
Prognostic Role of Subcutaneous and Visceral Adiposity in Hospitalized Octogenarians with COVID-19

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Setting and Participants
2.2. Data Collection
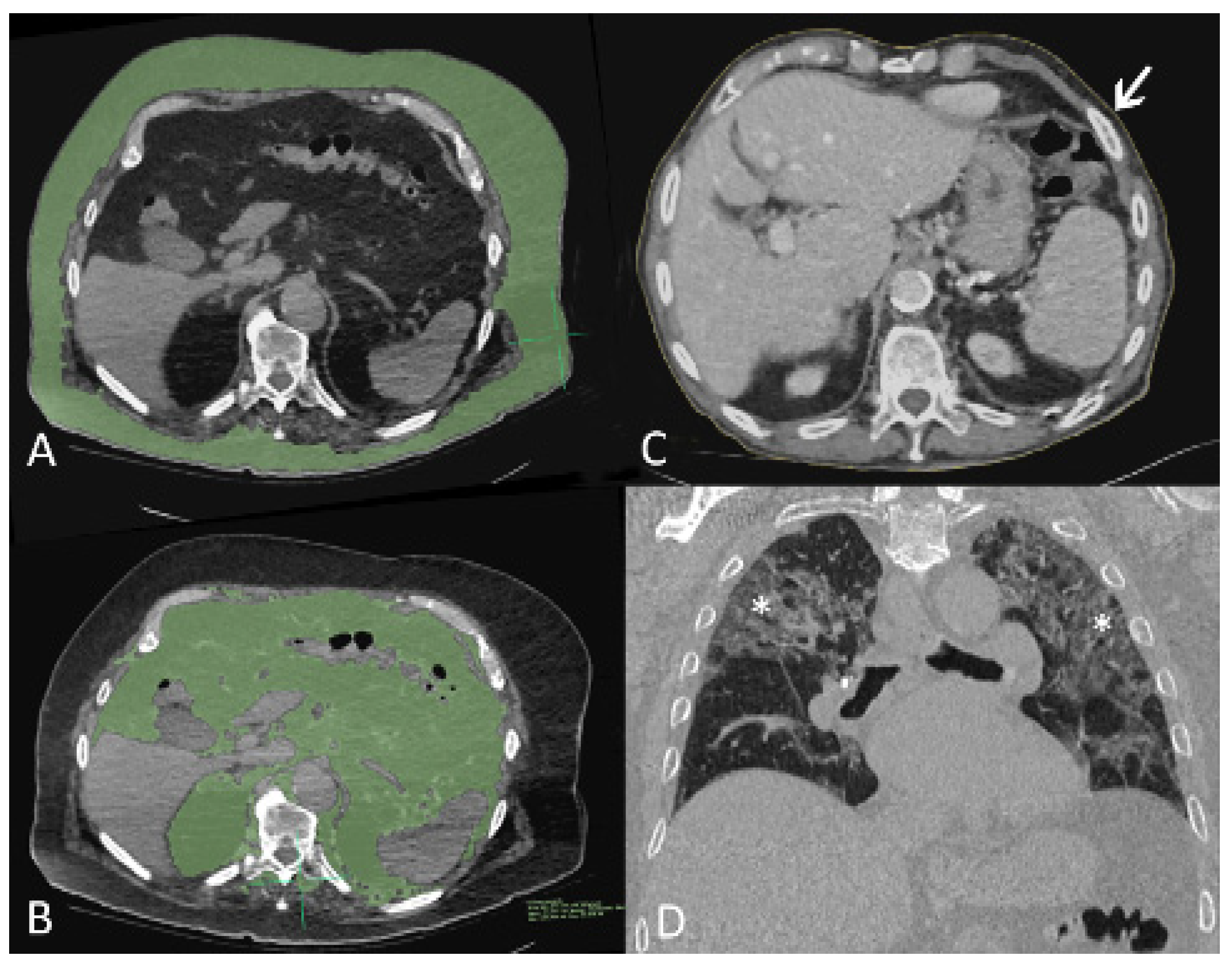
2.3. CT Scans Acquisitions, Interpretation and Quantification
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Adiposity Measures and the Radiological Extent of COVID-19 Pneumonia
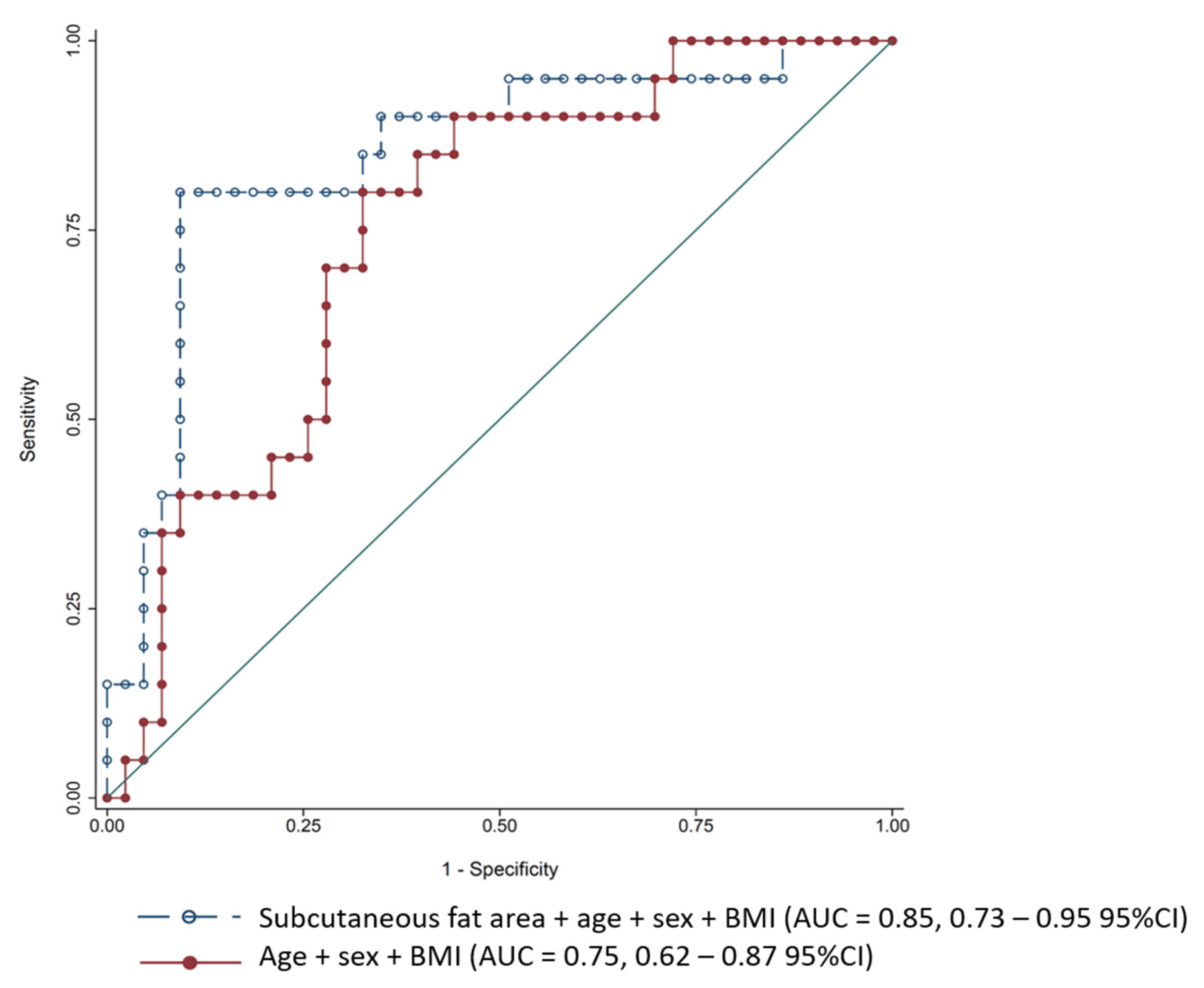
3.3. Adiposity Measures and In-Hospital Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mendes, A.; Serratrice, C.; Herrmann, F.R.; Genton, L.; Périvier, S.; Scheffler, M.; Fassier, T.; Huber, P.; Jacques, M.-C.; Prendki, V.; et al. Predictors of In-hospital mortality in older patients with COVID-19: The COVIDAge Study. J. Am. Med. Dir. Assoc. 2020, 21, 1546–1554.e3. [Google Scholar] [CrossRef]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Sarcopenia Is associated with incident disability, Institutionalization, and mortality in community-dwelling older men: The concord health and ageing in men project. J. Am. Med. Dir. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef]
- Cerri, A.P.; Bellelli, G.; Mazzone, A.; Pittella, F.; Landi, F.; Zambon, A.; Annoni, G. Sarcopenia and malnutrition in acutely ill hospitalized elderly: Prevalence and outcomes. Clin. Nutr. 2015, 34, 745–751. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in obesity among adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [Green Version]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective Cohort Study. BMJ 2020, 369, 1966. [Google Scholar] [CrossRef]
- Watanabe, M.; Caruso, D.; Tuccinardi, D.; Risi, R.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Tarallo, M.; Strigari, L.; Manfrini, S. Visceral Fat Shows the Strongest Association with the Need of Intensive Care in Patients with COVID-19. Metabolism 2020, 111, 154319. [Google Scholar] [CrossRef]
