 Rebeca R. C. Silva1,2,3†
Rebeca R. C. Silva1,2,3† Rodrigo C. Menezes1,3,4,5†
Rodrigo C. Menezes1,3,4,5† Stefania L. Garcia1,3,6†Hugo N. Pustilnik1,3,6†Isabella B. B. Ferreira1,2,3,4Kaique V. C. S. Aguiar7Nivaldo M. Filgueiras Filho6,7
Stefania L. Garcia1,3,6†Hugo N. Pustilnik1,3,6†Isabella B. B. Ferreira1,2,3,4Kaique V. C. S. Aguiar7Nivaldo M. Filgueiras Filho6,7 Mariana Araújo-Pereira1,3,4,5‡
Mariana Araújo-Pereira1,3,4,5‡ Bruno B. Andrade1,2,3,4,5,6*‡
Bruno B. Andrade1,2,3,4,5,6*‡- 1Multinational Organization Network Sponsoring Translational and Epidemiological Research (MONSTER) Initiative, Salvador, Brazil
- 2Escola Bahiana de Medicina e Saúde Pública (EBMSP), Salvador, Brazil
- 3Instituto de Pesquisa Translacional e Clínica (IPCT), Faculdade de Tecnologia e Ciências, Salvador, Brazil
- 4Laboratório de Inflamação e Biomarcadores, Instituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil
- 5Faculdade de Medicina, Universidade Federal da Bahia (UFBA), Salvador, Brazil
- 6Curso de Medicina, Universidade Salvador (UNIFACS), Salvador, Brazil
- 7Unidade de Terapia Intensiva, Hospital EMEC, Feira de Santana, Brazil
Introduction: The COVID-19 pandemic resulted in tremendous physical and psychological pressure on healthcare professionals, especially on those working in intensive care units (ICUs) and Emergency Departments (EDs). The present study intended to characterize the profile of these professionals which is associated with burnout and determine the potential predictors of such condition.
Methods: A Prospective cohort study was carried out in a tertiary hospital between March 2020 and March 2021, in Salvador, Brazil. A standardized and validated version of the Oldenburg Burnout inventory (OLBI) was applied to assess risk of burnout together with data forms designed to collect information on sociodemographic characteristics and religious beliefs. ICU and ED healthcare professionals were evaluated during off-hours at two distinct periods of the COVID-19 pandemic, in 2020 and in 2021. Differences in the results obtained from each study participant between the timepoints were compared. A binary logistic regression analysis was performed to identify the predictors of burnout development independent of other confounding factors.
Results: Seventy-seven healthcare professionals with a median age of 33 (interquartile range [IQR]: 31–37.5) years and predominantly female (72.7%; n = 56) were enrolled. There were 62 professionals at risk of developing burnout through the OLBI. Those had a median age of 33 (IQR: 31–37) and female predominance (71%, n = 44). Disengagement and burnout were the only features which frequencies significantly changed over time, with increasing detection at the latest timepoint. Alcohol consumption was found to be an important risk factor for burnout development [adjusted odds ratio (aOR): 10.8 (95% CI: 1.8–64.2)]. Importantly, working in the ICU [aOR: 0.04 (95%CI: 0.01–0.32)] and the habit of praying daily [aOR: 0.07 (95%CI: 0.01–0.41)] were characteristics linked to reduced odds of burnout.
Discussion: Disengagement substantially increased during the COVID-19 pandemic in healthcare professionals. Alcohol consumption favors the onset of burnout whereas habit of praying daily and working in the ICU are protective against such outcome. Institutional policies aimed at minimizing etilism may positively impact mental health of these professionals.
1. Introduction
Healthcare professionals who have worked during the COVID-19 pandemic suffered a high level of stress and anxiety, especially those in Intensive Care Units (ICU) and Emergencies (Dos Santos Barros et al., 2016). Studies have shown that these specialists have become a population that is particularly vulnerable to excessive levels of fear, fatigue and irritability due to their social and professional responsibility, in addition to the strenuous workday, due to the outrageous rapid increase in severe COVID-19 cases, overloading the healthcare services (de Oliveira et al., 2020; Di Tella et al., 2020; Dosil et al., 2020; Romero et al., 2020; Rossi et al., 2020; Rumeysa et al., 2020; Arpacioglu et al., 2021; Cipolotti et al., 2021).
Although “staff burn-out” was designated by Freudenberg in the 70’s as an experience of disappointment, physical and emotional exhaustion and loss of interest in work, the discussion about Burnout has substantially expanded over the recent years and robustly intensified during the COVID-19 pandemic. Currently, researchers define this condition as a psychological stress related to work and its main manifestations would be exhaustion and disengagement, but above all, exhaustion (Demerouti et al., 2001; Bakker et al., 2004; Demerouti, 2008; da Silva Schuster and da Veiga Dias, 2018). Previous studies have underscored that, as in other epidemics, the impact on mental health is strongly related to the greater number of individuals affected by the infectious contagion itself (Reardon, 2001; Ornell et al., 2020). Not only, factors such as long working hours, high workloads, lack of resources, and inadequate staffing have been identified as potential stressors, with the responsibilities of health professionals potentially exacerbating this phenomenon (West et al., 2016).
Furthermore, the insecurity, fear and sadness that permeate the scenario observed during the COVID-19 pandemic have revealed a chain of concepts related to sustaining what is in fact essential to life. Since spirituality has the potential to promote the idea of protection and humanization, by manifesting the character of hope, mastery of resilience and promotion of well-being, some healthcare professionals were able to exercise their belief as a coping strategy (Tavares, 2020). The primary goal of this study was to determine which characteristics can predict the development of burnout in healthcare professionals. Additionally, this study sought to measure the relationship of faith as a coping strategy trough a questionnaire of religious beliefs.
