

Bivalirudin vs. Enoxaparin in Intubated COVID-19 Patients: A Pilot Multicenter Randomized Controlled Trial

 and
and
Abstract
:1. Background
2. Materials and Methods
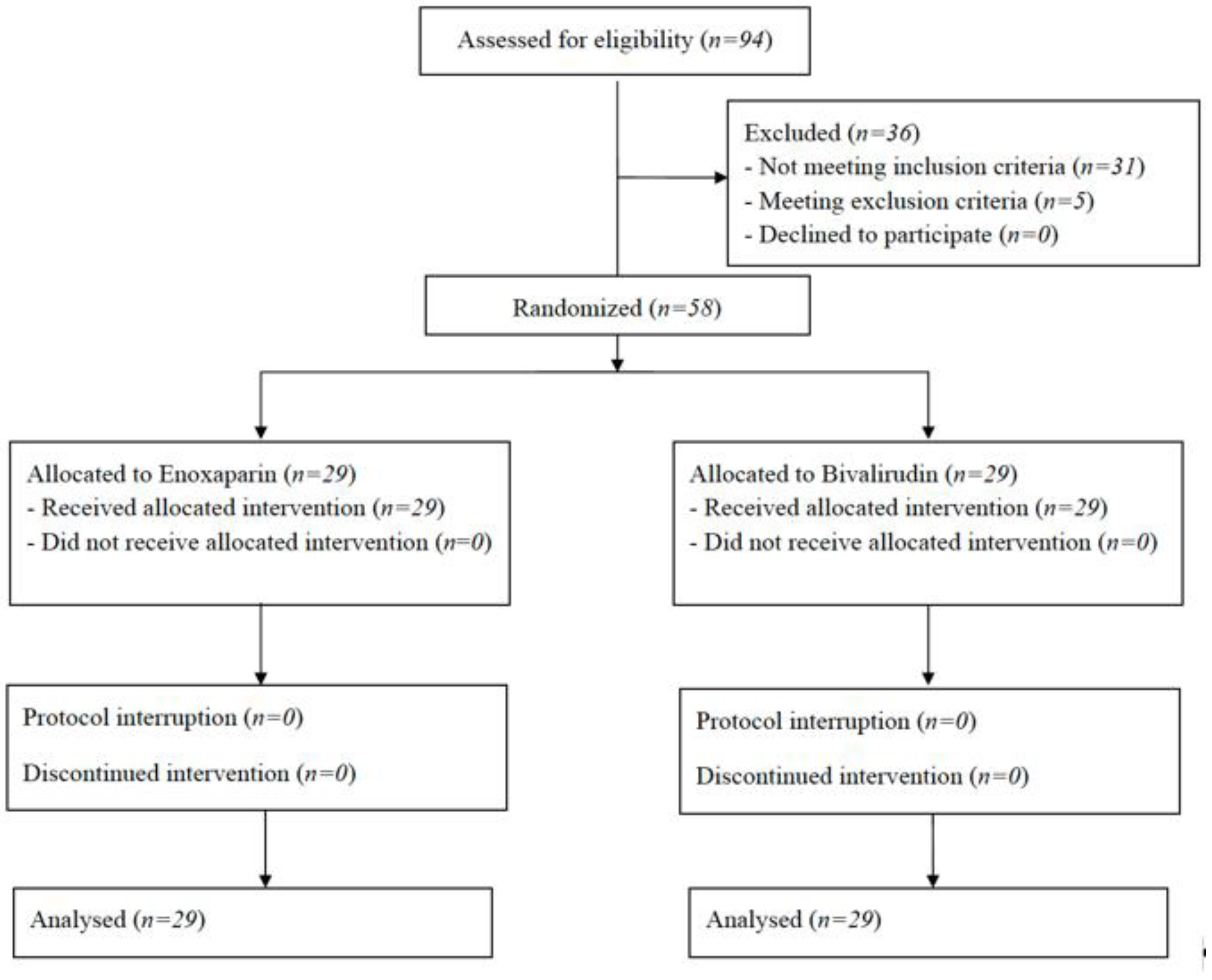
2.1. Population
2.2. Randomization
2.3. Treatments
2.4. Discontinuation of Study Drugs
2.5. Study Endpoints
2.6. Data Collection and Outcome Assessment
2.7. Statistical Analysis
3. Results
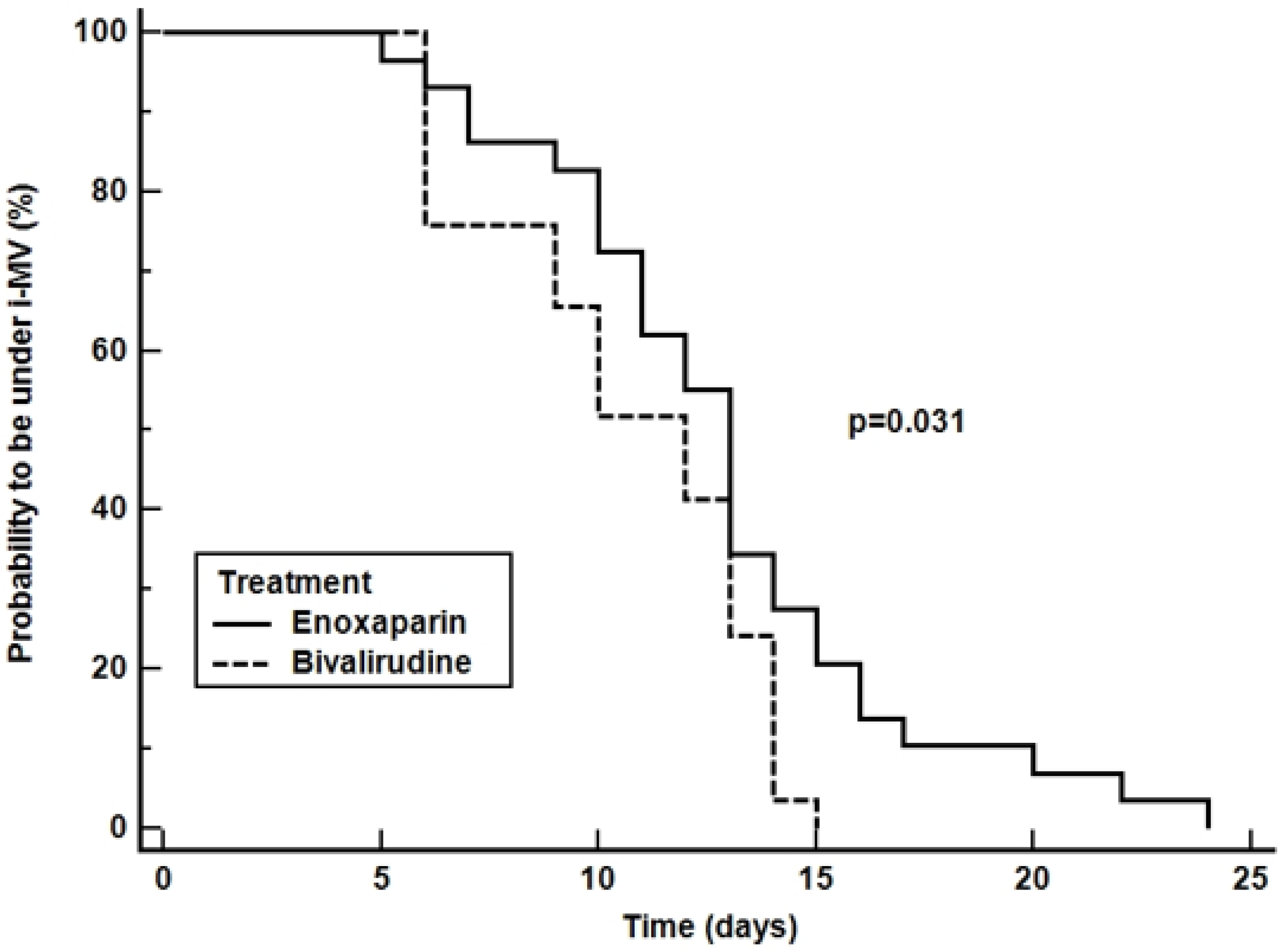
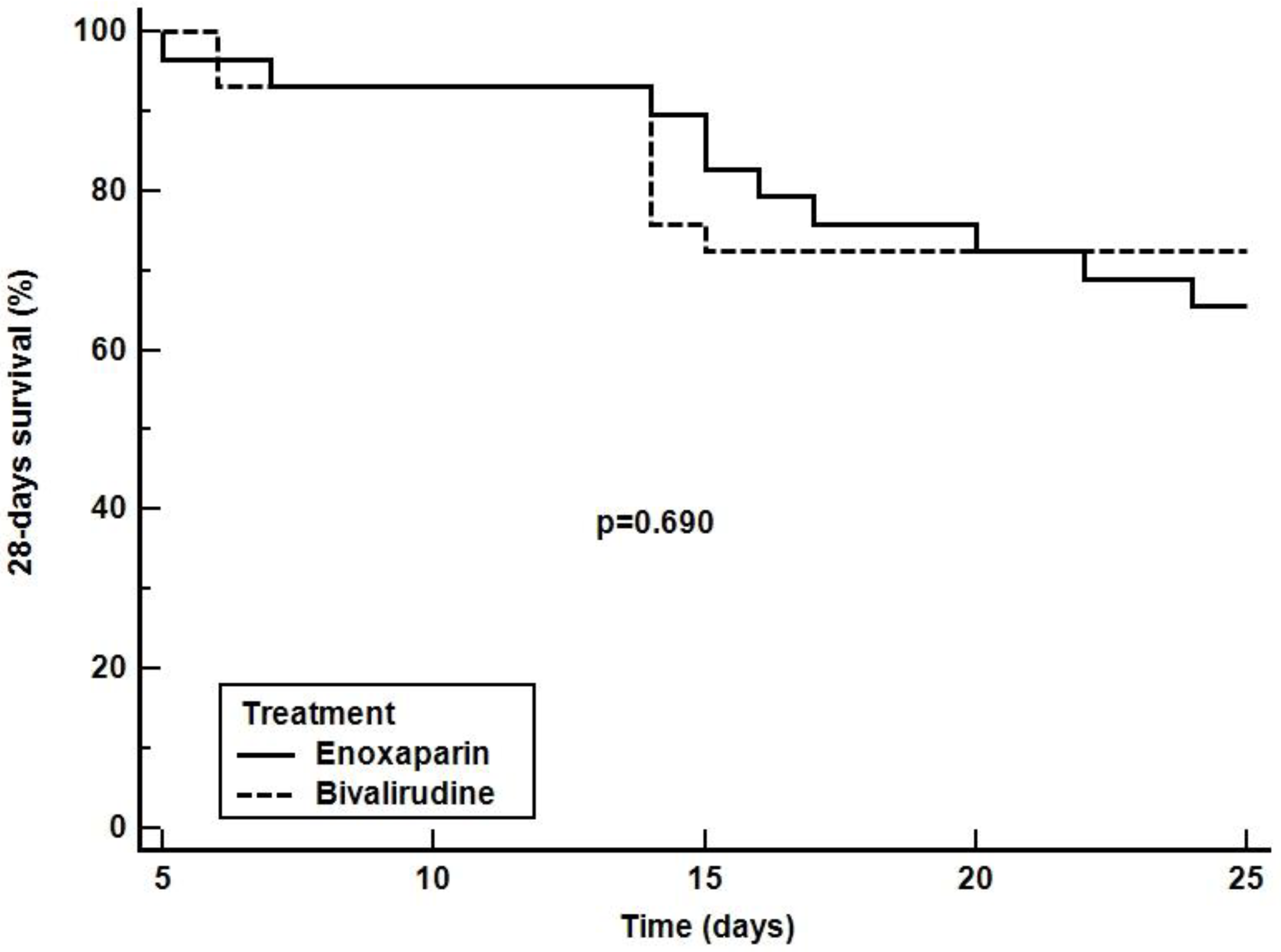
3.1. Primary Outcome
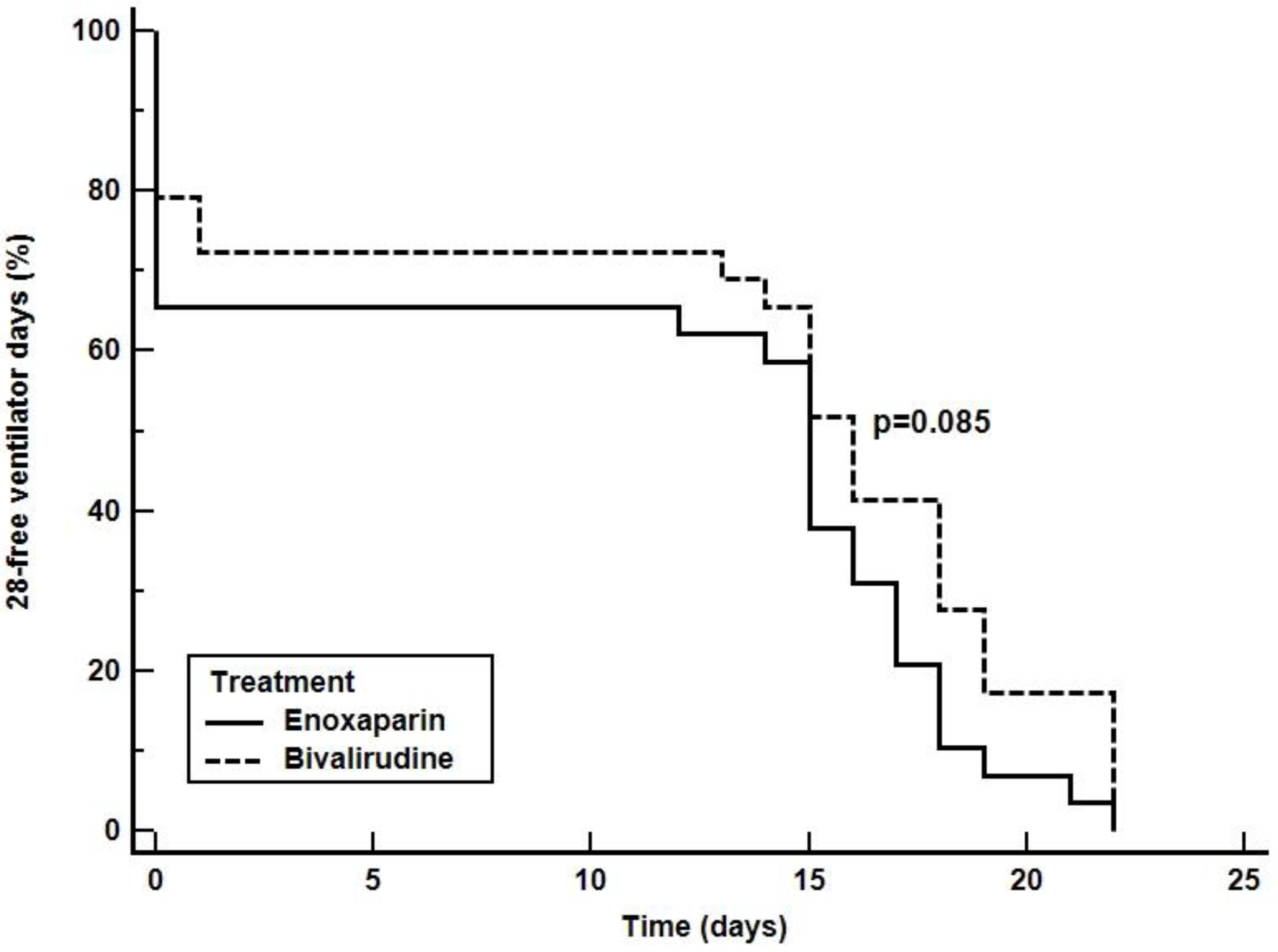
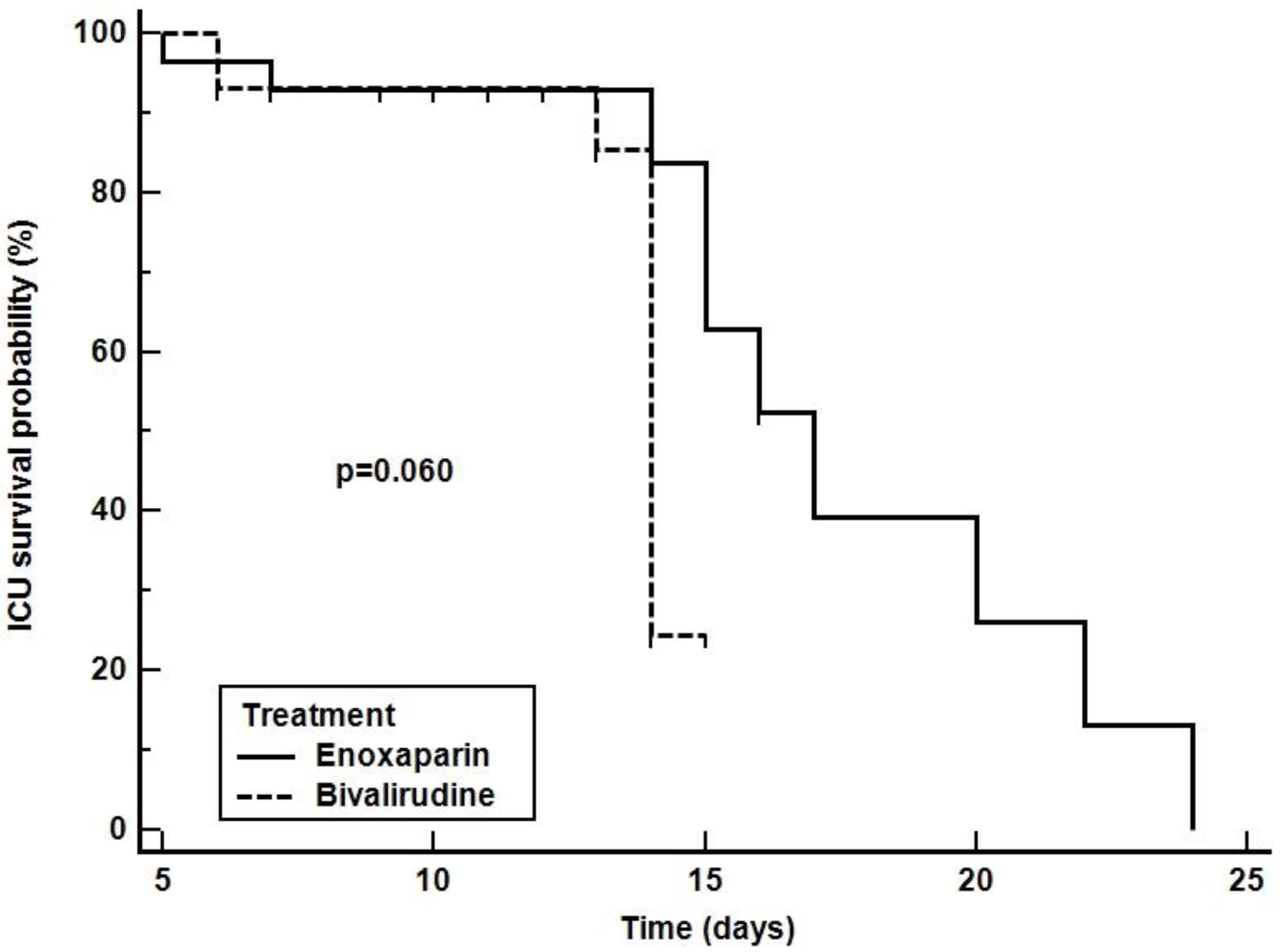
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABGs | Arterial Blood Gases |
| aPTT | activated Partial Thromboplastin Time |
| COVID-19 | CoronaVirus 2019 Disease |
| ECMO | Extra-Corporeal Membrane Oxygenation |
| FiO2 | inspired oxygen fraction |
| GFR | Glomerular Filtrate Rate |
| HIT | heparin-induced thrombocytopenia |
| ICU | Intensive Care Unit |
| PaCO2 | arterial partial pressure of carbon dioxide |
| PaO2 | arterial partial pressure of oxygen |
| PaO2/FiO2 | arterial partial pressure to inspired oxygen fraction ratio |
| PT-INR | Pro-Thrombin International Normalized Ratio |
| SAPS-II | Simplified Acute Physiology Score II |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SOFA | Sequential Organ Failure Assessment |
| SpO2 | peripheral oxygen saturation |
References
- Song, P.; Li, W.; Xie, J.; Hou, Y.; You, C. Cytokine storm induced by SARS-CoV-2. Clin. Chim. Acta 2020, 509, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Spiezia, L.; Boscolo, A.; Poletto, F.; Cerruti, L.; Tiberio, I.; Campello, E.; Navalesi, P.; Simioni, P. COVID-19-Related Severe Hypercoagulability in Patients Admitted to Intensive Care Unit for Acute Respiratory Failure. Thromb. Haemost. 