
Pneumothorax and/or Pneumomediastinum Worsens the Prognosis of COVID-19 Patients with Severe Acute Respiratory Failure: A Multicenter Retrospective Case-Control Study in the North-East of Italy

 , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcome Measures and Clinical Variables
2.3. Patients’ Management and Respiratory Support
2.4. Statistical Analysis
3. Results
3.1. Incidence and Clinical Characteristics of Patients
3.2. Assessment of Risks Factors
3.3. Assessment of Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABG | arterial blood gas analysis |
| ARDS | acute respiratory distress syndrome |
| COVID-19 | coronavirus disease 2019 |
| CRP | C-reactive protein |
| HFNC | heated humidified high-flow oxygen therapy |
| ICU | intensive care unit |
| IMCU | intermediate care unit |
| IV | invasive ventilation |
| FiO2 | fraction of inspired oxygen |
| PaO2 | arterial partial pressure of oxygen |
| PEEP | positive end-expiratory pressure |
| PNX | pneumothorax |
| PNM | pneumomediastinum |
| NLR | neutrophils to lymphocytes ratio |
| PS | pressure support |
| NIV | non-invasive ventilation |
| O2T | oxygen therapy |
| RA | room air |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
References
- Available online: https://covid19.who.int (accessed on 5 October 2021).
- Rivero, A.; Perez-Camacho, I.; Lozano, F.; Santos, J.; Camacho, A.; Serrano, A.; Cordero, E.; Jiménez, F.; Torres-Tortosa, M.; Torre-Cisneros, J. Andalusian Group for the Study of Infectious Diseases (GAEI). Etiology of spontaneous pneumothorax in 105 HIV-infected patients without highly active antiretroviral therapy. Eur. J. Radiol. 2009, 71, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Sihoe, A.D.; Wong, R.H.; Lee, A.T.; Lau, L.S.; Leung, N.Y.; Law, K.I.; Yim, A.P. Severe acute respiratory syndrome complicated by spontaneous pneumothorax. Chest 2004, 125, 2345–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, W.H.; Saha, B.K.; Hu, K.; Chopra, A. The incidence, clinical characteristics, and outcomes of pneumothorax in hospitalized COVID-19 patients: A systematic review. Heart Lung 2021, 50, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Al-Tarbsheh, A.H.; Shah, N.J.; Yaqoob, H.; Hu, K.; Feustel, P.J.; Ortiz-Pacheco, R.; Patel, K.M.; Oweis, J.; Kozlova, N.; et al. Pneumothorax in critically ill patients with COVID-19 infection: Incidence, clinical characteristics and outcomes in a case control multicenter study. Respir. Med. 2021, 184, 106464. [Google Scholar] [CrossRef] [PubMed]
- Lemmers, D.H.L.; Hilal, M.A.; Bnà, C.; Prezioso, C.; Cavallo, E.; Nencini, N.; Crisci, S.; Fusina, F.; Natalini, G. Pneumomediastinum and subcutaneous emphysema in COVID-19: Barotrauma or lung frailty? ERJ Open Res. 2020, 6, 00385–02020. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, A.W.; Ingle, T.; Newman, J.; Nadeem, I.; Jackson, K.; Lane, N.D.; Melhorn, J.; Davies, H.E.; Rostron, A.J.; Adeni, A. COVID-19 and pneumothorax: A multicentre retrospective case series. Eur. Respir. J. 2020, 56, 2002697. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, S.J.; Farrell, J.; Rostron, A.; Smith, I.; Openshaw, P.J.M.; Baillie, J.K.; Docherty, A.; Semple, M.G. COVID-19 Pneumothorax in the United Kingdom: A prospective observational study using the ISARIC WHO clinical characterisation protocol. Eur. Respir. J. 2021, 17, 2100929. [Google Scholar] [CrossRef] [PubMed]
- Miró, Ò.; Llorens, P.; Jiménez, S.; Piñera, P.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; García-Lamberetchs, E.J.; Jacob, J.; Alquézar-Arbé, A. Spanish Investigators on Emergency Situations Team (SIESTA) Network. Frequency, Risk Factors, Clinical Characteristics, and Outcomes of Spontaneous Pneumothorax in Patients with Coronavirus Disease 2019: A Case-Control, Emergency Medicine-Based Multicenter Study. Chest 2021, 159, 1241–1255. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, G.; Zhan, C.; Rosenberg, N. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation. Radiology 2020, 297, E252–E262. [Google Scholar] [CrossRef] [PubMed]
- The ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.aifa.gov.it/aggiornamento-sui-farmaci-utilizzabili-per-il-trattamento-della-malattia-covid19 (accessed on 22 May 2021).