2. Methods
2.1. Study design and participants
Prospective, descriptive, and analytical cohort, from June 2020 to March 2021, which included all health professionals from the emergency department and ICU, that provided consent, of a large COVID-19 referral hospital located in the state of Bahia, Brazil. Of 102 health professionals, 77 agreed to participate in this work (Figure 1).
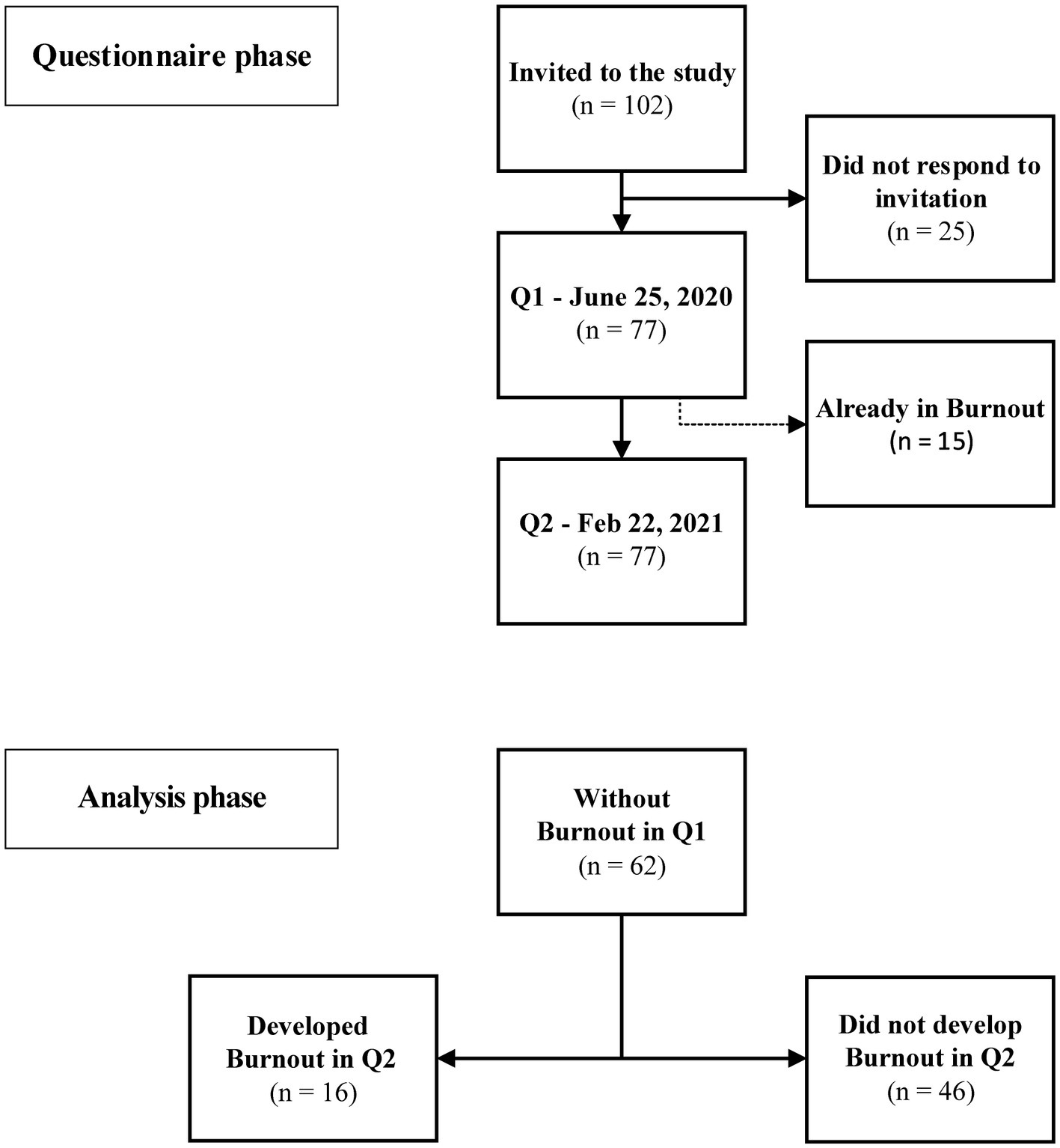
Figure 1. Study flowchart. The questionnaires phase demonstrates the time-points in which they were applied. There was no loss of follow-up between study periods. The analytical phase included only health professionals who did not have burnout in Q1.
2.2. Procedures
A self-administered online data questionnaire was applied at two different timepoints of the COVID-19 pandemic during commencement of off-work hours, first on June 25, 2020 (Q1), then on February 22, 2021 (Q2) (Figure 1). The first application of the questionnaire intends to identify those who are already in burnout and, therefore, are not able to develop Burnout developing the syndrome in Q2, in addition to discerning the baseline characteristics of the studied population. The second application aims to assess changes in baseline characteristics and to identify those who developed the syndrome during the study period. The information acquired in Q1 was used in a logistic model to predict the development of burnout in Q2.
Both questionnaires contained three sections: the first obtained socio-demographic data (age, gender, ethnicity, weight, occupation, financial satisfaction, chronic illnesses, physical activity, drug consumption, dissatisfaction with eating habits, psychological support and isolation due to COVID-19); the second section contained the questions that made up OLBI; the third section contained the questions that made up Beliefs. Details of these last two are described below. A copy of the questionnaire translated to English is shown in Supplementary File S1.
