
Modelling Analysis of COVID-19 Transmission and the State of Emergency in Japan


Abstract
:1. Introduction
2. Methods
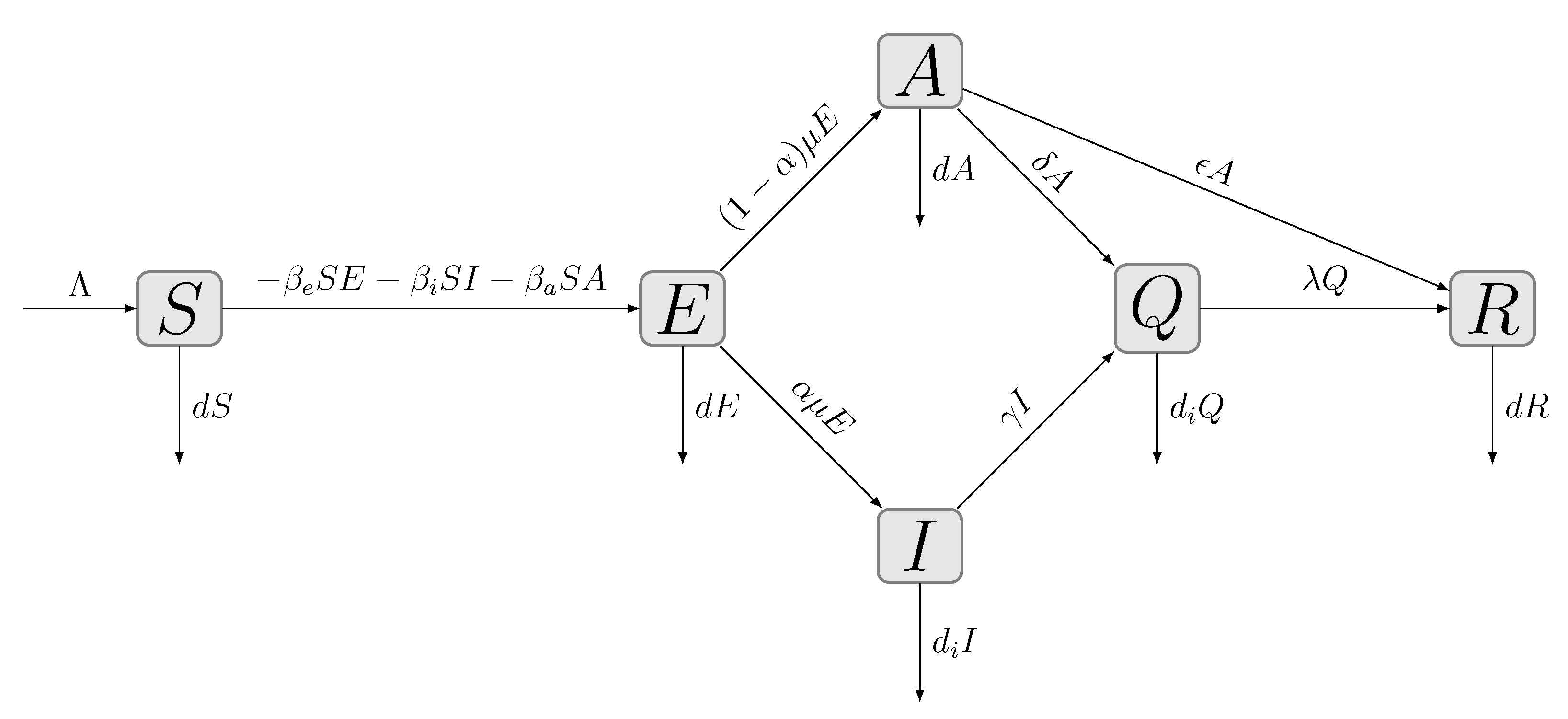
2.1. Model Description
2.2. Determination of the Transmission Parameters
2.3. COVID-19 Data and Stages for Analysis
3. Results
3.1. Simulated Results and Determined Model Parameters
3.2. Fitting of the Transmission Parameters
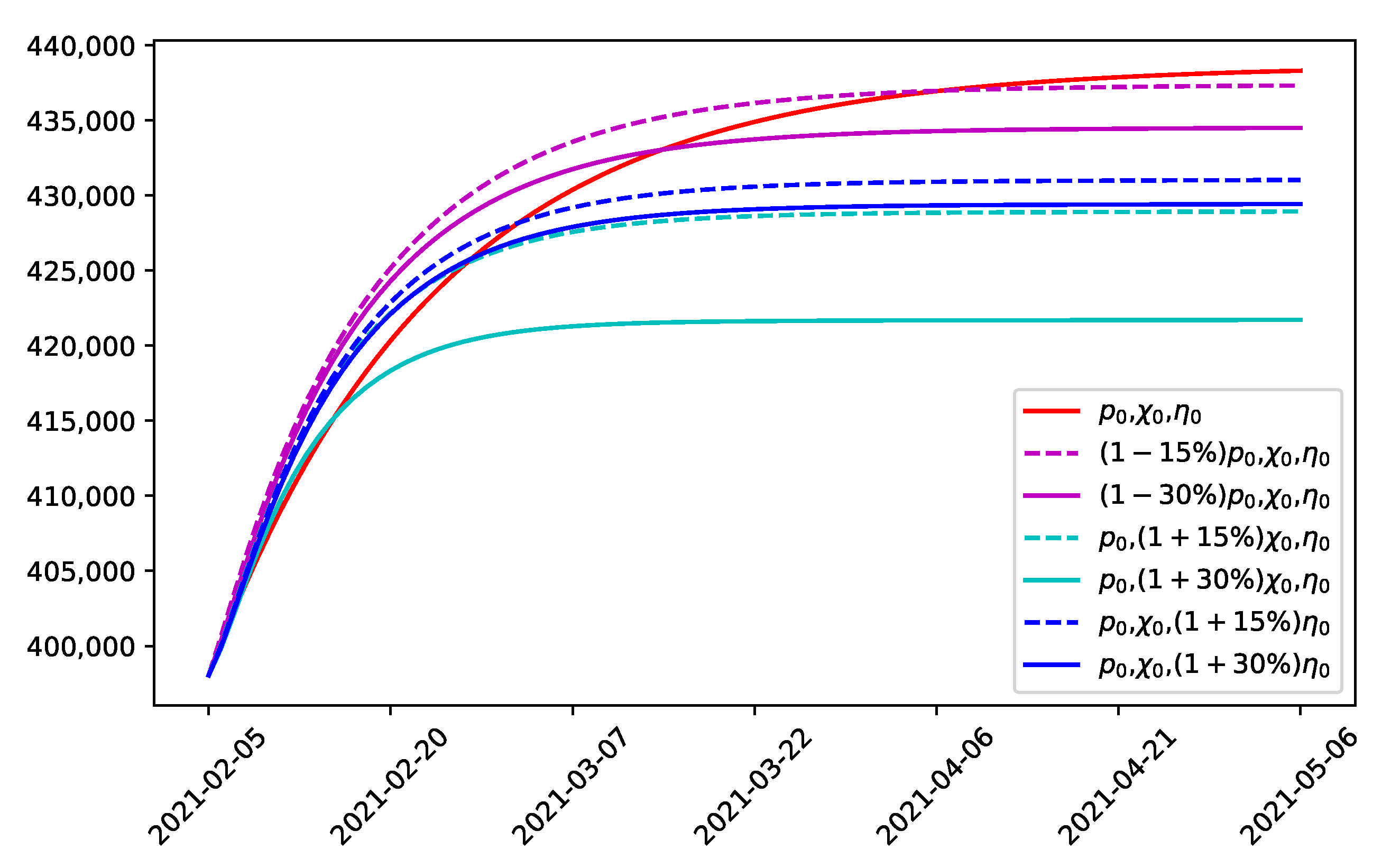
3.3. Prediction of Cumulative Confirmed Cases and Effect of Combined Strategies
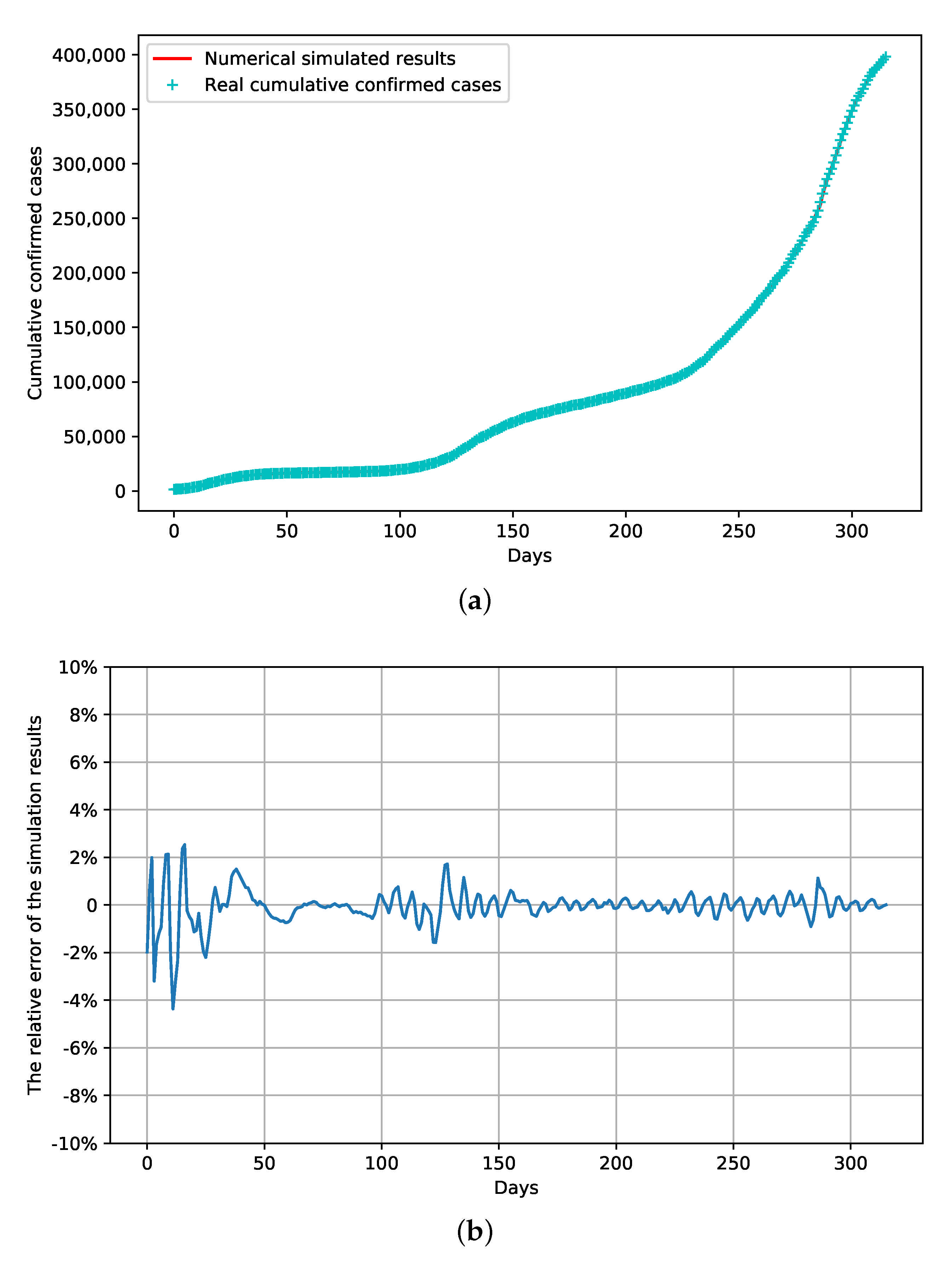
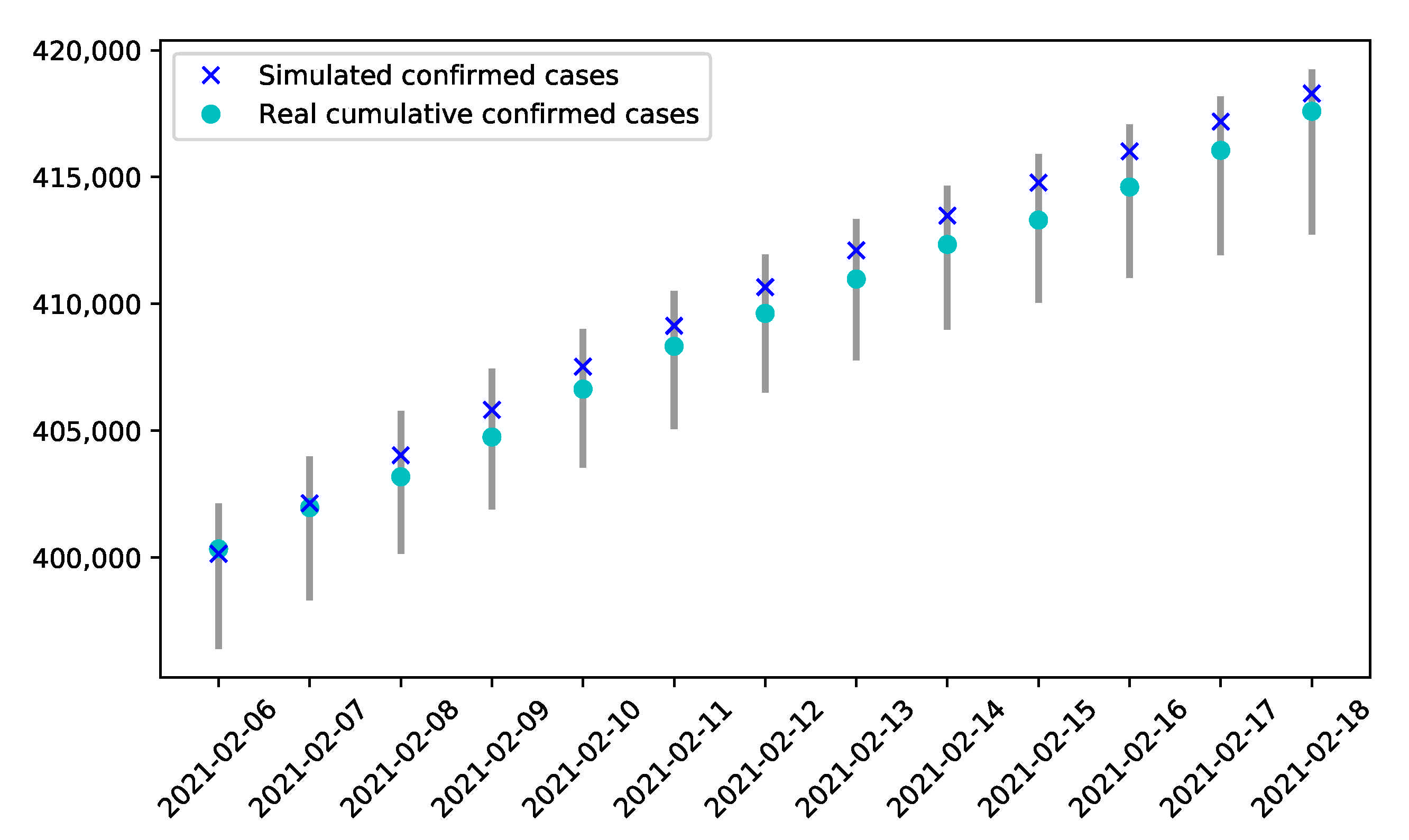
3.4. Verification of the Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in wuhan, china. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R. A novel coronavirus from patients with pneumonia in china, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Global Cumulative Confirmed Covid-19 Deaths and Cases, Who. Available online: https://covid19.who.int/ (accessed on 18 May 2021).
- Djaoue, S.; Kolaye, G.G.; Abboubakar, H.; Ari, A.A.A.; Damakoa, I. Mathematical modeling, analysis and numerical simulation of the COVID-19 transmission with mitigation of control strategies used in Cameroon. Chaos Solitons Fractals 2020, 139, 110281. [Google Scholar] [CrossRef] [PubMed]
- González-Bustamante, B. Evolution and early government responses to covid-19 in south america. World Dev. 2021, 137, 105180. [Google Scholar] [CrossRef] [PubMed]
- Karako, K.; Song, P.; Chen, Y.; Tang, W. Analysis of covid-19 infection spread in japan based on stochastic transition model. Biosci. Trends 2020, 14, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Y.; Li, Z.; Chua, Y.X.; Chaw, W.L.; Zhao, Z.; Er, B.; Pung, R.; Chiew, C.J.; Lye, D.C.; Heng, D. Evaluation of the effectiveness of surveillance and containment measures for the first 100 patients with covid-19 in singapore—2 January–29 February 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 307–311. [Google Scholar] [CrossRef]
- Panovska-Griffiths, J.; Kerr, C.C.; Stuart, R.M.; Mistry, D.; Klein, D.J.; Viner, R.M.; Bonell, C. Determining the optimal strategy for reopening schools, the impact of test and trace interventions, and the risk of occurrence of a second covid-19 epidemic wave in the uk: A modelling study. Lancet Child Adolesc. Health 2020, 4, 817–827. [Google Scholar] [CrossRef]
- Wells, C.R.; Townsend, J.P.; Pandey, A.; Moghadas, S.M.; Krieger, G.; Singer, B.; McDonald, R.H.; Fitzpatrick, M.C.; Galvani, A.P. Optimal covid-19 quarantine and testing strategies. Nat. Commun. 2021, 12, 356. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Chiew, C.J.; Lee, V.J. Can we contain the covid-19 outbreak with the same measures as for SARS? Lancet Infect. Dis. 2020, 20, e102–e107. [Google Scholar] [CrossRef] [Green Version]
- The First Reported Confirmed Case in Japan Announced by the Minstry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/stf/newpage_08906.html (accessed on 18 May 2021).
