Article Text

Abstract
WHO informed Egypt health authorities of individuals of different nationalities who proved positive for COVID-19 after returning from Egypt. Patients were among touristic group who visited Cairo and spent 1-week onboard Nile cruise ship. Investigation performed to confirm outbreak, detect source, and implement containment measures. Active case finding and contact tracing performed among contacts of the index cases and their contacts. Contacts defined as anyone within 6 feet from confirmed or suspected COVID-19 case for ≥15 min. Overall, 331 contacts, including 201 ship boarders and 130 hotel guests, were listed and interviewed using semistructured questionnaire and tested for COVID-19 by PCR. Among them, 136 (41.1%) were close contacts of index cases and 195 (58.9%) contacted secondary cases. Their mean age was 34.6±11.5 years, 251 (75.8%) were males and 126 (38.1%) non-Egyptians. Of them, 67 (20.2%) tested positive for COVID-19, including 57 (28.4%) ship boarders and 10 (7.7%) hotel guests. Per cent positive was significantly higher in: contacts of index cases, Egyptians, ship boarders and in males than corresponding categories (35.3% vs 9.7%, 22.9% vs 15.9%, 27.4% vs 7.7%, 24.7% vs 6.3%), respectively. Of all positive cases, 40 (59.7%) were asymptomatic where ship boarders, non-Egyptians, >50 years old and females were more likely to be asymptomatic than corresponding categories (85.0 vs 48.9%, 72.7 vs 54.5%, 100.0 vs 56.5%), respectively. COVID-19 patients among group of tourists triggered an outbreak onboard Nile ship and hotel in Egypt. Outbreak quickly contained through lab testing, case isolation, strict infection control measures and contact tracing which proved effective in reducing COVID-19 transmission early in pandemic.
- COVID-19
- epidemiology
- public health
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Contact tracing and extensive testing are considered types of the non-pharmaceutical interventions for epidemic control.
Contact tracing and case isolation are effective policies in containment and mitigation of COVID-19 pandemic.
COVID-19 can sustain outbreaks and spread easily within communities even through asymptomatic cases.
Global collaboration is needed to combat COVID-19.
Larger numbers of trained public health workers and laboratorians are urgently needed to combat future epidemics.
Introduction
Although it is an age-old public health intervention, contact tracing is now being implemented at an unprecedented scale. It has proved successful in fighting the epidemic of COVID-19, especially in its early stage, when combined with other measures.1 Studies indicated that isolation of cases and tracing of their contacts could successfully lower the reproduction number to less than one in the absence of other measures.2 The aim of tracing contacts of COVID-19 cases is to rapidly identify secondary cases to interrupt further transmission.
Many countries for example, China, South Korea and Germany have implemented extensive tracking programmes that have helped officials make major steps in reducing the outbreak. In other countries, contact tracing has faced many challenges, such as unavailability of extensive workforce, low response rate, inadequate use of technology, privacy concerns and a far less broad mandate.3 Although it has been suggested that the effectiveness of contact tracing could be enhanced through app-based digital tracing, manual tracing proved more effective.2
One modelling study suggested that Egypt had succeeded in delaying the peak of the COVID-19 curve after the seventh week of the pandemic as no exponential growth of transmission rate was identified.4 One of the most effective measures taken by Egypt for epidemic mitigation and flattening of the curve was contact tracing and case isolation.
The COVID-19 epidemic started in Egypt on the 14 February 2020, one and half months after the announcement of the epidemic in China. The first confirmed case was found in a Chinese man working in Cairo who was in close contact with a confirmed case who felt sick in China after returning from Egypt. The Chinese Embassy informed the Egyptian Health Authority of the case as soon as it was confirmed. All the 308 contacts of this first confirmed case were traced and followed up for 14 days, although in this instance no one tested positive for COVID-19.
On 27 February, a Canadian man working in a large enterprise in the far North of Egypt was presented at a healthcare facility with respiratory symptoms and found COVID-19 positive a few days after arriving in Egypt. Nearly 2750 people at the enterprise were traced and followed up for 14 days after exposure to the case and found negative for COVID-19.