2.2.1. Oldenburg burnout inventory
A validated Portuguese translation of the standardized OLBI was used to assess burnout risk (da Silva Schuster and da Veiga Dias, 2018). It consists in a self-report four-point Likert scale with eight questions for each dimension: disengagement and exhaustion (Demerouti et al., 2001). In such questionnaire, disengagement refers to distancing from work in terms of both object and content, and the development of cynical and negative attitudes (Bakker et al., 2004). Exhaustion is the feeling of physical fatigue, the need to rest, and feelings of overtaxing and emptiness in relation to work (Demerouti, 2008). As used in recent studies, mean scores ≥ 2.25 in exhaustion were considered as high exhaustion, whereas scores ≥ 2.1 on disengagement were considered as high disengagement. The presence of the two high scores indicated Burnout.
2.2.2. Beliefs
Furthermore, the long form of the standardized Beliefs questionnaire was also applied. This questionnaire was published in a report of the Fetzer Institute and the National Institute on Aging Working Group in a compilation of multidimensional measurement tools of religiousness and spirituality for use in health research. It consists in a self-report, not validated, five-point rating scale with seven questions that assess the degree of an individual’s beliefs. Its sum was used to estimate the degree of personal faith. The cognitive dimension of belief is central to religiosity and, despite differences from religion to religion, there is in all of them a search for the meaning of suffering and death, bringing comfort and serving as a coping mechanism (Fetzer Institute, and National Institute on Aging Working Group, 1999).
2.3. Statistical analysis
Median values with interquartile ranges (IQR) were used as measures of central tendency and dispersion, respectively. The Mann–Whitney U test (for two unmatched groups) and the Wilcoxon matched pair test (for two matched groups) were used to compare continuous variables. The categorical variables were compared using the Fischer’s exact test (in 2 × 2 tables) and were presented as number and frequency (%). A binary regression analysis, backwards stepwise method, was used to identify factors independently associated with burnout development. All variables that presented value of p < 0.1 in the univariable analysis were included in the final adjusted model. Differences with value of ps < 0.05 were considered statistically significant. Statistical analyzes were performed in R (version 4.1.1).
3. Results
3.1. Characteristics of the study participants at baseline
The median age of the population was 33 (IQR: 31–37) years, there was a predominance of women (72.7%; n = 56) and the most prevalent self-reported skin color was brown (61%; n = 47; Figure 2). There were 16 (20.8%) physicians, 20 (26.0%) nurses, 29 (37.7%) nursing technicians and 12 (15.6%) physiotherapists, 54 of whom worked in the ICU, 14 worked in the emergency department and 8 worked in both sectors. Also, 50 (64.9%) participants reported a monthly income lower than 5 minimum wages, 57 (74%) did less than 2 h of physical activity, 41 (53.2%) considered its nutrition inadequate, and 1 (1.3%) smoked. At baseline, 15 (19.5%) professionals were already in Burnout.
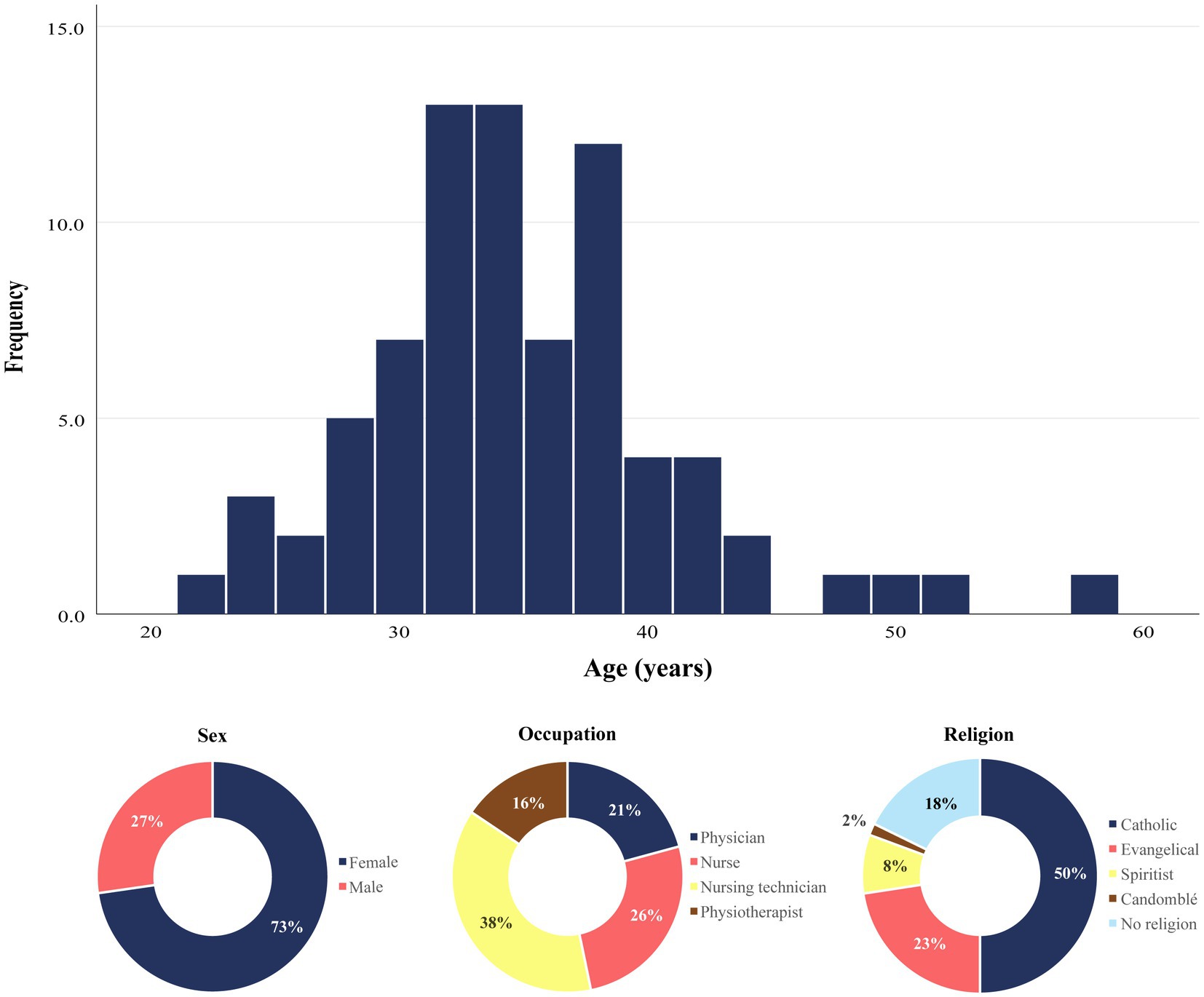
Figure 2. Population Characteristics. Upper panel: histogram depicting age distribution of the study participants at the baseline. Lower panel: Distribution of sex, occupation and religion types among the study participants. Data are frequencies of a total of 77 individuals who enrolled the study.
