
Occupational Disruptions during the COVID-19 Pandemic and Their Association with Healthcare Workers’ Mental Health


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Occupational Environment and Disruptions
3.2. Predictors of Occupational Change
3.3. Predictors of Individual Preparedness
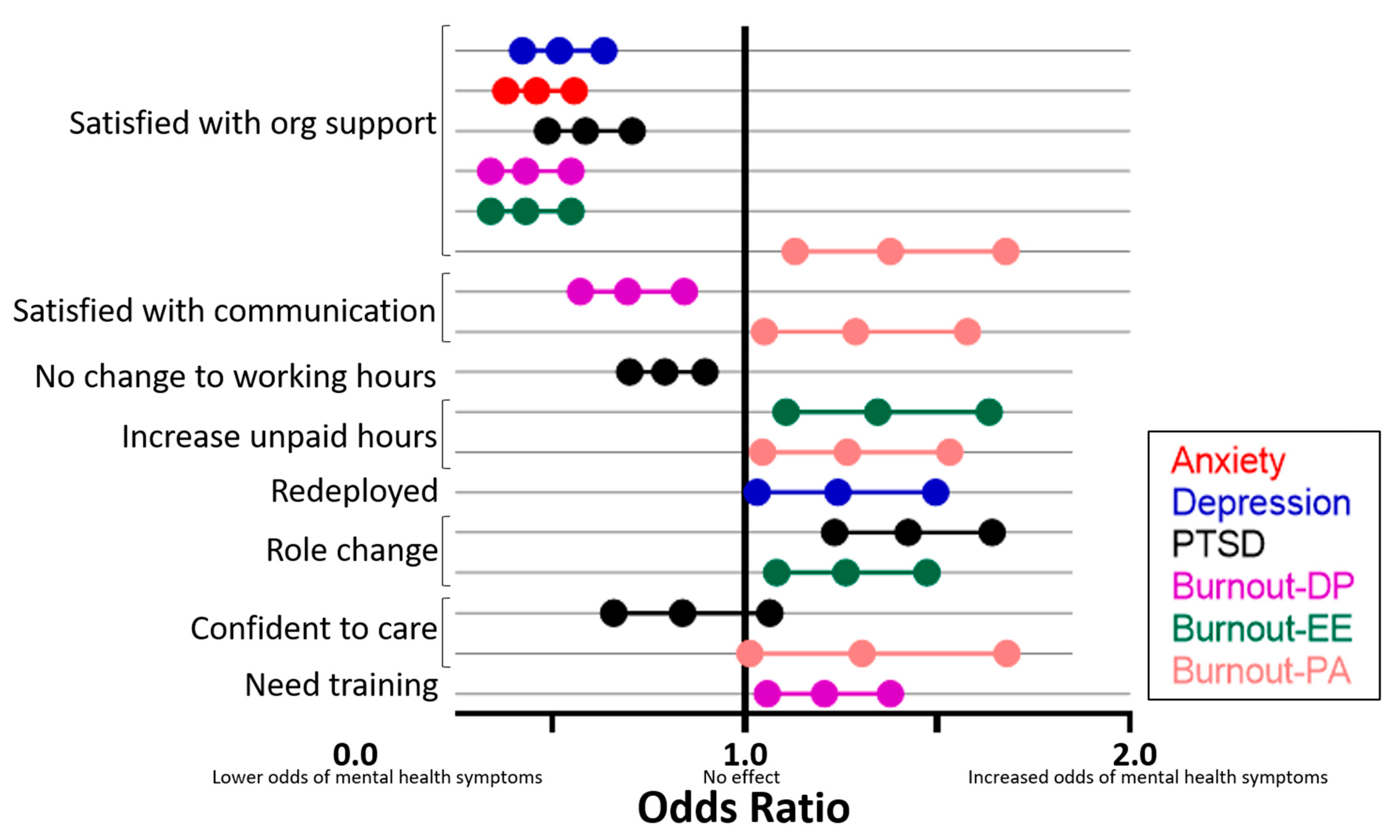
3.4. Occupational Change and Mental Health
4. Discussion
4.1. Prevalence of Occupational Change and Individual Preparedness
4.2. Impact on Mental Health
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Butt, C. Ten Graphs that Show the Rise and Fall of Victoria’s COVID-19-Second Wave; Age: Melbourne, Australia, 2020. [Google Scholar]
- Murray-Atfield, Y.; Dunstan, J. Melbourne Placed under Stage 4 Lockdown, 8pm Curfew, Regional Victoria Moved to Stage 3 Restrictions; Australian Broadcasting Corporation: Sydney, Australia, 2020; 8p. [Google Scholar]
- Australian Bureau of Statistics. Household Impacts of COVID-19 Survey 1–6 April 2020. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/household-impacts-covid-19-survey/1-6-apr-2020 (accessed on 6 April 2021).
