
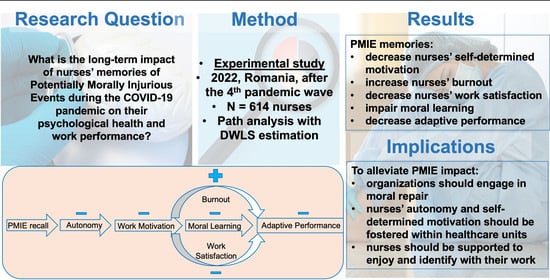
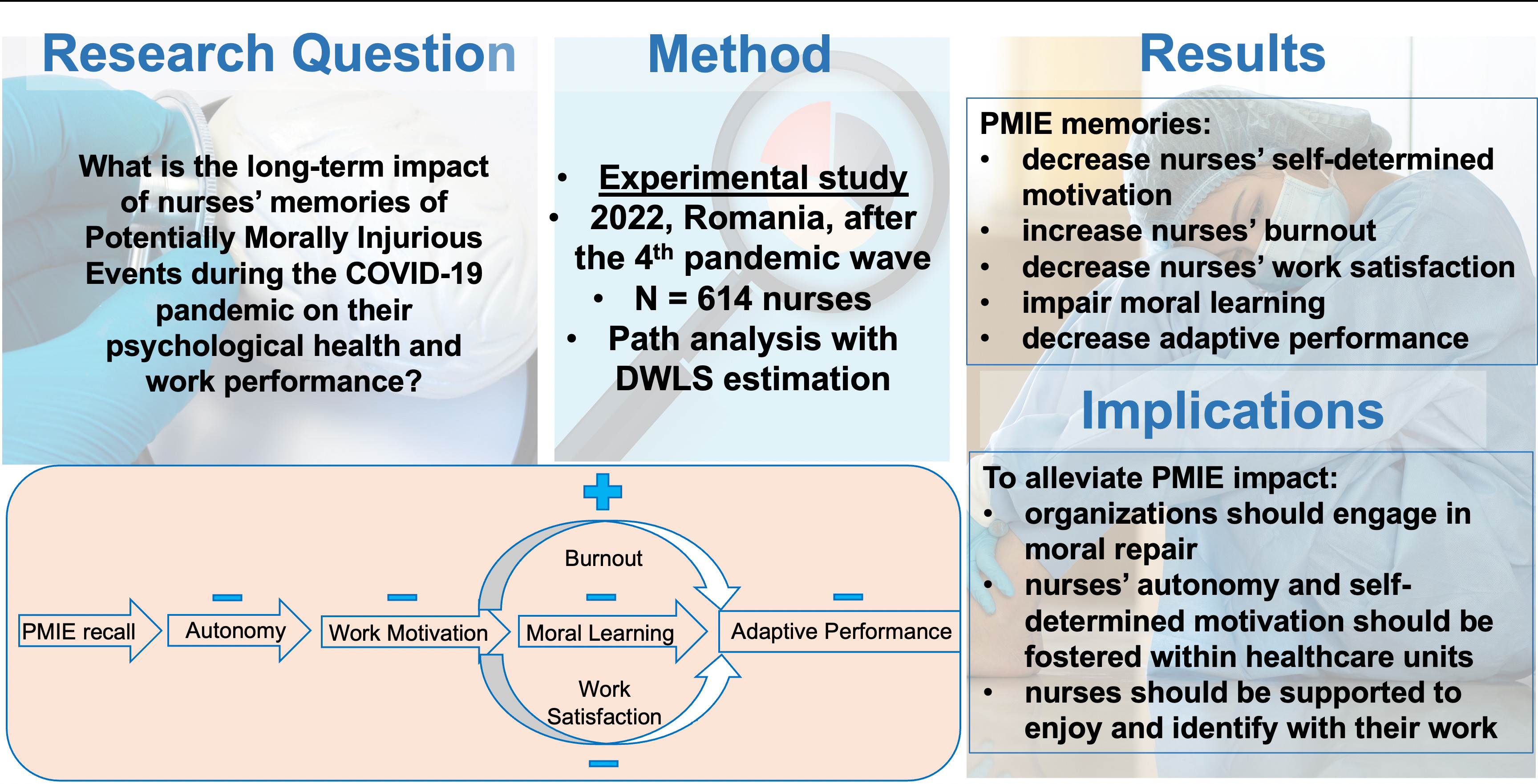
The Moral Impact of the COVID-19 Pandemic on Nurses’ Burnout, Work Satisfaction and Adaptive Work Performance: The Role of Autobiographical Memories of Potentially Morally Injurious Events and Basic Psychological Needs


Abstract
:
1. Introduction
1.1. Potentially Morally Injurious Events in Healthcare during the COVID-19 Pandemic
1.2. Autobiographical Episodic Memories of Moral Transgressions
1.3. Autonomy Thwarting in Work-Related, Autobiographical Episodic Memories
1.4. Work Motivation
1.5. Moral Learning following Moral Memory Recall
1.6. Burnout
1.7. Work Satisfaction
1.8. Adaptive Performance
1.9. Current Study
- Path 1: Burnout as the Main Mechanism
- 2.