- Available online: https://www.flipsnack.com/SIAARTI/siaarti_raccomandazioni_per_la_gestione_del_paziente_criti/full-view.html (accessed on 22 May 2021).
- Elsaaran, H.; AlQinai, S.; AlTarrah, D.; Abdulrasoul, M.; Al-Youha, S.; Almazeedi, S.; Al-Haddad, M.; Jamal, M.H.; Al-Sabah, S. Prevalence and risk factors of barotrauma in Covid-19 patients admitted to an intensive care unit in Kuwait; a retrospective cohort study. Ann. Med. Surg. 2021, 63, 102141. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, S.; Bilgi, D.Ö.; Köse, S.; Oya, G. Pneumothorax in patients with coronavirus disease 2019 pneumonia with invasive mechanical ventilation. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 351–355. [Google Scholar] [CrossRef]
- Greenberg, D.J.; Nabors, C.; Chandy, D.; Dhand, A. Pneumothorax and pneumomediastinum in patients hospitalized with coronavirus disease 2019 (COVID-19). Heart Lung 2021, 50, 386–387. [Google Scholar] [CrossRef]
- Elhakim, T.S.; Abdul, H.S.; Pelaez Romero, C.; Rodriguez-Fuentes, Y. Spontaneous pneumomediastinum, pneumothorax and subcutaneous emphysema in COVID-19 pneumonia: A rare case and literature review. BMJ Case Rep. 2020, 13, e239489. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Thiara, S.; Kanji, H.D.; Ronco, J.J. Spontaneous Pneumomediastinum in COVID-19: The Macklin Effect? Am. J. Respir. Crit. Care Med. 2021, 204, 989–990. [Google Scholar] [CrossRef] [PubMed]