- Petersen, A.; Bressem, K.; Albrecht, J.; Thieß, H.-M.; Vahldiek, J.; Hamm, B.; Makowski, M.R.; Niehues, A.; Niehues, S.M.; Adams, L.C. The Role of Visceral Adiposity in the Severity of COVID-19: Highlights from A unicenter Cross-sectional Pilot Study in Germany. Metabolism 2020, 110, 154317. [Google Scholar] [CrossRef]
- Calabrò, P.; Golia, E.; Maddaloni, V.; Malvezzi, M.; Casillo, B.; Marotta, C.; Calabro, R.; Golino, P. Adipose Tissue-Mediated Inflammation: The Missing Link between Obesity and Cardiovascular Disease? Intern. Emerg. Med. 2009, 4, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.C.; Busetto, L.; Cederholm, T.; Chourdakis, M.; Cuerda, C.; Delzenne, N.; Genton, L.; Schneider, S.; Singer, P.; et al. Nutritional Management of Individuals with Obesity and COVID-19: ESPEN Expert statements and Practical Guidance. Clin. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gupte, M.; Boustany-Kari, C.M.; Bharadwaj, K.; Police, S.; Thatcher, S.; Gong, M.C.; English, V.L.; Cassis, L.A. ACE2 is expressed in mouse adipocytes and regulated by a high-fat diet. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R781–R788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgonje, A.R.; Abdulle, A.E.; Timens, W.; Hillebrands, J.-L.; Navis, G.J.; Gordijn, S.J.; Bolling, M.C.; Dijkstra, G.; Voors, A.A.; Osterhaus, A.D.; et al. Angiotensin-Converting Enzyme 2 (ACE2), SARS-CoV-2 and the Pathophysiology of Coronavirus Disease 2019 (COVID-19). J. Pathol. 2020, 251, 228–248. [Google Scholar] [CrossRef]
- Zarkesh-Esfahani, H.; Pockley, A.G.; Wu, Z.; Hellewell, P.G.; Weetman, A.P.; Ross, R.J.M. Leptin Indirectly Activates Human Neutrophils via Induction of TNF-Alpha. J. Immunol. 2004, 172, 1809–1814. [Google Scholar] [CrossRef] [Green Version]
- Guglielmi, V.; Colangeli, L.; D’Adamo, M.; Sbraccia, P. Susceptibility and Severity of Viral Infections in Obesity: Lessons from Influenza to COVID-19. Does Leptin Play a Role? Int. J. Mol. Sci. 2021, 22, 3183. [Google Scholar] [CrossRef] [PubMed]
