
Updated Clinical Evaluation of the CLUNGENE® Rapid COVID-19 Antibody Test
by
 ,
,
Christopher C. Lamb
1,2,3,* ,
,
Fadi Haddad
4,5,6, 
Christopher Owens
7,
Alfredo Lopez-Yunez
7,
Marion Carroll
8 and
Jordan Moncrieffe
8 1
Weatherhead School of Management, Case Western Reserve University, 10900 Euclid Ave., Cleveland, OH 44106, USA
2
Silberman College of Business, Fairleigh Dickinson University, 1000 River Rd., Teaneck, NJ 07666, USA
3
BioSolutions Services LLC, 92 Irving Avenue, Englewood Cliffs, NJ 07632, USA
4
Fellow of the Infectious Disease Society of America (IDSA), 4040 Wilson Boulevard, Suite 300, Arlington, VA 22203, USA
5
Fadi Haddad, MD, Inc., 8860 Center Dr. Suite 320, La Mesa, CA 91942, USA
6
Sharp Grossmont Hospital, 5555 Grossmont Center Dr., La Mesa, CA 91942, USA
7
Alivio Medical Center, Indianapolis, IN 46219, USA
8
MedComp Sciences, LLC, 20503 MacHost Road, Zachary, LA 70791, USA
*
Author to whom correspondence should be addressed.
Healthcare 2021, 9(9), 1124; https://doi.org/10.3390/healthcare9091124
Submission received: 30 June 2021
/
Revised: 29 July 2021
/
Accepted: 11 August 2021
/
Published: 30 August 2021
(This article belongs to the Special Issue Novel Coronavirus (SARS-CoV-2) Outbreak: Epidemiology, Research and Implications for Public Health)
Abstract
:Background: COVID-19 antibody testing has been shown to be predictive of prior COVID-19 infection and an effective testing tool. The CLUNGENE® SARS-COV-2 VIRUS (COVID-19) IgG/IgM Rapid Test Cassette was evaluated for its utility to aide healthcare professionals. Method: Two studies were performed by using the CLUNGENE® Rapid Test. (1) An expanded Point-of-Care (POC) study at two clinical sites was conducted to evaluate 99 clinical subjects: 62 positive subjects and 37 negative subjects were compared to RT-PCR, PPA, and NPA (95% CI). Sensitivity was calculated from blood-collection time following symptom onset. (2) A cross-reactivity study was performed to determine the potential for false-positive results from other common infections. Results: The specificity of subjects with confirmed negative COVID-19 by RT-PCR was 100% (95% CI, 88.4–100.0%). The sensitivity of subjects with confirmed positive COVID-19 by RT-PCR was 96.77% (95% CI, 88.98–99.11%). In the cross-reactivity study, there were no false-positive results due to past infections or vaccinations unrelated to the SARS-CoV-2 virus. Conclusion: There is a need for a rapid, user-friendly, and inexpensive on-site monitoring system for diagnosis. The CLUNGENE® Rapid Test is a useful diagnostic test that provides results within 15 min, without high-complexity laboratory instrumentation.
1. Introduction
The COVID-19 pandemic SARS-CoV2 COVID-19 has infected over 140 million people worldwide and has caused approximately 3.89 million deaths as of 23 June 2021 [1]; however, some studies suggest that the actual number of global COVID-19 deaths may be about 6.9 million, which is more than double the recorded amount [2,3,4]. In response to the pandemic, the US Food and Drug Administration (FDA) authorized the use of COVID-19 serological tests through Emergency Use Authorizations (EUAs) to make COVID-19 in vitro diagnostic tests widely available to help identify individuals with an adaptive immune response indicating recent or prior infection [5]. Serology tests, or immunoassays, play a significant role in the fight against COVID-19 [6,7]. A prior history of SARS-CoV-2 infection is associated with a lower risk of infection, with an estimated protective effect of up to seven (7) months following primary infection; this supports the conclusion that convalescent plasma with specific antibodies to SARS-CoV-2 has powerful antiviral activity, which can reduce the viral load and mortality in patients with active COVID-19 infection [8,9,10].
There is an urgent need for a rapid, user-friendly, and inexpensive on-site monitoring system for diagnosis [11]. The CLUNGENE® SARS-COV-2 VIRUS (COVID-19) IgG/IgM Rapid (15 min) Test Cassette has been commercially available in the US under an FDA-approved Emergency Use Authorization (EUA201121) [12] and Europe (CE Mark reference 02PBJ267 dated 9 March 2020). The CLUNGENE® test has been previously studied, including the use of the test in the offices of general practitioners, evaluating the presence of antibodies in convalescent plasma donors, and how the test performs at a point of care facility [13,14,15]. The aim of this research was to better understand the sensitivity and specificity of the CLUNGENE® assay and the potential for false-positive results related to infections or vaccinations not linked to the SARS-CoV-2 virus.
2. Materials and Methods
2.1. Study #1
2.1.1. Design
In an initial study, a single Point-of-Care (POC) facility was used to estimate the sensitivity and specificity of the CLUNGENE® test [16]. The study was expanded to a second independent site. The two sites were Sharp Healthcare, a not-for-profit multi-center regional healthcare group located in San Diego, CA; and Alivio Medical Center, an urgent care/primary care center in Indianapolis, IN. Samples used for RT-PCR were nares swabs. Positive subjects were symptomatic for SAR-CoV-2 Virus infected and confirmed with RT-PCR positive tested nares swabs. Negative subjects were asymptomatic, from high-risk areas, and confirmed with negative RT-PCR tested nares swabs. Finger-prick whole-blood samples were used for SARS-COV-2 Virus IgG/IgM detection. The comparator method for RT-PCR was either Cobas Roche SARS-COV2 RT-PCR (Roche Diagnostics, 9115 Hague Road PO Box 50457, Indianapolis, IN 46250) or Thermo Fisher TaqPath COVID-19 Combo Kit (Thermo Fisher Scientific, 168 3rd Ave, Waltham, MA 02451, USA). Trained operators with no prior information about each subject drew samples. Subject inclusion criteria included individuals with a confirmed COVID-19 test result by SARS-CoV-2 RT-PCR. Subjects were excluded if they were unable to provide informed consent due to mental or cognitive disabilities.
