
Immunogenicity of BNT162b2 mRNA-Based Vaccine against SARS-CoV-2 in People with Cystic Fibrosis According to Disease Characteristics and Maintenance Therapies

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shteinberg, M.; Haq, I.; Polineni, D.; Davies, J. Cystic fibrosis. Lancet 2021, 397, 2195–2211. [Google Scholar] [CrossRef]
- Carr, S.B.; Cosgriff, R.; Harutyunyan, S.; Middleton, P.G.; Ruseckaite, R.; Ahern, S.; Daneau, G.; Filho, L.V.R.F.d.S.; Stephenson, A.L.; Cheng, S.Y.; et al. COVID-19 vaccine prioritisation for people with cystic fibrosis. J. Cyst. Fibros. 2021, 20, 715–716. [Google Scholar] [CrossRef] [PubMed]
- Michos, A.; Filippatos, F.; Tatsi, E.B.; Dellis, C.; Efthymiou, V.; Zarkada, I.; Troupi, E.; Syriopoulou, V.; Loukou, I. Immunogenicity of the COVID-19 BNT162b2 vaccine in adolescents and young adults with cystic fibrosis. J. Cyst. Fibros. 2022, 21, e184–e187. [Google Scholar] [CrossRef] [PubMed]
- Launay, O.; Boelle, P.Y.; Krivine, A.; Grenet, D.; Boussaud, V.; Rémus, N.; Corvol, H.; Chedevergne, F.; Hubert, D.; Sermet-Gaudelus, I.; et al. Factors associated with humoral immune response to pandemic A/H1N1(v) 2009 influenza vaccine in cystic fibrosis. Vaccine 2014, 32, 4515–4521. [Google Scholar] [CrossRef] [PubMed]
- Bubien, J.K.; Kirk, K.L.; Rado, T.A.; Frizzell, R.A. Cell cycle dependence of chloride permeability in normal and cystic fibrosis lymphocytes. Science 1990, 248, 1416–1419. [Google Scholar] [CrossRef]
- Teichgräber, V.; Ulrich, M.; Endlich, N.; Riethmüller, J.; Wilker, B.; De Oliveira-Munding, C.C.; Van Heeckeren, A.M.; Barr, M.L.; Von Kürthy, G.; Schmid, K.W.; et al. Ceramide accumulation mediates inflammation, cell death and infection susceptibility in cystic fibrosis. Nat. Med. 2008, 14, 382–391. [Google Scholar] [CrossRef]
- Hartl, D.; Gaggar, A.; Bruscia, E.; Hector, A.; Marcos, V.; Jung, A.; Greene, C.; McElvaney, G.; Mall, M.; Döring, G. Innate immunity in cystic fibrosis lung disease. J. Cyst. Fibros. 2012, 11, 363–382. [Google Scholar] [CrossRef]
- Bruscia, E.M.; Bonfield, T.L. Innate and Adaptive Immunity in Cystic Fibrosis. Clin. Chest Med. 2016, 37, 17–29. [Google Scholar] [CrossRef]
- Lynn, D.J.; Benson, S.C.; Lynn, M.A.; Pulendran, B. Modulation of immune responses to vaccination by the microbiota: Implications and potential mechanisms. Nat. Rev. Immunol. 2022, 22, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Hagan, T.; Cortese, M.; Rouphael, N.; Boudreau, C.; Linde, C.; Maddur, M.S.; Das, J.; Wang, H.; Guthmiller, J.; Zheng, N.Y.; et al. Antibiotics-Driven Gut Microbiome Perturbation Alters Immunity to Vaccines in Humans. Cell 2019, 178, 1313–1328.e13. [Google Scholar] [CrossRef]