- Kiernan, K.; MacIver, N.J. The Role of the Adipokine Leptin in Immune Cell Function in Health and Disease. Front. Immunol. 2020, 11, 3656. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in Inflammation and Metabolic Disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Ohashi, K.; Shibata, R.; Murohara, T.; Ouchi, N. Role of Anti-inflammatory Adipokines in Obesity-Related Diseases. Trends. Endocrinol. Metab. 2014, 25, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Tchernof, A.; Després, J.-P. Pathophysiology of Human Visceral Obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed]
- Favre, G.; Legueult, K.; Pradier, C.; Raffaelli, C.; Ichai, C.; Iannelli, A.; Redheuil, A.; Lucidarme, O.; Esnault, V. Visceral Fat is Associated to the Severity of COVID-19. Metabolism 2021, 115, 154440. [Google Scholar] [CrossRef]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A Manual of Guidelines to Score the Modified Cumulative Illness Rating Scale and its Validation in Acute Hospitalized Elderly Patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Lim, W.; van der Eerden, M.M.; Laing, R.; Boersma, W.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc anaysis of a prospective cohort study. Clin. Nutr. 2021, 40, 2420–2426. [Google Scholar] [CrossRef]
- Englert, J.A.; Rogers, A.J. Metabolism, Metabolomics, and Nutritional Support of Patients with Sepsis. Clin. Chest. Med. 2016, 37, 321–331. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Zhang, T.; Wang, Y.; Xia, L. The Centrality of Obesity in the Course of Severe COVID-19. Front. Endocrinol. 2021, 12, 620566. [Google Scholar] [CrossRef]
- Battisti, S.; Pedone, C.; Napoli, N.; Russo, E.; Agnoletti, V.; Nigra, S.G.; Dengo, C.; Mughetti, M.; Conte, C.; Pozzilli, P.; et al. Computed Tomography Highlights Increased Visceral Adiposity Associated with Critical Illness in COVID-19. Diabetes. Care 2020, 43, 129–130. [Google Scholar] [CrossRef]
- Deng, M.; Qi, Y.; Deng, L.; Wang, H.; Xu, Y.; Li, Z.; Meng, Z.; Tang, J.; Dai, Z. Obesity as a Potential Predictor of Disease Severity in Young COVID-19 Patients: A Retrospective Study. Obesity 2020, 28, 1815–1825. [Google Scholar] [CrossRef]