2020, 120, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bruni, A.; Garofalo, E.; Zuccala, V.; Curro, G.; Torti, C.; Navarra, G.; De Sarro, G.; Navalesi, P.; Longhini, F.; Ammendola, M. Histopathological findings in a COVID-19 patient affected by ischemic gangrenous cholecystitis. World J. Emerg. Surg. 2020, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- Zubair, A.S.; McAlpine, L.S.; Gardin, T.; Farhadian, S.; Kuruvilla, D.E.; Spudich, S. Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review. JAMA Neurol. 2020, 77, 1018–1027. [Google Scholar] [CrossRef]
- Promenzio, L.; Arcangeli, F.; Cortis, E.; Sama, E.; Longhini, F. Erythema Pernio-Like in Four Adolescents in the Era of the Coronavirus-2 Infection. Rev. Recent Clin. Trials 2021, 16, 216–219. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Du, C.; Zhang, Y.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botta, C.; Indrieri, A.; Garofalo, E.; Biamonte, F.; Bruni, A.; Pasqua, P.; Cesario, F.; Costanzo, F.S.; Longhini, F.; Mendicino, F. COVID-19: High-JAKing of the Inflammatory “Flight” by Ruxolitinib to Avoid the Cytokine Storm. Front. Oncol. 2020, 10, 599502. [Google Scholar] [CrossRef] [PubMed]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B.; et al. Drug treatments for covid-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Gupta, A.; Jimenez, D.; Burton, J.R.; Der Nigoghossian, C.; Chuich, T.; Nouri, S.N.; Dreyfus, I.; Driggin, E.; et al. Pharmacological Agents Targeting Thromboinflammation in COVID-19: Review and Implications for Future Research. Thromb. Haemost. 2020, 120, 1004–1024. [Google Scholar] [PubMed]
- Cattaneo, M.; Bertinato, E.M.; Birocchi, S.; Brizio, C.; Malavolta, D.; Manzoni, M.; Muscarella, G.; Orlandi, M. Pulmonary Embolism or Pulmonary Thrombosis in COVID-19? Is the Recommendation to Use High-Dose Heparin for Thromboprophylaxis Justified? Thromb. Haemost. 2020, 120, 1230–1232. [Google Scholar] [CrossRef]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Pano-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef]
- Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N.; Carrier, M.; Reynolds, H.R.; Kumar, A.; Turgeon, A.F.; et al. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [PubMed]