- Turck, D.; Braegger, C.P.; Colombo, C.; Declercq, D.; Morton, A.; Pancheva, R.; Robberecht, E.; Stern, M.; Strandvik, B.; Wolfe, S.; et al. ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children, and adults with cystic fibrosis. Clin. Nutr. 2016, 35, 557–577. [Google Scholar] [CrossRef] [PubMed]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Mileto, D.; Fenizia, C.; Cutrera, M.; Gagliardi, G.; Gigantiello, A.; De Silvestri, A.; Rizzo, A.; Mancon, A.; Bianchi, M.; De Poli, F.; et al. SARS-CoV-2 mRNA vaccine BNT162b2 triggers a consistent cross-variant humoral and cellular response. Emerg. Microbes Infect. 2021, 10, 2235–2243. [Google Scholar] [CrossRef] [PubMed]
- Moncunill, G.; Aguilar, R.; Ribes, M.; Ortega, N.; Rubio, R.; Salmerón, G.; Molina, M.J.; Vidal, M.; Barrios, D.; Mitchell, R.A.; et al. Determinants of early antibody responses to COVID-19 mRNA vaccines in a cohort of exposed and naïve healthcare workers. eBioMedicine 2022, 75, 103805. [Google Scholar] [CrossRef] [PubMed]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Meza-López, C.; Wang, L.F.; Sulbarán, A.C.M.; Torres-Hernández, P.C.; Bedolla-Barajas, M.; De la O-Gómez, B.; Balcázar-Félix, P.; Hernández-Bello, J. Neutralizing antibodies titers and side effects in response to bnt162b2 vaccine in healthcare workers with and without prior SARS-CoV-2 infection. Vaccines 2021, 9, 742. [Google Scholar] [CrossRef]
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High antibody response to two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef]
- Di Noia, V.; Pimpinelli, F.; Renna, D.; Barberi, V.; Pellini, R.; Morrone, A.; Giannarelli, D.; Cognetti, F. Clinical characteristics limiting the durability of humoral response to BNT162b2 in patients with solid cancer. Ann. Oncol. 2021, 33, 350–352. [Google Scholar] [CrossRef]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef]
- Singanayagam, A.; Glanville, N.; Girkin, J.L.; Ching, Y.M.; Marcellini, A.; Porter, J.D.; Toussaint, M.; Walton, R.P.; Finney, L.J.; Aniscenko, J.; et al. Corticosteroid suppression of antiviral immunity increases bacterial loads and mucus production in COPD exacerbations. Nat. Commun. 2018, 9, 2229. [Google Scholar] [CrossRef]
- Lee, C.; Klaustermeyer, W.B. Effect of high dose inhaled corticosteroids on cell mediated immunity in patients with asthma. Allergol. Immunopathol. 2012, 40, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Zalkinder, I.; Kuperman, O.; Skibin, A.; Apte, R.; Bearman, J.E.; Mielke, P.W.; Tal, A. Effect of prolonged use of inhaled steroids on the cellular immunity of children with asthma. J. Allergy Clin. Immunol. 1995, 95, 806–812. [Google Scholar] [CrossRef]
