
Explain Again: Why Are We Vaccinating Young Children against COVID-19?


MAP Sciences, The iLab, Stannard Way, Bedford MK44 3RZ, UK
*
Author to whom correspondence should be addressed.
COVID 2022, 2(4), 492-500; https://doi.org/10.3390/covid2040036
Submission received: 22 March 2022
/
Revised: 7 April 2022
/
Accepted: 10 April 2022
/
Published: 12 April 2022
(This article belongs to the Topic Acute Respiratory Viruses Molecular Epidemiology)
Abstract
:Public trust in governmental policies concerning public health measures is often now questioned. This is an acute problem with respect to vaccinations and particularly true regarding concerns around vaccination of children. Vaccination against COVID-19 is a particularly acute issue with many conspiracy theories circulating. These can almost certainly be countered by a strong evidence base. However, what if a policy is not based on strong evidence but on a judgement call? There is a strong evidence base concerning the beneficial and lifesaving attributes of immunization of adult and particularly vulnerable elderly groups against COVID-19. But what about young children? Here the benefit of immunization is not borne out by any publicly available data and would appear to be led by opinion, not evidence. The language used and vague statements giving a public justification for childhood vaccination COVID-19 immunization could be interpreted as misleading. Given a prevailing mistrust of government public health mandates, could these policies discourage childhood immunization and cost lives of children from other diseases?
1. Introduction
As clearly articulated by the World Health Organization: “there is a low public tolerance of vaccine adverse reactions. Vaccines are therefore only licensed when the frequency of severe reactions is rare and when only self-limiting reactions are reported’. However, under the Emergency Use Authorization, it was clear that the risk to life had to take precedence in a pandemic such as COVID-19 [1].
With time, the data has become clearer in terms of risk benefits and adverse reactions; and as we move from a pandemic crisis to a managed public health issue, the concerns of the public about such vaccinations must be met with clear facts and accurate explanation.
COVID-19 is a severe clinical condition of acute respiratory distress arising from infection with the virus SARS-CoV2. Only a significant minority of individuals infected develop the syndrome COVID-19. Clearly not all those infected with the virus develop COVID-19, but the older you are the more likely you are to develop COVID-19. Underlying health factors such as type 2 diabetes and obesity exacerbate this age morbidity and mortality trend [2].
The USA has a much more active child vaccination policy for SARS CoV2/COVID-19 than the UK and is currently advocating vaccination from 5 years of age; the UK advocates 11 years and above but this has moved more into line with the USA.
The United States CDC website states [3]:
- COVID-19 (SARS-CoV2) can make children very sick and cause children to be hospitalized. In some situations, the complications from infection can lead to death.
- Children are as likely to be infected with COVID-19 (SARS-CoV2) as adults.
- Children can get very sick from COVID-19.
- Children can have both short and long-term health complications from COVID-19.
- Children can spread COVID-19 (SARS-CoV2) to others, including at home and school.
Conflation of the term COVID-19 and SARS-CoV2 infection can be misleading even within official government public health information. Thus, SARS-CoV2 infection of the upper respiratory tract can be asymptomatic, mild, and moderately symptomatic but it does not amount to COVID-19 in the majority of those infected.
Similarly, the UK NHS Website states [4]:
- COVID-19 (SARS-CoV2 infection) is usually mild in most children, but it can make some children unwell.
- One dose of the COVID-19 vaccine gives good protection against your child getting seriously ill, but two doses give stronger and longer-lasting protection.
- Vaccinating children can also help stop the spread of COVID-19 (SARS-CoV2) to other people, including within schools.
The US CDC also states that “There are approximately 28 million children between the ages of 5 and 11 years old in the United States, and there have been nearly 2 million cases of COVID-19 within this age group during the pandemic. As of mid-October 2021, children ages 5 through 11 years have experienced more than 8300 COVID-19 related hospitalizations and nearly 100 deaths from COVID-19. In fact, COVID-19 ranks as one of the top 10 causes of death for children ages 5 through 11 years” [3].
Aside from the conflation of the terms COVID-19 and SARS-CoV2 infection, are these statements entirely accurate; and what evidence is driving policy to vaccinate children in these two nations against the SARS-CoV2 virus? Is it to reduce the incidence of COVID-19 syndrome in these child age groups or to control spread of the disease to the older population?
