
The Role of Resilience for Migrants and Refugees’ Mental Health in Times of COVID-19

 ,
,  ,
,
Abstract
:1. Introduction
2. Method
2.1. Materials
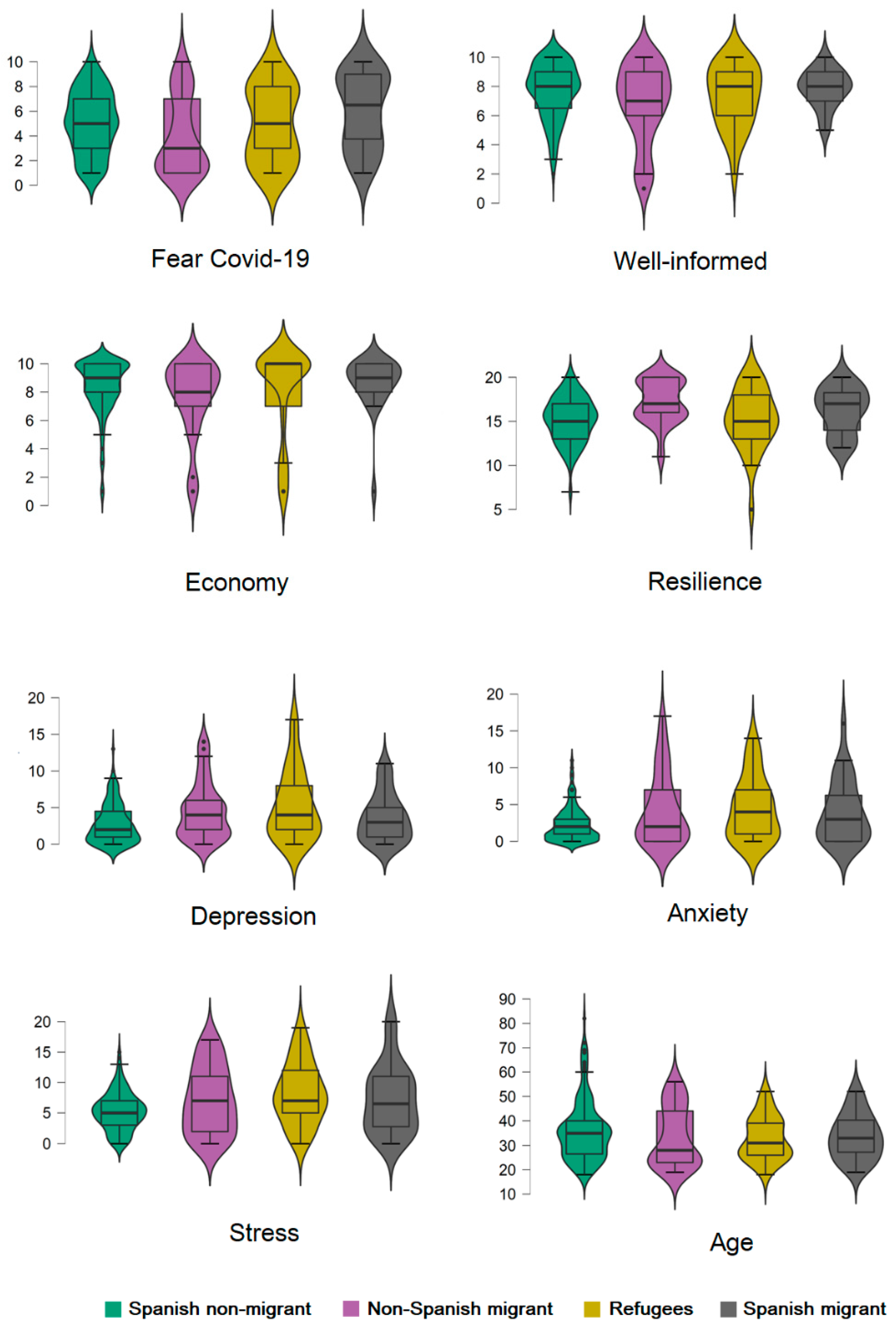
- (i)
- I fear COVID-19
- (ii)
- I consider that I have correctly informed myself about COVID-19
- (iii)
- I am concerned about the economic impact that this pandemic may have in my country.