3.2. Change in population profile over time during the COVID-19 pandemic
The Figure 3 summarizes the changes in the frequency of the characteristics evaluated in this study between the two timepoints. No variation was statistically significant. The most substantial difference was observed in the practice of physical activity, which showed a relative increase of 76.9% (from 26 to 46%, value of p = 0.060). Furthermore, the proportion of exhausted professionals remained similar between the timepoints, the increase in disengaged participants (from 20 to 32%, value of p = 0.097) being responsible for an increase of the same proportion of individuals in burnout. Accordingly, the rate of participants undergoing nutritional and psychological assistance rose slightly, respectively from 13 to 18.2% (value of p = 0.506) and 3.9 to 13% (value of p = 0.079).
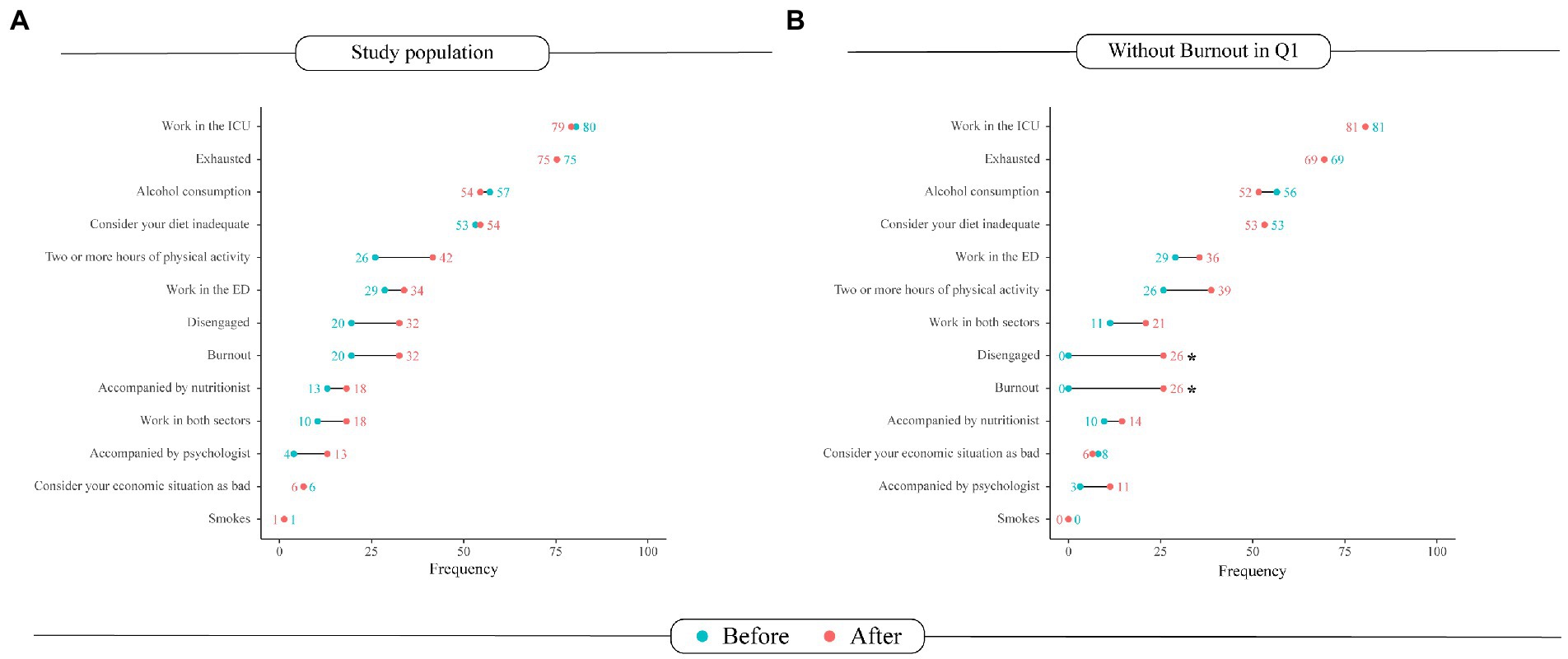
Figure 3. Changes in the Burnout questionnaire in the (A) overall study population and in the (B) participants who have not developed burnout. In blue, the frequencies of the characteristics in the first questionnaire are represented as % of the study participants. In red, frequencies obtained in the second questionnaire. Asterisks indicate statistically significant differences (value of p < 0.05). Intensive Care Unit (ICU), Emergency Department (ED).