2. Materials and Methods
Data regarding infection and deaths were taken from publicly available recourses published online, i.e., the Centre for Disease Control USA and the UK Office of National statistics. Additional data was taken from Our World in Data, John Hopkins University and StatisticaTM.
3. Results & Discussion
As the USA has now experienced two years of the SARS-CoV2/COVID-19 pandemic, that implies a SARS-CoV2 infection rate of about 1 million per year 5- to 11-year-olds. Similarly, that is 4150 hospitalization and about 50 deaths per year in which COVID-19 was a contributing factor/co-morbidity. Of the 20,000 plus child deaths a year in the USA the most common causes are accidents, suicide, followed by congenital disorders, cancers, heart disease and homicide; while respiratory disorders (which encompasses pneumonia and influenza) are in a much smaller 10th place [5].
Thus, to qualify as the 10th most common cause of mortality in 5- to 11-year-olds COVID-19 deaths must exceed those of influenza and other respiratory disorders combined. So how does SARS-CoV2/COVID-19 compare to child morbidity from influenza? [6]:
- The CDC estimates that from the 2010–2011 season to the 2019–2020 season, flu-related hospitalizations among children younger than 5 years old have ranged from 7000 to 26,000 in the United States.
- From the 2004–2005 season to the 2019–2020 season, flu-related deaths in children reported to CDC during regular flu seasons have ranged from 37 to 199 deaths. (During the 2009 H1N1 pandemic, 358 pediatric flu-related deaths were reported to CDC from April 2009 to September 2010.)
- Also of note, even though individual flu deaths in children must be reported to CDC, “it is likely that not all deaths are captured and that the number of actual deaths is higher. CDC has developed statistical models that account for the underreporting of flu-related deaths in children to estimate the actual number of deaths. During 2019–2020, for example, 199 deaths in children were reported to CDC but statistical modelling suggests approximately 434 deaths may have occurred” [6].
Although it is difficult to get exact comparatives for the 5–11 age grouping, 112 deaths occurred in children of 5–17 years old in 2019–2020. Thus, we might reasonably estimate 56 influenza co-morbidity deaths occurred in 2019–2020 for the 5–11 age group. More detailed estimates are available from the CDC for 2018–2019 flu season which would put the number of influenza infections for this age group at 3,311,426, hospitalizations at 9800 and deaths at 78 [7] (see Table 1).
In the UK, between 3 January 2020 to 7 May 2021, the Office for National Statistics (ONS), reported 15 children (less than 1 to 14 years of age) died with COVID-19 recorded as the cause or as a co-morbidity to other conditions; that equates to 11.25 per year [8]. If we compare this to child deaths from influenza, the prevailing rate of death for children under 15 (between 2000 and 2008) has been averaging 166 per year; although only 23% (38 per year) had no other risk factor [8,9]. For the year 2019 the ONS report had recorded 26 influenza deaths of children under 15 years of age [9]. However, for 15- to 18-year-olds the ONS also reported 22 deaths recorded with COVID-19 as the cause or co-morbidity (between 3 January 2020 and 7 May 2021), i.e., 16.5 per year. By comparison, in 2019, the ONS only recorded four deaths from influenza in a comparable age group of 15–19-year-olds [10]. The relative total UK childhood populations and percentage deaths from COVID-19 and influenza are shown in Table 2.