- Newby, J.M.; O’Moore, K.; Tang, S.; Christensen, H.; Faasse, K. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS ONE 2020, 15, e0236562. [Google Scholar] [CrossRef]
- Wright, L.; Steptoe, A.; Fancourt, D. Are we all in this together? Longitudinal assessment of cumulative adversities by socioeconomic position in the first 3 weeks of lockdown in the UK. J. Epidemiol. Community Health 2020, 74, 683. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.; Steptoe, A.; Fancourt, D. Are adversities and worries during the COVID-19 pandemic related to sleep quality? Longitudinal analyses of 48,000 UK adults. medRxiv 2020, 16, e0248919. [Google Scholar]
- Panda, N.; Sinyard, R.D.; Henrich, N.; Cauley, C.E.; Hannenberg, A.A.; Sonnay, Y.; Bitton, A.; Brindle, M.; Molina, G. Redeployment of Health Care Workers in the COVID-19 Pandemic: A Qualitative Study of Health System Leaders’ Strategies. J. Patient Saf. 2021, 17, 256–263. [Google Scholar] [CrossRef]
- Johnston, K.; Tyson, C.; Danny, I.; Meyer, L. Impact of the COVID-19 pandemic on the career of junior doctors. Med. J. Aust. 2021, 214, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Tibandebage, P.; Kida, T.; Mackintosh, M.; Ikingura, J. Can managers empower nurse-midwives to improve maternal health care? A comparison of two resource-poor hospitals in Tanzania. Int. J. Health Plan. Manag. 2016, 31, 379–395. [Google Scholar] [CrossRef] [Green Version]
- Lim, G.H.; Lim, B.L.; Vasu, A. Survey of factors affecting health care workers’ perception towards institutional and individual disaster preparedness. Prehospital Disaster Med. 2013, 28, 353–358. [Google Scholar] [CrossRef]
- Good, L. Addressing hospital nurses’ fear of abandonment in a bioterrorism emergency. AAOHN J. Off. J. Am. Assoc. Occup. Health Nurses 2007, 55, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Riley, M.R.; Mohr, D.C.; Waddimba, A.C. The reliability and validity of three-item screening measures for burnout: Evidence from group-employed health care practitioners in upstate New York. Stress Health 2018, 34, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Thoresen, S.; Tambs, K.; Hussain, A.; Heir, T.; Johansen, V.; Bisson, J. Brief measure of posttraumatic stress reactions: Impact of Event Scale-6. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 45, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development Environment for R. 2015. Available online: http://www.rstudio.com/ (accessed on 8 July 2021).
- Australian Institute of Health and Welfare. Health Workforce; Australian Institute of Health and Welfare: Canberra, Australia, 2020. Available online: https://www.aihw.gov.au/reports/australias-health/health-workforce (accessed on 14 February 2021).
- Medical Board of Australia. Registration Data Table—December 2020. Available online: https://www.medicalboard.gov.au/news/statistics.aspx (accessed on 28 April 2021).
