
Coronavirus Infections; Coinfection; Measles; Vaccines
Infecções por Coronavirus; Coinfecção; Sarampo; Vacinas
Healthcare workers (HCW) are at high risk of contracting the Coronavirus disease 2019 (COVID-19), even with the use of personal protective equipment, due to the greater exposure, work intensity, lack of rest, inadequate training, and while undressing11. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100-1. . In China, at least 3,387 HCW were infected, with 22 deaths11. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100-1. . Sadly, numbers are still growing, but by March 2020, Italy had reported the infection of over 2,600 HCW and, in April, the United States estimated more than 9,200 infected HCW.
Currently, there are no vaccines or specific antiviral drugs for COVID-19. Its frequent mutations facilitate fast transmissibility and difficult the designing of a vaccine22. Yin C. Genotyping coronavirus SARS-CoV-2: methods and implications. Genomics. 2020;S0888-7543(20)30318-9. . Vaccination exposes the body to antigens and activates the immune system without causing disease. However, even in a highly vaccinated population, outbreaks may still happen. In this letter, we describe a case of co-infection with SARS-CoV-2 and Measles morbillivirus in a front-line health worker in Brasil. The case report was approved by the Ethics Research Committee on March 15, 2020, under the number 012342020. The patient signed an informed consent form.
CASE
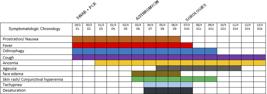
A 25-year-old male caucasian physician with mild asthma history and not in use of any medication, fighting in the front-line against COVID-19, presented prostration, sleeping difficulty, and fever (37.8ºC), for which he took antipyretics and analgesics. On the following two days, he evolved with odynophagia, dysphagia, worsening of prostration, productive cough, and anosmia. On the 3rd day, the patient reported dry cough and rhinorrhea. A nasopharyngeal swab was used and sent for RT-PCR COVID-19 testing. On the 5th day, new symptoms were added ( table 1 ): tachydyspnea, conjunctival hyperemia, morbilliform erythematous maculopapular non-itching rash on his face, trunk, limbs, and on the palms of both hands. ( figure 1 ). A physical exam also revealed palpable lymph nodes in the bilateral occipital and spinal accessory chains and clustered white lesions on the buccal mucosa (Koplik’s sign). Azithromycin 500mg, prednisone 20mg, antiemetic, antiallergic, and analgesic drugs were prescribed. On the next day, the patient presented desaturation and needed supplementary oxygen. Three days later, the patient had no rashes. The last symptoms to disappear were cough and anosmia (table).

RT-PCR were positive for COVID-19 and Measles morbilivirus. Serologies for measles were also positive [IgG: 3687 mUI / mL (positive reference value> 200 mUI / mL); IgM: 524 U / mL (positive reference value> 15 U / mL). The patient reported vaccination with three doses of MMR vaccine during childhood.
DISCUSSION
Measles is a highly contagious disease and still a common threat in the underdeveloped world33. Dabbagh A, Laws RL, Steulet C, Dumolard L, Mulders MN, Kretsinger K, et al. Progress toward regional measles elimination - worldwide, 2000-2017. MMWR Morb Mortal Wkly Rep. 2018;67(47):1323-9. . Live attenuated measles vaccine is considered to have high protective efficacy, especially after two doses (94% efficacy)44. Uzicanin A, Zimmerman L. Field effectiveness of live attenuated measles-containing vaccines: a review of published literature. J Infect Dis. 2011;204(Suppl 1):S133-48. . In countries with high vaccine coverage, as in Brasil, measles outbreaks happen mainly due to importation or vaccination failure55. Goldani LZ. Measles outbreak in Brasil, 2018. Braz J Infect Dis. 2018;22(5):359. . Nevertheless, the infection may happen in vaccinated patients due to suboptimal measles vaccine-induced humoral immunity and/or waning immunity in a low measles-exposure environment66. Haralambieva IH, Kennedy RB, Ovsyannikova IG, Schaid DJ, Poland GA. Current perspectives in aassessing humoral immunity after measles vaccination. Expert Rev Vaccines. 2019;18(1):75-87. .
Coronavirus and Measles morbillivirus have an evolutionary connection, as they share core proteins77. Saad ME, Elsalamony RA. Measles vaccines may provide partial protection against COVID-19. IJCBR. 2020;5(1):14-9. . Measles vaccination may increase the ability of the immune system to fight COVID-1977. Saad ME, Elsalamony RA. Measles vaccines may provide partial protection against COVID-19. IJCBR. 2020;5(1):14-9. . Coinfections may facilitate genetic exchange and generate recombinant viruses, influencing viral evolution, sensitivity to antiviral therapy, and disease course88. Kumar N, Sharma S, Barua S, Tripathi BN, Rouse BT. Virological and immunological outcomes of coinfections. Clin Microbiol Rev. 2018;31(4):e00111-17. , 99. Asner SA, Science ME, Tran D, Smieja M, Merglen A, Mertz D. Clinical disease severity of respiratory viral co-infection versus single viral infection: a systematic review and meta-analysis. PLoS One. 2014;9(6):e99392. .
Our patient presented a relatively benign course of both infections, which may be explained by competitive suppression between the viruses. In this case, similar viruses interfere with the replication of one another or there may have been a competition between the viruses for metabolites, replication sites, or host factors necessary for virus replication88. Kumar N, Sharma S, Barua S, Tripathi BN, Rouse BT. Virological and immunological outcomes of coinfections. Clin Microbiol Rev. 2018;31(4):e00111-17. .
Physicians are trained to think of a single virus causing a clinical syndrome. During the pandemic, it is clear that COVID-19 is going to be the first diagnostic hypothesis for most respiratory syndromes. But we must be aware of the similarities between viruses. Future studies should increase the knowledge about how frequent coinfections happen and how they interfere in the disease course.
REFERENCES
-
1Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100-1.
-
2Yin C. Genotyping coronavirus SARS-CoV-2: methods and implications. Genomics. 2020;S0888-7543(20)30318-9.
-
3Dabbagh A, Laws RL, Steulet C, Dumolard L, Mulders MN, Kretsinger K, et al. Progress toward regional measles elimination - worldwide, 2000-2017. MMWR Morb Mortal Wkly Rep. 2018;67(47):1323-9.
-
4Uzicanin A, Zimmerman L. Field effectiveness of live attenuated measles-containing vaccines: a review of published literature. J Infect Dis. 2011;204(Suppl 1):S133-48.
-
5Goldani LZ. Measles outbreak in Brasil, 2018. Braz J Infect Dis. 2018;22(5):359.
-
6Haralambieva IH, Kennedy RB, Ovsyannikova IG, Schaid DJ, Poland GA. Current perspectives in aassessing humoral immunity after measles vaccination. Expert Rev Vaccines. 2019;18(1):75-87.
-
7Saad ME, Elsalamony RA. Measles vaccines may provide partial protection against COVID-19. IJCBR. 2020;5(1):14-9.
-
8Kumar N, Sharma S, Barua S, Tripathi BN, Rouse BT. Virological and immunological outcomes of coinfections. Clin Microbiol Rev. 2018;31(4):e00111-17.
-
9Asner SA, Science ME, Tran D, Smieja M, Merglen A, Mertz D. Clinical disease severity of respiratory viral co-infection versus single viral infection: a systematic review and meta-analysis. PLoS One. 2014;9(6):e99392.
-
FundingThis work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Publication Dates
-
Publication in this collection
11 Sept 2020 -
Date of issue
Aug 2020
History
-
Received
07 June 2020 -
Accepted
12 June 2020