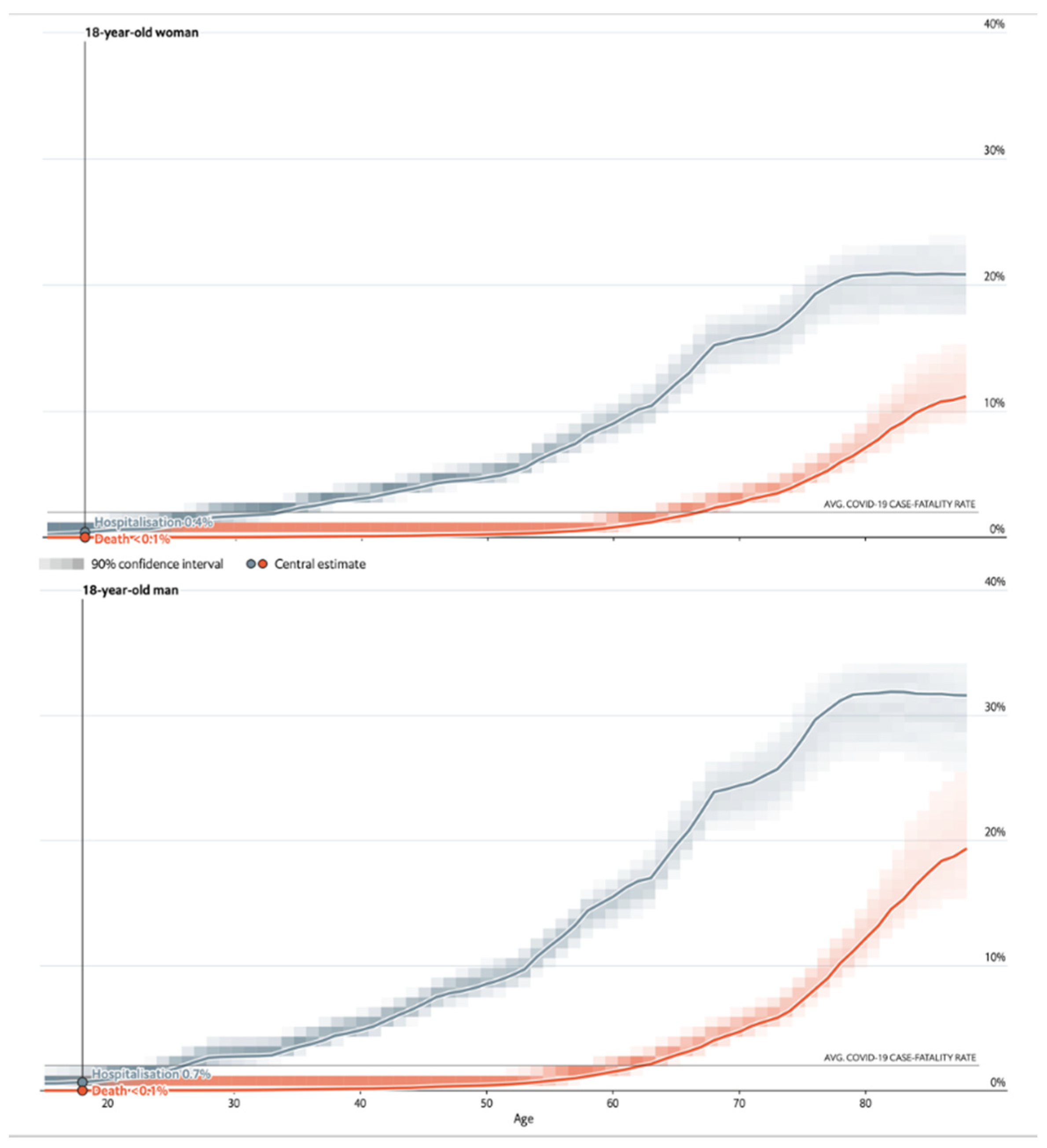
Even before the widespread introduction of COVID-19 vaccination young adults, particularly children under 15, had an extremely low probability of hospitalization and death from a SARS-CoV2 infection during this pandemic. Although not elaborated on here, the data on all over 30 s is clear; they risk of hospitalization and increased chance of death [12,13] (see Figure 1). For children who have no contributing risk factors such as diabetes or immune suppression, the risk is extremely low and about the same as that for influenza in a very low incidence non-outbreak year, let alone an epidemic or pandemic.
In 2022, it is without doubt that global collected data have clearly demonstrated that mRNA-based vaccination campaigns against SARS-CoV2 have been highly effective at reducing substantially the risk of hospitalization and death in the adult population [14]. However, it does not reduce the risk of catching the virus and passing it on as an asymptomatic or indeed mild symptomatic carrier. As the Director of the NIH, Dr. Anthony Fauci, has said publicly to the USA network CNN on the 11 January 2022: “[Omicron] “will ultimately find just about everybody”. However, those who are vaccinated and boosted “will very likely, with some exceptions, do reasonably well in the sense of not having hospitalization and death.” “[unvaccinated individuals are] going to get the brunt of the severe aspect of this.”
Thus, vaccination against COVID-19 does not give any significant protection from initial infection in the upper respiratory tract (i.e., oral mucosal immunity). This rapidly wains within about six months [14,15]. Fortunately, systemic immunity, including T-cell responses, last longer possibly up to a year [16], thus preventing the worst effects-hospitalization and death-in the more at-risk adult population [17]. However, this does not appear to be a prolonged effect, and annual SARS-CoV2 vaccinations are the most likely public health initiative we will have to adopt [18].