2.1.2. Methods
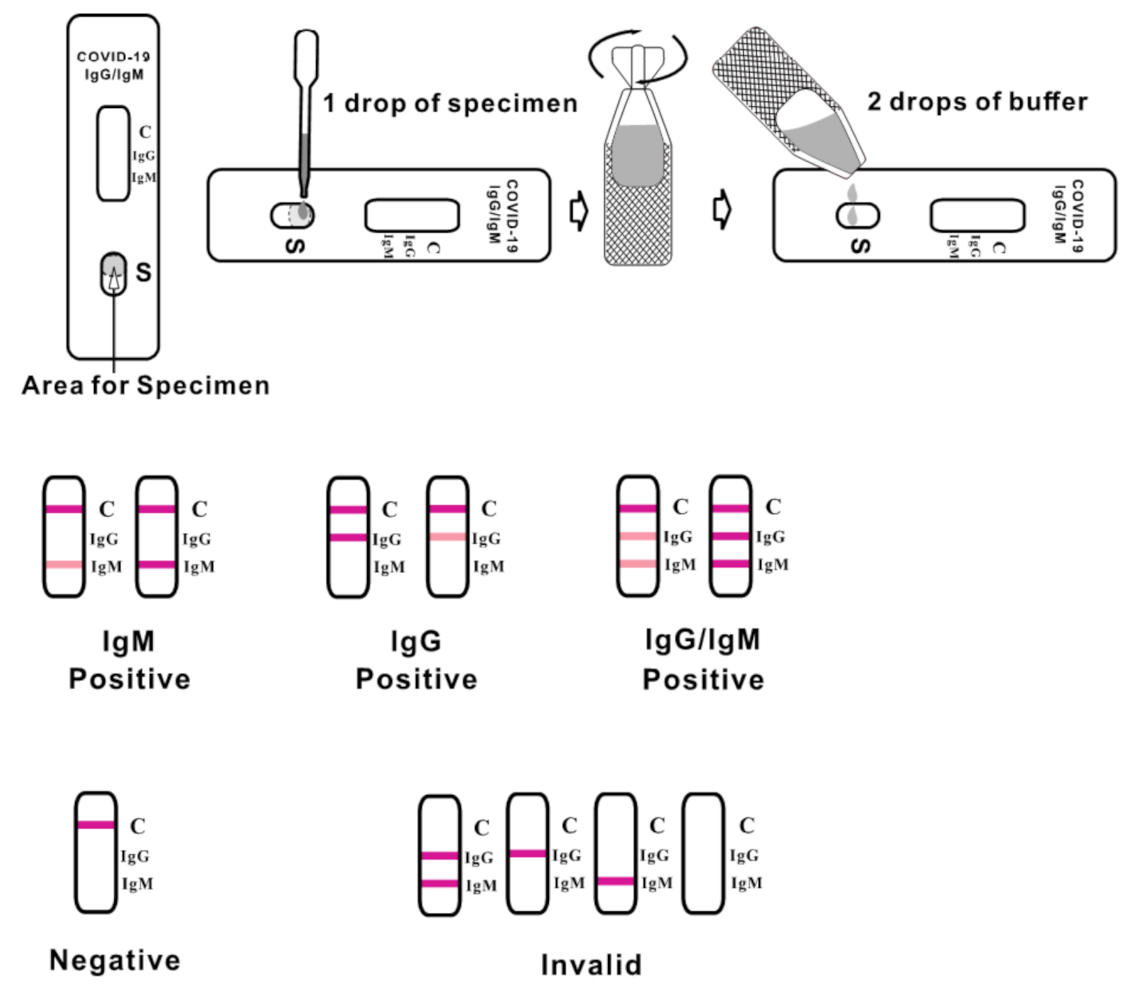
The CLUNGENE® Point-of-Care test was run according to the manufacturer’s instructions (see Figure 1). The test result was read after 15 min. Days from symptom onset were captured from an electronic medical record which documented self-reported data from patients reporting on the number of days they had been sick at the time of study enrollment.
Categorical variables were compared using the chi-squared or Fisher exact test, and continuous variables were compared using the Student t-test or Mann-Whitney U test, as appropriate. All tests were two tailed, and p < 0.05 was considered statistically significant. SPSS Statistics, IBM SPSS software, version 27.0 (SPSS, Inc., Chicago, IL, USA) was used for all calculations.
The CLUNGENE® test can be stored at ambient temperature between 4 and 30 degrees Celsius. The product is packaged in a box with 25 test kits, with each kit wrapped in an individual foil patch for proper storage and transportation. The test kit itself should be kept away from direct sunlight.
2.2. Study #2
2.2.1. Design
An initial cross-reactivity study was performed in which various common infectious agents were tested for potential false-positive results (Table 1). All tests were negative. In addition, as recommended by the US Food and Drug Administration [17], a follow-up study tested the cross-reactivity of the CLUNGENE® device to antibodies to common coronaviruses that are not SARS-CoV-2: anti-229E, anti-NL63, anti-OC43, and anti-HKU1; and those for which there is a high rate of vaccinations and/or infection in the US, i.e., anti-Haemophilus influenzae IgG and IgM. The testing was performed at Medcomp Sciences, an independent clinical medical laboratory [18].
2.2.2. Methods
The CLUNGENE® Point-of-Care test was run according to same manufacturer’s instructions as was performed with Study #1. Samples (50) used for the cross-reactivity study were obtained from Trina Bioreactives, Ag; Trina Bioreactives, Ag, (Grabenstrasse 8, 8606 Nänikon, Switzerland) is an ISO certified company providing specialized Sars-COV-2 in vitro diagnostic biomaterials [19]. The samples were collected under a protocol approved by the ethics committee of the National Medical Association, Baden-Wurttemburg, Germany (file #F-2012-027, “Plasma Samples for Studies”).
Test results were read after 15 min. Five (5) serum samples that were positive for IgM and five for IgG were analyzed in three (3) separate CLUNGENE® Point-of-Care test lots with each of the below antibodies:
- Anti-Haemophilus influenzae IgM,
- Anti-Haemophilus influenzae IgG,
- IgG, anti-coronavirus 229E IgG,
- Anti-coronavirus NL63 IgG,
- Anti-coronavirus OC43 IgG,
- Anti-coronavirus HKU1 IgG,
- Anti-coronavirus 229E IgM,
- Anti-coronavirus NL63 IgM,
- Anti-coronavirus OC43 IgM,
- Anti-coronavirus HKU1 IgM.