- Triggle, C.R.; Bansal, D.; Ding, H.; Islam, M.M.; Farag, E.A.B.A.; Hadi, H.A.; Sultan, A.A. A Comprehensive Review of Viral Characteristics, Transmission, Pathophysiology, Immune Response, and Management of SARS-CoV-2 and COVID-19 as a Basis for Controlling the Pandemic. Front. Immunol. 2021, 12, 631139. [Google Scholar] [CrossRef] [PubMed]
- Alon, R.; Sportiello, M.; Kozlovski, S.; Kumar, A.; Reilly, E.C.; Zarbock, A.; Garbi, N.; Topham, D.J. Leukocyte trafficking to the lungs and beyond: Lessons from influenza for COVID-19. Nat. Rev. Immunol. 2021, 21, 49–64. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 with PNX/PNM n = 53 | COVID-19 w/o PNX/PNM n = 106 | p-Value | |
|---|---|---|---|
| Male, n (%) | 43 (81.1%) | 86 (81.1%) | n.s. |
| Age (y) | 69 [62–75] | 69 [62–75] | n.s. |
| Days to PNX/PNM occurrence | n.a. | ||
| From symptoms onset | 17 [12–23.5] | ||
| From hospital admission | 9 [4–16] | ||
| PNX + PNM, n (%) | 22 (41.5%) | n.a. | |
| PNX alone, n (%) | 18 (33.5%) | ||
| PNM alone, n (%) | 13 (24.5%) | ||
| Side of PNX, n (%) | |||
| Right | 21 (52.5%) | ||
| Left | 14 (35%) | ||
| Bilateral | 5 (12.5%) | ||