So why vaccinate children if it has no obvious benefit in terms of reducing the risk of hospitalization or death for them as individuals?
The argument may have been that they are a reservoir and vector for the virus to then infect parents and grandparents who are at risk; and the knock-on effect in overloading health services at crisis point is therefore going to affect them. This is undoubtedly true [19], as children catch the virus at the same rate as any other age group (see Table 3).
Despite the efforts of some nations to eradicate the SAR-COV2 virus from their countries, this is not going to be possible. SARS-CoV2 is now endemic, and, like the flu, we have to look out for variant strains arising [20]. Data on vaccination and COVID-19 deaths in China is not available [21], but Omicron is a prime example of the problem variants present. China is particularly concerned about Omicron, and despite their firm and restrictive COVID-19 eradication isolation policies, there are report of shut downs and increasing COVID-19 deaths in Hong Kong [22].
Any further analogy to the public health management of COVID-19 exactly as we have for the flu does not hold true. Thus, after examination of current published data, it has to be asked: What is the scientific justification for vaccination of young children (e.g., less than 14) with these particular vaccines?
- It does not benefit them now [23];
- It will not benefit them in the future (as the systemic immunity will not last them into an adult age group that is susceptible) [15];
- It is NOT effectively contributing to any sensible global viral eradication program of the SARS-CoV2 viruses [20].
An argument that “it does them no harm and might be good” is unsound. All medicines have negative effects, and no licensed practitioner will prescribe a medicine if there is no illness or serious threat of illness. Indeed, most drugs are derived from what are effectively poisons; but they have a window of benefit in specific conditions. Widespread use of antibiotics without disease has given rise to life threatening superbugs [24]. Even taking too many vitamins and minerals can be dangerous; e.g., iron tablets are therapeutic for those who are anemic but for those who are not too much iron is highly toxic and accumulates in tissues. Also, vaccines are not entirely without risk, including the following:
- Antibody mediated (mostly IgE) hypersensitivity reactions, predominately arising from sensitivity developed to carrier oils and adjuvants in the vaccine formulations. Symptoms usually manifest within minutes and hours [25].
- Delayed-type hypersensitivity reactions (type IV hypersensitivity); T-cell mediated reactions that can be both CD4+ and/or CD8+ dependent, with a target allergen presented via major histocompatibility molecules to T-cell receptors. Activation of CD4+ T cells results in cytokine mediated inflammation, which is typically confined to a local area, but can sometimes be widespread. In reactions where CD8+ T cells are involved, the release of perforin and granzyme can lead to bystander cell injury and death by apoptosis [26]. Symptoms of delayed hypersensitivity generally have onset within 6 h to weeks and can range widely from localized skin symptoms to disseminated rashes with systemic symptoms and/or blistering of the skin and mucosal surfaces [27].
- Immunologically mediated neurological complications: such as Guillain–Barré syndrome, Muller Fisher syndrome and other demyelinating neuropathies (Bell’s palsy, acute disseminated encephalomyelitis, etc.) are known adverse events related to immunization [28,29]. These can be ongoing for many months and years.
- Antibody-dependent enhancement (ADE); whole dead virion protein vaccination can prime a new pathway by which a virus can propagate and spread within immune cells enabled by antibody mediated opsonization (ADE), thereby exacerbating severe illness caused by the viral infection in certain immunized individuals [30]. This is generally screened for very early in vaccine research and development [31].
There are growing reports of adverse effects in a minority of individuals receiving SARS-CoV2 (COVID-19) mRNA vaccines [32,33]. Perhaps the most relevant is that concerning myocarditis. Although a very rare condition, the risk of this condition is raised, mostly in males under 40 (by up to seven-fold) who receive repeat doses of the mRNA based COVID-19 vaccine [34,35]. However small the chance of an adverse reaction, you then must look back at the relative risk of adverse reactions, or requiring hospitalization, from these vaccinations, versus hospitalization and death from COVID-19 for this specific age group.
Although the comparative statistics described here are rough estimates, and no one has been able to calculate them for the very young age groups, the relative risk benefits of mRNA vaccination against SARS-CoV2 are not, currently, overwhelming obvious for children (see Table 4).
Judging relative risk of doing (or saying) anything is something we must do every day of our lives. Some of us use data and statistics to help in making such judgement call [37]. The judgement call to vaccinate young children is not at present clearly born out in the current datasets and statistics. Unlike for many other childhood viral diseases, such as Mumps, Measles, Rubella and even Influenza, this is not an age group at high risk of serious morbidity and mortality from SARS-CoV2.