Cross-reactivity was determined by using Beckman Coulter UniCel DxI Access Immunoassay System is an in vitro diagnostic device used for the quantitative, semi-quantitative, or qualitative determination of various analyte concentrations found in human body fluids (Table 2).
All QC materials were supplied and used as indicated by the manufacturer. A minimum of 2 levels of QC were processed per run in accordance with Westgard rules for 6-sigma quality requirements. QC results must fall within 3 standard deviations of historical data, as recorded in Levy–Jennings plots by the system. All QC results were documented and verified by Clinical Laboratory Scientist before processing samples (Table 3).
Qualitative results are reported as Positive/Reactive or Negative/Non-Reactive, depending on whether the analyte in question is above or below the established signal cutoff value (S/CO). Each analyte tested may have a different cutoff value, but each cutoff value is determined during calibration of the instrument, using the value of the calibrator.
3. Results
3.1. Results of Study #1
An analysis was run on 99 patients who completed the study (Table 4).
Thirty-seven (37) patients who had negative COVID-19 RT-PCR were tested and found antibody negative by using the CLUNGENE® test (95% CI, 90.60~100.00%). Three (3) out of four (4), or 75%, of RT-PCR positive COVID-19 subjects tested prior to day 7 of symptom onset were antibody positive (95% CI, 30.06~95.44%). Twenty-three (23), or 100%, of RT-PCR positive COVID-19 subjects tested positive between day 8 and 14 from symptom onset (95% CI, 85.69~100.00%). A total of 33 out of 35, or 94.28%, of RT-PCR positive COVID-19 subjects tested positive after day 14 from symptom onset were antibody positive (95% CI, 30.06~95.44%). In all 62 patients with confirmed COVID-19 with RT-PCR, the combined sensitivity of IgM and IgG was 96.77% (95% CI, 88.98–99.11%), meaning that there was 96.77 positive agreement between a positive RT-PCR test and a positive antibody test. The specificity was 100% (95% CI, 88.4–100.0%), meaning there was 100% agreement between a negative RT-PCR test and 100% negative antibody result. These results are displayed in Table 5.
The positive predictive value can be calculated, but the result is dependent on the prevalence of disease in the community. If a test for a disease has 96.77% sensitivity and 100% specificity, and the disease prevalence is 10%, the positive predictive value (PPV) is 100%, and the negative predictive value (NPV) is 99.64%. At the time of this publication, the positivity rate for the nares SARS CoV2 RT-PCR tests was between 8.2% and 10% in San Diego, CA (San Diego County), and Indianapolis, IN (Marion Country) [20].
3.2. Results of Study #2
The test results of negative quality-control samples were all negative, and the test results of the positive quality-control samples were all positive. The consistency rate of cross-reactivity of negative samples was 100%.
4. Discussion
In the first study, the performance characteristics of CLUNGENE® were evaluated and showed a specificity of 100% and a sensitivity of 96.77%. In the second study, there were no false-positive results due to past infections or vaccinations unrelated to the SARS-CoV-2 virus. These results are in line with the new European Commission’s Medical Device Coordination Group requirements for rapid COVID-19 antibody tests and consistent with previously published results [21,22,23,24,25].
Antibody testing is a useful aid to confirm past infection [26]. Recent findings confirm that antibody testing is predictive of prior COVID-19 infection, and rapid screening methods—even from finger pricks—are effective testing tools [27]. However, we see the potential for a much broader use and recommend a combined approach that uses both RT-PCR and serological testing. The advantage of the CLUNGENE® antibody test is its simplicity, since there is no need for specialized laboratory personnel to perform and interpret results. The low rate of false positivity makes this test ideal to rule in disease and eliminate the need for further RT-PCR testing if seroconversion occurs, since the CLUNGENE® antibody test can diagnose most infected COVID-19 patients. If the test is negative, a recommendation should be made to have a follow-up RT-PCR test.
Serology testing also has the potential to monitor the presence of antibodies. Studies confirm that a prior history of SARS-CoV-2 infection is associated with a lower risk of infection, with an estimated seven (7) month protective effect [9,10]. The association of SARS-CoV-2 Seropositive Antibody Test with Risk of Future Infection has now been established [28]. It is clear that titers of IgM and IgG antibodies against the receptor-binding domain (RBD) of the spike protein of SARS-CoV-2 decrease significantly between one (1) and seven (7) months, and concurrently, neutralizing activity decreases [29]. Monitoring the presence of antibodies from past infection could assist healthcare professionals in assessing the likely presence of neutralizing activity and immunity when managing patient care.
Given widespread availability, COVID-19 serology testing, similar to other infectious diseases, can now become routine [30]. Consideration should be given to adding COVID-19 antibody testing to the WHO List of Essential In Vitro Diagnostics (EDL), which now consists of 122 test categories, including most serious infectious diseases [31]. A rapid 15-min COVID-19 assay offers the ability to do this testing quickly and efficiently—tests are now available for less than $5 and routinely reimbursed in the US by public and private insurers [5].
In addition, the ability of the CLUNGENE® antibody test to detect antibodies to the coronavirus’s spike protein’s receptor binding domain means it has the potential to assess the efficacy of most vaccines, as well as convalescent plasma therapy [32]. Countries in Europe are now using antibody testing to determine if a second COVID-19 vaccine dose is required if a patient has a prior infection based on a positive antibody test [33]. Recently, airports and Blood Banks have been providing COVID-19 antibody testing services to determine whether a person has developed immunity to COVID-19 through vaccination or through contracting the virus previously [34,35]. Some countries, including China, require an antibody test. Limited evaluation of the CLUNGENE® antibody test has confirmed positive antibody test results following patients who have been vaccinated [36]. Pfizer’s recent data suggest that its vaccine is efficacious for only 6 months and that a third shot within 12 months is likely needed [37]. Furthermore, there is a potential issue regarding vaccine efficacy for recipients who do not receive a full dose; the US CDC estimates that 3% of vaccinated people who received a first dose did not receive a recommended second dose [38]. COVID-19 vaccination also fails to stimulate an immune response in many blood-cancer patients or those otherwise immunocompromised [39,40]. Additional studies are needed to confirm the efficacy of serology testing to monitor vaccine effectiveness.
Limitations
Limitations of the study include a small sample size from two geographic areas. The study also did not include special groups, such as pregnant women or children. The subjectivity of symptom reporting by patients can be a confounding factor in determining the duration of illness. Some patients may have been symptomatic for a different time period than they recalled. Lastly, the CLUNGENE® antibody test has not been compared with another test in the study.