- Hanania, N.A.; Sockrider, M.; Castro, M.; Holbrook, J.T.; Tonascia, J.; Wise, R.; Atmar, R.L. Immune response to influenza vaccination in children and adults with asthma: Effect of corticosteroid therapy. J. Allergy Clin. Immunol. 2004, 113, 717–724. [Google Scholar] [CrossRef] [PubMed]
- De Roux, A.; Marx, A.; Burkhardt, O.; Schweiger, B.; Borkowski, A.; Banzhoff, A.; Pletz, M.W.R.; Lode, H. Impact of corticosteroids on the immune response to a MF59-adjuvanted influenza vaccine in elderly COPD-patients. Vaccine 2006, 24, 1537–1542. [Google Scholar] [CrossRef] [PubMed]
- Coggins, S.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse Effects and Antibody Titers in Response to the BNT162b2 mRNA COVID-19 Vaccine in a Prospective Study of Healthcare Workers. Open Forum Infect. Dis. 2022, 9, ofab575. [Google Scholar] [CrossRef] [PubMed]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef]
- Kim, W.; Zhou, J.Q.; Horvath, S.C.; Schmitz, A.J.; Sturtz, A.J.; Lei, T.; Liu, Z.; Kalaidina, E.; Thapa, M.; Alsoussi, W.B.; et al. Germinal centre-driven maturation of B cell response to mRNA vaccination. Nature 2022, 604, 141–145. [Google Scholar] [CrossRef]
- Hartley, G.E.; Edwards, E.S.J.; Aui, P.M.; Varese, N.; Stojanovic, S.; McMahon, J.; Peleg, A.Y.; Boo, I.; Drummer, H.E.; Hogarth, P.M.; et al. Rapid generation of durable B cell memory to SARS-CoV-2 spike and nucleocapsid proteins in COVID-19 and convalescence. Sci. Immunol. 2020, 5, eabf8891. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef]
- Cele, S.; Jackson, L.; Khoury, D.S.; Khan, K.; Moyo-Gwete, T.; Tegally, H.; San, J.E.; Cromer, D.; Scheepers, C.; Amoako, D.; et al. SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. MedRxiv 2021. [Google Scholar] [CrossRef]
- Cao, Y.; Wang, J.; Jian, F.; Xiao, T.; Song, W.; Yisimayi, A.; Huang, W.; Li, Q.; Wang, P.; An, R.; et al. Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies. Nature 2021, 602, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Keeton, R.; Tincho, M.B.; Ngomti, A.; Baguma, R.; Benede, N.; Suzuki, A.; Khan, K.; Cele, S.; Bernstein, M.; Karim, F.; et al. T cell responses to SARS-CoV-2 spike cross-recognize Omicron. Nature 2022, 603, 488–492. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Number of patients | 143 (100) |
| Male sex | 75 (52.4) |
| Age | |
| Median (IQR) | 21 (18–25) |
| Adults | 123 (86.0) |
| Age group: 13–17 years | 20 (14.0) |