There are many vaccinations where the benefit to children’s lives vastly outweighs the risk of adverse reactions [38].
The anti-MMR vaccination rhetoric fueled a global crisis of confidence and is estimated to have cost 140,000 children lives worldwide [39], and resurgence of measles which was thought to be on the verge of eradication in many countries [40]. A wrong call on COVID-19 mRNA vaccination could reverse all the gains. [41].
Thus, it is difficult to advocate a blanket campaign for vaccination of all young children against COVID-19 using the current SARS-Cov2 mRNA vaccines based on the lack of scientific evidence of why we should. Furthermore, especially in the current climate, to do so may risk a greater harm to society as it could further erode public trust in public health vaccinations that do save children’s lives.
4. Conclusions
In conclusion, vaccination against COVID-19 of an individual child may be justified by prevailing risk factors, such as diabetes, obesity and immune compromising conditions, but that is specific to that child. The move to vaccinate all 5+ year old children with current mRNA COVID-19 vaccines requires review and a detailed public justification [42].
As an addendum, during review of this manuscript a reviewer pointed out the latest data released by six New York state public health scientists, not yet peer-reviewed, who analyzed cases and hospitalization rates for SARS-CoV2 from 13 December 2021 to 30 January 2022. This data included 852,384 fully vaccinated children aged 12 to 17 and 365,502 fully vaccinated children aged 5 to 11 [43].
- This study revealed that mRNA vaccine effectiveness against hospitalization during the Omicron variant surge declined from 85% to 73% for children aged 12 to 17.
- Amongst children aged 5 to 11, effectiveness fell even more significantly, from 100% to 48%.
- Vaccine effectiveness against testing positive declined from 66% to 51% among children aged 12 to 17. In the 5 to 11 years group, effectiveness dropped from 68% to 12%.
- In the last week of January, vaccine effectiveness against infection among 12-year-olds was 67%, but substantially lower at just 11% for 11-year-olds.
Author Contributions
Conceptualization, R.K.I. and T.S.M.; methodology, R.K.I.; formal analysis, R.K.I.; investigation, R.K.I. and T.S.M.; resources, T.S.M.; writing—original draft preparation, R.K.I.; writing—review and editing, T.S.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study as they are not applicable to data analysis only studies.
Informed Consent Statement
Not applicable.
Data Availability Statement
Links to all publicly archived datasets are detailed in the text.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vashishtha, V.M.; Kumar, P. Emergency use authorisation of Covid-19 vaccines:An ethical conundrum. Indian J. Med. Ethics 2021, 6, 20–22. [Google Scholar] [CrossRef]
- Zhu, Z.; Hasegawa, K.; Ma, B.; Fujiogi, M.; Camargo, C.A.; Liang, L. Association of obesity and its genetic predisposition with the risk of severe COVID-19: Analysis of population-based cohort data. Metabolism 2020, 112, 154345. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/children-teens.html (accessed on 6 February 2022).
- Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/coronavirus-vaccination/coronavirus-vaccine-for-children-aged-12-to-15/ (accessed on 6 February 2022).
- Cunningham, R.M.; Walton, M.A.; Carter, P.M. The Major Causes of Death in Children and Adolescents in the United States. N. Engl. J. Med. 2018, 379, 2468–2475. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/flu/spotlights/2020-2021/pediatric-flu-deaths-reach-new-high.htm (accessed on 6 February 2022).
- Available online: https://www.cdc.gov/flu/about/burden/2018-2019.html (accessed on 6 February 2022).
- Available online: https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/covid19deathsinukforchildrenfromages0to19sincemarch2020 (accessed on 6 February 2022).
- Cromer, D.; van Hoek, A.J.; Jit, M.; Edmunds, W.J.; Fleming, D.; Miller, E. The burden of influenza in England by age and clinical risk group: A statistical analysis to inform vaccine policy. J. Infect. 2014, 68, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/deathsfrominfluenzaonlyin2019and2020intheuk (accessed on 6 February 2022).
- Available online: https://www.statista.com/statistics/281174/uk-population-by-age/ (accessed on 6 February 2022).
- See How Age and Illnesses Change the Risk of Dying from Covid-The Economist. Available online: https://www.economist.com/graphic-detail/covid-pandemic-mortality-risk-estimator (accessed on 11 March 2021).