- Marietta, M.; Ageno, W.; Artoni, A.; De Candia, E.; Gresele, P.; Marchetti, M.; Marcucci, R.; Tripodi, A. COVID-19 and haemostasis: A position paper from Italian Society on Thrombosis and Haemostasis (SISET). Blood Transfus. 2020, 18, 167–169. [Google Scholar]
- Nadkarni, G.N.; Lala, A.; Bagiella, E.; Chang, H.L.; Moreno, P.R.; Pujadas, E.; Arvind, V.; Bose, S.; Charney, A.W.; Chen, M.D.; et al. Anticoagulation, Bleeding, Mortality, and Pathology in Hospitalized Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1815–1826. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [Green Version]
- Carroll, R.C.; Craft, R.M.; Whitaker, G.L.; Snider, C.C.; Kirby, R.K.; Elder, R.F.; Hennessey, M.D. Thrombelastography monitoring of resistance to enoxaparin anticoagulation in thrombophilic pregnancy patients. Thromb. Res. 2007, 120, 367–370. [Google Scholar] [CrossRef]
- Kaya, A.; Uzunhasan, I.; Ataoglu, H.E.; Turhan, N.; Baskurt, M.; Hatemi, A.; Ozkan, A.A.; Okcun, B.; Yigit, Z. Role of enoxaparin resistance in recurrent chest pain in the intensive care unit. J. Int. Med. Res. 2009, 37, 1436–1442. [Google Scholar] [CrossRef]
- Warkentin, T.E. Bivalent direct thrombin inhibitors: Hirudin and bivalirudin. Best Pract. Res. Clin. Haematol. 2004, 17, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Seelhammer, T.G.; Rowse, P.; Yalamuri, S. Bivalirudin for Maintenance Anticoagulation During Venovenous Extracorporeal Membrane Oxygenation for COVID-19. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Trigonis, R.; Smith, N.; Porter, S.; Anderson, E.; Jennings, M.; Kapoor, R.; Hage, C.; Moiz, S.; Garcia, J.; Rahman, O. Efficacy of Bivalirudin for Therapeutic Anticoagulation in COVID-19 Patients Requiring ECMO Support. J. Cardiothorac. Vasc. Anesth. 2022, 36, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Moller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Ng Gong, M.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef]