| Age group: 18–29 years | 107 (74.8) |
| Age group: 30–38 years | 16 (11.2) |
| Pancreatic insufficiency | 80 (55.9) |
| P. aeruginosa infection | 57 (39.9) |
| BMI, kg/m2, median (IQR) a | 22.4 (20.1; 24.4) |
| BMI, z-score, median (IQR) a,b | 0.10 (−0.55; 0.81)) |
| Underweight a,c | 8 (5.6) |
| ppFEV1 d | |
| Median (IQR) | 97 (82–106) |
| ≥80% | 107 (75.9) |
| 40–79% | 33 (23.4) |
| <40% | 1 (0.7) |
| Maintenance therapies | |
| Inhaled antibiotics | 24 (16.8) |
| Systemic antibiotics | 39 (27.3) |
| Azithromycin | 51 (35.7) |
| Inhaled corticosteroids | 65 (45.5) |
| Systemic corticosteroids | 3 (2.1) |
| CFTR modulators e | 36 (25.2) |
| Oxygen therapy | 1 (0.7) |
| Prior SARS-CoV-2 infection | |
| Yes | 16 |
| RT-PCR confirmed infection | 1 |
| Symptomatic infection | 1 |
| Unknown | 4 |
| Adverse reactions after the first or second dose of the BNT162b2 vaccine | |
| None | 7 (4.9) |
| Local | 128 (89.5) |
| Systemic | 103 (72.0) |
| Mild | 71 (49.7) |
| Moderate | 57 (39.9) |
| Severe | 0 |
| Group | No. | 3 Months from Second Dose | 6 Months from Second Dose | p-Value for the Main Effect a | p-Value for the Interaction with Time a |
|---|---|---|---|---|---|
| Sex | 0.494 | 0.694 | |||
| Males | 62 | 1174 (973–1417) | 829 (680–1010) | ||
| Females | 61 | 1063 (892–1267) | 764 (634–921) | ||
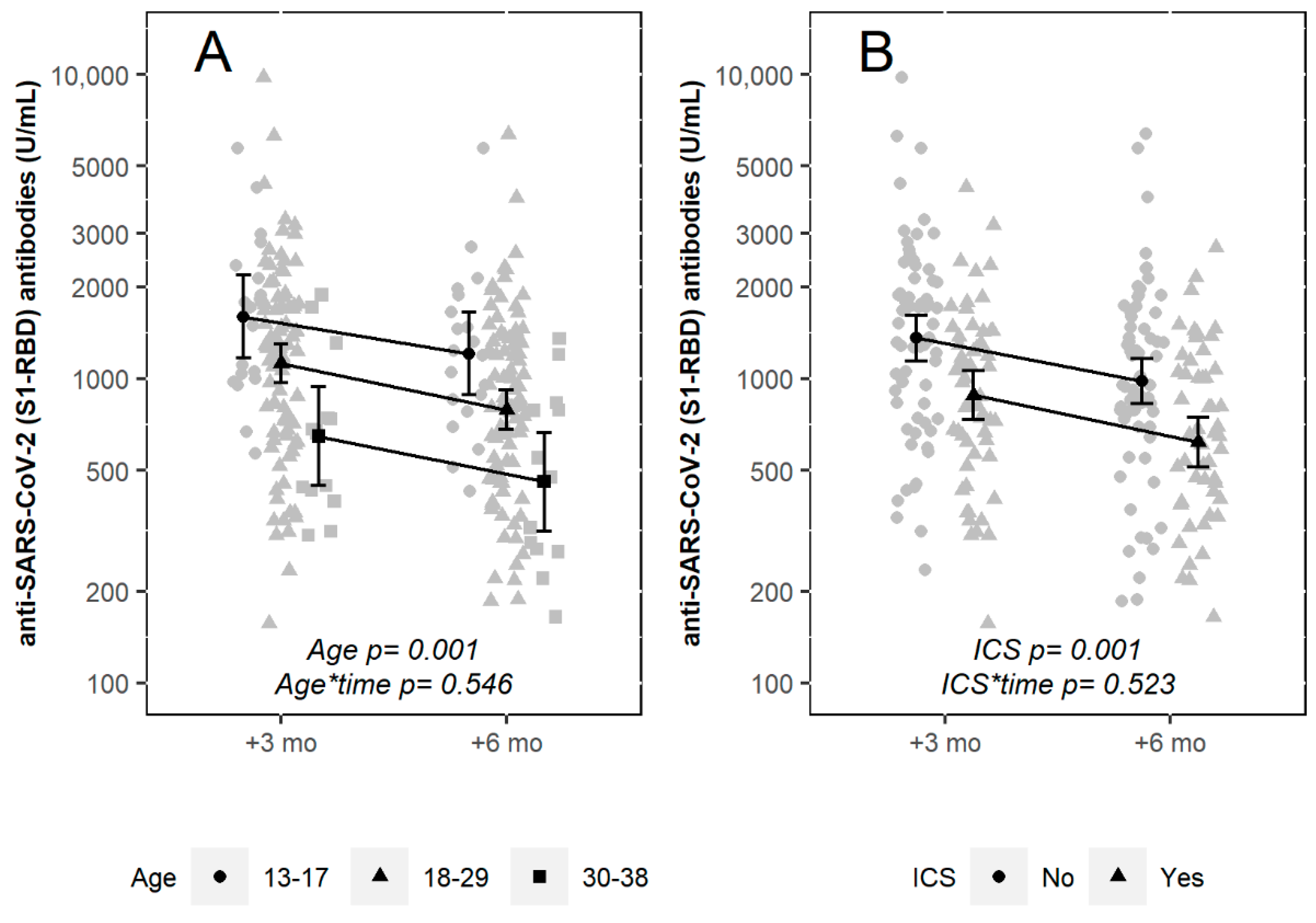
| Age group | 0.001 | 0.546 | |||
| 13–17 years | 20 | 1600 (1235–2074) | 1209 (924–1581) | ||
| 17–29 years | 89 | 1123 (965–1307) | 790 (675–926) | ||
| 29–38 years | 14 | 647 (477–878) | 458 (325–647) | ||
| Pancreatic insufficiency | <0.0001 | 0.035 | |||
| No | 51 | 1561 (1313–1857) | 1049 (880–1250) | ||
| Yes | 72 | 882 (750–1036) | 655 (545–786) | ||
| Underweight b | 0.411 | 0.555 | |||
| No | 114 | 1095 (956–1253) | 776 (673–896) | ||
| Yes | 8 | 1324 (900–1950) | 994 (722–1370) | ||
| P. aeruginosa infection | 0.001 | 0.178 | |||
| No | 72 | 1354 (1153–1592) | 940 (795–1111) | ||
| Yes | 51 | 852 (706–1028) | 630 (509–778) | ||
| Inhaled antibiotics | 0.155 | 0.389 | |||
| No | 101 | 1175 (1018–1356) | 829 (715–961) | ||
| Yes | 22 | 888 (676–1166) | 661 (473–922) | ||
| Systemic antibiotics | 0.004 | 0.409 | |||
| No | 87 | 1272 (1096–1475) | 895 (766–1045) | ||
| Yes | 36 | 818 (653–1023) | 600 (467–772) | ||
| Azithromycin | 0.057 | 0.073 | |||
| No | 77 | 1239 (1049–1464) | 854 (716–1018) | ||
| Yes | 46 | 939 (774–1140) | 707 (574–872) | ||
| Inhaled corticosteroids | 0.001 | 0.538 | |||
| No | 67 | 1360 (1143–1618) | 983 (825–1170) | ||
| Yes | 56 | 883 (743–1050) | 619 (510–751) | ||