5. Conclusions
In a pandemic crisis with significant economic and health implications, this study confirms the utility of serological testing for COVID-19 disease diagnosis providing rapid test results with a relatively high degree of sensitivity and specificity. Furthermore, given recent data regarding the relationship between positive serology and immunity, routine testing can be a useful tool to monitor antibody status for optimal patient care. Tests such as the CLUNGENE® SARS-COV-2 VIRUS (COVID-19) IgG/IgM Rapid Test Cassette can assist healthcare professionals to help identify individuals with an adaptive immune response indicating recent or prior infection, as intended by the US FDA under an EUA.
Author Contributions
Conceptualization, C.C.L.; methodology, C.C.L., F.H. and M.C.; software, F.H., C.O., M.C. and J.M.; validation, F.H., C.O., A.L.-Y. and M.C.; formal analysis, C.C.L., F.H., C.O. and M.C.; investigation, F.H., C.O., A.L.-Y., M.C. and C.C.L.; resources, all; data curation, F.H., C.O., M.C., J.M. and C.C.L.; writing—original draft preparation, C.C.L.; writing—review and editing, M.C., C.O., F.H. and A.L.-Y.; visualization, C.C.L.; supervision, C.C.L.; project administration, C.C.L.; funding acquisition, C.C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by Clongene and Speranza.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Sharp Center for Research (protocol ID: IgG/IgM COVID19; IRB#: 2005801; 21 May 2020). This was a formal IRB approved clinical study conducted within Sharp Healthcare, a not-for-profit multicenter regional healthcare group located in San Diego, California. Subjects were included if hospitalized or recently discharged following a SARS-CoV-2 RT-PCR nares test. A study protocol and informed consent were initiated and approved by the Sharp Institutional Review Board. Subjects were included if they were >18 years of age and understood the study and its requirements. Patients who had impairment of cognition or decision-making capacity were excluded. Subjects were screened by research coordinators to determine if they had a nares SARS-CoV-2 RT-PCR test result, and then consent was requested to enroll them in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available.
Acknowledgments
The author acknowledges Ryan Dagenais for editorial support with the manuscript; his efforts were funded by BioSolutions Services LLC.
Conflicts of Interest
Christopher C. Lamb, PhD, has worked with the manufacturers of SARS-CoV-2 tests for Emergency Use Authorization submissions to the US FDA. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Our World in Data. Total Confirmed COVID-19 Deaths and Cases, World. 2021. Available online: https://ourworldindata.org/grapher/cumulative-deaths-and-cases-covid-19?country=~OWID_WRL. (accessed on 24 June 2021).
- IHME. COVID-19 Has Caused 6.9 Million Deaths Globally, More Than Double What Official Reports Show. 2021. Available online: http://www.healthdata.org/news-release/covid-19-has-caused-69-million-deaths-globally-more-double-what-official-reports-show (accessed on 12 August 2021).
- IHME. Estimation of Total Mortality Due to COVID-19. Available online: http://www.healthdata.org/special-analysis/estimation-excess-mortality-due-covid-19-and-scalars-reported-covid-19-deaths (accessed on 12 August 2021).
- Noh, J.; Danuser, G. Estimation of the fraction of COVID-19 infected people in US states and countries worldwide. PLoS ONE 2021, 16, e0246772. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C. COVID-19 diagnostic testing: Lessons learned for innovative product development during a public health emergency. J. Commer. Biotechnol. 2020, 25, 52–61. [Google Scholar] [CrossRef]
- CDC. Interim Guidelines for COVID-19 Antibody Testing. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 12 August 2021).
- Yang, Y.; Yang, M.; Shen, C.; Wang, F.; Yuan, J.; Li, J.; Zhang, M.; Wang, Z.; Xing, L.; Wei, J.; et al. Evaluating the accuracy of different respiratory specimens in the laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. medRxiv 2020. [Google Scholar] [CrossRef]
- Bošnjak, B.; Stein, S.C.; Willenzon, S.; Cordes, A.K.; Puppe, W.; Bernhardt, G.; Ravens, I.; Ritter, C.; Schultze-Florey, C.R.; Gödecke, N.; et al. Low serum neutralizing anti-SARS-CoV-2 S antibody levels in mildly affected COVID-19 convalescent patients revealed by two different detection methods. Cell. Mol. Immunol. 2020, 18, 936–944. [Google Scholar] [CrossRef]
- Casadevall, A.; Dragotakes, Q.; Johnson, P.W.; Senefeld, J.W.; Klassen, S.A.; Wright, R.S.; Joyner, M.J.; Paneth, N.; Carter, R.E. Convalescent Plasma Use in the United States was inversely correlated with COVID-19 Mortality: Did Convalescent Plasma Hesitancy cost lives? medRxiv 2021. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Risk of SARS-CoV-2 Transmission from Newly Infected individuals with Documented Previous Infection or Vaccination. 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Risk-of-transmission-and-reinfection-of-SARS-CoV-2-following-vaccination.pdf (accessed on 12 August 2021).
- Yadav, S.; Sadique, M.A.; Ranjan, P.; Kumar, N.; Singhal, A.; Srivastava, A.K.; Khan, R. SERS based lateral flow immunoassay for point-of-care detection of SARS-CoV-2 in clinical samples. ACS Appl. Bio Mater. 2021, 4, 2974–2995. [Google Scholar] [CrossRef]
- FDA. In Vitro Diagnostics EUAs-Serology and Other Adaptive Immune Response Tests for SARS-CoV-2. 2021. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-serology-and-other-adaptive-immune-response-tests-sars-cov-2. (accessed on 12 August 2021).