- Path 2: Work Satisfaction as the Main Mechanism
- 3.
- Path 3: Moral Learning as the Main Mechanism
2. Materials and Methods
2.1. Sample
2.1.1. Participants Recruiting
2.1.2. Final Sample Description
2.1.3. Ethics
2.2. Procedure and Instruments
2.3. Data Analyses Strategy
3. Results
3.1. Socio-Demographic Differences
3.2. Self-Defining Memories of PMIEs and SMTs
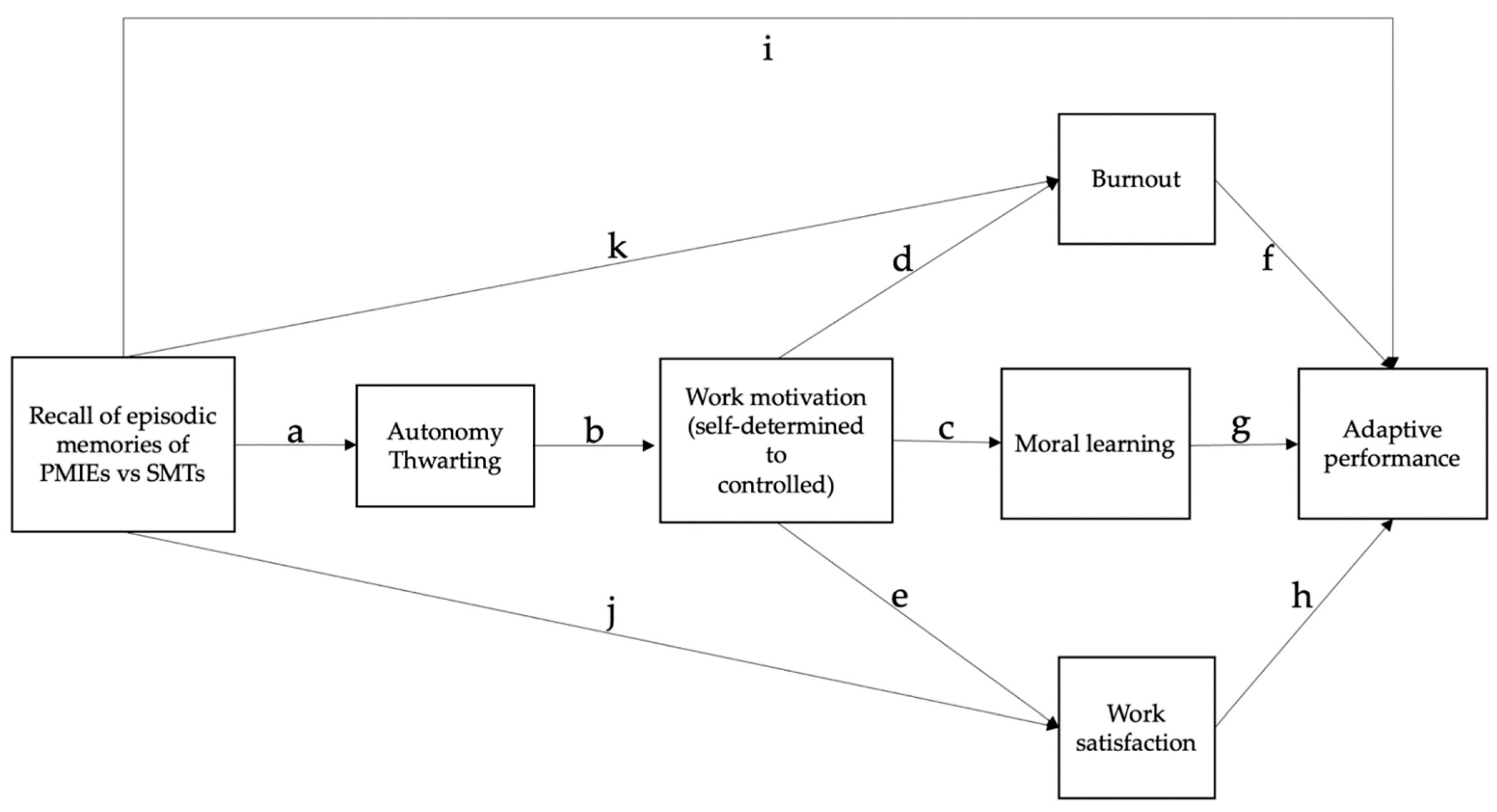
3.3. Path Analysis of the Conceptual Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Experimental Procedure
Appendix B

{kind=link}
{kind=link}
| Predictors | Outcome Variables | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adaptive Performance | Burnout | Work Satisfaction | Moral Learning | Work Motivation | Autonomy Thwarting | |||||||
| VIF | T | VIF | T | VIF | T | VIF | T | VIF | T | VIF | T | |
| Autonomy Thwarting | 1.68 | 0.59 | 1.37 | 0.73 | 1.37 | 0.73 | 1.37 | 0.73 | 1.13 | 0.88 | ||
| Moral Learning | 1.71 | 0.59 | ||||||||||
| Work Motivation | 1.94 | 0.52 | 1.62 | 0.62 | 1.62 | 0.62 | 1.62 | 0.62 | 1.13 | 0.89 | ||
| Work Satisfaction | 1.6 | 0.63 | ||||||||||
| Burnout | 1.67 | 0.6 | ||||||||||
| Experimental Condition a | 1.46 | 0.68 | 1.34 | 0.75 | 1.34 | 0.75 | 1.34 | 0.75 | 1.01 | 0.99 | ||
| Age | 1.03 | 0.97 | 1.01 | 0.99 | 1.01 | 0.99 | 1.01 | 0.99 | ||||
| Gender | 1.02 | 0.98 | 1.01 | 0.99 | 1 | 0.99 | ||||||
Appendix C. Outliers Treatment
| Paths a | Label | B d | SE | 95% CI b | z | p | Β e | H | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| Autonomy ← PMIE vs. SMT recall c | a | 1.65 | 0.2 | 1.27 | 2.03 | 8.44 | <0.001 | 0.34 | H2 |
| Autonomy ←Age | 0.02 | 0.01 | −0.00 | 0.05 | 1.77 | 0.077 | 0.08 | ||
| Work Motivation ← Autonomy | b | −1.37 | 0.13 | −1.63 | −1.11 | −10.39 | <0.001 | −0.36 | H3 |
| Work Motivation ← PMIE vs. SMT recall | −7.32 | 0.67 | −8.62 | −5.98 | −10.86 | <0.001 | −0.39 | ||
| Work Motivation ← Age | −0.02 | 0.04 | −0.09 | 0.05 | −0.57 | 0.571 | −0.02 | ||
| Work Motivation ← Gender | 2.09 | 0.94 | 0.28 | 3.93 | 2.22 | 0.026 | 0.08 | ||
| Moral Learning ← Work Motivation | c | 0.05 | 0.01 | 0.03 | 0.07 | 5.51 | <0.001 | 0.33 | H4 |
| Moral Learning ← Autonomy | −0.21 | 0.03 | −0.26 | −0.15 | −7.3 | <0.001 | −0.36 | ||
| Moral Learning ← PMIE vs. SMT recall | −0.36 | 0.14 | −0.62 | −0.08 | −2.53 | 0.012 | −0.12 | ||
| Moral Learning ← Gender | 0.26 | 0.13 | 0 | 0.51 | 1.94 | 0.052 | 0.06 | ||
| Work Satisfaction ← Work Motivation | e | 0.25 | 0.03 | 0.19 | 0.31 | 8.25 | <0.001 | 0.42 | |
| Work Satisfaction ← Autonomy | −0.57 | 0.09 | −0.75 | −0.38 | −6.05 | <0.001 | −0.25 | ||
| Work Satisfaction ← PMIE vs. SMT recall | j | −1.34 | 0.45 | −2.2 | −0.44 | −2.97 | 0.003 | −0.12 | |