3.3. Burnout development assessment
This stage of the analysis included only professionals who, in Q1, had no Burnout (n = 62). Those had a median age of 33 (IQR: 31–37) and a female predominance (71%, n = 44). The only variables that showed a significant change in frequency throughout the study were disengagement and burnout (Figure 3B). Regarding burnout development, there were no significant differences in age, sex, work department and self-reported skin color (Table 1). The logistic regression analysis model revealed two predictors of burnout that were independent of other confounding factors. The predictors were: working in the ICU (adjusted OR: 0.04; 95%CI: 0.01–0.32) and alcohol consumption (adjusted OR: 10.8; 95%CI: 1.8–64.2). Importantly, the habit of praying daily was shown to be a protective feature minimizing the odds of burnout in such adjusted analysis (adjusted OR: 0.07; 95%CI: 0.01–0.41; Figure 4).
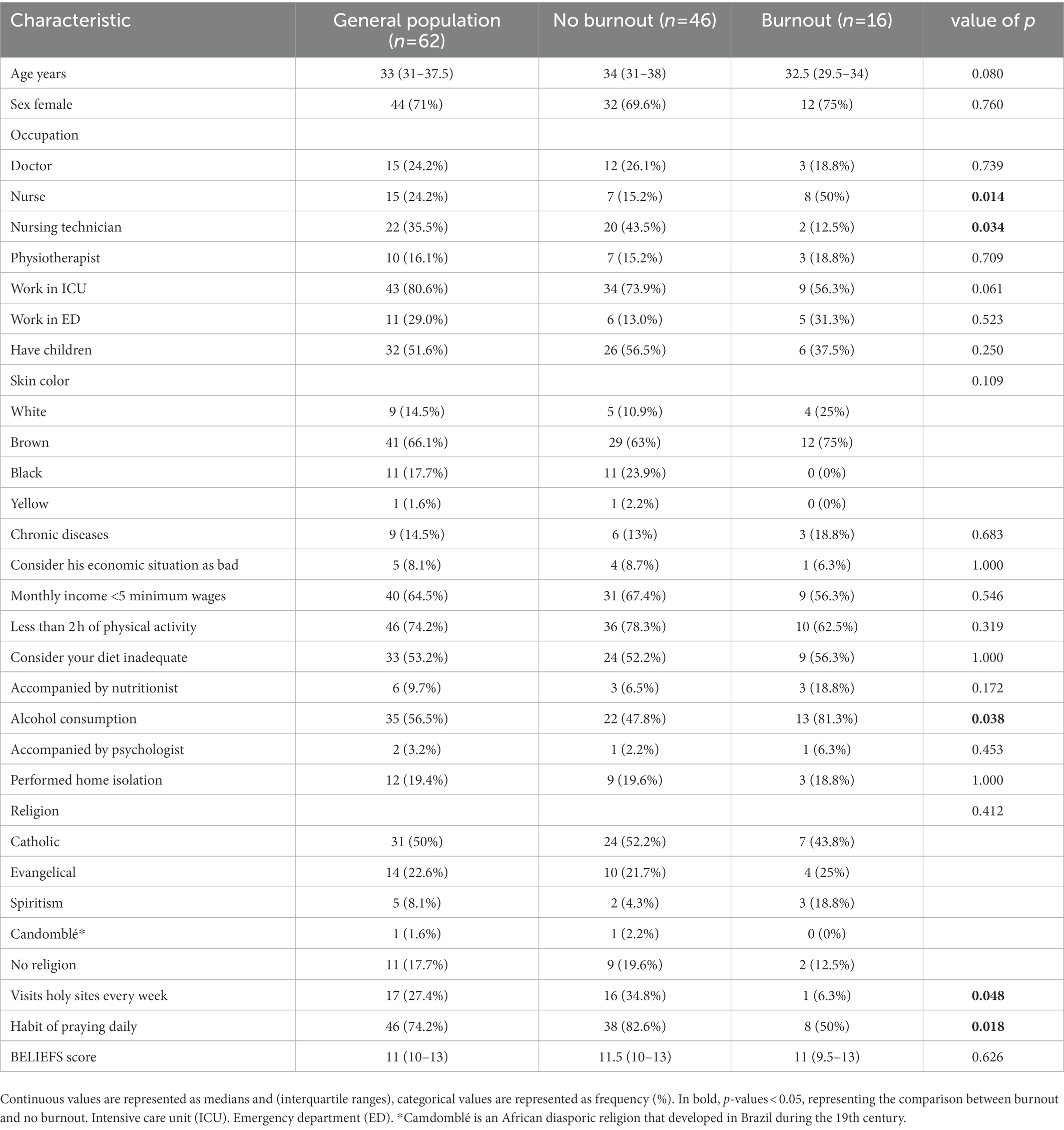
Table 1. Comparison according to the development of burnout.