- Cammarota, G.; Vaschetto, R.; Azzolina, D.; De Vita, N.; Olivieri, C.; Ronco, C.; Longhini, F.; Bruni, A.; Colombo, D.; Pissaia, C.; et al. Early extubation with immediate non-invasive ventilation versus standard weaning in intubated patients for coronavirus disease 2019: A retrospective multicenter study. Sci. Rep. 2021, 11, 13418. [Google Scholar] [CrossRef]
- Longhini, F.; Maugeri, J.; Andreoni, C.; Ronco, C.; Bruni, A.; Garofalo, E.; Pelaia, C.; Cavicchi, C.; Pintaudi, S.; Navalesi, P. Electrical impedance tomography during spontaneous breathing trials and after extubation in critically ill patients at high risk for extubation failure: A multicenter observational study. Ann. Intensive Care 2019, 9, 88. [Google Scholar] [CrossRef] [Green Version]
- Vaschetto, R.; Longhini, F.; Persona, P.; Ori, C.; Stefani, G.; Liu, S.; Yi, Y.; Lu, W.; Yu, T.; Luo, X.; et al. Early extubation followed by immediate noninvasive ventilation vs. standard extubation in hypoxemic patients: A randomized clinical trial. Intensive Care Med. 2019, 45, 62–71. [Google Scholar] [CrossRef]
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; Hess, D.; Hill, N.S.; Nava, S.; Navalesi, P.M.O.T.S.C.; Antonelli, M.; Brozek, J.; Conti, G.; et al. Official ERS/ATS clinical practice guidelines: Noninvasive ventilation for acute respiratory failure. Eur Respir. J. 2017, 50, 1602426. [Google Scholar] [CrossRef] [Green Version]
- Oczkowski, S.; Ergan, B.; Bos, L.; Chatwin, M.; Ferrer, M.; Gregoretti, C.; Heunks, L.; Frat, J.P.; Longhini, F.; Nava, S.; et al. ERS clinical practice guidelines: High-flow nasal cannula in acute respiratory failure. Eur. Respir. J. 2022, 59, 2101574. [Google Scholar] [CrossRef]
- Maggiore, S.M.; Jaber, S.; Grieco, D.L.; Mancebo, J.; Zakynthinos, S.; Demoule, A.; Ricard, J.D.; Navalesi, P.; Vaschetto, R.; Hraiech, S.; et al. High-Flow Versus VenturiMask Oxygen Therapy to Prevent Re-Intubation in Hypoxemic Patients After Extubation: A Multicenter, Randomized Clinical Trial. Am. J. Respir. Crit. Care Med. 2022. [Google Scholar] [CrossRef]
