
Outdoor Activity Participation Improves Adolescents’ Mental Health and Well-Being during the COVID-19 Pandemic

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Survey Instrument
2.3. Data Analysis
2.3.1. Data Preparation
2.3.2. Activity Grouping and SWB Scale Analysis
2.3.3. Hypothesis Testing
3. Results
3.1. Sample
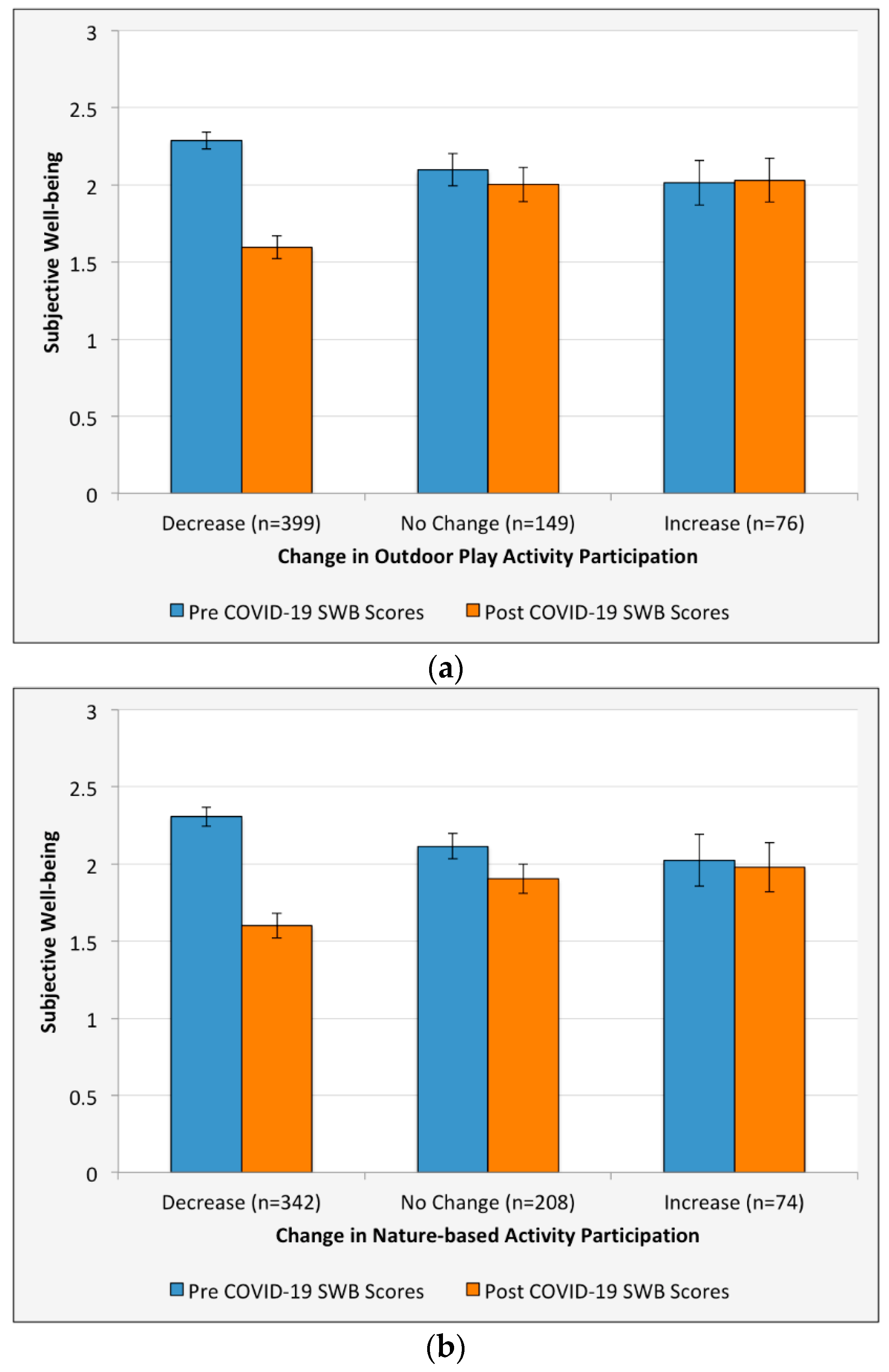
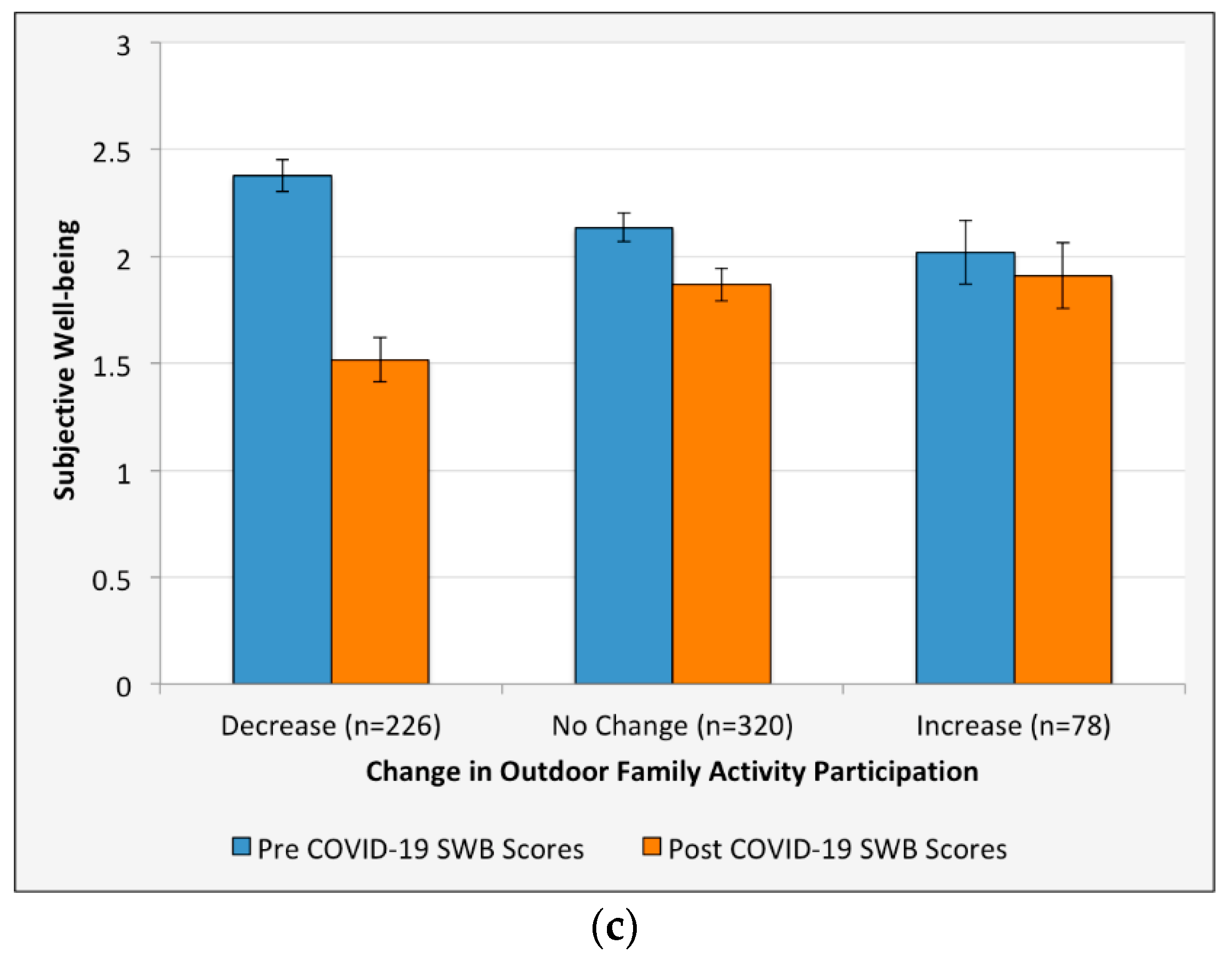
3.2. Subjective Well-Being and Mental Health Scores
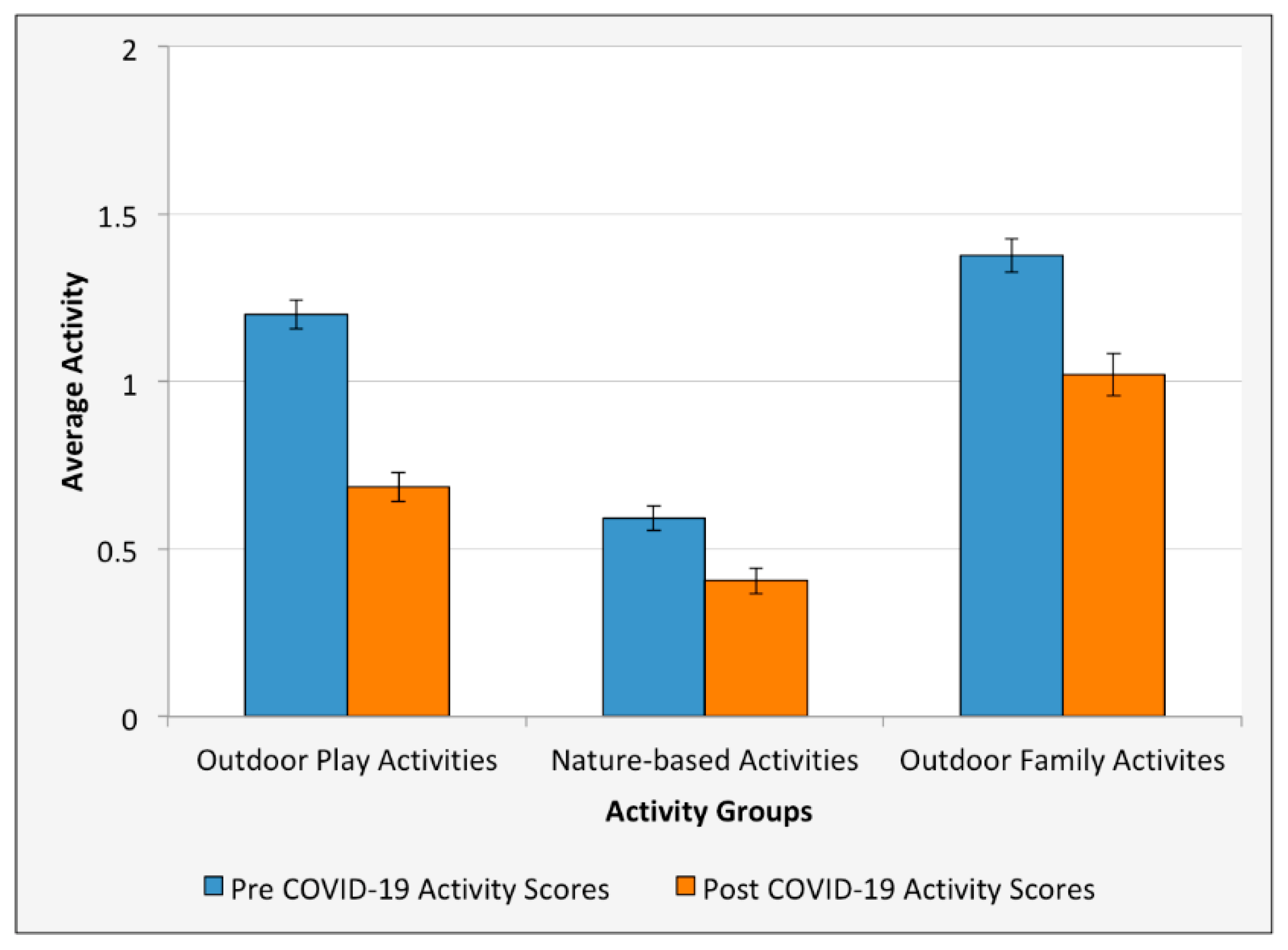
3.3. Outdoor Activity Scores
3.4. Linear Regression Model
4. Discussion
Recommendations for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Myers, S.S.; Patz, J.A. Emerging threats to human health from global environmental change. Annu. Rev. Environ. Resour. 2009, 34, 223–252. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, B.; Pande, N. Mediating role of resilience in the impact of mindfulness on life satisfaction and affect as indices of subjective well-being. Pers. Individ. Dif. 2016, 93, 63–67. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new Resilience scale: The Connor-Davidson Resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience Theory and Research on Children and Families: Past, Present, and Promise. J. Fam. Theory Rev. 2018, 10, 12–31. [Google Scholar] [CrossRef] [Green Version]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Well-Being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Park, N. The Role of Subjective Well-Being in Positive Youth Development. Ann. Am. Acad. Pol. Soc. Sci. 2004, 591, 25–39. [Google Scholar] [CrossRef]
- Tomyn, A.J.; Weinberg, M.K. Resilience and Subjective Wellbeing: A Psychometric Evaluation in Young Australian Adults. Aust. Psychol. 2018, 53, 68–76. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being: The science of happiness and a proposal for a national index. Am. Psychol. 2000, 55, 34–43. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Subjective well-being in mental health and human development research worldwide: An introduction. Soc. Indic. Res. 2006, 77, 1–10. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Health for the World’s Adolescents A Second Chance in the Second Decade; WHO Document Production Services: Geneva, Switzerland, 2014; pp. 1–20.