- Ragnesola, B.; Jin, D.; Lamb, C.C.; Shaz, B.H.; Hillyer, C.D.; Luchsinger, L.L. COVID19 antibody detection using lateral flow assay tests in a cohort of convalescent plasma donors. BMC Res. Notes 2020, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Osher, G.; Lamb, C.C.; Ibarra, Y.; Erickson-Samson, D. Observational Study of SARS-CoV-2 Antibody Immune Response in a Cohort of Patients at a North Suburban Chicago, Illinois Physician’s Practice. LymphoSign J. 2020, 7, 104–108. [Google Scholar] [CrossRef]
- Lamb, C.C.; Haddad, F.; Owens, C.D.; Lopez-Yunez, A.; Carroll, M.; Moncrieffe, J. Expanded Clinical Evaluation of the CLUNGENE® Rapid Covid-19 Antibody Test. J. Clin. Cell. Immunol. 2021, 12, 1–9. [Google Scholar]
- Haddad, F.; Lamb, C.C.; Kullar, R.; Sakoulas, G. Point-Of-Care Clinical Evaluation of the Clungene® SARS-CoV-2 Virus IgG/IgM 15-minute rapid test cassette with the Cobas® Roche RT-PCR platform in patients with or without Covid-19. LymphoSign J. 2021. [Google Scholar] [CrossRef]
- FDA. In Vitro Diagnostics EUAs. 2021. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/vitro-diagnostics-euas (accessed on 12 August 2021).
- MedComp Sciences. 2021. Available online: https://medcompsciences.com/ (accessed on 12 August 2021).
- Trina Bioreactives Ag. 2021. Available online: https://trinabio.com/ (accessed on 12 August 2021).
- SanDiegoCounty.gov. COVID-19 in San Diego County. 2021. Available online: https://www.sandiegocounty.gov/content/sdc/hhsa/programs/phs/community_epidemiology/dc/2019-nCoV/status.html (accessed on 12 August 2021).
- European Commission. MDCG 2021-2: Guidance on State of the Art of COVID-19 Rapid Antibody Tests. 2021. Available online: https://ec.europa.eu/health/sites/health/files/md_sector/docs/mdcg_2021-2_en.pdf. (accessed on 12 August 2021).
- Flower, B.; Brown, J.C.; Simmons, B.; Moshe, M.; Frise, R.; Penn, R.; Kugathasan, R.; Petersen, C.; Daunt, A.; Ashby, D.; et al. Clinical and laboratory evaluation of SARS-CoV-2 lateral flow assays for use in a national COVID-19 seroprevalence survey. Thorax 2020, 75, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Nicol, T.; Lefeuvre, C.; Serri, O.; Pivert, A.; Joubaud, F.; Dubée, V.; Kouatchet, A.; Ducancelle, A.; Lunel-Fabiani, F.; Le Guillou-Guillemette, H. Assessment of SARS-CoV-2 serological tests for the diagnosis of COVID-19 through the evaluation of three immunoassays: Two automated immunoassays (Euroimmun and Abbott) and one rapid lateral flow immunoassay (NG Biotech). J. Clin. Virol. 2020, 129, 104511. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.L.; Tseng, W.P.; Lin, C.H.; Lee, T.F.; Chung, M.Y.; Huang, C.H.; Chen, S.Y.; Hsueh, P.R.; Chen, S.C. Four point-of-care lateral flow immunoassays for diagnosis of COVID-19 and for assessing dynamics of antibody responses to SARS-CoV-2. J. Infect. 2020, 81, 435–442. [Google Scholar] [CrossRef]
- Zhu, X.; Wang, X.; Han, L.; Chen, T.; Wang, L.; Li, H.; Li, S.; He, L.; Fu, X.; Chen, S.; et al. Multiplex reverse transcription loop-mediated isothermal amplification combined with nanoparticle-based lateral flow biosensor for the diagnosis of COVID-19. Biosens. Bioelectron. 2020, 166, 112437. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; di Ruffano, L.F.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, CD013652. [Google Scholar] [CrossRef]
- Michigan Medicine. COVID-19 Antibody Tests, Even Rapid Finger Pricks, are Effective, New Study Finds. 2021. Available online: https://www.sciencedaily.com/releases/2021/03/210331173736.htm (accessed on 12 August 2021).
- Harvey, R.A.; Rassen, J.A.; Kabelac, C.A.; Turenne, W.; Leonard, S.; Klesh, R.; Meyer, W.A.; Kaufman, H.W.; Anderson, S.; Cohen, O.; et al. Association of SARS-CoV-2 seropositive antibody test with risk of future infection. JAMA Intern. Med. 2021, 181, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- John Hopkins Medicine. Immunology and Serology. 2021. Available online: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/immunology-and-serology (accessed on 12 August 2021).
- World Health Organization. Second WHO Model List of Essential In Vitro Diagnostics; World Health Organization: Genève, Switserland, 2019. [Google Scholar]
- Saluzzo, F.; Mantegani, P.; De Chaurand, V.P.; Quaresima, V.; Cugnata, F.; Di Serio, C.; Macé, A.; De Vos, M.; Sacks, J.A.; Cirillo, D.M. SARS-CoV-2 antibodies rapid tests: A valuable epidemiological tool in challenging settings. medRxiv 2021. [Google Scholar] [CrossRef]
- Aan de minister van Volksgezondheid, Welzijn en Sport. Verder uitstellen van de tweede dosis dan wel inzet van één dosis. 2021. Available online: https://www.alspatientsconnected.com/wp-content/uploads/2021/04/20210308-Advies-spoedvragen-VWS_COVID-19-vaccinatie-1-1.pdf (accessed on 27 August 2021).
- Mcglynn, M. New Covid Antibody Testing Service Opens at Shannon Airport. 2021. Available online: https://www.irishexaminer.com/news/munster/arid-40255340.html (accessed on 12 August 2021).
- The Blood Connection. NEW COVID-19 Antibody Testing. 2021. Available online: https://thebloodconnection.org/antibody-testing/ (accessed on 12 August 2021).
- Schipol.nl. Rapid Tests at Schiphol: Take a COVID-19 Test before Departure. 2021. Available online: https://www.schiphol.nl/en/page/testing-at-schiphol/ (accessed on 12 August 2021).
- Pfizer. Pfizer and Biontech Confirm High Efficacy and No Serious Safety Concerns through up to Six Months Following Second Dose in Updated Topline Analysis of Landmark Covid-19 Vaccine Study. 2021. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-confirm-high-efficacy-and-no-serious (accessed on 12 August 2021).
- Kriss, J.L.; Reynolds, L.E.; Wang, A.; Stokley, S.; Cole, M.M.; Harris, L.Q.; Shaw, L.K.; Black, C.L.; Singleton, J.A.; Fitter, D.L.; et al. COVID-19–Vaccine Second-Dose Completion and Interval Between First and Second Doses Among Vaccinated Persons—United States, December 14, 2020−February 14, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 389–395. [Google Scholar] [CrossRef]
- Agha, M.; Blake, M.; Chilleo, C.; Wells, A.; Haidar, G. Suboptimal response to COVID-19 mRNA vaccines in hematologic malignancies patients. MedRxiv 2021. [Google Scholar] [CrossRef]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CLUNGENE® Point-of-Care test manufacturer’s instructions.