2.2. Procedure
2.3. Participants and Ethics
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, H.; Nie, P.; Qian, L. Do Quarantine Experiences and Attitudes Towards COVID-19 Affect the Distribution of Mental Health in China? A Quantile Regression Analysis. Appl. Res. Qual. Life 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Valeriani, G.; Sarajlic Vukovic, I.; Lindegaard, T.; Felizia, R.; Mollica, R.; Andersson, G. Addressing Healthcare Gaps in Sweden during the COVID-19 Outbreak: On Community Outreach and Empowering Ethnic Minority Groups in a Digitalized Context. Healthcare 2020, 8, 445. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.S.; Feyissa, I.F.; Suk, S.-W. Panic and Trust during COVID-19: A Cross-Sectional Study on Immigrants in South Korea. Healthcare 2021, 9, 199. [Google Scholar] [CrossRef] [PubMed]
- Brunnet, A.E.; dos Santos Lobo, N.; Silveira, T.; Kristensen, C.H.; Derivois, D. Migrations, Trauma and Mental Health: A Literature Update on Psychological Assessment. L’Encéphale 2020, 46, 364–371. [Google Scholar] [CrossRef]
- Zlotnick, C.; Dryjanska, L.; Suckerman, S. Health Literacy, Resilience and Perceived Stress of Migrants in Israel during the COVID-19 Pandemic. Psychol. Health 2021, 1–17. [Google Scholar] [CrossRef]
- Siqueira, C.A.d.S.; de Freitas, Y.N.L.; Cancela, M.d.C.; Carvalho, M.; Oliveras-Fabregas, A.; de Souza, D.L.B. The Effect of Lockdown on the Outcomes of COVID-19 in Spain: An Ecological Study. PLoS ONE 2020, 15, e0236779. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Moret-Tatay, C. Personality and Attitudes Confronting Death Awareness During the COVID-19 Outbreak in Italy and Spain. Front. Psychiatry 2021, 12, 627018. [Google Scholar] [CrossRef]
- Cramer, H.; Kemper, K.; Mo, X.; Khayat, R. Are mindfulness and self-compassion associated with sleep and resilience in health professionals? Dtsch. Z. Für Akupunkt. 2016, 59, 28–29. [Google Scholar] [CrossRef] [Green Version]
- Haddadi, P.; Besharat, M.A. Resilience, Vulnerability and Mental Health. Procedia-Soc. Behav. Sci. 2010, 5, 639–642. [Google Scholar] [CrossRef] [Green Version]
- Olsson, C.A.; Bond, L.; Burns, J.M.; Vella-Brodrick, D.A.; Sawyer, S.M. Adolescent Resilience: A Concept Analysis. J. Adolesc. 2003, 26, 1–11. [Google Scholar] [CrossRef]
- Malhi, G.S.; Das, P.; Bell, E.; Mattingly, G.; Mannie, Z. Modelling Resilience in Adolescence and Adversity: A Novel Framework to Inform Research and Practice. Transl. Psychiatry 2019, 9, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fino, E.; Mema, D.; Russo, P.M. War Trauma Exposed Refugees and Posttraumatic Stress Disorder: The Moderating Role of Trait Resilience. J. Psychosom. Res. 2020, 129, 109905. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.J.; Zhang, Z.; Zhang, X.Y.; Tang, Y.; Chen, P.; Liang, M.Z.; Sun, Z.; Yu, Y.L. State or Trait? Measuring Resilience by Generalisability Theory in Breast Cancer. Eur. J. Oncol. Nurs. 2020, 46, 101727. [Google Scholar] [CrossRef]