- Danese, A.; Smith, P.; Chitsabesan, P.; Dubicka, B. Child and adolescent mental health amidst emergencies and disasters. Br. J. Psychiatry 2020, 216, 159–162. [Google Scholar] [CrossRef]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM 2020, 113, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Cindrich, S.L.; Lansing, J.E.; Brower, C.S.; McDowell, C.P.; Herring, M.P.; Meyer, J.D. Associations Between Change in Outside Time Pre- and Post-COVID-19 Public Health Restrictions and Mental Health: Brief Research Report. Front. Public Health 2021, 9, 1–6. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Sprang, G.; Silman, M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med. Public Health Prep. 2013, 7, 105–110. [Google Scholar] [CrossRef]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of covid-19 epidemic declaration on psychological consequences: A study on active weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Samuelsson, K.; Barthel, S.; Colding, J.; Macassa, G.; Giusti, M. Urban nature as a source of resilience during social distancing amidst the coronavirus pandemic. OSF Prepr. 2020. [Google Scholar] [CrossRef]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, 903–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015, 6, 1–8. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Stigsdotter, U.K.; Randrup, T.B.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F. Health promoting outdoor environments - Associations between green space, and health, health-related quality of life and stress based on a Danish national representative survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Hartig, T.; Evans, G.W.; Jamner, L.D.; Davis, D.S.; Gärling, T. Tracking restoration in natural and urban field settings. J. Environ. Psychol. 2003, 23, 109–123. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health- A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Berto, R. The role of nature in coping with psycho-physiological stress: A literature review on restorativeness. Behav. Sci. 2014, 4, 394–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, L.; Keena, K.; Pevec, I.; Stanley, E. Green schoolyards as havens from stress and resources for resilience in childhood and adolescence. Health Place 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Hartig, T.; Korpela, K.; Evans, G.W.; Gärling, T. A measure of restorative quality in environments. Scand. Hous. Plan. Res. 1997, 14, 175–194. [Google Scholar] [CrossRef]
- Mayer, F.S.; Frantz, C.M.P.; Bruehlman-Senecal, E.; Dolliver, K. Why is nature beneficial?: The role of connectedness to nature. Environ. Behav. 2009, 41, 607–643. [Google Scholar] [CrossRef]
- Nisbet, E.K.; Zelenski, J.M.; Murphy, S.A. Happiness is in our Nature: Exploring Nature Relatedness as a Contributor to Subjective Well-Being. J. Happiness Stud. 2011, 12, 303–322. [Google Scholar] [CrossRef]
- Pearson, D.G.; Craig, T. The great outdoors? Exploring the mental health benefits of natural environments. Front. Psychol. 2014, 5, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Corraliza, J.A.; Collado, S.; Bethelmy, L. Nature as a Moderator of Stress in Urban Children. Procedia Soc. Behav. Sci. 2012, 38, 253–263. [Google Scholar] [CrossRef] [Green Version]
- Wells, N.M.; Evans, G.W. NEARBY NATURE A Buffer of Life Stress Among Rural Children. Environ. Behav. 2003, 35, 311–330. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Hormazábal-Aguayo, I.; Fernández-Vergara, O.; Olivares, P.R.; Oriol-Granado, X. Physical activity, screen time and subjective well-being among children. Int. J. Clin. Heal. Psychol. 2020, 20, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, G.A.; Lazarus, N.B.; Cohen, R.D.; Leu, D.J. Psychosocial factors in the natural history of physical activity. Am. J. Prev. Med. 1991, 7, 12–17. [Google Scholar] [CrossRef]
- Valois, R.F.; Zullig, K.J.; Huebner, E.S.; Drane, J.W. Physical activity behaviors and perceived life satisfaction among public high school adolescents. J. Sch. Health 2004, 74, 59–65. [Google Scholar] [CrossRef]