- Yehya, N.; Harhay, M.O.; Curley, M.A.Q.; Schoenfeld, D.A.; Reeder, R.W. Reappraisal of Ventilator-Free Days in Critical Care Research. Am. J. Respir. Crit. Care Med. 2019, 200, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Barbar, S.; Noventa, F.; Rossetto, V.; Ferrari, A.; Brandolin, B.; Perlati, M.; De Bon, E.; Tormene, D.; Pagnan, A.; Prandoni, P. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: The Padua Prediction Score. J. Thromb. Haemost. 2010, 8, 2450–2457. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.X.; Xu, J.L.; Mao, Q.X.; Liu, R.; Zhang, W.Y.; Qian, H.Y.; Xu, L. Association of Padua prediction score with in-hospital prognosis in COVID-19 patients. QJM 2020, 113, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Rindi, L.V.; Al Moghazi, S.; Donno, D.R.; Cataldo, M.A.; Petrosillo, N. Predictive scores for the diagnosis of Pulmonary Embolism in COVID-19: A systematic review. Int. J. Infect. Dis. 2022, 115, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivosecchi, R.M.; Arakelians, A.R.; Ryan, J.; Murray, H.; Ramanan, R.; Gomez, H.; Phillips, D.; Sciortino, C.; Arlia, P.; Freeman, D.; et al. Comparison of Anticoagulation Strategies in Patients Requiring Venovenous Extracorporeal Membrane Oxygenation: Heparin Versus Bivalirudin. Crit. Care Med. 2021, 49, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Agracheva, N.; Di Prima, A.L.; Nisi, T.; De Bonis, M.; Isella, F.; Zangrillo, A.; Pappalardo, F. Primary anticoagulation with bivalirudin for patients with implantable ventricular assist devices. Artif. Organs 2014, 38, 342–346. [Google Scholar] [CrossRef]