| Work Satisfaction ← Age | −0.05 | 0.02 | −0.09 | −0.01 | −2.38 | 0.017 | −0.07 | ||
| Burnout ← Work Motivation | d | −0.34 | 0.05 | −0.44 | −0.24 | −6.5 | <0.001 | −0.36 | |
| Burnout ← Autonomy | 1.06 | 0.18 | 0.71 | 1.4 | 6.06 | <0.001 | 0.3 | ||
| Burnout ← PMIE vs. SMT recall | k | 2.66 | 0.81 | 1.03 | 4.2 | 3.3 | 0.001 | 0.15 | |
| Adaptive Performance ← Burnout | f | −0.32 | 0.07 | −0.46 | −0.19 | −4.61 | <0.001 | −0.14 | |
| Adaptive Performance ← Moral Learning | g | 3 | 0.41 | 2.21 | 3.81 | 7.42 | <0.001 | 0.22 | |
| Adaptive Performance ← Work Satisfaction | h | 0.63 | 0.11 | 0.41 | 0.85 | 5.5 | <0.001 | 0.18 | |
| Adaptive Performance ← Work Motivation | 0.62 | 0.08 | 0.47 | 0.79 | 7.71 | <0.001 | 0.3 | ||
| Adaptive Performance ← Autonomy | −1.02 | 0.24 | −1.47 | −0.55 | −4.32 | <0.001 | −0.13 | ||
| Adaptive Performance ← PMIE vs. SMT recall | i | −4.27 | 1.01 | −6.2 | −2.23 | −4.22 | <0.001 | −0.11 | |
| Adaptive Performance ← Age | −0.03 | 0.05 | −0.13 | 0.08 | −0.53 | 0.593 | −0.01 | ||
| Adaptive Performance ← Gender | −1.12 | 1.13 | −3.4 | 1.07 | −1 | 0.320 | −0.02 | ||
| Effects | Label | B b | SE | 95% CI c | z | p | Β d | H | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| Indirect Effect PMIE vs. SMT recall a to Adaptive Performance through Burnout | a*b*d*f | −0.24 | 0.07 | −0.41 | −0.12 | −3.31 | 0.001 | −0.01 | H5 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Burnout | i | −4.27 | 1.01 | −6.2 | −2.23 | −4.22 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Burnout | i + a*b*d*f | −4.52 | 1.01 | −6.44 | −2.47 | −4.51 | <0.001 | −0.12 | |
| Indirect Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | a*b*c*g | −0.35 | 0.09 | −0.55 | −0.2 | −3.81 | <0.001 | −0.01 | H7 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | i | −4.27 | 1.01 | −6.2 | −2.23 | −4.22 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | i + a*b*c*g | −4.62 | 1.02 | −6.57 | −2.57 | −4.55 | <0.001 | −0.12 | |
| Indirect Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | a*b*e*h | −0.35 | 0.1 | −0.56 | −0.19 | −3.67 | <0.001 | −0.01 | H6 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | i | −4.27 | 1.01 | −6.2 | −2.23 | −4.22 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | i + a*b*e*h | −4.62 | 1.02 | −6.57 | −2.56 | −4.54 | <0.001 | −0.12 | |
| Indirect Effect PMIE vs. SMT recall to Burnout | a*b*d | 0.76 | 0.17 | 0.46 | 1.14 | 4.43 | <0.001 | 0.04 | H5 |
| Direct Effect PMIE vs. SMT recall to Burnout | k | 2.66 | 0.81 | 1.03 | 4.2 | 3.3 | 0.001 | 0.15 | |
| Total Effect PMIE vs. SMT recall to Burnout | k + a*b*d | 3.62 | 0.76 | 1.89 | 4.88 | 4.52 | <0.001 | 0.2 | |
| Indirect Effect PMIE vs. SMT recall to Work Satisfaction | a*b*e | −0.56 | 0.11 | −0.80 | −0.37 | −5.1 | <0.001 | −0.05 | H6 |