- Zullig, K.J.; White, R.J. Physical Activity, Life Satisfaction, and Self-Rated Health of Middle School Students. Appl. Res. Qual. Life 2011, 6, 277–289. [Google Scholar] [CrossRef]
- Wicker, P.; Frick, B. The relationship between intensity and duration of physical activity and subjective well-being. Eur. J. Public Health 2015, 25, 868–872. [Google Scholar] [CrossRef] [Green Version]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R. Is physical activity in natural environments better for mental health than physical activity in other environments? Soc. Sci. Med. 2013, 91, 130–134. [Google Scholar] [CrossRef]
- House, J.S.; Landis, K.R.; Umberson, D. Social relationships and health. Science 1988, 241, 540–545. [Google Scholar] [CrossRef]
- Roe, J.J.; Ward Thompson, C.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, V.; Bamkole, O. The relationship between social cohesion and urban green space: An avenue for health promotion. Int. J. Environ. Res. Public Health 2019, 16, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humbert, M.L.; Chad, K.E.; Spink, K.S.; Muhajarine, N.; Anderson, K.D.; Bruner, M.W.; Girolami, T.M.; Odnokon, P.; Gryba, C.R. Factors that influence physical activity participation among high- and low-SES youth. Qual. Health Res. 2006, 16, 467–483. [Google Scholar] [CrossRef]
- Helliwell, J.F.; Putnam, R.D. The social context of well-being. Philos. Trans. R. Soc. B Biol. Sci. 2004, 359, 1435–1446. [Google Scholar] [CrossRef]
- Lewis, T. How Coronavirus Spreads through the Air: What We Know So Far. Available online: https://www.scientificamerican.com/article/how-coronavirus-spreads-through-the-air-what-we-know-so-far1/ (accessed on 6 July 2020).
- Bocarro, J.; Greenwood, P.B.; Henderson, K.A. An Integrative Review of Youth Development Research in Selected United States Recreation Journals. J. Park Recreat. Admi. 2008, 26, 4–27. [Google Scholar]
- Freeman, S.; Eykelbosh, A. COVID-19 and Outdoor Safety: Considerations for Use of Outdoor Recreational Spaces; National Collaborating Centre for Environmental Health: Vancouver, BC, Canada, 2020; pp. 1–15. [Google Scholar]
- Glover, T.D. Neighboring in the Time of Coronavirus? Paying Civil Attention While Walking the Neighborhood. Leis. Sci. 2020, 40, 1–7. [Google Scholar] [CrossRef]
- Jiao, W.Y.; Wang, L.N.; Liu, J.; Fang, S.F.; Jiao, F.Y.; Pettoello-Mantovani, M.; Somekh, E. Behavioral and Emotional Disorders in Children during the COVID-19 Epidemic. J. Pediatr. 2020, 221, 264–266. [Google Scholar] [CrossRef]
- Van Lancker, W.; Parolin, Z. COVID-19, school closures, and child poverty: A social crisis in the making. Lancet Public Heal. 2020, 5, 243–244. [Google Scholar] [CrossRef]
- Van Dorn, A.; Cooney, R.E.; Sabin, M.L. COVID-19 exacerbating inequalities in the US. Lancet 2020, 395, 1243–1244. [Google Scholar] [CrossRef]
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C.; Honermann, B.; Lankiewicz, E.; Mena, L.; Crowley, J.S.; et al. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef]
- Larson, L.R.; Szczytko, R.; Bowers, E.P.; Stephens, L.E.; Stevenson, K.T.; Floyd, M.F. Outdoor Time, Screen Time, and Connection to Nature: Troubling Trends Among Rural Youth? Environ. Behav. 2018, 00, 1–26. [Google Scholar] [CrossRef]
- Rigolon, A.; Browning, M.; Jennings, V. Inequities in the quality of urban park systems: An environmental justice investigation of cities in the United States. Landsc. Urban Plan. 2018, 178, 156–169. [Google Scholar] [CrossRef]
- Hadavi, S. Direct and Indirect Effects of the Physical Aspects of the Environment on Mental Well-Being. Environ. Behav. 2017, 49, 1071–1104. [Google Scholar] [CrossRef]
- Slater, S.J.; Christiana, R.W.; Gustat, J. Recommendations for keeping parks and green space accessible for mental and physical health during COVID-19 and other pandemics. Prev. Chronic Dis. 2020, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Berry, H.L.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef]