- Pieri, M.; Agracheva, N.; Bonaveglio, E.; Greco, T.; De Bonis, M.; Covello, R.D.; Zangrillo, A.; Pappalardo, F. Bivalirudin versus heparin as an anticoagulant during extracorporeal membrane oxygenation: A case-control study. J. Cardiothorac. Vasc. Anesth. 2013, 27, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Quaggiotti, L.; Fominskiy, E.; Landoni, G.; Calabro, M.G.; Ajello, S.; Bonizzoni, M.A.; Belletti, A.; Scandroglio, A.M. Anticoagulation Strategies in Critically Ill Patients With SARS-CoV-2 Infection: The Role of Direct Thrombin Inhibitors. J. Cardiothorac. Vasc. Anesth. 2022, 36, 2961–2967. [Google Scholar] [CrossRef]
- McCall, P.J.; Willder, J.M.; Stanley, B.L.; Messow, C.M.; Allan, J.; Gemmell, L.; Puxty, A.; Strachan, D.; Berry, C.; Shelley, B.G. Right ventricular dysfunction in patients with COVID-19 pneumonitis whose lungs are mechanically ventilated: A multicentre prospective cohort study. Anaesthesia 2022, 77, 772–784. [Google Scholar] [CrossRef] [PubMed]
- Serapide, F.; Quirino, A.; Scaglione, V.; Morrone, H.L.; Longhini, F.; Bruni, A.; Garofalo, E.; Matera, G.; Marascio, N.; Scarlata, G.G.M.; et al. Is the Pendulum of Antimicrobial Drug Resistance Swinging Back after COVID-19? Microorganisms 2022, 10, 957. [Google Scholar] [CrossRef] [PubMed]
- Vaschetto, R.; Turucz, E.; Dellapiazza, F.; Guido, S.; Colombo, D.; Cammarota, G.; Della Corte, F.; Antonelli, M.; Navalesi, P. Noninvasive ventilation after early extubation in patients recovering from hypoxemic acute respiratory failure: A single-centre feasibility study. Intensive Care Med. 2012, 38, 1599–1606. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Schunemann, H.J.; Angchaisuksiri, P.; Blair, C.; Dane, K.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; Kahn, S.R.; et al. American Society of Hematology living guidelines on the use of anticoagulation for thromboprophylaxis for patients with COVID-19: March 2022 update on the use of anticoagulation in critically ill patients. Blood Adv. 2022, 6, 4975–4982. [Google Scholar] [CrossRef] [PubMed]
- ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 2-care pathways, treatment, and follow-up. Cardiovasc. Res. 2022, 118, 1618–1666. [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bivalirudin (n = 29) | Enoxaparin (n = 29) | p Value | |