| Prevalence of subcutaneous emphysema, n (%) | 29 (54.7%) | n.a. | |
| Chest tube drainage treated, n (%) | 26 (49.1%) | n.a. | |
| Median RX resolution length (days) | 8 [5–13] | n.a. | |
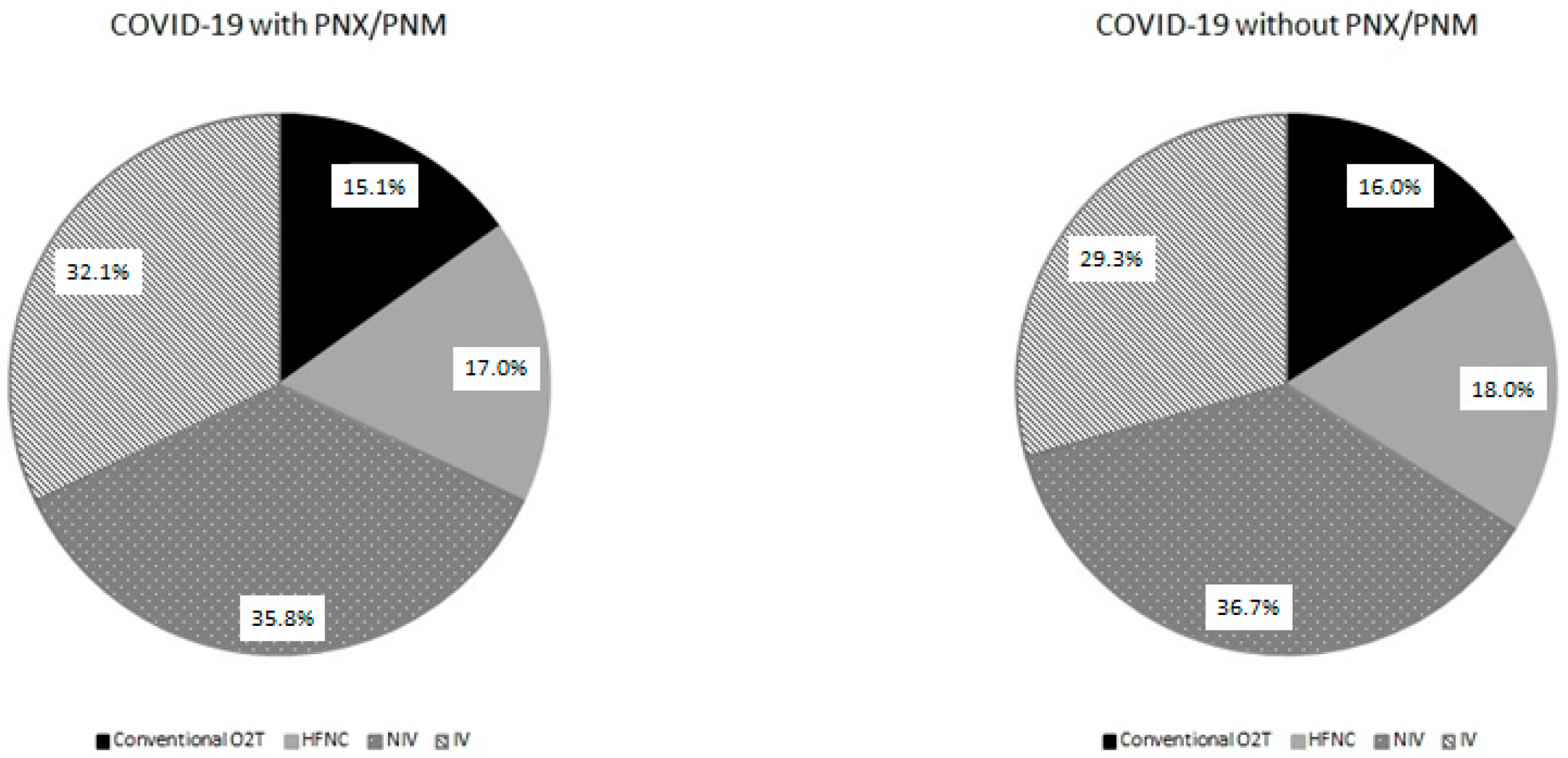
| Respiratory support, n (%) | |||
| Non-ventilated | 17 (32.1%) | 36 (34%) | |
| Conventional O2T | 8 (15.1%) | 17 (16%) | n.s. |
| HFNC | 9 (17%) | 19 (18%) | |
| Mechanically ventilated | 36 (67.9%) | 70 (66%) | |
| Non-invasively | 19 (35.8%) | 39 (36.7%) | |
| Invasively | 17 (32.1%) | 31 (29.3%) | |
| Endovenous steroid treatment | n.s. | ||
| Methylprednsiolone, n (%) | 35 (66.1%) | 76 (71.7%) | |
| Dexhametasone, n (%) | 18 (33.9%) | 30 (28.3%) | |
| Outcome | |||
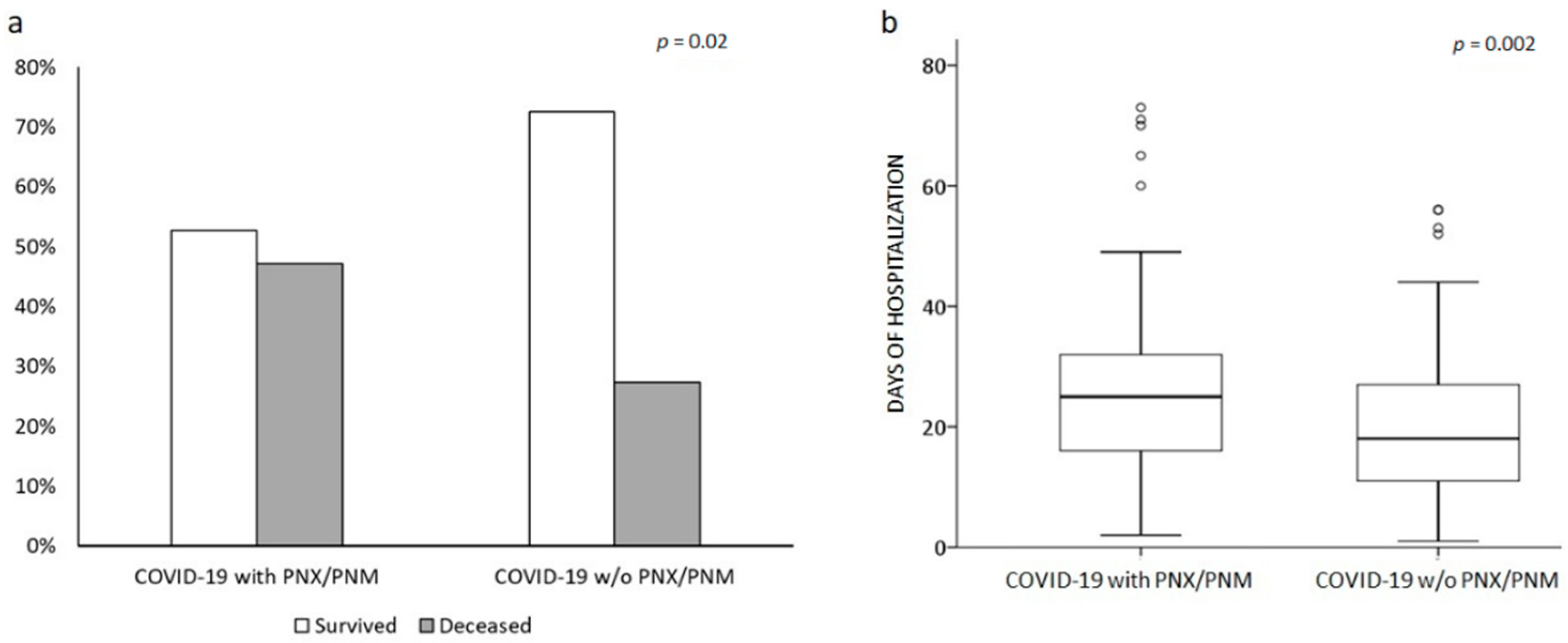
| Length of hospitalization in survived (days) | 25 [16–32.5] | 18 [10–27] | 0.002 |
| Deceased in-hospital, n (%) | 25 (47.2%) | 29 (27.4%) | 0.02 |
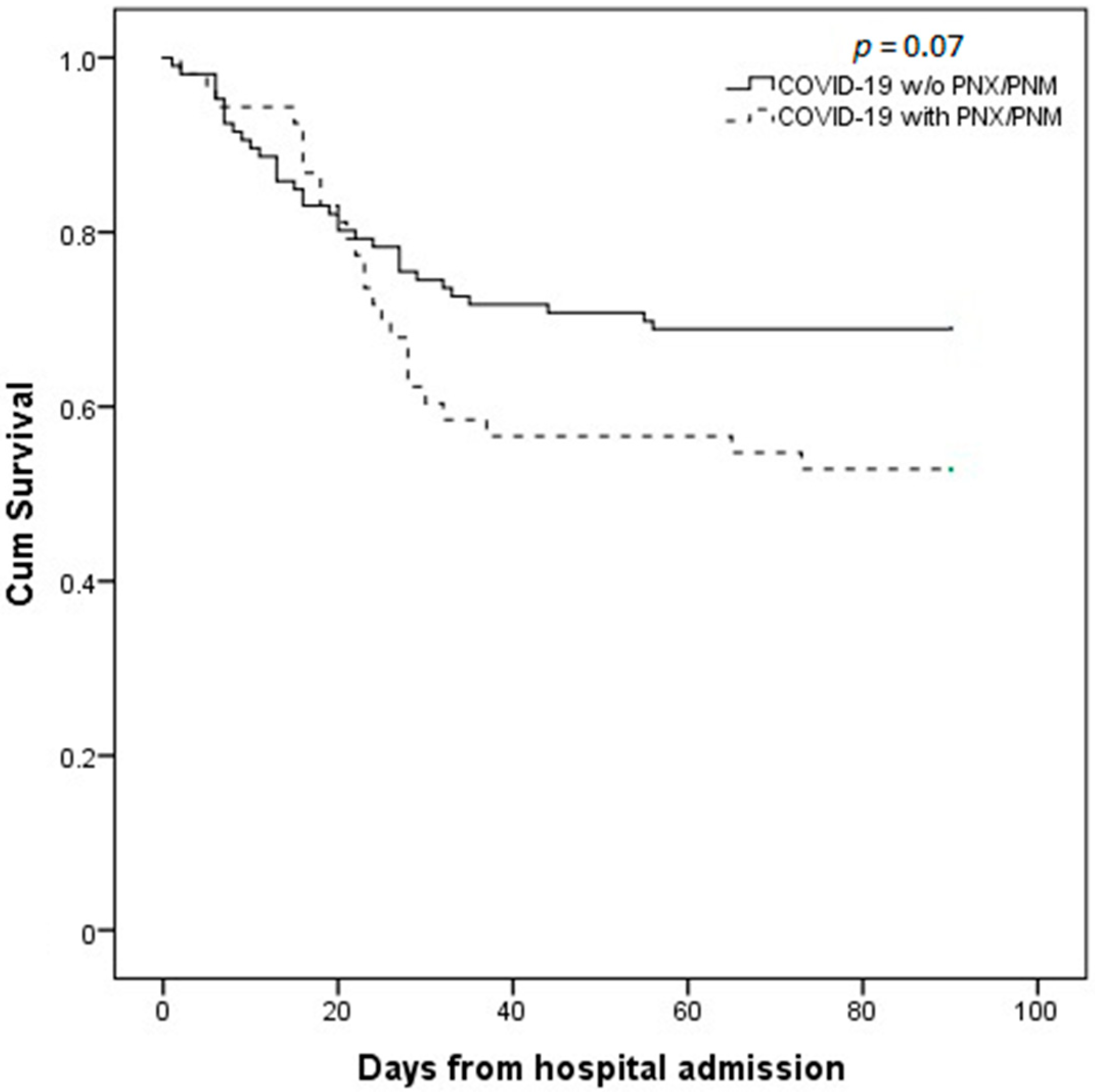
| Deceased at 90 days from admission, n (%) | 25 (47.2%) | 33 (31.1%) | 0.048 |
| COVID-19 with PNX/PNM n = 53 | COVID-19 w/o PNX/PNM n = 106 | p-Value | |
|---|---|---|---|
| Smoke habit, n (%) | |||
| Never | 30 (56.6%) | 54 (50.9%) | |
| Former | 19 (35.8%) | 43 (40.6%) | n.s. |
| Current | 4 (7.5%) | 9 (8.5%) | |
| Respiratory comorbidities, n (%) | |||