- Masten, A.S.; Narayan, A.J. Child development in the context of disaster, war, and terrorism: Pathways of risk and resilience. Annu. Rev. Psychol. 2012, 63, 227–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boas, T.C.; Christenson, D.P.; Glick, D.M. Recruiting large online samples in the United States and India: Facebook, Mechanical Turk, and Qualtrics. Polit. Sci. Res. Methods 2020, 8, 232–250. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.D.; Perry, B.D. The post-traumatic response in children and adolescents. Psychiatr. Clin. N. Am. 1994, 17, 311–326. [Google Scholar] [CrossRef]
- De Souza, C.M.; Hidalgo, M.P.L. World Health Organization 5-item well-being index: Validation of the Brazilian Portuguese version. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 239–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDowell, I. Measures of self-perceived well-being. J. Psychosom. Res. 2010, 69, 69–79. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kammann, R.; Christie, D.; Irwin, R.; Dixon, G. Properties of an inentory to measure happiness. N. Z. Psychol. 1979, 8, 1–9. [Google Scholar]
- Diener, E. Assessing Well-Being. The Collected Works of Ed Diener. Soc. Indic. Res. Ser. 39 2009, 25–65. [Google Scholar]
- Levine, L.J.; Prohaska, V.; Burgess, S.L.; Rice, J.A.; Laulhere, T.M. Remembering past emotions: The role of current appraisals. Cogn. Emot. 2001, 15, 393–417. [Google Scholar] [CrossRef]
- Dwyer-Lindgren, L.; Mackenbach, J.P.; van Lenthe, F.J.; Mokdad, A.H. Self-reported general health, physical distress, mental distress, and activity limitation by US county, 1995–2012. Popul. Health Metr. 2017, 15, 1–12. [Google Scholar] [CrossRef]
- Ahmad, F.; Jhajj, A.K.; Stewart, D.E.; Burghardt, M.; Bierman, A.S. Single item measures of self-rated mental health: A scoping review. BMC Health Serv. Res. 2014, 14, 1–11. [Google Scholar] [CrossRef] [Green Version]
- DeCastellarnau, A. A classification of response scale characteristics that affect data quality: A literature review. Qual. Quant. 2018, 52, 1523–1559. [Google Scholar] [CrossRef]
- Larson, L.R.; Green, G.T.; Cordell, H.K. Children’s Time Outdoors: Results and Implications of the National Kids Survey. J. Park Recreat. Adm. 2011, 29, 1–20. [Google Scholar]
- U.S. Census Bureau Census Regions and Divisions of the United States. 2020. Available online: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf (accessed on 6 July 2020).
- Bland, J.M.; Altman, D.G. Multiple significance tests: The Bonferroni method. BMJ 1995, 310, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinholz, D.L.; Matz, R.L.; Cole, R.; Apkarian, N. STEM is not a monolith: A preliminary analysis of variations in STEM disciplinary cultures and implications for change. CBE Life Sci. Educ. 2019, 18, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L.M. Mental health in adolescence: Is America’s youth flourishing? Am. J. Orthopsychiatry 2006, 76, 395–402. [Google Scholar] [CrossRef]
- De Bellis, M.D.; Zisk, A. The Biological Effects of Childhood Trauma. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 185–222. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, N. Prolonged Stress Leads to Serious Health Problems: Preventive Approaches. Int. J. Health Sci. (Qassim.) 2016, 10, 5–6. [Google Scholar]
- Fairclough, S.J.; Boddy, L.M.; Mackintosh, K.A.; Valencia-Peris, A.; Ramirez-Rico, E. Weekday and weekend sedentary time and physical activity in differentially active children. J. Sci. Med. Sport 2015, 18, 444–449. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention Visiting Parks and Recreational Facilities: Protect Yourself and Others from COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/visitors.html (accessed on 6 July 2020).
- Kohl, H.W.; Hobbs, K.E. Development of Physical Activity Behaviors Among Children and Adolescents. Pediatrics 1998, 101, 549–554. [Google Scholar] [PubMed]
- Physical Activity Guidelines Advisory Committee Physical activity guidelines advisory committee report, 2008: To the Secretary of Health and Human Services. Nutr. Rev. 2009, 67, 114–120.
