 (4.3%) | 23 (30.5%) |
| Ratio reported to unreported case ‡ | 1:2 | |
| No. of Samples | Positive Results | Negative Results | |
|---|---|---|---|
| Baseline/visit 1 (November 2020) | |||
| Participants | 810 | ||
| Collected gargle samples | 772 (95.3%) | ||
| Valid † RT-PCR results | 727 (89.8%) | 6 (0.8%) | 721 (99.2%) |
| Anti-SARS-CoV-2 IgG/IgM | 808 (99.8%) | 23 (2.9%) | 785 (97.2%) |
| Visit 2 (December 2020) | |||
| Participants | 628 | ||
| Collected gargle samples | 605 (96.3%) | ||
| Valid † RT-PCR results | 513 (81.7%) | 7 (1.4%) | 506 (98.6%) |
| Visit 3 (January 2021) | |||
| Participants | 581 | ||
| Collected gargle samples | 567 (97.6%) | ||
| Valid † RT-PCR results | 497 (85.5%) | 3 (0.6%) | 494 (99.4%) |
| Visit 4 (February 2021) | |||
| Participants | 590 | ||
| Collected gargle samples | 569 (96.4%) | ||
| Valid † RT-PCR results | 546 (92.5%) | 3 (0.6%) | 543 (99.5%) |
| Anti-SARS-CoV-2 IgG/IgM | 588 (99.7%) | 29 (4.9%) | 559 (95.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres Reyes, C.R.; Steinmann, E.; Timmesfeld, N.; Trampisch, H.-J.; Stein, J.; Schütte, C.; Skrygan, M.; Meyer, T.; Sakinc-Güler, T.; Schlottmann, R.; et al. Students in Dormitories Were Not Major Drivers of the Pandemic during Winter Term 2020/2021: A Cohort Study with RT-PCR and Antibody Surveillance in a German University City. COVID 2021, 1, 345-356. https://doi.org/10.3390/covid1010029
Torres Reyes CR, Steinmann E, Timmesfeld N, Trampisch H-J, Stein J, Schütte C, Skrygan M, Meyer T, Sakinc-Güler T, Schlottmann R, et al. Students in Dormitories Were Not Major Drivers of the Pandemic during Winter Term 2020/2021: A Cohort Study with RT-PCR and Antibody Surveillance in a German University City. COVID. 2021; 1(1):345-356. https://doi.org/10.3390/covid1010029
Chicago/Turabian StyleTorres Reyes, Christian Rafael, Eike Steinmann, Nina Timmesfeld, Hans-Joachim Trampisch, Julien Stein, Christian Schütte, Marina Skrygan, Thomas Meyer, Türkan Sakinc-Güler, Renate Schlottmann, and et al. 2021. "Students in Dormitories Were Not Major Drivers of the Pandemic during Winter Term 2020/2021: A Cohort Study with RT-PCR and Antibody Surveillance in a German University City" COVID 1, no. 1: 345-356. https://doi.org/10.3390/covid1010029