
Cognitive Diversity as the Quality of Leadership in Crisis: Team Performance in Health Service during the COVID-19 Pandemic



Abstract
:1. Introduction
1.1. Crisis Leadership
1.2. Team Performance
1.3. Cognitive Diversity
1.4. Decision-Making during a Crisis
2. Materials and Methods
2.1. Sampling
2.2. Variable Measures
3. Results
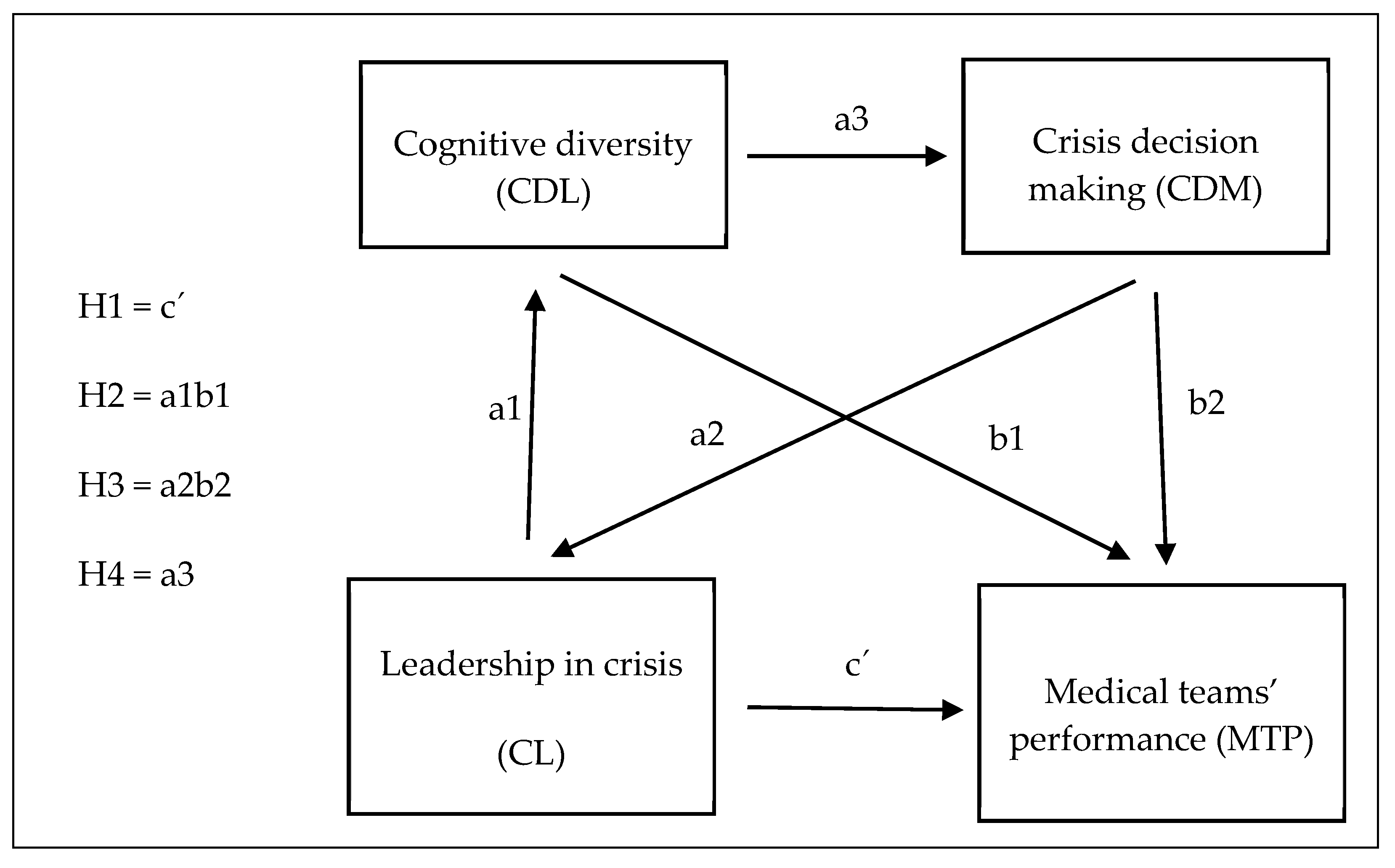
- There is a relationship between team performance (Y) and leadership competencies during a crisis (X).