{kind=link}
Table 1.
Common infectious agents used in cross-reactivity study.
| Analog |
|---|
| Anti-HBe, anti-HBc and HBsAg |
| Anti-Hepatitis C Virus (HCV) |
| Anti-Human Immunodeficiency Virus (HIV)-1 |
| Anti-HIV-2 |
| Anti-influenza A IgG |
| Anti-influenza B IgG |
| Anti-influenza A IgM |
| Anti-influenza B IgM |
| Anti-respiratory syncytial virus (RSV) IgG |
| Anti-respiratory syncytial virus (RSV) IgM |
| Anti-Mycoplasma pneumoniae (MP) IgM |
| Anti-Chlamydia pneumoniae (CP) IgM |
| Human parainfluenza virus PCR positive (Paired Convalescent) |
| Anti-Treponema pallidum (TP) |
| Rheumatoid factor (RF) 521.00 IU/mL RF 342.50 IU/mL RF 347.00 IU/mL RF 310.00 IU/mL RF 565.00 IU/mL RF 125.00IU/mL RF 796.00 IU/mL RF 500.00 IU/mL RF 825.00 IU/mL RF 144.00 IU/mL RF 158.00 IU/mL RF 122.00 IU/mL RF 197.00 IU/mL RF 146.00 IU/mL |
| Antinuclear antibodies (ANA) 1:240 |
| Common human pathogenic coronaviruses: HCoV-HKU1 HCoV-NL63 HCoV-OC43 HCoV-229E |
Table 2.
Reagents: reference numbers C58961 and C58957 Beckman Coulter Immunoassay System.
| Reagent | Reference Number | Material Type |
|---|---|---|
| Access SARS-CoV-2 IgG Calibrator | Ref. No. C58963 | |
| Access SARS-CoV-2 IgG Calibrator | Ref. No. C58958 | |
| Access SARS-CoV-2 IgG QC | Ref. No. C58964 | Quality Control (QC) |
| Access SARS-CoV-2 IgM QC | Ref. No. C58959 | Quality Control (QC) |
| Access Substrate | Ref. No. 81906 | Quality Control (QC) |
| Access Wash Buffer II | Ref. No. A16792 | Quality Control (QC) |
| UniCel DxI Wash Buffer II | Ref. No. A16793 | Quality Control (QC) |
Table 3.
Quality control for DXI600 analysis of cross-reactivity.
| Rack/Pos. | Sample ID Patient/Lot ID | Type Dilution | Test | Calibrator Results 1 | RLUs 2 | Completion | |
|---|---|---|---|---|---|---|---|
| 207/1 | COV-2IgG QC1 922605 | Serum | COV2G | Non-Reactive | 0.02 S/CO | 7143 | 27 April 2021 10:20 AM |
| 207/2 | COV-2IgG QC2 922605B | Serum | COV2G | Reactive | 2.49 S/CO | 995255 | 27 April 2021 10:20 AM |
| 207/3 | COV-2IgM QC1 922821 | Serum | COV2M | Non-Reactive | 0.16 S/CO | 11220 | 27 April 2021 10:27 AM |
| COV2M(2) | Non-Reactive | 0.16 S/CO | 11053 | 27 April 2021 10:27 AM | |||
| 207/4 | COV-2IgM QC2 922821 | Serum | COV2M | Reactive | 4.23 S/CO | 301471 | 27 April 2021 10:28 AM |
| COV2M(2) | Reactive | 2.62 S/CO | 186854 | 27 April 2021 10:27 AM | |||
1 S/CO: Signal/Cutoff. 2 RLUs: Relative Light Units.
Table 4.
Antibody percent agreement.
| Group | Days Post Symptom Onset | #PCR Total | Candidate Device Results | ||
|---|---|---|---|---|---|
| Results | PPA | 95% CI | |||
| IgG Positive | 0~7 | 4 | 2 | 50.00% | 15.00~85.00% |
| 8~14 | 23 | 23 | 100.00% | 85.69~100.00% | |
| ≥15 | 35 | 33 | 94.28% | 81.39~98.42% | |
| Total | 62 | 58 | 93.55% | 84.55~97.46% | |
| IgM Positive | 0~7 | 4 | 3 | 75.00% | 30.06~95.44% |
| 8~14 | 23 | 21 | 91.30% | 73.21~97.58% | |
| ≥15 | 35 | 27 | 77.14% | 60.98~87.93% | |
| Total | 62 | 51 | 82.26% | 70.96~89.79% | |
| IgG/IgM Combined Antibody Positive | 0~7 | 4 | 3 | 75.00% | 30.06~95.44% |
| 8~14 | 23 | 23 | 100.00% | 85.69~100.00% | |
| ≥15 | 35 | 34 | 97.14% | 85.47~99.49% | |
| Total | 62 | 60 | 96.77% | 88.98~99.11% | |
| IgG Negative | N/A | 37 | 37 | 100.00% | 90.60~100.00% |
Table 5.
Line Table Data.