- Parsons, M.; Glavac, S.; Hastings, P.; Marshall, G.; McGregor, J.; McNeill, J.; Morley, P.; Reeve, I.; Stayner, R. Top-down Assessment of Disaster Resilience: A Conceptual Framework Using Coping and Adaptive Capacities. Int. J. Disaster Risk Reduct. 2016, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.; Lami, A.; Moret-Tatay, C. An Italian Adaptation of the Brief Resilient Coping Scale (BRCS) and Attitudes during the Covid-19 Outbreak. Front. Psychol. 2021, 12, 641213. [Google Scholar] [CrossRef]
- Gatt, J.M.; Alexander, R.; Emond, A.; Foster, K.; Hadfield, K.; Mason-Jones, A.; Reid, S.; Theron, L.; Ungar, M.; Wouldes, T.A.; et al. Trauma, Resilience, and Mental Health in Migrant and Non-Migrant Youth: An International Cross-Sectional Study Across Six Countries. Front. Psychiatry 2020, 10, 997. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Mengual, N.; Aragonés-Barbera, I.; Moret-Tatay, C.; Moliner-Albero, A.R. The Relationship of Fear of Death between Neuroticism and Anxiety during the Covid-19 Pandemic. Front. Psychiatry 2021, 12, 648498. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F. Long-Term Stability of Depression, Anxiety, and Stress Syndromes. J. Abnorm. Psychol. 1998, 107, 520–526. [Google Scholar] [CrossRef]
- Daza, P.; Novy, D.M.; Stanley, M.A.; Averill, P. The Depression Anxiety Stress Scale-21: Spanish translation and validation with a Hispanic sample. J. Psychopathol. Behav. Assess. 2002, 24, 195–205. [Google Scholar] [CrossRef]
- Apóstolo, J.L.A.; Mendes, A.C.; Azeredo, Z.A. Adaptation to Portuguese of the Depression, Anxiety and Stress Scales (DASS). Rev. Lat. Am. Enfermagem 2006, 14, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Clara, I.P.; Cox, B.J.; Enns, M.W. Confirmatory Factor Analysis of the Depression-Anxiety-Stress Scales in Depressed and Anxious Patients. J. Psychopathol. Behav. Assess. 2001, 23, 61–67. [Google Scholar] [CrossRef]
- Moret-Tatay, C.; Fernández-Muñoz, J.J.; Civera-Mollá, C.; Navarro-Pardo, E.; Alcover-de-la-Hera, C. Psychometric Properties and Factor Structure of the BRCS in an Elderly Spanish Sample. Ann. Psicol. 2015, 31, 1030. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, V.G.; Wallston, K.A. The Development and Psychometric Evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Daniels, J.P. Venezuelan Migrants “Struggling to Survive” amid COVID-19. Lancet 2020, 395, 1023. [Google Scholar] [CrossRef]