| Asthma | 3 (5.7%) | 3 (2.8%) | n.s. |
| COPD | 3 (5.7%) | 9 (8.5%) | n.s. |
| Chronic interstitial disease | 3 (5.1%) | 1 (0.9%) | n.s. |
| Other Comorbidities, n (%) | |||
| Hypertension | 25 (47.2%) | 61 (57.5%) | n.s. |
| Obesity | 6 (11.3%) | 22 (20.8%) | n.s. |
| Type 2 diabetes | 8 (15.1%) | 24 (22.6%) | n.s. |
| Dyslipidemia | 8 (15.1%) | 30 (28.3%) | n.s. |
| Chronic kidney disease | 2 (3.7%) | 6 (5%) | n.s. |
| Chronic heart disease | 10 (18.8%) | 14 (22.6%) | n.s. |
| Laboratory test on admission, n (%) | |||
| Platelets (×106 cell/mcL) | 216 [148–330] | 237 [181–330] | n.s. |
| n.v. 140,000–440,000 | |||
| Lymphocytes (cell/mcL) | 670 [465–860] | 760 [540–1100] | 0.017 |
| n.v. 1000–4500 | |||
| Neutrophils (cell/mcL) | 5910 [4670–8590] | 6060 [3790–8000] | n.s. |
| n.v. 1800–8000 | |||
| NL ratio | 9.7 [6.4–18.7] | 6.1 [4.2–12.8] | 0.028 |
| n.v. 1.8 | |||
| C-RP (mg/dL) | 9.7 [3.6–14.4] | 8.6 [4.1–19.1] | n.s. |
| n.v. <0.5 mg/dL | |||
| D-dimer (ng/mL) | 1216 [755–1966] | 856 [552–1561] | n.s. |
| n.v. <500 ng/dL | |||
| P/F ratio (mmHg) | 220 [132–291] | 174 [109–257] | n.s. |
| n.v. >400 mmHg | |||
| Days from symptoms onset to hospital admission | 7 [4.5–10] | 5 [2–8] | 0.005 |