| # and Site | Subject ID | Age | Gender (F/M) | Whole Blood Specimen Collection Date | Days after Symptom Onset | CLUNGENE® Rapid Test Result (Pos/Neg) | PCR Test Date | PCR Confirmation Result | |
|---|---|---|---|---|---|---|---|---|---|
| IgM | IgG | ||||||||
| 1a | 007sgh | 66 | F | 1 June 2020 | Neg | Neg | 30 May 2020 | Neg | |
| 2a | 008sgh | 65 | F | 1 June 2020 | Neg | Neg | 29 May 2020 | Neg | |
| 3a | 009sgh | 72 | M | 1 June 2020 | Neg | Neg | 31 May 2020 | Neg | |
| 4a | 010sgh | 67 | F | 5 June 2020 | Neg | Neg | 27 May 2020 | Neg | |
| 5a | 011sgh | 44 | M | 5 June 2020 | Neg | Neg | 1 June 2020 | Neg | |
| 6a | 012sgh | 31 | F | 5 June 2020 | Neg | Neg | 1 June 2020 | Neg | |
| 7a | 013sgh | 77 | F | 5 June 2020 | Neg | Neg | 1 June 2020 | Neg | |
| 8a | 024smh | 37 | M | 5 June 2020 | 11 | Neg | Pos | 2 June 2020 | Pos |
| 9a | 025sgh | 89 | M | 5 June 2020 | Neg | Neg | 11 June 2020 | Neg | |
| 10a | 023sgh | 91 | F | 6 June 2020 | Neg | Neg | 9 June 2020 | Neg | |
| 11a | 024sgh | 81 | M | 8 June 2020 | Neg | Neg | 9 June 2020 | Neg | |
| 12a | 026sgh | 59 | M | 8 June 2020 | Neg | Neg | 11 June 2020 | Neg | |
| 13a | 019sgh | 69 | F | 9 June 2020 | 20 | Neg | Pos | 23 May 2020 | Pos |
| 14a | 028sgh | 58 | M | 10 June 2020 | Neg | Neg | 11 June 2020 | Neg | |
| 15a | 021sgh | 63 | F | 11 June 2020 | 13 | Neg | Pos | 6 June 2020 | Pos |
| 16a | 027sgh | 77 | F | 11 June 2020 | Neg | Neg | 1 June 2020 | Neg | |
| 17a | 029sgh | 29 | M | 12 June 2020 | 8 | Pos | Pos | 8 June 2020 | Pos |
| 18a | 033sgh | 69 | M | 12 June 2020 | Neg | Neg | 5 June 2020 | Neg | |
| 19a | 034sgh | 53 | M | 12 June 2020 | Neg | Neg | 11 June 2020 | Neg | |
| 20a | 035sgh | 77 | M | 12 June 2020 | Neg | Neg | 11 June 2020 | Neg | |
| 21a | 036sgh | 74 | M | 12 June 2020 | Neg | Neg | 10 June 2020 | Neg | |
| 22a | 037sgh | 30 | F | 12 June 2020 | Neg | Neg | 9 June 2020 | Neg | |
| 23a | 038sgh | 22 | M | 12 June 2020 | Neg | Neg | 6 June 2020 | Neg | |
| 24a | 001sgh | 38 | M | 15 June 2020 | 26 | Pos | Pos | 23 May 2020 | Pos |
| 25a | 006sgh | 53 | M | 18 June 2020 | 23 | Neg | Pos | 29 May 2020 | Pos |
| 26a | 027smh | 47 | M | 18 June 2020 | 14 | Pos | Pos | 14 June 2020 | Pos |
| 27a | 039sgh | 60 | M | 18 June 2020 | 13 | Pos | Pos | 14 June 2020 | Pos |
| 28a | 043sgh | 22 | F | 18 June 2020 | 18 | Neg | Pos | 14 June 2020 | Pos |
| 29a | 040sgh | 70 | M | 19 June 2020 | 17 | Pos | Pos | 12 June 2020 | Pos |
| 30a | 044sgh | 32 | F | 19 June 2020 | Neg | Neg | 17 June 2020 | Neg | |
| 31a | 045sgh | 66 | M | 19 June 2020 | Neg | Neg | 10 June 2020 | Neg | |
| 32a | 046sgh | 65 | M | 19 June 2020 | Neg | Neg | 9 June 2020 | Neg | |
| 33a | 050sgh | 31 | M | 26 June 2020 | 8 | Pos | Pos | 18 June 2020 | Pos |
| 34a | 051sgh | 44 | M | 26 June 2020 | 10 | Pos | Pos | 21 June 2020 | Pos |
| 35a | 052sgh | 35 | M | 26 June 2020 | 7 | Pos | Pos | 19 June 2020 | Pos |
| 36a | 055sgh | 57 | M | 26 June 2020 | Neg | Neg | 21 June 2020 | Neg | |
| 37a | 056sgh | 69 | F | 26 June 2020 | Neg | Neg | 22 June 2020 | Neg | |
| 38a | 057sgh | 67 | M | 26 June 2020 | Neg | Neg | 21 June 2020 | Neg | |
| 39a | 058sgh | 59 | F | 26 June 2020 | Neg | Neg | 17 June 2020 | Neg | |
| 40a | 059sgh | 39 | M | 26 June 2020 | 6 | Neg | Neg | 20 June 2020 | Pos |
| 41a | 060sgh | 28 | F | 26 June 2020 | Neg | Neg | 24 June 2020 | Neg | |
| 42a | 061sgh | 51 | F | 26 June 2020 | Neg | Neg | 23 June 2020 | Neg | |
| 43a | 062sgh | 71 | F | 26 June 2020 | 11 | Pos | Pos | 23 June 2020 | Pos |
| 44a | 072sgh | 62 | M | 2 July 2020 | 17 | Pos | Pos | 15 June 2020 | Pos |
| 45a | 031smh | 31 | F | 2 July 2020 | 22 | Pos | Pos | 11 June 2020 | Pos |
| 46a | 066sgh | 43 | F | 2 July 2020 | 15 | Pos | Neg | 24 June 2020 | Pos |
| 47a | 068sgh | 60 | M | 2 July 2020 | 12 | Pos | Pos | 25 June 2020 | Pos |
| 48a | 075sgh | 62 | F | 2 July 2020 | 7 | Pos | Pos | 25 June 2020 | Pos |
| 49a | 081sgh | 73 | M | 9 July 2020 | 9 | Pos | Pos | 4 July 2020 | Pos |
| 50a | 082sgh | 63 | M | 9 July 2020 | 11 | Pos | Pos | 3 July 2020 | Pos |
| 51a | 084sgh | 68 | M | 9 July 2020 | 15 | Pos | Pos | 2 July 2020 | Pos |
| 52a | 088sgh | 56 | F | 9 July 2020 | 10 | Pos | Pos | 7 July 2020 | Pos |
| 53a | 090sgh | 88 | F | 9 July 2020 | 20 | Neg | Pos | 7 July 2020 | Pos |
| 54a | 089sgh | 56 | F | 17 July 2020 | 16 | Pos | Pos | 4 July 2020 | Pos |
| 55a | 094sgh | 19 | F | 17 July 2020 | 15 | Pos | Pos | 11 July 2020 | Pos |