A few days later, other confirmed COVID-19 cases were captured through Egyptian event-based surveillance among tourists of different nationalities who had recently visited Egypt. These cases were not directly communicated to the appropriate ministries.
Outbreak detection
On 29 February 2020, WHO informed Egypt Ministry of Health and Population (MoHP) under the International Health Regulations (IHR) of two French patients who were confirmed for COVID-19 few days after returning from a touristic trip to Egypt. They started their trip in Cairo then boarded a Nile ship from Luxor to Aswan in Southern Egypt and travelled back to Cairo by air where they spent nights in two large hotels and visited about 35 touristic areas. Two teams started to trace their contacts in all the places they visited. No symptoms were reported from the contacts identified.
On 1 March 2020, Taiwan health authorities informed Egypt IHR focal person of a Taiwanese woman who tested positive for COVID-19 a few days after returning from a trip to Egypt and the United Arab Emirates. Tracing this patient revealed that she stayed in a hotel in Cairo and was on board the same Nile ship with the two French patients.
As of the 3 March, WHO/EMRO informed the Egyptian MoHP of two American citizens who tested positive with COVID-19 after returning from Egypt. They were also passengers onboard the Nile ship with the French and Taiwanese patients during the same period from 9 to 18 February.
Outbreak investigations
Outbreak investigation began by identifying close contacts of the tourist group using the US Centers for Disease Control and Prevention contacts case definition.5 A team was deployed to the Nile ship to investigate the event and evaluate the preparedness of healthcare facilities in Luxor and Aswan to manage incoming COVID-19 cases. The investigation team arrived on the 4 March 2020, 26 days after first arrival and 15 days from the last departure of the group from the Nile ship (table 1).
Comparison between findings of outbreak investigations onboard MS A'SARA Nile cruise ship and the Cairo hotel, Egypt, March 2020
A sensitive case definition of fever and/ or respiratory symptoms within the last 14 days was applied for active case detection among current guests and staff members who were onboard 1 February—4 March 2020. Close contact was defined as anyone who was within 6 feet of a person among the tourist group >15 min.5 They were listed using the ship records, contacted, and interviewed by phone or face-to-face. Suspected cases and contacts interviewed using semistructured questionnaire that includes demographics, clinical symptoms and exposures. They asked to provide nasopharyngeal/oropharyngeal swab for lab testing. Specimens were placed in Viral Transport Media and immediately transferred to the Central Public Health Laboratory (CPHL) in Cairo for SARS-COV-2 testing by Real-Time PCR.
The second day Lab results indicated that 45 specimens were positive for SARS-CoV-2, including 33 (73.3%) asymptomatic patients. the ship was quarantined between Luxor and Aswan and investigations extended to include contacts of the newly confirmed cases. Cases were sent to COVID-19 isolation hospitals where they received medical care and released after having two negative PCR tests separated by 48 hours. Contacts were isolated onboard the ship and those who left before the investigation were placed under home-based isolation and followed up for 14 days (table 1).
A second team was deployed to the hotel on 4 March, 15 days after the group checked out (table 1). Team identified and interviewed the tourist group contacts and identified suspected cases using the same questionnaire and specimens were sent to CPHL for testing.
Lab results indicated that three (8.1%) of the 37 specimens collected from the hotel staff were positive for SARS-CoV-2. All patients are working at the main restaurant. The hotel was quarantined, and patients immediately transferred to hospital. Investigation and lab testing were extended to include all staff of the main restaurant, contacts of the confirmed cases and any staff member with respiratory symptoms last 14 days.
Findings
A total of 331 contacts were investigated including 201 in the ship and 130 in the hotel. Among them, 136 (41.1%) were close contacts of the tourist group and 195 (58.9%) contacts of the secondary cases. Contacts’ mean age was 34.6±11.5 years, 251 (75.8%) were males, 205 (61.9%) were Egyptians, and 126 (38.1%) non-Egyptians (table 1).