- Available online: https://covid19researchdatabase.org/ (accessed on 27 January 2022).
- Vahidy, F.S.; Pischel, L.; Tano, M.E.; Pan, A.P.; Boom, M.L.; Sostman, H.D.; Nasir, K.; Saad, B. Real World Effectiveness of COVID-19 mRNA Vaccines against Hospitalizations and Deaths in the United States. Ome Medrxiv 2021. [Google Scholar] [CrossRef]
- Edridge, A.W.D.; Kaczorowska, J.; Hoste, A.C.R.; Bakker, M.; Klein, M.; Loens, K.; Jebbink, M.F.; Matser, A.; Kinsella, C.M.; Rueda, P.; et al. Seasonal coronavirus protective immunity is short-lasting. Nat. Med. 2020, 26, 1691–1693. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.-B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168.e14. [Google Scholar] [CrossRef]
- Katikireddi, S.V.; Cerqueira-Silva, T.; Vasileiou, E.; Robertson, C.; Amele, S.; Pan, J.; Taylor, B.; Boaventura, V.; Werneck, G.L.; Flores-Ortiz, R.; et al. Two-dose ChAdOx1 nCoV-19 vaccine protection against COVID-19 hospital admissions and deaths over time: A retrospective, population-based cohort study in Scotland and Brazil. Lancet 2021, 399, 25–35. [Google Scholar] [CrossRef]
- Borio, L.L.; Bright, R.A.; Emanuel, E.J. A National Strategy for COVID-19 Medical Countermeasures. JAMA J. Am. Med. Assoc. 2022, 327, 215. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 6 February 2022).
- Baker, R.E.; Park, S.W.; Wagner, C.E.; Metcalf, C.J.E. The limits of SARS-CoV-2 predictability. Nat. Ecol. Evol. 2021, 5, 1052–1054. [Google Scholar] [CrossRef]
- Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer? (accessed on 6 February 2022).
- Xiao, Y.; Li, Y.; Du, N.; Luo, L.; Su, D. Challenges facing Chinese primary care in the context of COVID-19. Fam. Pract. 2022, 179, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Kostoff, R.N.; Calina, D.; Kanduc, D.; Briggs, M.B.; Vlachoyiannopoulos, P.; Svistunov, A.A.; Tsatsakis, A. Why are we vaccinating children against COVID-19? Toxicol. Rep. 2021, 8, 1665–1684. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S. Key Takeaways from the U.S. CDC’s 2019 Antibiotic Resistance Threats Report for Frontline Providers. Crit. Care Med. 2020, 48, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Stone, C.A.; Rukasin, C.; Beachkofsky, T.M.; Phillips, E.J. Immune-mediated adverse reactions to vaccines. Br. J. Clin. Pharmacol. 2019, 85, 2694–2706. [Google Scholar] [CrossRef]
- Justiz Vaillant, A.A.; Vashisht, R.; Zito, P.M. Immediate Hypersensitivity Reactions. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513315/ (accessed on 15 November 2021).
- Williams, S.E.; Klein, N.P.; Halsey, N.; Dekker, C.L.; Baxter, R.P.; Marchant, C.D.; LaRussa, P.S.; Sparks, R.C.; Tokars, J.I.; Pahud, B.A.; et al. Overview of the Clinical Consult Case Review of adverse events following immunization: Clinical Immunization Safety Assessment (CISA) network 2004–2009. Vaccine 2011, 29, 6920–6927. [Google Scholar] [CrossRef] [Green Version]
- Phillips, E.J.; Bigliardi, P.L.; Bircher, A.J.; Broyles, A.; Chang, Y.-S.; Hung, S.-I.; Lehloenya, R.; Mockenhaupt, M.; Peter, J.; Pirmohamed, M.; et al. Controversies in drug allergy: Testing for delayed reactions. J. Allergy Clin. Immunol. 2019, 143, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Gable, K.L.; Afshari, Z.; Sufit, R.L.; Allen, J.A. Distal Acquired Demyelinating Symmetric Neuropathy after Vaccination. J. Clin. Neuromuscul. Dis. 2013, 14, 117–122. [Google Scholar] [CrossRef]
- Huisman, W.; Martina, B.; Rimmelzwaan, G.; Gruters, R.; Osterhaus, A. Vaccine-induced enhancement of viral infections. Vaccine 2009, 27, 505–512. [Google Scholar] [CrossRef]
- Iwata-Yoshikawa, N.; Shiwa, N.; Sekizuka, T.; Sano, K.; Ainai, A.; Hemmi, T.; Kataoka, M.; Kuroda, M.; Hasegawa, H.; Suzuki, T.; et al. A lethal mouse model for evaluating vaccine-associated enhanced respiratory disease during SARS-CoV-2 infection. Sci. Adv. 2022, 8, eabh3827. [Google Scholar] [CrossRef]
- Available online: https://vaers.hhs.gov/index.html (accessed on 6 February 2022).