| CFTR modulators | 0.005 | 0.16 | |||
| No | 89 | 1266 (1088–1471) | 883 (756–1033) | ||
| Yes | 34 | 807 (652–998) | 606 (471–779) |
| Potential Determinant of Antibody Response | β Coefficients a | 95% CI | p-Value b |
|---|---|---|---|
| Intercept | 3.368 | (3.231 to 3.505) | |
| Age group:18–29 vs. 13–17 | −0.142 | (−0.283 to −0.002) | 0.047 |
| Age group: 30–38 vs. 13–17 | −0.354 | (−0.552 to −0.157) | <0.001 |
| PI vs. PS | −0.089 | (−0.215 to 0.037) | 0.165 |
| Pa infection (Yes vs. No) | −0.081 | (−0.200 to 0.037) | 0.177 |
| SAB (Yes vs. No) | −0.068 | (−0.188 to 0.052) | 0.267 |
| ICS (Yes vs. No) | −0.121 | (−0.225 to −0.018) | 0.022 |
| CFTRmod (Yes vs. No) | −0.046 | (−0.169 to 0.078) | 0.469 |
| Prior infection by SARS-CoV-2 (Yes vs. No) | 0.704 | (0.552 to 0.857) | <0.001 |
| Time from second injection: 6 vs. 3 months | −0.153 | (−0.172 to −0.133) | <0.001 |
| Group | No. | 3 Months from Second Dose | 6 Months from Second Dose | p-Value for the Main Effect a | p-Value for the Interaction with Time a |
|---|---|---|---|---|---|
| Severity of adverse reactions | 0.526 | 0.576 | |||
| None/Mild | 71 | 1165 (974–1392) | 820 (678–993) | ||
| Moderate | 52 | 1056 (880–1268) | 764 (633–922) | ||
| Systemic reactions | 0.819 | 0.226 | |||
| No | 32 | 1119 (856–1463) | 836 (623–1123) | ||
| Yes | 91 | 1117 (964–1293) | 782 (672–911) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alicandro, G.; Daccò, V.; Cariani, L.; Rosazza, C.; Sciarrabba, C.S.; Ferraro, F.; Lanfranchi, C.; Medino, P.; Girelli, D.; Colombo, C. Immunogenicity of BNT162b2 mRNA-Based Vaccine against SARS-CoV-2 in People with Cystic Fibrosis According to Disease Characteristics and Maintenance Therapies. Biomedicines 2022, 10, 1998. https://doi.org/10.3390/biomedicines10081998
Alicandro G, Daccò V, Cariani L, Rosazza C, Sciarrabba CS, Ferraro F, Lanfranchi C, Medino P, Girelli D, Colombo C. Immunogenicity of BNT162b2 mRNA-Based Vaccine against SARS-CoV-2 in People with Cystic Fibrosis According to Disease Characteristics and Maintenance Therapies. Biomedicines. 2022; 10(8):1998. https://doi.org/10.3390/biomedicines10081998
Chicago/Turabian StyleAlicandro, Gianfranco, Valeria Daccò, Lisa Cariani, Chiara Rosazza, Calogero Sathya Sciarrabba, Federica Ferraro, Chiara Lanfranchi, Paola Medino, Daniela Girelli, and Carla Colombo. 2022. "Immunogenicity of BNT162b2 mRNA-Based Vaccine against SARS-CoV-2 in People with Cystic Fibrosis According to Disease Characteristics and Maintenance Therapies" Biomedicines 10, no. 8: 1998. https://doi.org/10.3390/biomedicines10081998