- There is a relationship between mediator variables (M1, M2) and leadership competencies during a crisis (X).
- There is a relationship between team performance (Y) and mediator variables (M1, M2), in which X does not participate.
- C represents the total effect,
- the mediated (indirect) effect of X on Y by M1 and M2 is expressed in the form A1 * B1 + A2 * B2 + A1 * B2 * D21, where the term D21 is the path from M1 to M2,
- the difference C’ = C − A1 * B1 + A2 * B2 + A1 * B2 * D21 is the pure (direct) effect of X on Y without the participation of M.
- We have found that the relationships expressed by steps A and B are significant, so there are relationships of cognitive diversity of leadership in crisis (M1) and decision-making (M2) and leadership competencies (X) and at the same time there is a relationship between team efficiency (Y) and both mediator variables (M1, M2), in which X does not participate. As a result of the significance of these relations, a precondition for the existence of mediation arises.
- The product of parameters A1 * B1 + A2 * B2 + A1 * B2 * D21, where member D21 is the path from M1 to M2 is significant, so the indirect effect of leadership competencies (X) on team efficiency (Y) through decision-making, supported by cognitive diversity of leadership in crisis has been confirmed. The main hypothesis has thus been supported.
- Both indirect and direct effects are significant. In percentage terms, we can see that about 48% of the total effect is due to the direct effect and about 52% to the indirect effect. As the indirect effect does not reach more than 80% of the total effect, it is a partial mediation.
4. Discussion
5. Conclusions and Research Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Stacho, Z.; Stachová, K.; Papula, J.; Papulová, Z.; Kohnová, L. Effective communication in organisations increases their competitiveness. Pol. J. Manag. Stud. 2019, 19, 391–403. [Google Scholar] [CrossRef]
- Sfantou, D.F.; Laliotis, A.; Patelarou, A.E.; Sifaki-Pistolla, D.; Matalliotakis, M.; Patelarou, E. Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review. Healthcare 2017, 5, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squires, M.A.E.; Tourangeau, A.N.N.; Laschinger, H.K.S.; Doran, D. The link between leadership and safety outcomes in hospitals. J. Nurs. Manag. 2010, 18, 914–925. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.A.; Cummings, G.G. The relationship between nursing leadership and patient outcomes: A systematic review. J. Nurs. Manag. 2007, 15, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, L.R.; Chuang, Y.-T.; Berta, W.B.; Norton, P.G.; Ng, P.; Tregunno, D.; Richardson, J. The relationship between organizational leadership for safety and learning from patient safety events. Health Serv. Res. 2010, 45, 607–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pihlainen, V.; Kivinen, T.; Lammintakanen, J. Management and leadership competence in hospitals: A systematic literature review. Leadersh. Health Serv. 2016, 29, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Ackerly, D.C.; Sangvai, D.G.; Udayakumar, K.; Shah, B.R.; Kalman, N.S.; Cho, A.H.; Schulman, K.A.; Fulkerson, W.J.; Dzau, V.J. Training the next generation of physician—Executives: An innovative residency pathway in management and leadership. Acad. Med. 2011, 86, 575–579. [Google Scholar] [CrossRef]
- Enterkin, J.; Robb, E.; McLaren, S. Clinical leadership for high-quality care: Developing future ward leaders. J. Nurs. Manag. 2012, 21, 206–216. [Google Scholar] [CrossRef]