- Nursing and Midwifery Board. Nursing and Midwifery Board of Australia Registrant Data. Available online: https://www.nursingmidwiferyboard.gov.au/about/statistics.aspx (accessed on 4 May 2021).
- Rimmer, A. Over 80% of doctors work unpaid overtime, NHS survey shows. BMJ 2015, 350, h1086. [Google Scholar] [CrossRef]
- Tsai, Y.-H.; Huang, N.; Chien, L.-Y.; Chiang, J.-H.; Chiou, S.-T. Work hours and turnover intention among hospital physicians in Taiwan: Does income matter? BMC Health Serv. Res. 2016, 16, 667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrie, K.; Crawford, J.; LaMontagne, A.D.; Milner, A.; Dean, J.; Veness, B.G.; Christensen, H.; Harvey, S.B. Working hours, common mental disorder and suicidal ideation among junior doctors in Australia: A cross-sectional survey. BMJ Open 2020, 10, e033525. [Google Scholar] [CrossRef] [Green Version]
- Fair Work Ombudsman, Unpaid Work Fact Sheet. 2017. Available online: https://www.fairwork.gov.au/tools-and-resources/fact-sheets/unpaid-work/unpaid-work-unpaid-work (accessed on 11 June 2021).
- Daly, N.; Robb, K. Junior doctors to launch new class action claiming unrostered, unpaid overtime. ABC News, 19 May 2021. Available online: https://www.abc.net.au/news/2021-05-19/junior-doctors-new-class-action-claiming-unpaid-overtime/100147606(accessed on 11 June 2021).
- ABC News. Victorian Schools Return for Term Two Online during Coronavirus Pandemic. 2020. Available online: https://www.abc.net.au/news/2020-04-15/coronavirus-sends-victorian-schools-online-for-term-two/12149390 (accessed on 6 April 2021).
- McHugh, M.D. Hospital nurse staffing and public health emergency preparedness: Implications for policy. Public Health Nurs. 2010, 27, 442–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, F.; Kyratsis, Y. Emergency nurse disaster preparedness during mass gatherings: A cross-sectional survey of emergency nurses’ perceptions in hospitals in Mecca, Saudi Arabia. BMJ Open 2017, 7, e013563. [Google Scholar] [CrossRef] [Green Version]
- Mosca, N.W.; Sweeney, P.M.; Hazy, J.M.; Brenner, P. Assessing bioterrorism and disaster preparedness training needs for school nurses. J. Public Health Manag. Pract. JPHMP 2005, 11, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Veenema, T.G.; Griffin, A.; Gable, A.R.; MacIntyre, L.; Simons, R.N.; Couig, M.P.; Walsh, J.J., Jr.; Lavin, R.P.; Dobalian, A.; Larson, E. Nurses as Leaders in Disaster Preparedness and Response—A Call to Action. J. Nurs. Scholarsh. Off. Publ. Sigma Tau Int. Honor. Soc. Nurs. 2016, 48, 187–200. [Google Scholar] [CrossRef]
- Farra, S.L.; Smith, S.; Bashaw, M.A. Learning Outcome Measurement in Nurse Participants After Disaster Training. Disaster Med. Public Health Prep. 2016, 10, 728–733. [Google Scholar] [CrossRef]
- Rudy, S.J.; Polomano, R.; Murray, W.B.; Henry, J.; Marine, R. Team management training using crisis resource management results in perceived benefits by healthcare workers. J. Contin. Educ. Nurs. 2007, 38, 219–226. [Google Scholar] [CrossRef] [PubMed]