| 56a | 096sgh | 36 | M | 17 July 2020 | 27 | Pos | Pos | 14 July 2020 | Pos |
| 57a | 097sgh | unknown | F | 17 July 2020 | Neg | Neg | 14 July 2020 | Neg | |
| 58a | 098sgh | unknown | M | 17 July 2020 | Neg | Neg | 8 July 2020 | Neg | |
| 59a | 099sgh | 48 | F | 21 July 2020 | 9 | Pos | Pos | 18 July 2020 | Pos |
| 60a | 100sgh | 48 | F | 21 July 2020 | 14 | Pos | Pos | 17 July 2020 | Pos |
| 61a | 101sgh | 72 | M | 21 July 2020 | 16 | Neg | Neg | 25 July 2020 | Pos |
| 62a | 053sgh | 50 | F | 23 July 2020 | 27 | Neg | Pos | 26 June 2020 | Pos |
| 63a | 073sgh | 38 | M | 23 July 2020 | 34 | Pos | Pos | 30 June 2020 | Pos |
| 64a | 103sgh | 29 | M | 24 July 2020 | 12 | Pos | Pos | 15 July 2020 | Pos |
| 65a | 104sgh | 40 | M | 24 July 2020 | 21 | Pos | Pos | 11 July 2020 | Pos |
| 66a | 106sgh | 45 | M | 28 July 2020 | 15 | Neg | Pos | 22 July 2020 | Pos |
| 67a | 113sgh | 46 | F | 31 July 2020 | 7 | Pos | Neg | 25 July 2020 | Pos |
| 68a | 114sgh | 79 | F | 4 August 2020 | 12 | Pos | Pos | 30 July 2020 | Pos |
| 69a | 110sgh | 51 | F | 5 August 2020 | 15 | Pos | Pos | 29 July 2020 | Pos |
| 70a | 109sgh | 63 | M | 7 August 2020 | 19 | Pos | Pos | 25 July 2020 | Pos |
| 71a | 119sgh | 60 | F | 8 August 2020 | 10 | Pos | Pos | 7 August 2020 | Pos |
| 72a | 105sgh | 38 | M | 12 August 2020 | 31 | Pos | Pos | 20 July 2020 | Pos |
| 73a | 120sgh | 73 | M | 13 August 2020 | 22 | Pos | Pos | 26 July 2020 | Pos |
| 74a | 123sgh | 47 | M | 13 August 2020 | 12 | Pos | Pos | 10 August 2020 | Pos |
| 75a | 124sgh | 80 | M | 13 August 2020 | 30 | Pos | Pos | 20 July 2020 | Pos |
| 76a | 118sgh | 94 | F | 14 August 2020 | 15 | Neg | Pos | 31 July 2020 | Pos |
| 77a | 117sgh | 28 | F | 14 August 2020 | 14 | Pos | Pos | 5 August 2020 | Pos |
| 78a | 121sgh | 62 | F | 17 August 2020 | 14 | Pos | Pos | 12 August 2020 | Pos |
| 1b | C011 | 29 | F | 12 December 2020 | 14 | Pos | Pos | 30 November 2020 | Pos |
| 2b | A005 | 44 | F | 12 December 2020 | Neg | Neg | 6 December 2020 | Neg | |
| 3b | C020 | 30 | F | 12 December 2020 | 14 | Pos | Pos | 28 November 2020 | Pos |
| 4b | C012 | 52 | M | 14 December 2020 | 14 | Pos | Pos | 5 December 2020 | Pos |
| 5b | C032 | 46 | M | 14 December 2020 | Neg | Neg | 10 December 2020 | Neg | |
| 6b | C033 | 18 | M | 14 December 2020 | Neg | Neg | 10 December 2020 | Neg | |
| 7b | C004 | 74 | M | 19 December 2020 | 26 | Pos | Pos | 3 December 2020 | Pos |
| 8b | C030 | 28 | M | 19 December 2020 | Neg | Neg | 16 December 2020 | Neg | |
| 9b | C016 | 39 | F | 21 December 2020 | 19 | Pos | Pos | 10 December 2020 | Pos |
| 10b | C031 | 18 | F | 21 December 2020 | Neg | Neg | 16 December 2020 | Neg | |
| 11b | C009 | 53 | F | 29 December 2020 | 18 | Pos | Pos | 19 December 2020 | Pos |
| 12b | C010 | 55 | M | 29 December 2020 | 19 | Pos | Pos | 19 December 2020 | Pos |
| 13b | C028 | 46 | M | 29 December 2020 | 24 | Pos | Pos | 18 December 2020 | Pos |
| 14b | C005 | 19 | F | 31 December 2020 | 21 | Pos | Pos | 18 December 2020 | Pos |
| 15b | C006 | 19 | F | 31 December 2020 | 21 | Pos | Pos | 18 December 2020 | Pos |
| 16b | C007 | 42 | F | 31 December 2020 | 21 | Pos | Pos | 18 December 2020 | Pos |
| 17b | C019 | 42 | F | 31 December 2020 | 15 | Pos | Pos | 18 December 2020 | Pos |
| 18b | C026 | 51 | F | 31 December 2020 | Neg | Neg | 31 December 2020 | Neg | |
| 19b | C027 | 43 | F | 31 December 2020 | Neg | Neg | 31 December 2020 | Neg | |
| 20b | C029 | 54 | M | 31 December 2020 | 15 | Pos | Pos | 26 December 2020 | Pos |
| 21b | C013 | 40 | M | 4 January 2021 | 28 | Pos | Pos | 15 December 2020 | Pos |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lamb, C.C.; Haddad, F.; Owens, C.; Lopez-Yunez, A.; Carroll, M.; Moncrieffe, J. Updated Clinical Evaluation of the CLUNGENE® Rapid COVID-19 Antibody Test. Healthcare 2021, 9, 1124. https://doi.org/10.3390/healthcare9091124
AMA Style
Lamb CC, Haddad F, Owens C, Lopez-Yunez A, Carroll M, Moncrieffe J. Updated Clinical Evaluation of the CLUNGENE® Rapid COVID-19 Antibody Test. Healthcare. 2021; 9(9):1124. https://doi.org/10.3390/healthcare9091124
Chicago/Turabian StyleLamb, Christopher C., Fadi Haddad, Christopher Owens, Alfredo Lopez-Yunez, Marion Carroll, and Jordan Moncrieffe. 2021. "Updated Clinical Evaluation of the CLUNGENE® Rapid COVID-19 Antibody Test" Healthcare 9, no. 9: 1124. https://doi.org/10.3390/healthcare9091124
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.