- Ferner, R.E.; Stevens, R.J.; Anton, C.; Aronson, J.K. Spontaneous Reporting to Regulatory Authorities of Suspected Adverse Drug Reactions to COVID-19 Vaccines Over Time: The Effect of Publicity. Drug Saf. 2022, 45, 137–144. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Anthony Harnden, A.; Coupland, C.A.C.; et al. Risk of myocarditis following sequential COVID-19 vaccinations by age and sex. Medrxiv 2021. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US from December 2020 to August 2021. JAMA J. Am. Med. Assoc. 2022, 327, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 6 February 2022).
- Simons, M.R.; Zurynski, Y.; Cullis, J.; Morgan, M.; Davidson, A. Does evidence-based medicine training improve doctors’ knowledge, practice and patient outcomes? A systematic review of the evidence. Med. Teach. 2019, 41, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Nandi, A.; Shet, A. Why vaccines matter: Understanding the broader health, economic, and child development benefits of routine vaccination. Hum. Vaccines Immunother. 2020, 16, 1900–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.who.int/news/item/05-12-2019-more-than-140-000-die-from-measles-as-cases-surge-worldwide (accessed on 6 February 2022).
- Feemster, K.A.; Szipszky, C. Resurgence of measles in the United States: How did we get here? Curr. Opin. Pediatr. 2020, 32, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Drew, L. The case for mandatory vaccination. Nature 2019, 575, S58–S60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozlov, M. What COVID vaccines for young kids could mean for the pandemic. Nature 2021, 599, 18–19. [Google Scholar] [CrossRef]
- Dorabawila, V.; Hoefer, D.; Bauer, U.E.; Bassett, M.T.; Lutterloh, E.; Rosenberg, E.S. Effectiveness of the BNT162b2 vaccine among children 5–11 and 12–17 years in New York after the Emergence of the Omicron Variant. medRxiv 2022. [Google Scholar] [CrossRef]
Figure 1.
Age dependent risk for females (Top panel) and males (Bottom panel) in the United States of Hospitalization and death from COVID-19 when found positive for SARS-CoV2 before the introduction of COVID-19 mRNA vaccines. Indicated is the risk for an 18-year-old woman and an 18-year-old man. Illustration taken from the Economist rendering of data collected by C-19RD. https://www.economist.com/graphic-detail/covid-pandemic-mortality-risk-estimator (accessed on 27 January 2021); https://covid19researchdatabase.org/ (accessed on 27 January 2021).
Figure 1.
Age dependent risk for females (Top panel) and males (Bottom panel) in the United States of Hospitalization and death from COVID-19 when found positive for SARS-CoV2 before the introduction of COVID-19 mRNA vaccines. Indicated is the risk for an 18-year-old woman and an 18-year-old man. Illustration taken from the Economist rendering of data collected by C-19RD. https://www.economist.com/graphic-detail/covid-pandemic-mortality-risk-estimator (accessed on 27 January 2021); https://covid19researchdatabase.org/ (accessed on 27 January 2021).


{kind=link}
Table 1.
Comparative infection yearly hospitalization and death rates for SARS-CoV2 and influenza for 5–11-year-olds in the USA. Estimates from CDC data.
Table 1.
Comparative infection yearly hospitalization and death rates for SARS-CoV2 and influenza for 5–11-year-olds in the USA. Estimates from CDC data.
| Infections | Hospitalizations | Deaths | |
|---|---|---|---|
| SARS-CoV2 * | 1 million/28 million (3.5%) | 4150/28 million (0.015%) | 50/28 million (0.00018%) |
| Influenza ** | 3 million/28 million (10%) | 9800/28 million (0.035%) | 78/28 million (0.00028%) |
* CDC data yearly average after two years of COVID-19 pandemic ** CDC data pre-COVID-19 pandemic for 2018–2019 Influenza season.
Table 2.