- VanDevanter, N.; Raveis, V.H.; Kovner, C.T.; McCollum, M.; Keller, R. Challenges and Resources for Nurses Participating in a Hurricane Sandy Hospital Evacuation. J. Nurs. Scholarsh. Off. Publ. Sigma Tau Int. Honor. Soc. Nurs. 2017, 49, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Vanhaecht, K.; Seys, D.; Bruyneel, L.; Cox, B.; Kaesemans, G.; Cloet, M.; van den Broeck, K.; Cools, O.; de Witte, A.; Lowet, K.; et al. COVID-19 is having a destructive impact on health-care workers’ mental well-being. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2021, 33, 1–6. [Google Scholar]
- De Leo, A.; Cianci, E.; Mastore, P.; Gozzoli, C. Protective and Risk Factors of Italian Healthcare Professionals during the COVID-19 Pandemic Outbreak: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 453. [Google Scholar] [CrossRef]
- Al Knawy, B.A.; Al-Kadri, H.M.F.; Elbarbary, M.; Arabi, Y.; Balkhy, H.H.; Clark, A. Perceptions of postoutbreak management by management and healthcare workers of a Middle East respiratory syndrome outbreak in a tertiary care hospital: A qualitative study. BMJ Open 2019, 9, e017476. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.-C.; Chen, T.-F.; Chou, S.-M. SARS: Key factors in crisis management. J. Nurs. Res. JNR 2005, 13, 58–65. [Google Scholar] [CrossRef]
- Shih, F.-J.; Turale, S.; Lin, Y.-S.; Gau, M.-L.; Kao, C.-C.; Yang, C.-Y.; Liao, Y.-C. Surviving a life-threatening crisis: Taiwan’s nurse leaders’ reflections and difficulties fighting the SARS epidemic. J. Clin. Nurs. 2009, 18, 3391–3400. [Google Scholar] [CrossRef] [PubMed]
- Lau, M.W.; Li, W.E.; Llewellyn, A.; Cyna, A.M. Prevalence and associations of psychological distress in Australian junior medical officers. Intern. Med. J. 2017, 47, 1190–1196. [Google Scholar] [CrossRef]
- Mellins, C.A.; Mayer, L.E.S.; Glasofer, D.R.; Devlin, M.J.; Albano, A.M.; Nash, S.S.; Engle, E.; Cullen, C.; Ng, W.Y.K.; Allmann, A.E.; et al. Supporting the well-being of health care providers during the COVID-19 pandemic: The CopeColumbia response. Gen. Hosp. Psychiatry 2020, 67, 62–69. [Google Scholar] [CrossRef]
- Doobay-Persaud, A.; Evert, J.; DeCamp, M.; Evans, C.T.; Jacobsen, K.H.; Sheneman, N.E.; Goldstein, J.L.; Nelson, B.D. Extent, nature and consequences of performing outside scope of training in global health. Glob. Health 2019, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.; Landivar, L.C.; Ruppanner, L.; Scarborough, W.J. COVID-19 and the Gender Gap in Work Hours. Gend. Work Organ. 2020, 28, 101–112. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Household Impacts of COVID-19 Survey: Coronavirus (COVID-19) Impacts on Jobs, Unpaid Care, Domestic Work, Mental Health and Related Services, and Life after COVID-19 Restrictions; Australian Bureau of Statistics: Canberra, Australia, 2020. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/household-impacts-covid-19-survey/6-10-july-2020 (accessed on 6 April 2021).