|---|---|---|---|
| Age (years) | 65 [58; 71] | 60 [52; 69] | 0.249 |
| Male-n (%) | 13 (44.8%) | 18 (62.1%) | 0.864 |
| BMI (kg/m2) | 27.7 [25.6; 31.6] | 27.0 [24.7; 29.4] | 0.591 |
| SAPS-II | 55 [50; 60] | 56 [51; 60] | 0.779 |
| SOFA | 11 [8; 12] | 8 [7; 12] | 0.117 |
| Padua Score | 6 [5; 6] | 5 [5; 6] | 0.076 |
| Hemodynamic | |||
| HR (beats/min) | 70 [61; 89] | 84 [60; 100] | 0.256 |
| MAP (mmHg) | 89 [80; 96] | 89 [83; 95] | 0.669 |
| Need for norepinephrine-n (%) | 15 (51.7%) | 11 (37.9%) | 0.689 |
| Norepinephrine (mcg*kg/min) | 0.3 [0.2; 0.4] | 0.4 [0.3; 0.5] | 0.119 |
| Mechanical ventilation | |||
| Controlled Volume Mode | 29 (100%) | 29 (100%) | >0.999 |
| PEEP (cmH2O) | 10 [8; 10] | 10 [8; 12] | 0.254 |
| Tidal Volume (ml) | 440 [415; 475] | 430 [405; 465] | 0.988 |
| Driving Pressure (cmH2O) | 10 [9; 11] | 10 [8; 11] | 0.338 |
| Static Compliance | 48.9 [39.6; 56.1] | 44.4 [39.6; 52.0] | 0.371 |
| Prone Position-n (%) | 20 (69.0%) | 19 (65.5%) | 0.089 |
| Arterial Blood Gases | |||
| pH | 7.37 [7.37; 7.42] | 7.40 [7.37; 7.43] | 0.287 |
| PaCO2 (mmHg) | 41.4 [38.3; 45.5] | 39.2 [38.0; 45.3] | 0.560 |
| PaO2/FiO2 | 140 [124; 152] | 143 [134; 165] | 0.202 |
| HCO3 (mMol/L) | 24.3 [22.9; 26.1] | 24.5 [23.9; 26.2] | 0.455 |
| Lac (mMol/L) | 1.7 [1.0; 2.4] | 1.5 [0.9; 2.4] | 0.834 |
| Blood tests | |||
| Platelets count | 248 [182; 314] | 247 [163; 347] | 0.726 |
| aPTT | 33 [30; 38] | 33 [29; 36] | 0.662 |
| PT | 12 [11; 13] | 12 [11; 13] | 0.949 |
| INR | 1.10 [1.02; 1.19] | 1.10 [1.01; 1.17] | 0.774 |
| D-dimer | 7.65 [4.25; 13.32] | 8.03 [5.45; 14.24] | 0.854 |
| Fibrinogen | 428 [357; 625] | 548 [377; 743] | 0.107 |
| Procalcitonin | 3.49 [0.18; 10.21] | 1.72 [0.15; 7.04] | 0.648 |
| C-Reactive Protein | 64.5 [25.0; 127.0] | 78.2 [37.1; 138.5] | 0.565 |
| Comorbidities-n (%) | |||
| Chronic Respiratory Failure | 8 (27.6%) | 5 (17.2%) | 0.530 |