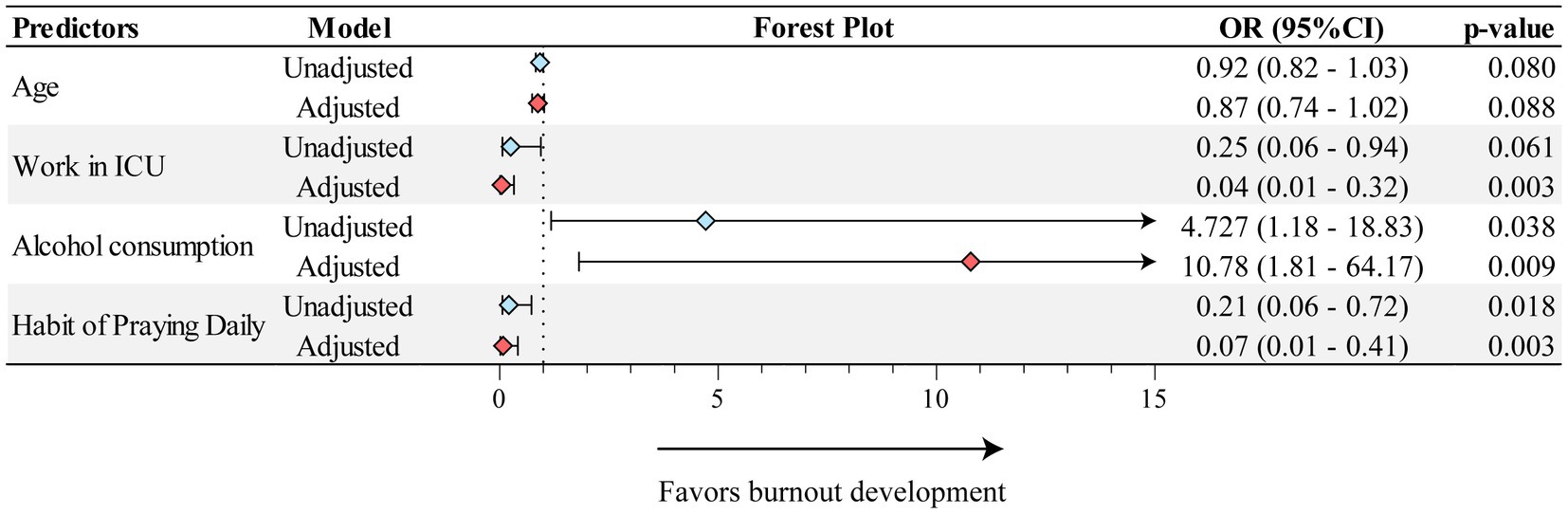
Figure 4. Adjusted and unadjusted binary regression model for Burnout development. The model presents only the variables which passed on the final step of the regression analysis. Multivariable regression was adjusted for differences in values characteristics with statistical relevance (value of p < 0.1). Odds Ratio (OR); Intensive Care Unit (ICU).
4. Discussion
This study evaluated the occurrence of burnout in a population under the prolonged effect of a stressful event, which was the COVID-19 pandemic, and identified the predictors for the development of such syndrome, in a country heavily affected by SARS-CoV-2 plague. The study participants represent the population of healthcare professionals who worked on the frontlines in the fight against the pandemic. One important contribution of this study was the observation that Burnout has no predilection for age, sex, race/skin color and work department (either ED or ICU). However, there appeared to be an association regarding the area of activity, in which nurses and nursing technicians were differentially predisposed to develop burnout, in line with another study carried out with Swedish health professionals, including nurses, midwives and biomedical technicians who developed burnout (Peterson et al., 2008). Of note, these relationships were not sustained after adjustment of other confounding factors in the present study, indicating that additional investigations are required to clarify whether area of activity of healthcare professionals is indeed an independent contributing factor for burnout development in other settings than those depicted here.
Despite the challenges that arose in the daily lives the professionals, such as the tiring and indispensable requirement for the use and removal of all Personal Protective Equipment (PPE) necessary to guarantee collective protection (Cabarkapa et al., 2020), the strenuous working hours and inadequate working conditions, it should be noted that those professionals were already exhausted before the pandemic and remained exhausted during the period we applied the second questionnaire. In this setting, the most significant change in profile was driven by “disengagement.” According to a study of Romanian psychiatric residents, all participants who experienced high burnout (n = 26) were satisfied with their salary, but dissatisfied with the resources available for patient care (Tipa et al., 2019). These factors are capable of intensifying negative symptoms, such as feelings of vulnerability, powerlessness and fear, resulting in an exacerbated effort in the workplace with limited opportunities for recovery (Bai et al., 2004; Talaee et al., 2022). These conditions were more common in healthcare professionals who had difficulty sleeping, difficulty concentrating, feelings of indifference and of anxiety, in agreement with another study of Swedish healthcare professionals in which the data revealed self-reported depression, anxiety, sleep, memory impairment, neck and back pain (Peterson et al., 2008). A study of 227 physicians reported some ways to reduce anxiety and burnout rates, through interventions that taught them about the psychology of burnout, stress, coping with patient death and suffering management, as well as providing information about prevalence rates among physicians. The results were based on a before-and-after analysis of symptoms, producing a significant decrease in physicians’ levels of burnout and anxiety. From this, it can be inferred that despite the fact that burnout has several triggers, anxiety probably is one of the main intrinsic and potentiating factors of the syndrome, considering that it was the only factor that had an important decrease concomitant with exhaustion (Medisauskaite and Kamau, 2019).