- Dobson, H.; Malpas, C.B.; Burrell, A.J.C.; Gurvich, C.; Chen, L.; Kulkarni, J.; Winton-Brown, T. Burnout and psychological distress amongst Australian healthcare workers during the COVID-19 pandemic. Australas. Psychiatry 2020, 29, 26–30. [Google Scholar] [CrossRef]
- Hines, S.E.; Chin, K.H.; Glick, D.R.; Wickwire, E.M. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Hollingsworth, C.E.; Wesley, C.; Huckridge, J.; Finn, G.M.; Griksaitis, M.J. Impact of child death on paediatric trainees. Arch. Dis. Child. 2018, 103, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.V.; Naumann, D.N.; Fellows, J.L.; Bowley, D.M.; Suggett, N. Post-traumatic stress disorder amongst surgical trainees: An unrecognised risk? Surg. J. R. Coll. Surg. Edinb. Irel. 2017, 15, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Leinweber, J.; Creedy, D.K.; Rowe, H.; Gamble, J. Responses to birth trauma and prevalence of posttraumatic stress among Australian midwives. Women Birth J. Aust. Coll. Midwives 2017, 30, 40–45. [Google Scholar] [CrossRef]
- Imo, U.O. Burnout and psychiatric morbidity among doctors in the UK: A systematic literature review of prevalence and associated factors. BJPsych Bull. 2017, 41, 197–204. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Frequency (n = 7846) | Percent (%) |
|---|---|---|
| Age (years) | ||
| 20–30 | 1860 | 23.7 |
| 31–40 | 2250 | 28.7 |
| 41–50 | 1738 | 22.2 |
| >50 | 1998 | 25.5 |
| Gender | ||
| Male | 1458 | 18.6 |
| Female | 6344 | 80.9 |
| Non-binary | 19 | 0.2 |
| Prefer not to say | 25 | 0.3 |
| State | ||
| Victoria | 6685 | 85.2 |
| All other Australian states | 1161 | 14.8 |
| Location of practice | ||
| Metropolitan | 6373 | 81.2 |
| Regional | 1407 | 17.9 |
| Remote | 66 | 0.8 |
| Occupation | ||
| Nursing | 3088 | 39.4 |
| Medical * | 2436 | 31.1 |
| Allied health | 1314 | 16.7 |
| Administrative staff | 485 | 6.2 |
| Other roles ** | 523 | 6.7 |
| Characteristic | Frequency (n = 7846) | Percent (%) |
|---|---|---|
| Employment status BEFORE pandemic | ||
| Full-time | 3783 | 48.2 |
| Part-time | 3654 | 46.6 |
| Casual/other | 409 | 5.2 |
| CURRENT employment status | ||
| Full-time | 3818 | 48.7 |
| Part-time | 3642 | 46.4 |
| Casual/other | 386 | 4.9 |
| Change in work status (full-time, part-time, or casual) * | ||
| Step up in work status | 400 | 5.1 |
| Step down in work status | 354 | 4.5 |
| Health organisation type | ||
| Public | 5605 | 76.8 |
| Community | 1140 | 15.6 |
| Private | 260 | 3.6 |
| Other ** | 293 | 4.0 |
| Any change in working hours since the pandemic commenced *** | ||
| Increased paid work hours | 1634 | 20.8 |
| Increased unpaid work hours | 1686 | 21.5 |
| Decreased paid or unpaid work hours | 886 | 11.3 |
| No change | 4039 | 51.5 |
| Household income altered due to COVID-19 pandemic | ||
| Increased | 820 | 10.5 |