| Direct Effect PMIE vs. SMT recall to Work Satisfaction | j | −1.34 | 0.45 | −2.2 | −0.44 | −2.98 | 0.003 | −0.12 | |
| Total Effect PMIE vs. SMT recall to Work Satisfaction | j + a*b*e | −1.9 | 0.43 | −2.74 | −1.05 | −4.43 | <0.001 | −0.17 | |
References
- Rushton, C.H.; Thomas, T.A.; Antonsdottir, I.M.; Nelson, K.E.; Boyce, D.; Vioral, A.; Swavely, D.; Ley, C.D.; Hanson, G.C. Moral Injury and Moral Resilience in Health Care Workers during COVID-19 Pandemic. J. Palliat. Med. 2021, 25, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Williamson, V.; Murphy, D.; Greenberg, N. COVID-19 and experiences of moral injury in front-line key workers. Occup. Med. 2020, 70, 317–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbaum, L. Facing COVID-19 in Italy: Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line. N. Engl. J. Med. 2020, 382, 1873–1875. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during COVID-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Maftei, A.; Holman, A.C. The prevalence of exposure to potentially morally injurious events among physicians during the COVID-19 pandemic. Eur. J. Psychotraumatol. 2021, 12, 1898791. [Google Scholar] [CrossRef]
- Helion, C.; Helzer, E.G.; Kim, S.; Pizarro, D.A. Asymmetric memory for harming versus being harmed. J. Exp. Psychol. Gen. 2020, 149, 889–900. [Google Scholar] [CrossRef]
- Stanley, M.L.; Cabeza, R.; Smallman, R.; De Brigard, F. Memory and Counterfactual Simulations for Past Wrongdoings Foster Moral Learning and Improvement. Cogn. Sci. 2021, 45, e13007. [Google Scholar] [CrossRef]
- Huang, S.; Stanley, M.L.; De Brigard, F. The phenomenology of remembering our moral transgressions. Mem. Cognit. 2020, 48, 277–286. [Google Scholar] [CrossRef]
- Deci, E.L.; Olafsen, A.H.; Ryan, R.M. Self-determination theory in work organizations: The state of a science. Annu. Rev. Organ. Psychol. Organ. Behav. 2017, 4, 19–43. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; The Guilford Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Philippe, F.L.; Lopes, M.; Houlfort, N.; Fernet, C. Work-related episodic memories can increase or decrease motivation and psychological health at work. Work Stress 2019, 33, 366–384. [Google Scholar] [CrossRef]
- Philippe, F.L.; Bernard-Desrosiers, L. The Odyssey of Episodic Memories: Identifying the Paths and Processes through which they Contribute to Well-Being. J. Pers. 2017, 85, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Singer, J.A. A Cross-Cultural Study of Self-Defining Memories in Chinese and American College Students. Front. Psychol. 2021, 11, 622527. [Google Scholar] [CrossRef] [PubMed]
- Maloney, D.M.; Egan, S.M. The effect of autonomy on counterfactual thinking about controllable events. J. Cogn. Psychol. 2017, 29, 337–351. [Google Scholar] [CrossRef]