- Yoder-Wise, P.S. The future of leadership. JONA J. Nurs. Adm. 2014, 44, 318–320. [Google Scholar] [CrossRef]
- Procházková, K. Úroveň vlastností a osobnostných kvalít v kontexte rozvoja vodcovstva: Level of traits and qualities in the context of leadership development. Ekon. A Manaž. 2020, 17, 67–74. [Google Scholar]
- Chow, I.H.-S. Cognitive diversity and creativity in teams: The mediating roles of team learning and inclusion. Chin. Manag. Stud. 2018, 12, 369–383. [Google Scholar] [CrossRef]
- Mitchell, R.; Boyle, B.; O’Brien, R.; Malik, A.; Tian, K.; Parker, V.; Giles, M.; Joyce, P.; Chiang, V. Balancing cognitive diversity and mutual understanding in multidisciplinary teams. Healthc. Manag. Rev. 2017, 42, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Meissner, P.; Wulf, T. The effect of cognitive diversity on the illusion of control bias in strategic decisions: An experimental investigation. Eur. Manag. J. 2017, 35, 430–439. [Google Scholar] [CrossRef]
- Kim, T.; David, E.M.; Liu, Z. Perceived cognitive diversity and creativity: A multilevel study of motivational mechanisms and boundary conditions. J. Creat. Behav. 2020. [Google Scholar] [CrossRef] [Green Version]
- Hoever, I.J.; Van Knippenberg, D.; Van Ginkel, W.P.; Barkema, H.G. Fostering team creativity: Perspective taking as key to unlocking diversity’s potential. J. Appl. Psychol. 2012, 97, 982–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.J.; Kim, T.-Y.; Lee, J.-Y.; Bian, L. Cognitive team diversity and individual team member creativity: A cross-level interaction. Acad. Manag. J. 2012, 55, 197–212. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Zhang, Q. Development and validation of team creativity measures: A complex systems perspective. Creat. Innov. Manag. 2014, 23, 264–275. [Google Scholar] [CrossRef]
- Boin, A.; Stern, E.; Sundelius, B. The Politics of Crisis Management: Public Leadership under Pressure; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Helsloot, I.; Groenendaal, J. It’s meaning making, stupid! Success of public leadership during flash crises. J. Contingencies Crisis Manag. 2017, 25, 350–353. [Google Scholar] [CrossRef]
- Haddon, A.; Loughlin, C.; McNally, C. Leadership in a time of financial crisis: What do we want from our leaders? Leadersh. Organ. Dev. J. 2015, 36, 612–627. [Google Scholar] [CrossRef]
- Klein, K.J.; Ziegert, J.C.; Knight, A.P.; Xiao, Y. Dynamic delegation: Shared, hierarchical, and deindividualized leadership in extreme action teams. Adm. Sci. Q. 2006, 51, 590–621. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Faraj, S.; Sims, H.P., Jr. Contingent leadership and effectiveness of trauma resuscitation teams. J. Appl. Psychol. 2005, 90, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- Halverson, S.K.; Murphy, S.E.; Riggio, R.E. Charismatic Leadership in Crisis Situations. Small Group Res. 2004, 35, 495–514. [Google Scholar] [CrossRef]
- Procházková, K. Transformačné Vedenie v Slovenskej Manažérskej Praxi. Revue Mlad. Vedcov 2013, 154–156. [Google Scholar]
- James, E.H.; Wooten, L.P.; Dushek, K. Crisis Management: Informing a New Leadership Research Agenda. Acad. Manag. Ann. 2011, 5, 455–493. [Google Scholar] [CrossRef]
- Nembhard, I.M.; Edmondson, A.C. Making it safe: The effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams. J. Organ. Behav. 2006, 27, 941–966. [Google Scholar] [CrossRef]