| Decreased | 2415 | 30.8 |
| No change | 4611 | 58.8 |
| Concerned about household income due to COVID-19 pandemic | 2416 | 30.8 |
| Redeployed to a new area of work | 1318 | 16.8 |
| Confidence working in new work area **** | 5.0 | 1.6 |
| Change in work role | 2139 | 27.3 |
| Confidence working in new role **** | 5.2 | 1.3 |
| Received training to care for patients with COVID-19 | 2792 | 35.6 |
| Received training on PPE during the pandemic | 5137 | 65.5 |
| Needs more training regarding PPE or managing people with COVID-19 | 3001 | 50.4 |
| Exposed to confirmed/suspected COVID patients (n = 7832 responses) | 4561 | 58.2 |
| Communication received from the workplace during the pandemic has been useful and timely | ||
| Strongly or somewhat agree | 5833 | 74.4 |
| Neither agree nor disagree | 801 | 10.2 |
| Strongly or somewhat disagree | 1212 | 15.4 |
| Believed their workplace actively supported their well-being and mental health during the pandemic | ||
| Very well or somewhat supported | 5352 | 68.3 |
| Neither supported nor unsupported | 1219 | 15.5 |
| Very or somewhat unsupported | 1275 | 16.2 |
| Characteristics | Increased Paid Hours | Increased Unpaid Hours | Redeployed | Work Role Changed | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Personal predictors | ||||||||
| Female gender | 1.32 (1.08–1.61) | 0.006 | N/A | N/A | 1.20 (1.00–1.44) | 0.046 | ||
| Age (years) | ||||||||
| 20–30 | 1.45 (1.07–1.98) | 0.018 | 1.21 (0.82–1.79) | 0.344 | 1.15 (0.86–1.54) | 0.342 | N/A | |
| 31–40 | 1.36 (1.04–1.77) | 0.023 | 1.28 (0.95–1.72) | 0.105 | 1.11 (0.85–1.44) | 0.446 | N/A | |
| 41–50 | 1.44 (1.16–1.78) | 0.001 | 1.19 (0.94–1.52) | 0.151 | 1.25 (1.00–1.57) | 0.052 | N/A | |
| State (VIC) | 0.98 (0.79–1.21) | 0.838 | 0.83 (0.68–1.02) | 0.077 | N/A | N/A | ||
| Prior mental health condition | N/A | N/A | N/A | 1.23 (1.07–1.42) | 0.004 | |||
| Experienced family or friend infected with COVID-19 | N/A | 1.27 (1.06–1.52) | 0.009 | 1.19 (1.03–1.37) | 0.016 | 1.15 (0.99–1.34) | 0.065 | |
| Number of years’ experience since graduating | ||||||||
| 5–10 | 0.89 (0.72–1.10) | 0.277 | 1.55 (1.13–2.12) | 0.007 | 0.69 (0.56–0.85) | <0.001 | N/A | |
| 11–15 | 0.68 (0.52–0.90) | 0.007 | 2.10 (1.47–2.99) | <0.001 | 0.72 (0.55–0.93) | 0.012 | N/A | |
| ≥15 | 0.79 (0.60–1.04) | 0.089 | 3.02 (2.11–4.32) | <0.001 | 0.66 (0.51–0.86) | 0.002 | N/A | |
| Number of children | ||||||||
| 1–2 | N/A | 1.19 (0.98–1.44) | 0.086 | 0.82 (0.69–0.98) | 0.031 | N/A | ||
| 3+ | N/A | 0.91 (0.64–1.28) | 0.575 | 0.99 (0.74–1.33) | 0.950 | N/A | ||
| Elderly care | ||||||||
| 1–2 | N/A | 0.92 (0.69–1.23) | 0.579 | 0.96 (0.74–1.24) | 0.731 | N/A | ||
| 3+ | N/A | 0.54 (0.12–2.55) | 0.437 | 2.66 (1.24–5.71) | 0.012 | N/A | ||
| Household income altered | ||||||||
| Increased | 0.05 (0.04–0.07) | <0.001 | 0.83 (0.61–1.13) | 0.229 | 0.59 (0.47–0.75) | 0.001 | 0.53 (0.42–0.68) | 0.001 |