- Bashirian, S.; Jenabi, E.; Khazaei, S.; Barati, M.; Karimi-Shahanjarini, A.; Zareian, S.; Rezapur-Shahkolai, F.; Moeini, B. Factors associated with preventive behaviours of COVID-19 among hospital staff in Iran in 2020: An application of the Protection Motivation Theory. J. Hosp. Infect. 2020, 105, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [Green Version]
- Kakemam, E.; Chegini, Z.; Rouhi, A.; Ahmadi, F.; Majidi, S. Burnout and its relationship to self-reported quality of patient care and adverse events during COVID-19: A cross-sectional online survey among nurses. J. Nurs. Manag. 2021, 29, 1974–1982. [Google Scholar] [CrossRef]
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors related to physician burnout and its consequences: A review. Behav Sci. 2018, 8, 98. [Google Scholar] [CrossRef] [Green Version]
- Spector, P.E. Job Satisfaction: Application, Assessment, Causes, and Consequences; Sage Publications: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Lavoie-Tremblay, M.; Gélinas, C.; Aubé, T.; Tchouaket, E.; Tremblay, D.; Gagnon, M.P.; Côté, J. Influence of caring for COVID-19 patients on nurse’s turnover, work satisfaction and quality of care. J. Nurs. Manag. 2022, 30, 33–43. [Google Scholar] [CrossRef]
- Papathanasiou, I.V.; Fradelos, E.C.; Kleisiaris, C.F.; Tsaras, K.; Kalota, M.A.; Kourkouta, L. Motivation, leadership, empowerment and confidence: Their relation with nurses’ burnout. Mater. Socio Med. 2014, 26, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Lamiani, G.; Ciconali, M.; Argentero, P.; Vegni, E. Clinicians’ moral distress and family satisfaction in the intensive care unit. J. Health Psychol. 2020, 25, 1894–1904. [Google Scholar] [CrossRef]
- Williamson, V.; Stevelink, S.; Greenberg, N. Occupational moral injury and mental health: Systematic review and meta-analysis. Br. J. Psychiatry 2018, 212, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamiani, G.; Biscardi, D.; Meyer, E.C.; Giannini, A.; Vegni, E. Moral Distress Trajectories of Physicians 1 Year after the COVID-19 Outbreak: A Grounded Theory Study. Int. J. Environ. Res. Public Health 2021, 18, 13367. [Google Scholar] [CrossRef] [PubMed]
- Mantri, S.; Song, Y.K.; Lawson, J.M.; Berger, J.E.; Koenig, H.G. Moral injury and burnout in health care professionals during the COVID-19 pandemic. J. Nerv. Mental Dis. 2021, 209, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Tenbrunsel, A.E.; Messick, D.M. Ethical fading: The role of self deception in unethical behavior. Soc. Justice Res. 2004, 17, 223–236. [Google Scholar] [CrossRef]