| ARDS at admission, n (%) | 45 (84.9%) | 96 (90.5%) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonato, M.; Fraccaro, A.; Landini, N.; Zanardi, G.; Catino, C.; Savoia, F.; Malacchini, N.; Zeraj, F.; Peditto, P.; Catalanotti, V.; et al. Pneumothorax and/or Pneumomediastinum Worsens the Prognosis of COVID-19 Patients with Severe Acute Respiratory Failure: A Multicenter Retrospective Case-Control Study in the North-East of Italy. J. Clin. Med. 2021, 10, 4835. https://doi.org/10.3390/jcm10214835
Bonato M, Fraccaro A, Landini N, Zanardi G, Catino C, Savoia F, Malacchini N, Zeraj F, Peditto P, Catalanotti V, et al. Pneumothorax and/or Pneumomediastinum Worsens the Prognosis of COVID-19 Patients with Severe Acute Respiratory Failure: A Multicenter Retrospective Case-Control Study in the North-East of Italy. Journal of Clinical Medicine. 2021; 10(21):4835. https://doi.org/10.3390/jcm10214835
Chicago/Turabian StyleBonato, Matteo, Alessia Fraccaro, Nicholas Landini, Giuseppe Zanardi, Cosimo Catino, Francesca Savoia, Nicola Malacchini, Fabiola Zeraj, Piera Peditto, Vito Catalanotti, and et al. 2021. "Pneumothorax and/or Pneumomediastinum Worsens the Prognosis of COVID-19 Patients with Severe Acute Respiratory Failure: A Multicenter Retrospective Case-Control Study in the North-East of Italy" Journal of Clinical Medicine 10, no. 21: 4835. https://doi.org/10.3390/jcm10214835