- Liden, R.C.; Antonakis, J. Considering context in psychological leadership research. Hum. Relat. 2009, 62, 1587–1605. [Google Scholar] [CrossRef]
- Martínez-Córcoles, M. High reliability leadership: A conceptual framework. J. Contingencies Crisis Manag. 2018, 26, 237–246. [Google Scholar] [CrossRef]
- Bowers, M.R.; Hall, J.R.; Srinivasan, M.M. Organizational culture and leadership style: The missing combination for selecting the right leader for effective crisis management. Bus. Horiz. 2017, 60, 551–563. [Google Scholar] [CrossRef]
- Prochazkova, K. Vplyv Kultúry Na Vedenie Medzinárodných Tímov. Zmeny Uplatňovaní Manaz. Funkc. Kontexte štvrtej Priem. Revoluc. Adapt. Procesy Podn. Slov. I. Recenzovaný Zb. Ved. Statí 2020, 1, 47–55. [Google Scholar]
- Baran, B.E.; Scott, C.W. Organizing ambiguity: A grounded theory of leadership and sensemaking within dangerous contexts. Mil. Psychol. 2010, 22, S42–S69. [Google Scholar] [CrossRef]
- Wooten, L.P.; James, E.H. Linking Crisis Management and Leadership Competencies: The Role of Human Resource Development. Adv. Dev. Hum. Resour. 2008, 10, 352–379. [Google Scholar] [CrossRef] [Green Version]
- Furst, S.A.; Reeves, M. Queens of the Hill: Creative Destruction and the Emergence of Executive Leadership of Women. Leadersh. Q. 2008, 19, 372–384. [Google Scholar] [CrossRef]
- Schoenberg, A. Do crisis plans matter? A new perspective on leading during a crisis. Public Relat. Q. 2005, 50, 2–6. [Google Scholar]
- Madera, J.M.; Smith, D.B. The Effects of Leader Negative Emotions on Evaluations of Leadership in a Crisis Sit-uation: The Role of Anger and Sadness. Leadersh. Q. 2009, 20, 103–114. [Google Scholar] [CrossRef]
- Kolbe, M.; Burtscher, M.J.; Wacker, J.; Grande, B.; Nohynkova, R.; Manser, T.; Spahn, D.R.; Grote, G. Speaking up is related to better team performance in simulated anesthesia inductions: An observational study. Anesth. Analg. 2012, 115, 1099–1108. [Google Scholar] [CrossRef] [Green Version]
- Mission Command: Applying Principles of Military Leadership to the SARS-CoV-2 (COVID-19) Crisis. Available online: https://militaryhealth.bmj.com/content/167/1/3.info (accessed on 11 March 2021).
- Wade, G.H.; Osgood, B.; Avino, K.; Bucher, G.; Bucher, L.; Foraker, T.; French, D.; Sirkowski, C. Influence of organizational characteristics and caring attributes of managers on nurses’ job enjoyment. J. Adv. Nurs. 2008, 64, 344–353. [Google Scholar] [CrossRef]
- Kilduff, M.; Angelmar, R.; Mehra, A. Top management-team diversity and firm performance: Examining the role of cognitions. Organ. Sci. 2000, 11, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Van Der Vegt, G.S.; Janssen, O. Joint impact of interdependence and group diversity on innovation. J. Manag. 2003, 29, 729–751. [Google Scholar] [CrossRef]
- Martins, L.L.; Schilpzand, M.C.; Kirkman, B.L.; Ivanaj, S.; Ivanaj, V. A Contingency view of the effects of cognitive diversity on team performance: The moderating roles of team psychological safety and relationship conflict. Small Group Res. 2012, 44, 96–126. [Google Scholar] [CrossRef]
- Van Der Vegt, G.S.; Bunderson, J.S.; Oosterhof, A. Expertness diversity and interpersonal helping in teams: Why those who need the most help end up getting the least. Acad. Manag. J. 2006, 49, 877–893. [Google Scholar] [CrossRef]
- Cox, T.H.; Blake, S. Managing cultural diversity: Implications for organizational competitiveness. Acad. Manag. Perspect. 1991, 5, 45–56. [Google Scholar] [CrossRef]