To the detriment of the context of the COVID-19 pandemic, there is a need for these professionals to have coping strategies to attenuate negative symptoms. Therefore, our study had a secondary aim to sought to measure the relationship of faith as a coping strategy through a non-validated questionnaire of religious beliefs and habits. The habit of praying every day was a significant protective factor for burnout, and this may occur through the perception of divine protection, as mentioned by Tavares Quelho, while discussing spirituality as a dimension of protection and humanization, in addition to bringing the character of hope (Tavares, 2020). A different study with healthcare professionals in Hong Kong demonstrated in a regression analysis that daily spiritual practice acts as a protective factor not only against burnout, but also against depression and anxiety (Shaniuk, 2020).
Some coping strategies, such as substance abuse, may have positive short-term effects, but can have negative long-term repercussions (Costa and Moss, 2018). Our findings reveal that a significant portion of the study population consumed alcohol, and this feature was an independent risk factor for the development of burnout. This observation reinforces the hypothesis that alcohol abuse is associated with higher levels of burnout. Likewise, the Swedish study of healthcare professionals found that alcohol consumption was indeed the factor that most clearly differentiated the exhausted/disengaged group from the non-exhausted group (Peterson et al., 2008; Galaiya et al., 2020).
Importantly, the present study has some limitations. This was a single-center study that may suffer from unmeasured effects. Due to the small sample size, a more detailed analysis of habits was not carried out, such as the quantification of alcohol consumption, the modality of physical activity or the assessment of personality traits. The latter can influence the associations described in this study. People with higher levels of extroversion and openness are more likely to drink alcohol, and individuals with higher levels of neuroticism may have difficulty managing their emotions and may turn to alcohol as a coping mechanism. Not only that, higher levels of neuroticism can turn a person away from religious beliefs (Khoynezhad et al., 2012; Lui et al., 2022). Regarding the interpretation of the spiritual influence and religious beliefs on the professional’s mental health status, even with the Beliefs scale, faith is not objectively measurable, and there is no gold standard for the analysis of this variable. As a weakness, religious beliefs may lead to a false sense of security and delay professional assistance (Koenig, 2012). Regardless, the results presented here are relevant an contribute to the knowledge in the field as they demonstrate a solid interaction between specific characteristics of healthcare professionals and occurrence of burnout in a population that dramatically suffered with the COVID-19 pandemic in one of the countries which had the highest disease burden in the world.
5. Conclusion
Among Brazilian healthcare professionals from ED and ICU from a hospital directly affected by COVID-19 pandemic, alcohol use was the strongest factor predisposing to increasing risk of burnout whereas the habit of praying daily and working in the ICU were protective against such syndrome. These findings may guide decision-making strategies to implement institutional measures to reduce risk of burnout in extreme conditions such as the catastrophic scenario caused by the SARS-CoV-2 virus.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of Federal University of Bahia. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RS, RM, IF, SG, HP, NF, and BA: conceptualization, design of study, and manuscript draft. RS, RM, IF, and KA: investigation and visualization. RS, RM, NF, and KA: data acquisition. RS, RM, IF, MA-P, SG, HP, and BA: data analysis and interpretation. RS, RM, IF, SG, HP, and BA: supervision, critical revision, editing and final approval of the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by the Intramural Research Program of the Oswaldo Cruz Foundation, Brazil.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1058417/full#supplementary-material
References
Arpacioglu, S., Gurler, M., and Cakiroglu, S. (2021). Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int. J. Soc. Psychiatry 67, 84–89. doi: 10.1177/0020764020940742
Bai, Y. M., Lin, C. C., Lin, C. Y., Chen, J. Y., Chue, C. M., and Chou, P. (2004). Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 55, 1055–1057. doi: 10.1176/appi.ps.55.9.1055
Bakker, A. B., Demerouti, E., and Verbeke, W. (2004). Using the job demands-resources model to predict burnout and performance. Hum. Resour. Manag. 43, 83–104. doi: 10.1002/hrm.20004
Cabarkapa, S., Nadjidai, S. E., Murgier, J., and Ng, C. H. (2020). The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: a rapid systematic review. Brain Behav. Immun. Health 8:100144. doi: 10.1016/j.bbih.2020.100144
Cipolotti, L., Chan, E., Murphy, P., van Harskamp, N., and Foley, J. A. (2021). Factors contributing to the distress, concerns, and needs of UK neuroscience health care workers during the COVID-19 pandemic. Psychol. Psychother. Theory Res. Pract. 94, 536–543. doi: 10.1111/papt.12298
Costa, D. K., and Moss, M. (2018). The cost of caring: emotion, burnout, and psychological distress in critical care clinicians. Ann. Am. Thorac. Soc. 15, 787–790. doi: 10.1513/AnnalsATS.201804-269PS
da Silva Schuster, M., and da Veiga Dias, V. (2018). Oldenburg Burnout Inventory - validação de uma nova forma de mensurar Burnout no Brasil. Cien. Saude Colet. 23, 553–562. doi: 10.1590/1413-81232018232.27952015
de Oliveira, W. A., de Oliveira-Cardoso, É. A., Da Silva, J. L., and Dos Santos, M. A. (2020). Psychological and occupational impacts of the recent successive pandemic waves on health workers: an integrative review and lessons learned. Estud. Psicol. (Campinas) 37, 1–12. doi: 10.1590/1982-0275202037e200066
Demerouti, E. (2008). “Measurement of burnout and engagement” in Handbook of Stress and Burnout in Health Care. ed. J. R. B. Halbesleben (Hauppauge, NY: Nova Science Publisher), 1–25.