- Wu, Q.; Ge, T.; Emond, A.; Foster, K.; Gatt, J.M.; Hadfield, K.; Mason-Jones, A.J.; Reid, S.; Theron, L.; Ungar, M.; et al. Acculturation, Resilience, and the Mental Health of Migrant Youth: A Cross-Country Comparative Study. Public Health 2018, 162, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Sundvall, M.; Titelman, D.; DeMarinis, V.; Borisova, L.; Çetrez, Ö. Safe but Isolated—An Interview Study with Iraqi Refugees in Sweden about Social Networks, Social Support, and Mental Health. Int. J. Soc. Psychiatry 2020, 67, 351–359. [Google Scholar] [CrossRef]
- Hjemdal, O.; Vogel, P.A.; Solem, S.; Hagen, K.; Stiles, T.C. The Relationship between Resilience and Levels of Anxiety, Depression, and Obsessive-Compulsive Symptoms in Adolescents. Clin. Psychol. Psychother. 2011, 18, 314–321. [Google Scholar] [CrossRef]
- Venta, A.; Bailey, C.; Muñoz, C.; Godinez, E.; Colin, Y.; Arreola, A.; Abate, A.; Camins, J.; Rivas, M.; Lawlace, S. Contribution of Schools to Mental Health and Resilience in Recently Immigrated Youth. Sch. Psychol. 2019, 34, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Yang, X.; Zeng, C.; Wang, Y.; Shen, Z.; Li, X.; Lin, D. Resilience, Social Support, and Coping as Mediators between COVID-19-related Stressful Experiences and Acute Stress Disorder among College Students in China. Appl. Psychol. Health Well-Being 2020, 12, 1074–1094. [Google Scholar] [CrossRef]
- Leppin, A.L.; Gionfriddo, M.R.; Sood, A.; Montori, V.M.; Erwin, P.J.; Zeballos-Palacios, C.; Bora, P.R.; Dulohery, M.M.; Brito, J.P.; Boehmer, K.R.; et al. The Efficacy of Resilience Training Programs: A Systematic Review Protocol. Syst. Rev. 2014, 3, 20. [Google Scholar] [CrossRef] [Green Version]
- Forbes, S.; Fikretoglu, D. Building Resilience: The Conceptual Basis and Research Evidence for Resilience Training Programs. Rev. Gen. Psychol. 2018, 22, 452–468. [Google Scholar] [CrossRef]
- Lima, M.P.; Moret-Tatay, C.; Irigaray, T.Q. Locus of Control, Personality and Depression Symptoms in Cancer: Testing a Moderated Mediation Model. Clin. Psychol. Psychother. 2021. [Google Scholar] [CrossRef] [PubMed]
- Teismann, T.; Brailovskaia, J. Entrapment, Positive Psychological Functioning and Suicide Ideation: A Moderation Analysis. Clin. Psychol. Psychother. 2020, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 95% CI for Cohen’s d | ||||||
|---|---|---|---|---|---|---|
| Variable | Migrant | Non-Migrant | p | Cohen’s d | Lower | Upper |
| Fear COVID-19 | 4.81 (3.16) | 5.09 (2.51) | 0.434 | 0.102 | −0.153 | 0.356 |
| Well-informed | 7.23 (2.24) | 7.66 (1.88) | 0.106 | 0.210 | −0.045 | 0.465 |