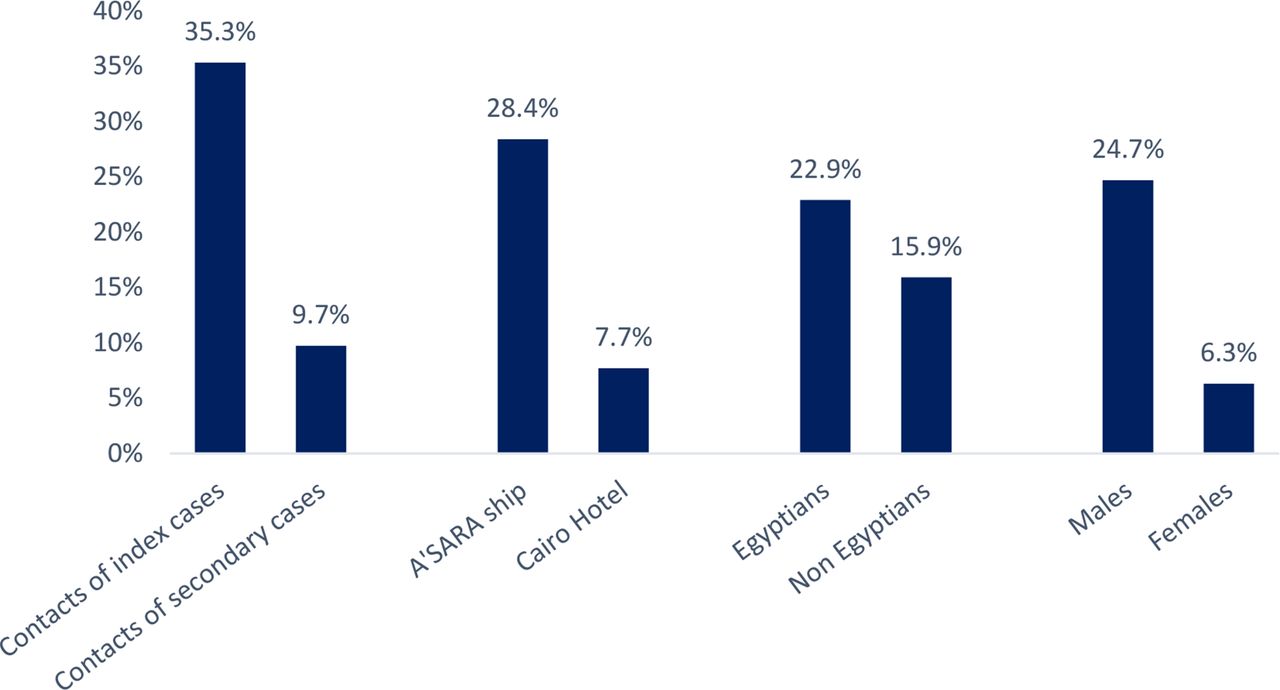
Of them 67 (20.2%) were lab confirmed including 48 (71.6%) contacts of the tourist group and 19 (28.4%) contacts of secondary cases. Patients’ mean age was 34.6±12, 62 (92.5%) were males and 44 (65.7%) were <50 years of age (table 1). Per cent positive was significantly higher among contacts of the tourist group, ship boarders, males and Egyptians compared with the corresponding categories (35.3 vs 9.7%, 28.4 vs 7.7%, 24.7 vs 6.3% and 22.9 vs 15.9%, respectively) (figure 1).

Attack rates among different categories of contacts investigated, COVID-19 outbreak investigation, Egypt, March 2020 (n=67).
Of all positive cases, 40 (59.7%) were asymptomatic to the end of quarantine period. Higher per cent of asymptomatic cases were reported among ship boarders, non-Egyptians, ≥50 years of age and in females than corresponding categories (63.2 vs 40.0%, 85.0 vs 48.9%, 69.6 vs 45.5% and 100.0 vs 56.5%, respectively) (figure 2).

{kind=link}
{kind=link}
Per cent of asymptomatic cases among different categories of positive contacts investigated, COVID-19 outbreak investigation, Egypt, March 2020 (n=67).
Among 27 symptomatic cases, the most reported symptoms were cough 11 (40.7%), fever 7 (25.9%), sore throat 7 (25.9%), and runny nose 5 (18.5%).