- Horwitz, S.K. The compositional impact of team diversity on performance: Theoretical considerations. Hum. Resour. Dev. Rev. 2005, 4, 219–245. [Google Scholar] [CrossRef]
- Harrison, D.A.; Klein, K.J. What’s the difference? Diversity constructs as separation, variety, or disparity in organizations. Acad. Manag. Rev. 2007, 32, 1199–1228. [Google Scholar] [CrossRef] [Green Version]
- Miller, C.C.; Burke, L.M.; Glick, W.H. Cognitive diversity among upper-echelon executives: Implications for strategic decision processes. Strateg. Manag. J. 1998, 19, 39–58. [Google Scholar] [CrossRef] [Green Version]
- Pieterse, A.N.; van Knippenberg, D.; van Ginkel, W.P. Diversity in goal orientation, team reflexivity, and team performance. Organ. Behav. Hum. Decis. Process. 2011, 114, 153–164. [Google Scholar] [CrossRef]
- Milliken, F.J.; Martins, L.L. Searching for common threads: Understanding the multiple effects of diversity in organizational groups. Acad. Manag. Rev. 1996, 21, 402–433. [Google Scholar] [CrossRef] [Green Version]
- Van Knippenberg, D.; Schippers, M. Work group diversity. Annu. Rev. Psychol. 2007, 58, 515–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak, R. The effects of cognitive diversity and cohesiveness on absorptive capacity. Int. J. Innov. Manag. 2019, 24, 2050019. [Google Scholar] [CrossRef]
- Friedrich, A.L.; Brav, A. Job design for learning in work groups. J. Work. Learn. 2007, 19, 269–285. [Google Scholar] [CrossRef]
- Van Knippenberg, D. Team innovation. Annu. Rev. Organ. Psychol. Organ. Behav. 2017, 4, 211–233. [Google Scholar] [CrossRef]
- Marcel, J.J.; Barr, P.S.; Duhaime, I.M. The influence of executive cognition on competitive dynamics. Strat. Manag. J. 2011, 32, 115–138. [Google Scholar] [CrossRef]
- Bakonyi, Z. Why do firms centralise their strategic decision-making during crisis? A qualitative study. J. Organ. Chang. Manag. 2018, 31, 1191–1205. [Google Scholar] [CrossRef]
- Aghion, P.; Bloom, N.; van Reenen, J. Incomplete Contracts and the Internal Organization of Firms; National Bureau of Economic Research, Inc.: Cambridge, MA, USA, 2013. [Google Scholar]
- Higgins, G.; Freedman, J. Improving decision making in crisis. J. Bus. Contin. Emerg. Plan. 2013, 7, 65–76. [Google Scholar]
- Markman, A. Slow Down to Make Better Decisions in a Crisis. Coronavirus and Business: The Insights You Need from Harvard Business Review. 2020. Available online: https://hbr.org/2020/03/slow-down-to-make-better-decisions-in-a-crisis (accessed on 11 March 2021).
- Hirsh, J.B.; Mar, R.A.; Peterson, J.B. Psychological entropy: A framework for understanding uncertainty-related anxiety. Psychol. Rev. 2012, 119, 304–320. [Google Scholar] [CrossRef] [Green Version]
- Reeves, M.; Lang, N.; Carlsson-Szlezak, P. Lead Your Business through the Coronavirus Crisis. Harv. Bus. Rev. 2020, 27, 2–7. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Kash, B.A.; Cheon, O.; Halzack, N.M.; Miller, T.R. Measuring team effectiveness in the health care setting: An inventory of survey tools. Health Serv. Insights 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- McGuire, M.J.; Noronha, G.; Samal, L.; Yeh, H.-C.; Crocetti, S.; Kravet, S. Patient safety perceptions of primary care providers after implementation of an electronic medical record system. J. Gen. Intern. Med. 2013, 28, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P.; Luecken, L.J. How and for whom? Mediation and moderation in health psychology. Health Psychol. 2008, 27, S99–S100. [Google Scholar] [CrossRef] [Green Version]