- Mufarichah, A.; Pardiman, P.; Asiyah, S. Analysis of the Adaptability of Nurses during the COVID-19 Pandemic. Bp. Int. Res. Crit. Inst. (BIRCI-J.) Humanit. Soc. Sci. 2021, 4, 5671–5680. [Google Scholar] [CrossRef]
- Niskala, J.; Kanste, O.; Tomietto, M.; Miettunen, J.; Tuomikoski, A.M.; Kyngäs, H.; Mikkonen, K. Interventions to improve nurses’ job satisfaction: A systematic review and meta-analysis. J. Adv. Nurs. 2020, 76, 1498–1508. [Google Scholar] [CrossRef]
- Jundt, D.K.; Shoss, M.K.; Huang, J.L. Individual adaptive performance in organizations: A review. J. Organ. Behav. 2015, 36, S53–S71. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Raiu, V.C.; Azoicai, D.; Popovici, D.E.; Apetrei, C. COVID-19 in Romania: What Went Wrong? Front. Public Health 2021, 9, 813941. [Google Scholar] [CrossRef]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004. [Google Scholar]
- Park, S.; Park, S. Employee adaptive performance and its antecedents: Review and synthesis. Hum. Resour. Dev. Rev. 2019, 18, 294–324. [Google Scholar] [CrossRef]
- Borges, L.M.; Holliday, R.; Barnes, S.M.; Bahraini, N.H.; Kinney, A.; Forster, J.E.; Brenner, L.A. A longitudinal analysis of the role of potentially morally injurious events on COVID-19-related psychosocial functioning among healthcare providers. PLoS ONE 2021, 16, e0260033. [Google Scholar] [CrossRef]
- Tremblay, M.A.; Blanchard, C.M.; Taylor, S.; Pelletier, L.G.; Villeneuve, M. Work Extrinsic and Intrinsic Motivation Scale: Its value for organizational psychology research. Can. J. Behav. Sci. 2009, 41, 213–226. [Google Scholar] [CrossRef]
- Bérubé, N.; Donia, M.; Gagné, M.; Houlfort, N.; Lvina, E. Validation Evidence for the Work Domain Satisfaction Scale in Two Languages. Int. J. Psychol. Stud. 2016, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. MBI: Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Bria, M.; Spânu, F.; Băban, A.; Dumitraşcu, D.L. Maslach burnout inventory–general survey: Factorial validity and invariance among Romanian healthcare professionals. Burn. Res. 2014, 1, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Charbonnier-Voirin, A.; Roussel, P. Adaptive performance: A new scale to measure individual performance in organizations. Can. J. Adm. Sci. 2012, 29, 280–293. [Google Scholar] [CrossRef]
- Li, C.H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Methods 2016, 48, 936–949. [Google Scholar] [CrossRef] [Green Version]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Riedel, P.-L.; Kreh, A.; Kulcar, V.; Lieber, A.; Juen, B. A Scoping Review of Moral Stressors, Moral Distress and Moral Injury in Healthcare Workers during COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 1666. [Google Scholar] [CrossRef]