| Cardiovascular disease | 9 (31.0%) | 6 (20.7%) | 0.550 |
| Arterial Hypertension | 12 (41.4%) | 11 (37.9%) | 0.999 |
| Diabetes | 4 (13.8%) | 3 (10.3%) | 0.999 |
| Hypothyroidism | 2 (6.7%) | 3 (10.3%) | 0.999 |
| Hyperthyroidism | 3 (10.3%) | 4 (13.8%) | 0.999 |
| Bivalirudin (n = 29) | Enoxaparin (n = 29) | p Value | |
|---|---|---|---|
| Thrombo-embolic complications | 5 (17.2) | 15 (51.7) | 0.012 |
| Thrombotic complications | 3 (10.3) | 10 (34.5) | 0.056 |
| Embolic complications | 2 (6.9) | 5 (17.2) | 0.423 |
| Tracheostomy | 4 (13.8) | 6 (20.7) | 0.730 |
| Reintubation | 4 (13.8) | 4 (13.8) | 0.999 |
| 28-free ventilation days (days) | 15 [0; 17] | 16 [1; 19] | 0.162 |
| ICU Length of Stay (days) | 14 [12; 14] | 15 [13; 15] | 0.076 |
| ICU Mortality n (%) | 8 (27.6) | 10 (34.5) | 0.777 |
| 28-days mortality n (%) | 8 (27.6) | 10 (34.5) | 0.777 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garofalo, E.; Cammarota, G.; Neri, G.; Macheda, S.; Biamonte, E.; Pasqua, P.; Guzzo, M.L.; Longhini, F.; Bruni, A., on behalf of the BivaCOVID authors. Bivalirudin vs. Enoxaparin in Intubated COVID-19 Patients: A Pilot Multicenter Randomized Controlled Trial. J. Clin. Med. 2022, 11, 5992. https://doi.org/10.3390/jcm11205992
Garofalo E, Cammarota G, Neri G, Macheda S, Biamonte E, Pasqua P, Guzzo ML, Longhini F, Bruni A on behalf of the BivaCOVID authors. Bivalirudin vs. Enoxaparin in Intubated COVID-19 Patients: A Pilot Multicenter Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(20):5992. https://doi.org/10.3390/jcm11205992
Chicago/Turabian StyleGarofalo, Eugenio, Gianmaria Cammarota, Giuseppe Neri, Sebastiano Macheda, Eugenio Biamonte, Pino Pasqua, Maria Laura Guzzo, Federico Longhini, and Andrea Bruni on behalf of the BivaCOVID authors. 2022. "Bivalirudin vs. Enoxaparin in Intubated COVID-19 Patients: A Pilot Multicenter Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 20: 5992. https://doi.org/10.3390/jcm11205992