- Bloom, N.; Propper, C.; Seiler, S.; Van Reenen, J. *** Article Withdrawn*** Management Practices in Hospitals; HEDG, c/o Department of Economics, University of York: York, UK, 2009. [Google Scholar]
- Veronesi, G.; Kirkpatrick, I.; Vallascas, F. Clinicians on the board: What difference does it make? Soc. Sci. Med. 2013, 77, 147–155. [Google Scholar] [CrossRef]
- Lega, F.; Prenestini, A.; Spurgeon, P. Is management essential to improving the performance and sustainability of health care systems and organizations? A systematic review and a roadmap for future studies. Value Health 2013, 16, S46–S51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vainieri, M.; Ferrè, F.; Giacomelli, G.; Nuti, S. Explaining performance in health care: How and when top management competencies make the difference. Heathc. Manag. Rev. 2019, 44, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, C.; Nakhate, D.V.; Rautrao, M.R.R. Role of HR trends in corona-crisis management and organizational sustainability readiness. Int. J. Adv. Sci. Technol. 2020, 29, 2278–2286. [Google Scholar]


{kind=link}
| Variable | Category | Frequency | Percentage | Variable | Category | Frequency | Percentage |
|---|---|---|---|---|---|---|---|
| Number of employees | up to 10 | 10 | 4.6 | Ownership | private | 92 | 42.6 |
| 11–50 | 24 | 11.1 | public | 124 | 57.4 | ||
| 51 to 250 | 86 | 39.8 | Total | 216 | 100 | ||
| over 250 | 69 | 44.4 | |||||
| Total | 216 | 100 | |||||
| Position | Informed employee | 54 | 25 | Years of experience as team leader | Less than 1 year | 2 | 0.9 |
| low mgmt. | 46 | 21.3 | Up to 5 years | 10 | 4.6 | ||
| middle mgmt. | 92 | 42.6 | 6 to 10 years | 48 | 22.2 | ||
| top mgmt. | 24 | 11.1 | over 10 years | 156 | 72.2 | ||
| Total | 216 | 100 | Total | 216 | 100 | ||
| gender | male | 90 | 41.7 | Age of leaders | up to 30 years | ||
| female | 126 | 58.3 | from 30 to 50 years | ||||
| total | 216 | 100 | over 50 years | ||||
| Total | |||||||
| Education | secondary | 10 | 4.6 | ||||
| specialized managerial | 32 | 14.8 | |||||
| university 1st degree | 6 | 2.8 | |||||
| university 2nd degree | 124 | 57.4 | |||||
| university 3rd degree | 44 | 20.4 | |||||
| Total | 216 | 100 | |||||
| Crisis Leadership 1 = Strongly Disagree and 5 = Strongly Agree | Team Efficiency 1 = Strongly Disagree and 5 = Strongly Agree |
|---|---|
|
|
| Cognitive diversity1 = strongly disagree and 5 = strongly agree | |
| I assume that individual people who are part of leadership in crises are different from each other in the way of thinking, their knowledge and skills, the way they see the world, their beliefs about what is right or what is wrong. | |
| Decision-making during a crisis 1 = strongly disagree and 5 = strongly agree | |
| |
| Variable | Mean | SD | CL | CDM | CDL | MTP | Age | Gender | Position | Experience | Size | Education |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CL | 3.39 | 1.14 | ||||||||||
| CDM | 3.64 | 1.12 | 0.940 ** | |||||||||
| CDL | 3.73 | 0.97 | 0.395 ** | 0.355 ** | ||||||||
| MTP | 3.66 | 1.06 | 0.891 ** | 0.888 ** | 0.501 ** | |||||||
| Age | 2.22 | 0.53 | 0.250 ** | 0.228 ** | 0.079 | 0.243 ** | ||||||
| Gender | 1.58 | 0.49 | 0.351 ** | 0.320 ** | 0.005 | 0.316 ** | 0.035 | |||||
| Position | 2.40 | 0.98 | 0.314 ** | 0.329 ** | −0.018 | 0.186 ** | 0.203 ** | −0.040 | ||||
| Experience | 3.66 | 0.61 | 0.264 ** | 0.245 ** | 0.271 ** | 0.263 ** | 0.518 ** | 0.049 | 0.212 ** | |||