| Economy | 8.02 (2.67) | 8.35 (1.94) | 0.279 | 0.141 | −0.114 | 0.395 |
| Resilience | 16.38 (2.88) | 15.17 (2.56) | <0.001 | −0.448 | −0.704 | −0.190 |
| Depression | 4.55 (4.02) | 2.73 (2.65) | <0.001 | −0.554 | −0.812 | −0.295 |
| Anxiety | 4.30 (4.47) | 2.31 (2.31) | <0.001 | −0.589 | −0.847 | −0.329 |
| Stress | 7.48 (5.31) | 5.28 (3.09) | <0.001 | −0.527 | −0.785 | −0.269 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Fear COVID-19 (1) | — | ||||||
| Well-Informed (2) | 0.133 * | — | |||||
| Economy (3) | 0.170 ** | 0.124 | — | ||||
| Resilience (4) | −0.007 | 0.097 | 0.096 | — | |||
| Depression (5) | 0.016 | −0.080 | 0.027 | −0.357 *** | — | ||
| Anxiety (6) | 0.197 ** | −0.002 | 0.111 | −0.224 *** | 0.603 *** | — | |
| Stress (7) | 0.146 * | 0.011 | 0.018 | −0.234 *** | 0.606 *** | 0.733 *** | — |
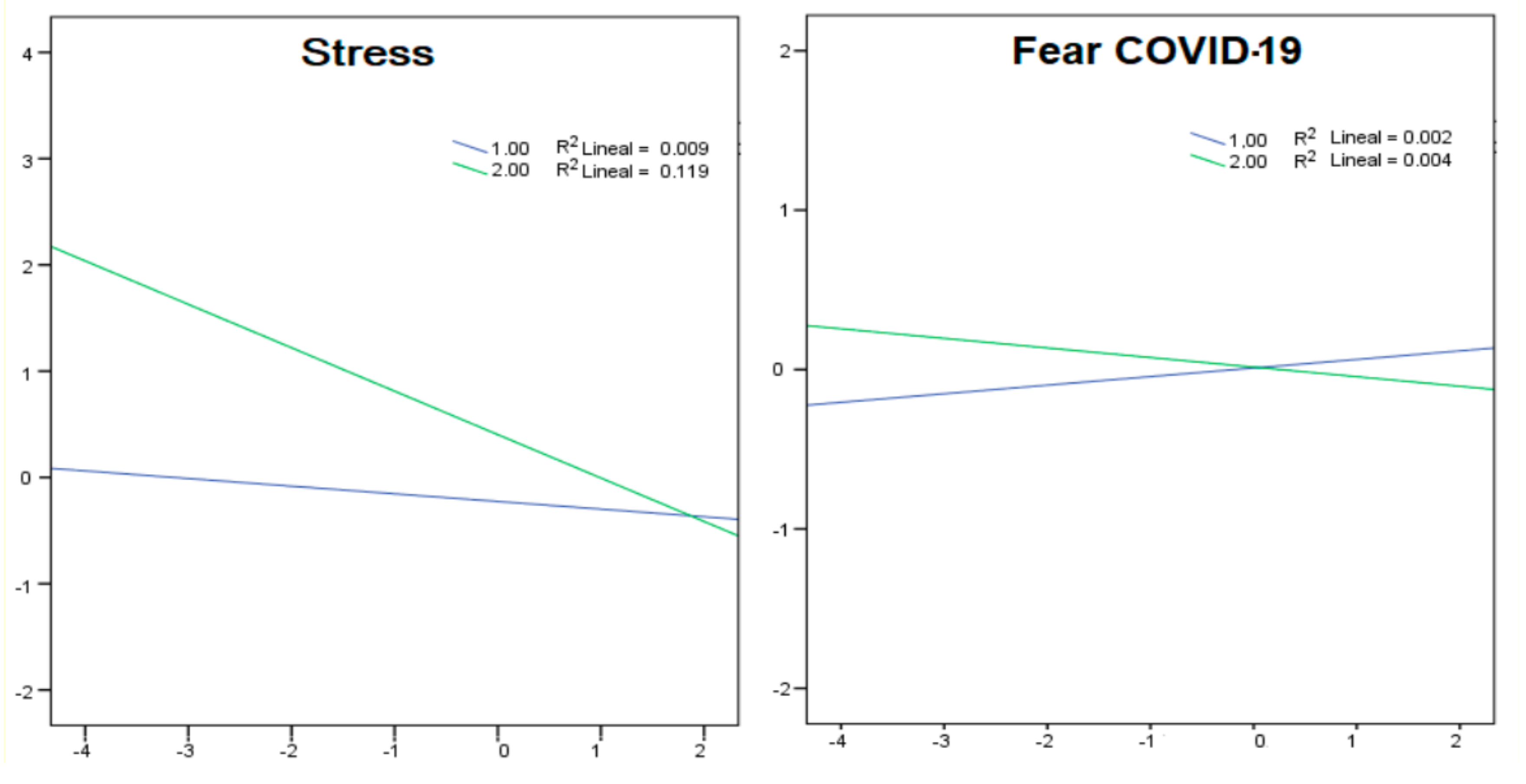
| Model | Coeff | SE | t | p | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| Depression | Constant | 0.0324 | 0.0609 | 0.5315 | 0.5955 | −0.0876 | 0.1524 |
| Group | 0.7044 | 0.1329 | 5.2992 | <0.001 | 0.4425 | 0.9662 | |
| Resilience | −0.3349 | 0.0624 | −5.3668 | <0.001 | −0.4578 | −0.212 | |
| Interaction | −0.3044 | 0.13 | −2.341 | 0.02 | −0.5605 | −0.0483 | |
| Anxiety | Constant | 0.0312 | 0.062 | 0.5025 | 0.6158 | −0.091 | 0.1533 |
| Group | 0.6768 | 0.1392 | 4.8603 | <0.001 | 0.4025 | 0.9511 | |
| Resilience | −0.2036 | 0.059 | −3.4526 | 0.0007 | −0.3197 | −0.0874 | |
| Interaction | −0.2928 | 0.127 | −2.3056 | 0.022 | −0.5429 | −0.0426 | |
| Stress | Constant | 0.0358 | 0.0603 | 0.5938 | 0.5532 | −0.083 | 0.1547 |
| Group | 0.6289 | 0.1324 | 4.7502 | <0.001 | 0.3681 | 0.8896 | |
| Resilience | −0.2121 | 0.0557 | −3.8074 | 0.0002 | −0.3218 | −0.1024 | |
| Interaction | −0.3366 | 0.1138 | −2.9569 | 0.0034 | −0.5609 | −0.1124 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solà-Sales, S.; Pérez-González, N.; Van Hoey, J.; Iborra-Marmolejo, I.; Beneyto-Arrojo, M.J.; Moret-Tatay, C. The Role of Resilience for Migrants and Refugees’ Mental Health in Times of COVID-19. Healthcare 2021, 9, 1131. https://doi.org/10.3390/healthcare9091131
Solà-Sales S, Pérez-González N, Van Hoey J, Iborra-Marmolejo I, Beneyto-Arrojo MJ, Moret-Tatay C. The Role of Resilience for Migrants and Refugees’ Mental Health in Times of COVID-19. Healthcare. 2021; 9(9):1131. https://doi.org/10.3390/healthcare9091131
Chicago/Turabian StyleSolà-Sales, Sara, Natalia Pérez-González, Julie Van Hoey, Isabel Iborra-Marmolejo, María José Beneyto-Arrojo, and Carmen Moret-Tatay. 2021. "The Role of Resilience for Migrants and Refugees’ Mental Health in Times of COVID-19" Healthcare 9, no. 9: 1131. https://doi.org/10.3390/healthcare9091131