- The Basic Polices for Novel Coronavirus Disease Control by the Government of Japan. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html (accessed on 18 May 2021).
- The Current Covid-19 Situation in Japan, Who. Available online: https://www.who.int/countries/jpn/ (accessed on 18 May 2021).
- Declaration of a State of Emergency in Response to the Novel Coronavirus Disease (January 13). Available online: https://japan.kantei.go.jp/ongoingtopics/_00039.html (accessed on 18 May 2021).
- Kuniya, T. Prediction of the epidemic peak of coronavirus disease in japan, 2020. J. Clin. Med. 2020, 9, 789. [Google Scholar] [CrossRef] [Green Version]
- Carcione, J.M.; Santos, J.E.; Bagaini, C.; Ba, J. A simulation of a covid-19 epidemic based on a deterministic SEIR model. Front. Public Health 2020, 8, 230. [Google Scholar] [CrossRef]
- Jiao, J.; Liu, Z.; Cai, S. Dynamics of an SEIR model with infectivity in incubation period and homestead-isolation on the susceptible. Appl. Math. Lett. 2020, 107, 106442. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Flasche, S.; Clifford, S.; Pearson, C.A.; Munday, J.D. The effect of control strategies to reduce social mixing on outcomes of the covid-19 epidemic in wuhan, china: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Zeng, Z.; Wang, K.; Wong, S.-S.; Liang, W.; Zanin, M.; Liu, P.; Cao, X.; Gao, Z.; Mai, Z. Modified SEIR and ai prediction of the epidemics trend of covid-19 in china under public health interventions. J. Thorac. Dis. 2020, 12, 165. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Sutton, D.; Fuchs, K.; D’alton, M.; Goffman, D. Universal screening for SARS-CoV-2 in women admitted for delivery. N. Engl. J. Med. 2020, 382, 2163–2164. [Google Scholar] [CrossRef]
- Peto, J. Covid-19 mass testing facilities could end the epidemic rapidly. BMJ 2020, 368, m1163. [Google Scholar] [CrossRef] [Green Version]
- Death Rate of Japan. Available online: https://www.macrotrends.net/countries/JPN/japan/death-rate (accessed on 18 May 2021).
- Allen, L.J.; Van den Driessche, P. The basic reproduction number in some discrete-time epidemic models. J. Differ. Equ. Appl. 2008, 14, 1127–1147. [Google Scholar] [CrossRef]
- Official Statistics of Covid-19 from the Japanese Government. Available online: https://www.mhlw.go.jp/stf/covid-19/open-data.html (accessed on 18 May 2021).
- Basic Policies to Contain the Covid-19 Spread in Japan. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html (accessed on 18 May 2021).
- Declaration of the State of Emergency in Several Prefectures. Available online: https://japan.kantei.go.jp/ongoingtopics/_00018.html (accessed on 18 May 2021).
- The Declaration of the State of Emergency Nationwide. Available online: https://japan.kantei.go.jp/ongoingtopics/_00020.html (accessed on 18 May 2021).
- The Promotion of Contact Confirming Application. Available online: https://www.mhlw.go.jp/stf/newpage_11954.html (accessed on 18 May 2021).
- Salivapcr Testing for Asymptomatic Infection. Available online: https://www.mhlw.go.jp/stf/newpage_12488.html (accessed on 18 May 2021).
- Strengthened the pcr Testing. Available online: https://www.mhlw.go.jp/stf/newpage_12892.html (accessed on 18 May 2021).
- Announced the Employment Subsidy. Available online: https://www.mhlw.go.jp/stf/houdou/houdou_list_202008.html (accessed on 18 May 2021).