| Facility Size | 2.24 | 0.83 | −0.044 | −0.047 | −0.047 | 0.029 | −0.058 | 0.163 ** | −0.038 | 0.163 ** | ||
| Education | 4.56 | 1.44 | −0.180 ** | −0.142 ** | −0.038 | −0.204 ** | −0.052 | −0.092 | 0.145 ** | −0.079 | −0.144 ** | |
| Sphere | 1.57 | 0.494 | −0.257 ** | −0.253 ** | −0.352 ** | −0.268 ** | −0.238 ** | 0.032 | 0.140 ** | −0.115 ** | 0.410 ** | 0.046 |
| Source | Type III Sum of Squares | df | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Corrected Model | 199,192 | 16 | 12,449 | 57,616 | 0.000 |
| Intercept | 1096 | 1 | 1096 | 5071 | 0.025 |
| Sphere | 0.281 | 1 | 0.281 | 1300 | 0.256 |
| Age | 0.054 | 1 | 0.054 | 0.249 | 0.618 |
| Gender | 0.052 | 1 | 0.052 | 0.243 | 0.623 |
| Position | 2111 | 1 | 2111 | 9768 | 0.002 |
| Experience | 0.009 | 1 | 0.009 | 0.040 | 0.842 |
| Size | 1484 | 1 | 1484 | 6868 | 0.009 |
| Education | 0.003 | 1 | 0.003 | 0.012 | 0.913 |
| Leadership | 112,583 | 1 | 112,583 | 521,036 | 0.000 |
| Error | 42,999 | 199 | 0.216 | ||
| Total | 3,138,350 | 216 | |||
| Corrected Total | 242,191 | 215 |
| Model 1/Step C | ||||||
| Dependent Variable: Result | ||||||
| Parameter | B | Std. Error | t | Sig. | 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||||
| Intercept | 0.820 | 0.145 | 5.651 | 0.000 | 0.534 | 1.106 |
| Leadership | 0.861 | 0.029 | 29.202 | 0.000 | 0.803 | 0.919 |
| Model 2/Step A | ||||||
| Dependent Variable: Cognitive Diversity of Leadership in Crisis | ||||||
| Parameter | B | Std. Error | t | Sig. | 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||||
| Intercept | 3.005 | 0.280 | 10.725 | 0.000 | 2.453 | 3.557 |
| Leadership | 0.344 | 0.057 | 6.042 | 0.000 | 0.232 | 0.456 |
| Model 3/Step A | ||||||
| Dependent Variable: Decision-making | ||||||
| Parameter | B | Std. Error | t | Sig. | 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||||
| Intercept | 0.365 | 0.147 | 2.479 | 0.014 | 0.075 | 0.656 |
| Leadership | 0.904 | 0.026 | 34.619 | 0.000 | 0.853 | 0.955 |
| Model 4/Step B | ||||||
| Dependent Variable: Result | ||||||
| Parameter | B | Std. Error | t | Sig. | 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||||
| Intercept | 0.017 | 0.155 | 0.107 | 0.915 | −0.289 | 0.322 |
| Leadership | 0.414 | 0.070 | 5.922 | 0.000 | 0.276 | 0.552 |
| Cognitive Diversity | 0.205 | 0.030 | 6.791 | 0.000 | 0.146 | 0.265 |
| Decision-making | 0.412 | 0.071 | 5.776 | 0.000 | 0.271 | 0.552 |
| Indirect effect | ||||||
| A1 * B1 | 0.071 | |||||
| A2 * B2 | 0.372 | |||||
| A1 * B2 * D21 | 0.004 | |||||
| Indirect | 0.447 | |||||
| z | 6.652 | |||||
| Sig. | 0.000 | |||||
| Effect | Coefficient | % | ||||
| Total | 0.861 | 100 | ||||
| Direct | 0.414 | 48 | ||||
| Indirect | 0.447 | 52 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joniaková, Z.; Jankelová, N.; Blštáková, J.; Némethová, I. Cognitive Diversity as the Quality of Leadership in Crisis: Team Performance in Health Service during the COVID-19 Pandemic. Healthcare 2021, 9, 313. https://doi.org/10.3390/healthcare9030313
Joniaková Z, Jankelová N, Blštáková J, Némethová I. Cognitive Diversity as the Quality of Leadership in Crisis: Team Performance in Health Service during the COVID-19 Pandemic. Healthcare. 2021; 9(3):313. https://doi.org/10.3390/healthcare9030313
Chicago/Turabian StyleJoniaková, Zuzana, Nadežda Jankelová, Jana Blštáková, and Ildikó Némethová. 2021. "Cognitive Diversity as the Quality of Leadership in Crisis: Team Performance in Health Service during the COVID-19 Pandemic" Healthcare 9, no. 3: 313. https://doi.org/10.3390/healthcare9030313