| Decreased | 0.05 (0.04–0.06) | <0.001 | 0.77 (0.58–1.03) | 0.079 | 0.56 (0.46–0.68) | 0.001 | 0.40 (0.32–0.49) | 0.001 |
| Has concerns about income | 1.02 (0.85–1.21) | 0.851 | N/A | 1.25 (1.06–1.47) | 0.009 | 1.13 (0.96–1.32) | 0.140 | |
| Professional predictors | ||||||||
| Occupation | ||||||||
| Nursing | 1.37 (1.15–1.63) | 0.001 | 0.54 (0.44- 0.67) | <0.001 | 1.53 (1.29–1.80) | 0.001 | 1.47 (1.21–1.77) | 0.001 |
| Allied health | 0.71 (0.56–0.90) | 0.005 | 0.69 (0.54–0.87) | 0.002 | 1.652 (1.34–2.04) | 0.001 | 1.90 (1.55–2.33) | 0.010 |
| Other roles | 0.96 (0.67–1.38) | 0.814 | 0.75 (0.53–1.08) | 0.120 | 0.97 (0.67–1.42) | 0.882 | 1.54 (1.24–1.93) | 0.001 |
| Frontline area | ||||||||
| ICU | 0.90 (0.70–1.16) | 0.420 | 1.44 (0.79–2.61) | 0.236 | 0.89 (0.65–1.23) | 0.497 | 0.79 (0.47–1.32) | 0.365 |
| Anaesthetics and surgery | 0.51 (0.38- 0.66) | <0.001 | 1.13 (0.69–1.85) | 0.621 | 3.52 (2.67–4.64) | 0.001 | 1.06 (0.73–1.53) | 0.776 |
| Medical specialty areas | 0.70 (0.58–0.85) | <0.001 | 1.83 (1.18–2.84) | 0.007 | 3.53 (2.80–4.46) | 0.001 | 1.03 (0.74–1.42) | 0.878 |
| Other * | 0.87 (0.64–1.18) | 0.375 | 2.89 (1.76–4.75) | 0.001 | 3.24 (2.36–4.46) | 0.001 | 1.33 (0.92–1.92) | 0.130 |
| Primary care, community and residential aged care | 0.77 (0.59–1.00) | 0.051 | 1.84 (1.15–2.93) | 0.011 | 2.44 (1.81–3.29) | 0.001 | 1.21 (0.86–1.69) | 0.272 |
| Currently works with COVID-19 patients | N/A | N/A | 1.90 (1.64–2.21) | 0.001 | N/A | |||
| Anticipates working with COVID-19 patients | N/A | 1.17 (0.98–1.40) | 0.089 | N/A | 1.05 (0.91–1.22) | 0.499 | ||
| Characteristics | Training to Care | Confident to Care for People with COVID-19 | Confident in Using PPE | Need Training | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Personal Predictors | ||||||||
| Female gender | 0.66 (0.58–0.76) | <0.001 | 0.64 (0.51–0.80) | <0.001 | N/A | 1.36 (1.21–1.61) | <0.001 | |
| Age (years) | ||||||||
| 20–30 | 1.00 (0.85–1.17) | 0.996 | 0.80 (0.56–1.16) | 0.248 | 0.80 (0.62–1.03) | 0.082 | 1.64 (1.40–1.94) | <0.001 |
| 31–40 | 0.99 (0.84–1.15) | 0.906 | 0.73 (0.54–1.00) | 0.057 | 0.64 (0.51–0.81) | 0.001 | 1.53 (1.31–1.79) | <0.001 |
| 41–50 | 1.05 (0.88–1.25) | 0.556 | 0.66 (0.51–0.85) | 0.001 | 0.60 (0.46–0.77) | 0.001 | 1.44 (1.22–1.69) | <0.001 |
| State (VIC) | N/A | 1.51 (1.20–1.90) | 0.001 | 1.96 (1.60–2.39) | 0.001 | 0.64 (0.54–0.76) | 0.001 | |
| Has prior mental health condition | N/A | 0.78 (0.65–0.92) | 0.005 | 0.75 (0.64–0.89) | 0.001 | N/A | ||
| Experienced family or friend infected with COVID-19 | 1.13 (1.01–1.27) | 0.026 | 1.00 (0.84–1.19) | 0.955 | 0.95 (0.80–1.12) | 0.504 | 1.10 (0.98–1.24) | 0.098 |
| Regional location | 0.99 (0.86–1.15) | 0.951 | 0.78 (0.63–0.98) | 0.033 | 0.81 (0.67–0.99) | 0.035 | 1.25 (1.07–1.45) | 0.004 |