- Extended Applications for Subsidies for Business Suspension. Available online: https://www.mhlw.go.jp/stf/newpage_13766.html (accessed on 18 May 2021).
- Ensured the Vacation and Welfare of the Patients. Available online: https://www.mhlw.go.jp/stf/newpage_13997.html (accessed on 18 May 2021).
- Abandoned the Policy of the Two-Week Quarantine Upon Entry. Available online: https://www.sohu.com/a/423581473_120707383 (accessed on 18 May 2021).
- Signed an Agreement on Provision of Information Sharing of Cluster Countermeasures for Covid-19. Available online: https://www.mhlw.go.jp/stf/newpage_14984.html (accessed on 18 May 2021).
- Announcement to Send Additional Medical Staff from the Self-Defense Forces. Available online: https://www.asahi.com/articles/ASND73G6NND7IIPE007.html (accessed on 18 May 2021).
- The Declaration of the Second State of Emergency. Available online: https://www.mhlw.go.jp/stf/newpage_15933.html (accessed on 18 May 2021).
- Declared the Second Nationwide State of Emergency. Available online: https://japan.kantei.go.jp/ongoingtopics/_00039.html (accessed on 18 May 2021).
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence that D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef]
- Meyerowitz, E.A.; Richterman, A.; Bogoch, I.I.; Low, N.; Cevik, M. Towards an accurate and systematic characterisation of persistently asymptomatic infection with SARS-CoV-2. Lancet Infect Dis. 2021, 21, e163–e169. [Google Scholar] [CrossRef]
- González-Rubio, J.; Navarro-López, C.; López-Nájera, E.; López-Nájera, A.; Jiménez-Díaz, L.; Navarro-López, J.D.; Nájera, A. A systematic review and meta-analysis of hospitalised current smokers and covid-19. Int. J. Environ. Res. Public Health 2020, 17, 7394. [Google Scholar] [CrossRef] [PubMed]
- Zhan, X.X.; Liu, C.; Zhou, G.; Zhang, Z.K.; Sun, G.Q.; Zhu, J.J.; Jin, Z. Coupling dynamics of epidemic spreading and information diffusion on complex networks. Appl. Math. Comput. 2018, 332, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H. Japanese strategy to COVID-19: How does it work? Glob. Health Med. 2020, 2, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Yen, Y.F.; Yu, S.H.; Su, E.C. An Examination on the Transmission of COVID-19 and the Effect of Response Strategies: A Comparative Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5687. [Google Scholar] [CrossRef]
- Akamatsu, T.; Nagae, T.; Osawa, M.; Satsukawa, K.; Sakai, T.; Mizutani, D. Model-based analysis on social acceptability and feasibility of a focused protection strategy against the COVID-19 pandemic. Sci. Rep. 2021, 11, 2003. [Google Scholar] [CrossRef]
- Nakano, T.; Ikeda, Y. Novel Indicator to Ascertain the Status and Trend of COVID-19 Spread: Modeling Study. J. Med. Internet. Res. 2020, 22, e20144. [Google Scholar] [CrossRef]
- Tanaka, T.; Yamaguchi, T.; Sakamoto, Y. Estimation of the percentages of undiagnosed patients of the novel coronavirus (SARS-CoV-2) infection in Hokkaido, Japan by using birth-death process with recursive full tracing. PLoS ONE 2020, 15, e0241170. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Period | Note |
|---|---|---|
| 1 | 2020.01.06–03.27 | The first case appeared in Japan [11]. |
| 2 | 2020.03.28–04.06 | A series of basic policies were announced [27]. |
| 3 | 2020.04.07–04.15 | Declared the state of emergency in several prefectures [28]. |
| 4 | 2020.04.16–05.25 | Declared the first nationwide state of emergency [29]. |