Demerouti, E., Nachreiner, F., Bakker, A. B., and Schaufeli, W. B. (2001). The job demands-resources model of burnout. J. Appl. Psychol. 86, 499–512. doi: 10.1037/0021-9010.86.3.499
Di Tella, M., Romeo, A., Benfante, A., and Castelli, L. (2020). Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 26, 1583–1587. doi: 10.1111/jep.13444
Dos Santos Barros, M. M., De Almeida, S. P., Barreto, A. L. P., Faro, S. R. S., De Araújo, M. R. M., and Faro, A. (2016). Síndrome de Burnout em Médicos Intensivistas: Estudo em UTIs de Sergipe. Temas Psicol. 24, 377–389. doi: 10.9788/TP2016.1-26
Dosil, M., Ozamiz-etxebarria, N., and Redondo, I. (2020). Since January 2020 Elsevier has Created a COVID-19 Resource Centre with Free Information in English and Mandarin on the Novel Coronavirus COVID-19. The COVID-19 Resource Centre is Hosted on Elsevier Connect, the Company’s Public News and Information. 14. Amsterdam: Elevier, 106–112.
Fetzer Institute, and National Institute on Aging Working Group. (1999). Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research. Kalamazoo, Michigan: John E. Fetzer Institute.
Galaiya, R., Kinross, J., and Arulampalam, T. (2020). Factors associated with burnout syndrome in surgeons: a systematic review. Ann. R. Coll. Surg. Engl. 102, 401–407. doi: 10.1308/rcsann.2020.0040
Khoynezhad, G., Rajaei, A. R., and Sarvarazemy, A. (2012). Basic religious beliefs and personality traits. Iran. J. Psychiatry 7, 82–86.
Koenig, H. G. (2012). Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatry 2012, 1–33. doi: 10.5402/2012/278730
Lui, P. P., Chmielewski, M., Trujillo, M., Morris, J., and Pigott, T. D. (2022). Linking big five personality domains and facets to alcohol (Mis)use: a systematic review and meta-analysis. Alcohol Alcohol. 57, 58–73. doi: 10.1093/alcalc/agab030
Medisauskaite, A., and Kamau, C. (2019). Reducing burnout and anxiety among doctors: randomized controlled trial. Psychiatry Res. 274, 383–390. doi: 10.1016/j.psychres.2019.02.075
Ornell, F., Schuch, J. B., Sordi, A. O., and Kessler, F. H. P. (2020). ‘“Pandemic fear”’ and COVID-19: mental health burden and strategies. Braz. J. Psychiatry 42, 232–235. doi: 10.1590/1516-4446-2020-0008
Peterson, U., Demerouti, E., Bergström, G., Samuelsson, M., Åsberg, M., and Nygren, Å. (2008). Burnout and physical and mental health among Swedish healthcare workers. J. Adv. Nurs. 62, 84–95. doi: 10.1111/j.1365-2648.2007.04580.x
Romero, C. S., Catalá, J., Delgado, C., Ferrer, C., Errando, C., Iftimi, A., et al. (2020). COVID-19 psychological impact in 3109 healthcare workers in Spain: the PSIMCOV group. Psychol. Med. 52, 188–194. doi: 10.1017/S0033291720001671
Rossi, R., Socci, V., Pacitti, F., Di Lorenzo, G., Di Marco, A., Siracusano, A., et al. (2020). Mental health outcomes among frontline and second-line health care workers during the coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 3, 3–6. doi: 10.1001/jamanetworkopen.2020.10185
Rumeysa, E., Kurtulmus, A., Arpacioglu, S., and Karadere, E. (2020). Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 290, 113–130. doi: 10.1016/j.psychres.2020.113130
Shaniuk, P. M. (2020). The spiritual works of mercy as a tool to prevent burnout in medical trainees. Linacre Q. 87, 399–406. doi: 10.1177/0024363920920400
Talaee, N., Varahram, M., Jamaati, H., Salimi, A., Attarchi, M., Kazempour Dizaji, M., et al. (2022). Stress and burnout in health care workers during COVID-19 pandemic: validation of a questionnaire. J. Public Health (Germany) 30, 531–536. doi: 10.1007/s10389-020-01313-z
Tavares, C. Q. (2020). Dimensões do cuidado na perspectiva da espiritualidade durante a pandemia pelo novo coronavírus (COVID-19). J. Health NPEPS 5, 1–4. doi: 10.30681/252610104517
Tipa, R. O., Tudose, C., and Pucarea, V. L. (2019). Measuring burnout among psychiatric residents using the Oldenburg burnout inventory (OLBI) instrument. J. Med. Life 12, 354–360. doi: 10.25122/jml-2019-0089
Keywords: COVID-19, burnout syndrome, health professionals, ICU, beliefs, emergency
Citation: Silva RRC, Menezes RC, Garcia SL, Pustilnik HN, Ferreira IBB, Aguiar KVCS, Filgueiras Filho NM, Araújo-Pereira M and Andrade BB (2023) Assessment of the risk of burnout and its associated factors in healthcare professionals during the COVID-19 pandemic: A prospective cohort study. Front. Psychol. 14:1058417. doi: 10.3389/fpsyg.2023.1058417
Edited by:
Michela Di Trani, Sapienza University of Rome, ItalyReviewed by:
Daniela De Berardinis, Fatebenefratelli Hospital, ItalyMartin Klasen, RWTH Aachen University, Germany
Copyright © 2023 Silva, Menezes, Garcia, Pustilnik, Ferreira, Aguiar, Filgueiras Filho, Araújo-Pereira and Andrade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bruno B. Andrade, ✉ bruno.andrade@fiocruz.br
†These authors have contributed equally to this work
‡These authors share senior authorship