| Household income altered | ||||||||
| Increased | N/A | 0.78 (0.56–1.08) | 0.147 | 0.73 (0.54–0.99) | 0.041 | 1.11 (0.91–1.36) | 0.314 | |
| Decreased | N/A | 0.77 (0.57–1.02) | 0.077 | 0.86 (0.66–1.14) | 0.296 | 1.12 (0.94–1.34) | 0.220 | |
| Has concerns about income | 0.89 (0.79–1.01) | 0.075 | 0.64 (0.52–0.78) | 0.001 | 0.63 (0.52–0.75) | 0.001 | 1.56 (1.36–1.79) | 0.001 |
| Professional predictors | ||||||||
| Number of years’ experience since graduating | ||||||||
| 6–10 | N/A | 1.22 (0.95–1.56) | 0.118 | N/A | N/A | |||
| 11–15 | N/A | 1.50 (1.10–2.05) | 0.010 | N/A | N/A | |||
| ≥ 15 | N/A | 1.81 (1.31–2.50) | 0.001 | N/A | N/A | |||
| Occupation | ||||||||
| Nursing | 1.55 (1.37–1.76) | 0.001 | 1.54 (1.26–1.88) | <0.001 | 1.56 (1.29–1.89) | <0.001 | 0.49 (0.43–0.56) | 0.001 |
| Allied health | 0.60 (0.50–0.73) | 0.001 | 1.09 (0.84–1.42) | 0.508 | 1.18 (0.91–1.52) | 0.216 | 0.52 (0.43–0.63) | 0.001 |
| Other roles | 0.28 (0.22–0.35) | 0.001 | 0.80 (0.53–1.22) | 0.313 | 0.99 (0.75–1.33) | 0.967 | 0.71 (0.57–0.88) | 0.002 |
| Frontline area | ||||||||
| ICU | 2.51 (2.03–3.11) | 0.001 | 1.44 (1.00–2.07) | 0.048 | 1.03 (0.75–1.42) | 0.851 | 0.62 (0.50–0.76) | <0.001 |
| Anaesthetics and surgery | 1.08 (0.88–1.32) | 0.448 | 0.55 (0.40–0.75) | 0.001 | 0.81 (0.60–1.10) | 0.177 | 0.99 (0.81–1.22) | 0.946 |
| Medical specialty areas | 0.86 (0.74–1.01) | 0.079 | 0.80 (0.62–1.05) | 0.111 | 0.99 (0.78–1.27) | 0.947 | 1.05 (0.89–1.23) | 0.573 |
| Other * | 0.81 (0.64–1.04) | 0.104 | 0.65 (0.44–0.96) | 0.034 | 0.96 (0.67–1.38) | 0.823 | 0.86 (0.67–1.10) | 0.237 |
| Primary care, community and residential aged care | 0.41 (0.33–0.51) | 0.001 | 0.44 (0.31–0.62) | 0.001 | 0.59 (0.44–0.79) | 0.001 | 1.60 (1.29–1.98) | <0.001 |
| Currently works with COVID-19 patients | 3.32 (2.95–3.74) | 0.001 | 2.76 (2.28–3.33) | 0.001 | 1.61 (1.34–1.93) | 0.001 | 0.52 (0.46–0.59) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smallwood, N.; Pascoe, A.; Karimi, L.; Bismark, M.; Willis, K. Occupational Disruptions during the COVID-19 Pandemic and Their Association with Healthcare Workers’ Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 9263. https://doi.org/10.3390/ijerph18179263
Smallwood N, Pascoe A, Karimi L, Bismark M, Willis K. Occupational Disruptions during the COVID-19 Pandemic and Their Association with Healthcare Workers’ Mental Health. International Journal of Environmental Research and Public Health. 2021; 18(17):9263. https://doi.org/10.3390/ijerph18179263
Chicago/Turabian StyleSmallwood, Natasha, Amy Pascoe, Leila Karimi, Marie Bismark, and Karen Willis. 2021. "Occupational Disruptions during the COVID-19 Pandemic and Their Association with Healthcare Workers’ Mental Health" International Journal of Environmental Research and Public Health 18, no. 17: 9263. https://doi.org/10.3390/ijerph18179263