No suspected COVID-19 cases were reported to the near healthcare facilities. The overall attack rate on board the Nile Cruise was 57/201 (28.4%), and among Cairo hotel staff was 10/130 (7.7%).
It was obvious that the index case was someone onboard the Nile ship, most probably among the French tourists, who started to feel symptoms the day they arrived in Egypt. The SARS-COV-2 virus circulated between the Nile ship guests and crew for ten days. When the group stayed in the Cairo hotel, the virus was transmitted to the hotel restaurant staff and to Egypt’s second nationally confirmed case.
The outbreak spread easily on the Nile ship because of the close confines and limited ventilation in small spaces. Ineffective communication and unavailability of full data about index cases led to a delay in identifying the source of infection to interrupt disease transmission. Legally, the sharing of private health data is impermissible due to risk of privacy violation and other fundamental rights of citizens.6 Policy-makers must reconcile the risks and benefits for sharing personal and health data in case of a pandemic, while ensuring full transparency, accountability and a commitment to immediately stop using the data when the crisis is over.
Although some studies suggested that the transmission of COVID-19 occurs by asymptomatic cases,7 most of the asymptomatic cases identified among guests and Nile ship crew could have contributed to the higher rate of disease transmission seen on board the Nile ship. This was similar to the situation onboard the Diamond Princess.8 However, the percentage of asymptomatic cases on the Nile ship was much higher than that reported on the Diamond Princess (63.2 vs 17.9%).9 This may explain why there was a higher attack rate reported on the Nile ship than the Diamond princess (28.6 vs 16.7%). The difference could be also explained by the small size of the Nile Ship and delays in implementation of outbreak interventions.
The per cent of asymptomatic cases in this study was higher in females, a finding also reported in other studies, and also higher in older ages, which is in contrast to most other outbreak studies.7 10 Yang et al found that the damage to the immune system in COVID-19 patients with asymptomatic infections was milder compared those with symptomatic infections, a finding supported by the less consumption of CD4 +T lymphocyte in asymptomatic than symptomatic infections.7
It was suggested that BCG vaccine provides some protection against other diseases including COVID-19 because it appears to help boost the immune system.11 Hence it was assumed that the low prevalence of the disease in some countries could be linked to the compulsory BCG vaccination in these countries. BCG vaccine has been provided to all children below 6 months of age in Egypt since 1974, whereas it was removed from the immunisation schedule in Europe and USA because of Tuberculosis eradication during the same era. A higher attack rate occurred among Egyptians compared with the non-Egyptians in this outbreak, in contradiction to this assumption. The higher attack rate among Egyptians could be related to longer duration of stay onboard before intervention and crowded/poorly ventilated conditions in staff living areas.
The transmission of the disease in Cairo hotel was much slower than that in the Nile ship. Reasons could be earlier intervention, shorter duration of the group stay, larger communal spaces and better ventilation systems in the hotel.
Contact tracing, in combination with testing of contacts and case isolation, is considered a key component of pandemic control measures as and when lockdown measures are gradually lifted.12 Contact tracing has proved effective in optimising testing strategies, minimising testing delays, and therefore, reducing onward transmission. Although contact tracing is useful in this regard, it is also labour intensive and cost prohibitive in some contexts. In our outbreak investigation, the suspected index cases were among a touristic group who visited many tourist attractions and accommodation facilities in Cairo, Luxor, and Aswan. Their trip schedule started with one night in Cairo hotel then ten days onboard a Nile ship between Luxor and Aswan, then back to the hotel in Cairo before leaving to their respective countries. The group did sightsee and visited oriental bazaars for souvenirs in all cities they visited. MoHP teams investigated all places they visited during their trip to Egypt, in addition to the near healthcare facilities for active cases related to these contacts. The mission was facilitated in collaboration between the Egyptian tourism authorities, Egyptian National Police, and MoHP.
Outbreak control measures
As soon as outbreak confirmed onboard the ship, all ship boarders were considered contacts. Field clinics were set up to identify suspected cases, specimens collected and shipped to CPHL every day. Laboratory results delivered within 24 hours, confirmed cases were notified and managed according to Egyptian case management protocol. All patients immediately transferred to isolation hospitals.