- Yang, Y.; Ding, L.; Zou, X.; Shen, Y.; Hu, D.; Hu, X.; Li, Z.; Kamel, I.R. Visceral Adiposity and High Intramuscular Fat Deposition Independently Predict Critical Illness in Patients with SARS-CoV-2. Obesity 2020, 28, 2040–2048. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Intra-Hospital Death | |||
|---|---|---|---|---|
| Total | No | Yes | p Value | |
| N | 64 | 43 | 21 | |
| Age, year | 86.4 ± 6.0 | 86.3 ± 5.8 | 86.7 ± 6.6 | 0.797 |
| Male sex | 30 (46.9%) | 14 (32.6%) | 16 (76.2%) | 0.001 |
| Time from symptoms to hospital admission, day | 3.6 ± 3.1 | 4.1 ± 3.5 | 2.6 ± 1.7 | 0.026 |
| Length of stay, day | 12.5 ± 5.6 | 13.7 ± 5.0 | 10.0 ± 6.1 | 0.025 |
| FIM | 75.5 ± 31.1 | 82.5 ± 28.4 | 52.9 ± 29.8 | 0.005 |
| CFS | 5.7 ± 1.8 | 5.2 ± 1.7 | 6.8 ± 1.4 | <0.001 |
| CIRS-G | 19.3 ± 6.1 | 18.3 ± 6.4 | 21.1 ± 5.0 | 0.060 |
| CAM | 13 (20.6%) | 6 (14.0%) | 7 (35.0%) | 0.092 |
| CURB-65 | 0.648 | |||
| 1 | 10 (15.6%) | 8 (18.6%) | 2 (9.5%) | |
| 2 | 29 (45.3%) | 20 (46.5%) | 9 (42.9%) | |
| 3 | 23 (35.9%) | 14 (32.6%) | 9 (42.9%) | |
| 4 | 2 (3.1%) | 1 (2.3%) | 1 (4.8%) | |
| ARDS | 16 (25.0%) | 3 (7.0%) | 13 (61.9%) | <0.001 |
| BMI kg/m2 | 24.1 ± 4.4 | 23.6 ± 4.3 | 25.1 ± 4.6 | 0.217 |
| BMI kg/m2 | 0.247 | |||
| <20 | 10 (15.9%) | 8 (18.6%) | 2 (10.0%) | |
| 20–24.9 | 29 (46.0%) | 21 (48.8%) | 8 (40.0%) | |
| 25–29.9 | 18 (28.6%) | 10 (23.3%) | 8 (40.0%) | |
| 30+ | 6 (9.5%) | 4 (9.3%) | 2 (10.0%) | |
| NRS | 0.315 | |||
| 0–2 | 14 (21.9%) | 13 (30.2%) | 1 (4.8%) | |
| 3–4 | 20 (31.3%) | 10 (23.3%) | 10 (47.6%) | |
| 5–7 | 30 (46.9%) | 20 (46.5%) | 10 (47.6%) | |
| Hypertension | 44 (68.8%) | 31 (72.1%) | 13 (61.9%) | 0.566 |
| Dyslipidemia | 26 (40.6%) | 16 (37.2%) | 10 (47.6%) | 0.588 |
| Heart Failure | 24 (40.0%) | 13 (32.5%) | 11 (55.0%) | 0.105 |
| Diabetes | 14 (21.9%) | 9 (20.9%) | 5 (23.8%) | >0.99 |
| Kidney disease | 14 (21.9%) | 10 (23.3%) | 4 (19.0%) | >0.99 |
| Liver disease | 4 (6.3%) | 2 (4.7%) | 2 (9.5%) | 0.592 |
| COPD | 4 (6.3%) | 3 (7.0%) | 1 (4.8%) | >0.99 |
| Smoking | 0.789 | |||
| No smoking | 46 (71.9%) | 32 (74.4%) | 14 (66.7%) | |
| Past | 15 (23.4%) | 9 (20.9%) | 6 (28.6%) | |