Comparative of UK Child Deaths involving SARS-CoV2/COVID-19 and influenza from data taken from UK Office of National Statistics and Statistica 2022 [9,10,11].
| AGE (Years) | Age Specific UK Population | Respiratory Virus | Annual Deaths 2019–2021 | Mortality Rate |
|---|---|---|---|---|
| <1 to 14 | 11,975,000 | SARS-CoV2 | 11.25 | 0.000094% |
| Influenza | 26 | 0.00022% | ||
| 15–19 | 3,651,000 | SARS-CoV2 | 16.5 | 0.00045% |
| Influenza | 4 | 0.00011% |
Table 3.
Risk for SAR-CoV2 Infection, Hospitalization, and COVID-19 Death by Age Group.
| Rate Compared to 18–29 Yeasrs old 1 | 0–4 Years Old | 5–17 Years Old | 18–29 Years Old | 30–39 Years Old | 40–49 Years Old | 50–64 Years Old | 65–74 Years Old | 75–84 Years Old | 85+ Years Old |
|---|---|---|---|---|---|---|---|---|---|
| Cases 2 | <1× | 1× | Reference group | 1× | 1× | 1× | 1× | 1× | 1× |
| Hospitalization 3 | <1× | <1× | Reference group | 2× | 2× | 4× | 5× | 8× | 10× |
| Death 4 | <1× | <1× | Reference group | 4× | 10× | 25× | 65× | 140× | 340× |
All rates are relative to the 18- to 29-year-old age category. This group was selected as the reference group because it has accounted for the largest cumulative number of COVID-19 cases compared to other age groups. Sample interpretation: Compared with 18- to 29-year-olds, the rate of death is four times higher in 30- to 39-year-olds, and 340 times higher in those who are 85 years and older (in the table, a rate of 1× indicates no difference compared to the 18- to 29-year-old age category). Super script numbers 1–4 refer to CDC data references listed on the weblink https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 6 February 2022).
Table 4.
Data and statistical comparison of adverse reactions from all COVID-19 vaccinations in the UK (ALL AGE GROUPS), compiled from the Yellow Card system of the UK Medicine and Health-devices Regulatory Authority (MHRA) (https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 6 February 2022) [36]).
Table 4.
Data and statistical comparison of adverse reactions from all COVID-19 vaccinations in the UK (ALL AGE GROUPS), compiled from the Yellow Card system of the UK Medicine and Health-devices Regulatory Authority (MHRA) (https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 6 February 2022) [36]).
| Vaccine | 1st and 2nd Doses | Booster | Adverse Reaction Reports | Deaths Soon after Vaccination ** | Myocarditis and Pericarditis | GB and MF |
|---|---|---|---|---|---|---|
| Pfizer | 50.5 mil | 36.7 mil | 1,286,984 (2.55%) | 702 (0.0014%) | 1109 (0.0022%) | 92 (0.0002%) |
| Astra Zeneca | 46.7 mil | 231,168 (0.50%) | 1200 (0.0026%) | 425 (0.0009%) | 486 (0.0010%) | |
| Moderna | 3 mil | 32,936 (1.10%) | 33 (0.0011%) | 283 (0.0094%) | 12 (0.0004%) | |
| All | 136.9 million COVID-19 vaccination doses | 1,552,248 * (1.13%) | 1972 ** (0.0014%) | 130 per 100,000 (expect 37–47 per 100,000) | 40 per 100,000 (expect 2 per 100,000) | |
* The vaccine given was not recorded on 1160 Adverse reaction reports. ** Pre-pandemic UK total recorded deaths (all age groups) per week varied from 8900 (summer) to 12,600 (winter). Since over 75% of the UK population have been vaccinated at least once this death rate does not exceed that expected from other causes.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Iles, R.K.; Makhzoumi, T.S. Explain Again: Why Are We Vaccinating Young Children against COVID-19? COVID 2022, 2, 492-500. https://doi.org/10.3390/covid2040036
AMA Style
Iles RK, Makhzoumi TS. Explain Again: Why Are We Vaccinating Young Children against COVID-19? COVID. 2022; 2(4):492-500. https://doi.org/10.3390/covid2040036
Chicago/Turabian StyleIles, Ray Kruse, and Tarek Sultani Makhzoumi. 2022. "Explain Again: Why Are We Vaccinating Young Children against COVID-19?" COVID 2, no. 4: 492-500. https://doi.org/10.3390/covid2040036