Medications, masks, gloves and disinfectants were provided to all staff at both facilities. The Ship crew and hotel staff were trained on infection prevention and control measures. All passengers were instructed to stay at their rooms and food was served at rooms under infection control measures.
Challenges and lessons learnt
The first challenge was the delay and difficulty in obtaining information on the index cases. The group stayed from 9 February to 20 February, while the first IHR report to Egypt was in 29 February. Early information provided on such cases was ambiguous and did not help in pinpointing the source of infection. More details were only made available when a second report was sent to Egypt on the third of March. This led to a delay in index case detection and allowed disease spread.
Early in the outbreak WHO released a case definition that depends on identifying symptomatic cases. As the pandemic progressed studies suggested a role for the presymptomatic and asymptomatic cases in transmission of infection.13 This investigation revealed that three-quarters of the cases detected on the Nile ship were preasymptomatic or asymptomatic, a finding that could be reflected to community transmission. It is essential that individuals exposed to suspected or confirmed COVID-19 patients be quickly identified and quarantined to prevent disease spread. US CDC recommends testing of all close contacts of persons with COVID-19 because of the potential for asymptomatic and presymptomatic transmission.14 Contact tracing could help target this group where lab capacity is limited especially in middle-income and low-income countries.
Since it was impossible to test 900 hotel staff members a targeted testing strategy was implemented. Testing first performed to the staff directly contacted the touristic group, followed by contacts of positive contacts in addition to all symptomatic staff members. The possibility of finding contacts to the touristic group among hotel guests was nil because of the long period since they checked out.
From an economic point of view, confirmed COVID-19 cases among tourists in Egypt had a devastating effect on the touristic season. Many hotels and hostels and Nile ships were closed due to suspected asymptomatic or mild COVID-19 cases. Owners of such places resisted outbreak investigation within their facilities to avoid orders of closure. Security authorities helped to facilitate investigation teams’ mission and coordinate with touristic facilities in Egypt.
Ship tourists at first resisted movement restriction and complained of the strict preventive measures implemented. However, they complied to instructions when the investigation team provided them with accurate description of the current situation based on available information with clear instructions to follow.
Unavailability of nearby laboratories capable of SARS-CoV-2 testing was the most difficult challenge. At first, MoHP assigned CPHL for SARS-CoV-2 testing. Shipping the samples of suspected cases 1000 Km by car for testing was not easy, especially when public transportation and air travel was banned. Later, MoHP assigned more regional labs through developing the infrastructure for PCR tests.
Conclusions
A localised outbreak of COVID-19 occurred onboard a Nile Cruise Ship in Egypt. The source of the outbreak was tourists who spread the infection to others onboard the ship and hotel staff in Cairo 1000 km from the origin of the ship’s route.
The delay in reporting of index cases has contributed to delayed interventions. Timely and effective communication across borders is essential for early case detection and identification of the source of outbreaks.
Outbreak control measures included active case finding, contact tracing, lab testing, and case isolation were implemented. Contact tracing and case isolation proved effective in slowing the rate of COVID-19 spread. To overcome the fiscal and workforce difficulties of contact tracing targeted laboratory testing and follow-up strategy could be used, especially in middle-income and low-income countries. A wide case definition that includes asymptomatic contacts of confirmed cases should also be used to catch more cases and prevent further disease transmission. Increasing the number of trained public health workers and laboratorians is urgently needed to combat future epidemics.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Egyptian Ministry of Health and Population Institutional Review Board (IRB). Participants gave informed consent to participate in the study before taking part.
Footnotes
Handling editor Seye Abimbola
Contributors HH contributed to outbreak investigation and prepared the manuscript, HH is responsible for the overall content as a guarantor, BE and RK participated in outbreak investigation and field work, HAE planned for the work, MF supervised field work and data collection, SES critically reviewed manuscript, SS performed lab work, AM critically reviewed manuscript, SA drafted manuscript, AE oversee field work and manuscript development. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.