| Present | 3 (4.7%) | 2 (4.7%) | 1 (4.8%) | |
| Stroke | 16 (25.8%) | 11 (26.2%) | 5 (25.0%) | >0.99 |
| Parkinson disease | 3 (4.8%) | 2 (4.7%) | 1 (5.0%) | >0.99 |
| Cognitive disorders | 33 (51.6%) | 23 (53.5%) | 10 (47.6%) | 0.791 |
| Known swallowing disorders | 4 (6.3%) | 2 (4.7%) | 2 (9.5%) | 0.592 |
| Active neoplasia | 5 (7.8%) | 3 (7.0%) | 2 (9.5%) | >0.99 |
| Immunosuppression | 3 (4.7%) | 2 (4.7%) | 1 (4.8%) | >0.99 |
| Albumin | 35.5 ± 8.0 | 35.7 ± 8.8 | 34.8 ± 5.2 | 0.641 |
| C-Reactive Protein | 56.2 ± 66.1 | 48.0 ± 41.2 | 73.9 ± 100.2 | 0.279 |
| Lymphocytes nb-abs | 1.3 ± 1.2 | 1.3 ± 1.3 | 1.1 ± 0.7 | 0.395 |
| Radiological Measures | ||||
| Extent of COVID-19 pneumonia | 0.813 | |||
| 0–25% | 33 (54.1%) | 22 (53.7%) | 11 (55.0%) | |
| 26–50% | 13 (21.3%) | 10 (24.4%) | 3 (15.0%) | |
| 51–75% | 11 (18.0%) | 7 (17.1%) | 4 (20.0%) | |
| 76–100% | 4 (6.6%) | 2 (4.9%) | 2 (10.0%) | |
| AC (mm) | 714.0 ± 196.3 | 743.9 ± 183.6 | 652.9 ± 211.6 | 0.101 |
| TF (mm2) | 267.5 ± 143.0 | 285.4 ± 142.6 | 231.1 ± 140.1 | 0.156 |
| SF (mm2) | 126.2 ± 86.4 | 142.7 ± 85.0 | 92.6 ± 81.1 | 0.028 |
| VF (mm2) | 141.3 ± 84.0 | 142.7 ± 81.9 | 138.5 ± 90.2 | 0.858 |
| Extent of COVID-19 Pneumonia | Model 1—Univariate | Model 2—Adjusted For Age and Sex | Model 3—Adjusted for Age, Sex and BMI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | R2 | OR | 95% CI | p Value | R2 | OR | 95% CI | p Value | R2 | |
| Age | 1.011 | 0.932–1.095 | 0.794 | 0.5% | ||||||||
| Male sex | 1.678 | 0.637–4.416 | 0.294 | 0.8% | ||||||||
| BMI | 1.004 | 0.905–1.114 | 0.934 | 0.1% | 0.001 | 0.001–0.055 | 0.985 | 0.5% | ||||
| Upper abdominal circumference | 1.041 | 1.014–1.068 | 0.003 | 7.3% | 1.041 | 1.014–1.069 | 0.002 | 8.0% | 1.042 | 1.015–1.071 | 0.002 | 8.2% |
| Total fat area | 1.766 | 1.230–2.537 | 0.002 | 7.9% | 1.806 | 1.249–2.609 | 0.002 | 9.1% | 1.851 | 1.27–2.695 | 0.001 | 9.5% |
| Subcutaneous fat area | 1.817 | 1.078–3.060 | 0.025 | 3.7% | 1.856 | 1.094–3.149 | 0.022 | 4.7% | 1.917 | 1.124–3.271 | 0.017 | 4.8% |