- Scott, D.; Willits, F.K. Adolescent and adult leisure patterns: A reassessment. J. Leis. Res. 1998, 30, 319–330. [Google Scholar] [CrossRef]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19–Related School Closings and Risk of Weight Gain Among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nisbet, E.K.; Zelenski, J.M. Underestimating nearby nature: Affective forecasting errors obscure the happy path to sustainability. Psychol. Sci. 2011, 22, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Buchecker, M.; Degenhardt, B. The effects of urban inhabitants’ nearby outdoor recreation on their well-being and their psychological resilience. J. Outdoor Recreat. Tour. 2015, 10, 55–62. [Google Scholar] [CrossRef]
- Isaacs, A.J.; Critchley, J.A.; Tai, S.S.; Buckingham, K.; Westley, D.; Harridge, S.D.R.; Smith, C.; Gottlieb, J.M. Exercise evaluation randomised trial (EXERT): A randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only. Health Technol. Assess. (Rockv.) 2007, 11, 1–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godbey, G. Outdoor Recreation, Health, and Wellness: Understanding and Enhancing the Relationship. SSRN 2009, RFF Discus, 1–42. [Google Scholar] [CrossRef] [Green Version]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Campbell, A.M. An increasing risk of family violence during the Covid-19 pandemic: Strengthening community collaborations to save lives. Forensic Sci. Int. Reports 2020, 2. [Google Scholar] [CrossRef]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dai, D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landsc. Urban Plan. 2011, 102, 234–244. [Google Scholar] [CrossRef]
- Gilman, R.; Huebner, S. A review of life satisfaction research with children and adolescents. Sch. Psychol. Q. 2003, 18, 192–205. [Google Scholar] [CrossRef]
- Rigolon, A. A complex landscape of inequity in access to urban parks: A literature review. Landsc. Urban Plan. 2016, 153, 160–169. [Google Scholar] [CrossRef]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities “just green enough”. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Rethink Outside: Blue Sky Funders Forum. Available online: https://rethinkoutside.org/about/ (accessed on 4 July 2020).
- Outdoors for All: Sierra Club. Available online: https://www.sierraclub.org/outdoors-for-all (accessed on 4 July 2020).
- Kim-Prieto, C.; Diener, E.; Tamir, M.; Scollon, C.; Diener, M. Integrating the diverse definitions of happiness: A time-sequential framework of subjective well-being. J. Happiness Stud. 2005, 6, 261–300. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Item | Subjective Well-Being Means | Subjective Well-Being Factor Loadings |
|---|---|---|
| Subjective well-being scale | 2.21 | |
| Cheerful and in good spirits | 2.25 | 0.87 |
| Calm and relaxed | 2.13 | 0.84 |
| Active and full of energy | 2.60 | 0.82 |
| Interested and curious about the world around me | 2.19 | 0.80 |
| Eigenvalue | 2.78 | |
| % of variance explained | 70% | |
| Chronbach’s alpha | 0.85 |
| Item | Activity Means | Nature-Based Factor | Outdoor Play Factor |
|---|---|---|---|
| Nature-based Activity Scale | 0.68 | ||
| Paddling (canoeing, kayaking) | 0.51 | 0.76 | 0.21 |
| Hunting | 0.36 | 0.76 | 0.03 |
| Camping | 0.71 | 0.73 | 0.21 |
| Fishing | 0.66 | 0.72 | 0.16 |
| Wildlife viewing | 0.81 | 0.70 | 0.24 |
| Hiking | 0.82 | 0.67 | 0.28 |
| Collecting (flowers, bugs, rocks, feathers, shells, leaves, seeds) | 0.71 | 0.64 | 0.27 |
| Playing in the woods (building forts, playing games in the woods) | 0.88 | 0.55 | 0.50 * |
| Outdoor Play Activity Scale | 1.20 | ||
| Bicycling outside | 1.22 | 0.23 | 0.76 |
| Going for walks or runs outside | 1.36 | 0.18 | 0.74 |
| Playing sports outside | 1.42 | 0.05 | 0.71 |
| Swimming outside | 1.16 | 0.17 | 0.67 |
| Skating (skateboard, rollerblades, scooter) | 0.84 | 0.42 * | 0.67 |
| Eigenvalues | 5.64 | 1.54 | |
| % of variance explained | 43% | 12% | |
| Chronbach’s alpha | 0.88 | 0.78 |