| 5 | 2020.05.26–06.18 | Lifted the state of emergency [12]. |
| 6 | 2020.06.19–07.16 | Promoted cellphone app for contact information [30]. |
| 7 | 2020.07.17–08.07 | Started saliva PCR testing to detect asymptomatic infection [31]. |
| 8 | 2020.08.08–08.24 | Strengthened the testing intensity [32]. |
| 9 | 2020.08.25–09.25 | Announced employment subsidy [33]. |
| 10 | 2020.09.26–10.08 | Extended applications for subsidies for business suspension [34]. |
| 11 | 2020.10.09–11.01 | Ensured the vacation and welfare of the patients [35]. |
| 12 | 2020.11.02–11.20 | Abandoned two-week quarantine policy upon entry [36]. |
| 13 | 2020.11.21–12.07 | Signed an agreement on provision of information sharing of cluster countermeasures for COVID-19 [37]. |
| 14 | 2020.12.08–2021.01.07 | Announced to send additional medical staffs [38]. |
| 15 | 2021.01.08–01.15 | Declared another state of emergency in several prefectures [39]. |
| 16 | 2021.01.16–02.18 | Declared the second nationwide state of emergency [40]. |
| Stage | (per day) | (per day) | (per day) | |||
|---|---|---|---|---|---|---|
| 1 | 0.0858 | 0.2183 | 0.3217 | 0.1 | 0.5244 | 0.2057 |
| 2 | 0.1635 | 0.4668 | 0.5562 | 0.1712 | 0.6374 | 0.3701 |
| 3 | 0.0849 | 0.1933 | 0.2357 | 0.2074 | 0.4771 | 0.3829 |
| 4 | 0.0534 | 0.1929 | 0.1800 | 0.2274 | 0.4603 | 0.5485 |
| 5 | 0.0971 | 0.3404 | 0.3103 | 0.1232 | 0.3188 | 0.3695 |
| 6 | 0.1213 | 0.4235 | 0.3864 | 0.1295 | 0.3238 | 0.3304 |
| 7 | 0.1015 | 0.3625 | 0.3175 | 0.1251 | 0.3839 | 0.2930 |
| 8 | 0.0335 | 0.1394 | 0.1371 | 0.1002 | 0.6536 | 0.1275 |
| 9 | 0.0478 | 0.1317 | 0.1165 | 0.1019 | 0.9107 | 0.1020 |
| 10 | 0.0491 | 0.1305 | 0.1976 | 0.1128 | 0.1374 | 0.1877 |
| 11 | 0.0742 | 0.2187 | 0.2113 | 0.1121 | 0.7453 | 0.1655 |
| 12 | 0.0867 | 0.2727 | 0.2929 | 0.2215 | 0.4233 | 0.1700 |
| 13 | 0.0724 | 0.2574 | 0.1623 | 0.1006 | 0.9378 | 0.1273 |
| 14 | 0.0633 | 0.2795 | 0.1932 | 0.1042 | 0.0588 | 0.1625 |
| 15 | 0.0489 | 0.1721 | 0.1897 | 0.1001 | 0.5687 | 0.1969 |
| 16 | 0.0444 | 0.1613 | 0.1585 | 0.1000 | 0.6152 | 0.2652 |
| Stage | 95% CI | Stage | 95% CI | ||
|---|---|---|---|---|---|
| 1 | 1.52 | (1.47, 2.12) | 9 | 0.86 | (0.83, 0.88) |
| 2 | 1.99 | (1.90, 2.27) | 10 | 1.03 | (0.96, 1.12) |
| 3 | 0.92 | (0.83, 1.00) | 11 | 1.2 | (1.16, 1.26) |
| 4 | 0.59 | (0.53, 0.61) | 12 | 1.52 | (1.46, 1.63) |
| 5 | 1.23 | (1.19, 1.27) | 13 | 1.12 | (1.01, 1.15) |
| 6 | 1.61 | (1.56, 1.67) | 14 | 1.44 | (1.31, 1.92) |
| 7 | 1.39 | (1.37, 1.44) | 15 | 0.91 | (0.89, 1.90) |
| 8 | 0.81 | (0.79, 0.89) | 16 | 0.67 | (0.38, 0.71) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Shu, Z.; Huang, X.; Peng, K.; Pan, J. Modelling Analysis of COVID-19 Transmission and the State of Emergency in Japan. Int. J. Environ. Res. Public Health 2021, 18, 6858. https://doi.org/10.3390/ijerph18136858
Chen Z, Shu Z, Huang X, Peng K, Pan J. Modelling Analysis of COVID-19 Transmission and the State of Emergency in Japan. International Journal of Environmental Research and Public Health. 2021; 18(13):6858. https://doi.org/10.3390/ijerph18136858
Chicago/Turabian StyleChen, Zhongxiang, Zhiquan Shu, Xiuxiang Huang, Ke Peng, and Jiaji Pan. 2021. "Modelling Analysis of COVID-19 Transmission and the State of Emergency in Japan" International Journal of Environmental Research and Public Health 18, no. 13: 6858. https://doi.org/10.3390/ijerph18136858