| Visceral fat area | 2.692 | 1.461–4.961 | 0.001 | 7.9% | 2.784 | 1.489–5.206 | 0.001 | 9% | 2.862 | 1.523–5.379 | 0.001 | 9.3% |
| Model 1—Univariate | Model 2—Adjusted for Age and Sex | Model 3—Adjusted for Age, Sex and BMI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-Hospital Mortality | OR | 95% CI | p Value | R2 | OR | 95% CI | p Value | R2 | OR | 95% CI | p Value | R2 |
| Age | 1.012 | 0.927–1.105 | 0.784 | 0.9% | ||||||||
| Male sex | 6.628 | 2.017–21.781 | 0.002 | 13.8% | ||||||||
| BMI | 1.083 | 0.958–1.223 | 0.201 | 2.1% | 1.102 | 0.956–1.271 | 0.182 | 15.3% | ||||
| Upper abdominal circumference | 0.975 | 0.946–1.003 | 0.086 | 3.9% | 0.953 | 0.914–0.994 | 0.025 | 23.1% | 0.95 | 0.913–0.989 | 0.013 | 25.2% |
| Total fat area | 0.746 | 0.496–1.119 | 0.158 | 2.7% | 0.579 | 0.342–0.982 | 0.043 | 19.8% | 0.578 | 0.336–0.993 | 0.047 | 21.2% |
| Subcutaneous fat area | 0.416 | 0.183–0.944 | 0.036 | 6.8% | 0.219 | 0.067–0.717 | 0.012 | 25.5% | 0.231 | 0.071–0.751 | 0.015 | 26.4% |
| Visceral fat area | 0.941 | 0.500–1.769 | 0.85 | 0.4% | 0.783 | 0.385–1.591 | 0.499 | 14.4% | 0.78 | 0.376–1.617 | 0.505 | 15.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheffler, M.; Genton, L.; Graf, C.E.; Remuinan, J.; Gold, G.; Zekry, D.; Serratrice, C.; Herrmann, F.R.; Mendes, A. Prognostic Role of Subcutaneous and Visceral Adiposity in Hospitalized Octogenarians with COVID-19. J. Clin. Med. 2021, 10, 5500. https://doi.org/10.3390/jcm10235500
Scheffler M, Genton L, Graf CE, Remuinan J, Gold G, Zekry D, Serratrice C, Herrmann FR, Mendes A. Prognostic Role of Subcutaneous and Visceral Adiposity in Hospitalized Octogenarians with COVID-19. Journal of Clinical Medicine. 2021; 10(23):5500. https://doi.org/10.3390/jcm10235500
Chicago/Turabian StyleScheffler, Max, Laurence Genton, Christophe E. Graf, Jorge Remuinan, Gabriel Gold, Dina Zekry, Christine Serratrice, François R. Herrmann, and Aline Mendes. 2021. "Prognostic Role of Subcutaneous and Visceral Adiposity in Hospitalized Octogenarians with COVID-19" Journal of Clinical Medicine 10, no. 23: 5500. https://doi.org/10.3390/jcm10235500