| Variable | Categories | N | % |
|---|---|---|---|
| Gender | Male | 306 | 49.0% |
| Female | 314 | 50.3% | |
| Non-binary | 3 | 0.5% | |
| Race | White | 373 | 59.8% |
| Black | 71 | 11.4% | |
| Hispanic | 78 | 12.5% | |
| Asian/Pacific Islander | 42 | 6.7% | |
| Native American | 6 | 1.0% | |
| Other | 6 | 1.0% | |
| Two or more races | 45 | 7.2% | |
| Age | 10 years | 78 | 12.5% |
| 11 years | 70 | 11.2% | |
| 12 years | 63 | 10.1% | |
| 13 years | 79 | 12.7% | |
| 14 years | 77 | 12.3% | |
| 15 years | 53 | 8.5% | |
| 16 years | 81 | 13.0% | |
| 17 years | 76 | 12.2% | |
| 18 years | 47 | 7.5% | |
| Community | Rural area | 126 | 20.2% |
| Small city or town | 126 | 20.2% | |
| Suburb near a large city | 228 | 36.5% | |
| Large city | 144 | 23.1% | |
| Region | South | 252 | 40.4% |
| West | 136 | 21.8% | |
| Midwest | 106 | 17.0% | |
| Northeast | 130 | 20.8% |
| Variable | Pre COVID-19 | Post COVID-19 | Paired t Test | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | p | |
| Subjective well-being | 2.21 | 0.616 | 1.75 | 0.750 | 14.870 | <0.001 |
| Mental health | 4.31 | 0.798 | 3.92 | 0.965 | 10.919 | <0.001 |
| Outdoor play activities | 1.20 | 0.545 | 0.68 | 0.566 | 18.333 | <0.001 |
| Nature-based activities | 0.68 | 0.540 | 0.41 | 0.492 | 13.526 | <0.001 |
| Outdoor family activities | 1.38 | 0.636 | 1.02 | 0.799 | 10.156 | <0.001 |
| General Outdoor Activities | 3.68 | 1.174 | 2.89 | 1.453 | 11.819 | <0.001 |
| Difference in SWB Score (Post-Pre) | B | Standard Error | Standard Beta | p |
|---|---|---|---|---|
| Pre COVID-19 SWB score | −0.44 | 0.04 | −0.35 | 0.000 *** |
| Pre COVID-19 participation in play-based activities | 0.30 | 0.08 | 0.21 | 0.000 *** |
| Pre COVID-19 participation in nature-based activities | −0.08 | 0.07 | −0.06 | 0.271 |
| Pre COVID-19 participation in outdoor family activities | −0.02 | 0.05 | −0.01 | 0.714 |
| Change in play-based activity participation during COVID-19 | 0.44 | 0.07 | 0.40 | 0.000 *** |
| Change in nature-based activity participation during COVID-19 | 0.21 | 0.09 | 0.14 | 0.016 * |
| Change in outdoor family activity participation during COVID-19 | 0.06 | 0.04 | 0.07 | 0.128 |
| Gender | −0.01 | 0.05 | −0.01 | 0.804 |
| Age | −0.00 | 0.01 | −0.00 | 0.941 |
| Income | 0.00 | 0.02 | 0.00 | 0.913 |
| Race: White (reference group) | ||||
| Black | 0.03 | 0.08 | 0.01 | 0.713 |
| Hispanic | 0.06 | 0.08 | 0.02 | 0.478 |
| Asian/Pacific Islander | 0.02 | 0.10 | 0.01 | 0.832 |
| Native American | −0.31 | 0.25 | −0.04 | 0.219 |
| Other | −0.29 | 0.25 | −0.04 | 0.246 |
| Prefer not to answer | −0.20 | 0.35 | −0.02 | 0.572 |
| Identify as more than one race | 0.02 | 0.10 | 0.01 | 0.851 |
| Community type: Suburbs near a large city (reference group) | ||||
| Rural area | −0.07 | 0.07 | −0.04 | 0.313 |
| Small city or town | 0.00 | 0.07 | 0.00 | 0.974 |
| Large city | −0.10 | 0.07 | −0.05 | 0.141 |
| Geographic region: South (reference group) | ||||
| West | −0.05 | 0.07 | −0.03 | 0.414 |
| Midwest | −0.03 | 0.07 | −0.01 | 0.723 |
| Northeast | 0.03 | 0.07 | −0.01 | 0.687 |
| Intercept | 0.59 | 0.14 | 0.000 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackson, S.B.; Stevenson, K.T.; Larson, L.R.; Peterson, M.N.; Seekamp, E. Outdoor Activity Participation Improves Adolescents’ Mental Health and Well-Being during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2506. https://doi.org/10.3390/ijerph18052506
Jackson SB, Stevenson KT, Larson LR, Peterson MN, Seekamp E. Outdoor Activity Participation Improves Adolescents’ Mental Health and Well-Being during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(5):2506. https://doi.org/10.3390/ijerph18052506
Chicago/Turabian StyleJackson, S. Brent, Kathryn T. Stevenson, Lincoln R. Larson, M. Nils Peterson, and Erin Seekamp. 2021. "Outdoor Activity Participation Improves Adolescents’ Mental Health and Well-Being during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 5: 2506. https://doi.org/10.3390/ijerph18052506