- Liu, X.; Xu, Y.; Chen, Y.; Chen, C.; Wu, Q.; Xu, H.; Zhu, P.; Waidley, E. Ethical dilemmas faced by frontline support nurses fighting COVID-19. Nurs. Ethics 2022, 29, 7–18. [Google Scholar] [CrossRef]
- Smallwood, N.; Pascoe, A.; Karimi, L.; Willis, K. Moral Distress and Perceived Community Views Are Associated with Mental Health Symptoms in Frontline Health Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 8723. [Google Scholar] [CrossRef]
- Krijgsheld, M.; Tummers, L.G.; Scheepers, F.E. Job performance in healthcare: A systematic review. BMC Health Serv. Res. 2022, 22, 149. [Google Scholar] [CrossRef] [PubMed]
- French, L.; Hanna, P.; Huckle, C. “If I die, they do not care”: U.K. National Health Service staff experiences of betrayal-based moral injury during COVID-19. Psychol. Trauma 2022, 14, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Galletta, M.; Portoghese, I.; Pili, S.; Piazza, M.F.; Campagna, M. The effect of work motivation on a sample of nurses in an Italian healthcare setting. Work 2016, 54, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Falatah, R. The Impact of the Coronavirus Disease (COVID-19) Pandemic on Nurses’ Turnover Intention: An Integrative Review. Nurs. Rep. 2021, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Toode, K.; Routasalo, P.; Helminen, M.; Suominen, T. Hospital nurses’ work motivation. Scand. J. Caring Sci. 2015, 29, 248–257. [Google Scholar] [CrossRef]
- McHan, K.; Johnston-Taylor, E.; Piscopo, B.; Abate, E.; Dehom, S. Nursing values and moral identity in baccalaureate nursing students. J. Prof. Nurs. 2022, 39, 171–176. [Google Scholar] [CrossRef]
- Strohminger, N.; Knobe, J.; Newman, G. The True Self: A Psychological Concept Distinct From the Self. Perspect. Psychol. Sci. 2017, 12, 551–560. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Statistics Romania. Activity of the Healthcare and Prevention Network for the Year 2020 [Activitatea Rețelei Sanitare și de Ocrotire a Sănătății–Anul 2020]; Editura Institutului Național de Statistică: Bucharest, Romania, 2021; ISSN 2784-2223. Available online: https://insse.ro/cms/sites/default/files/field/publicatii/activitatea_retelei_sanitare_in_anul_2020.pdf (accessed on 15 June 2022).
- World Health Organization. State of the World’s Nursing 2020; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-000329-3. Available online: https://apps.who.int/iris/bitstream/handle/10665/331673/9789240003293-eng.pdf (accessed on 15 June 2022).
- Skitka, L.J.; Hanson, B.E.; Morgan, G.S.; Wisneski, D.C. The psychology of moral conviction. Annu. Rev. Psychol. 2021, 72, 347–366. [Google Scholar] [CrossRef]
- Hines, S.E.; Chin, K.H.; Glick, D.R.; Wickwire, E.M. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 488. [Google Scholar] [CrossRef]
- Kreh, A.; Brancaleoni, R.; Magalini, S.C.; Chieffo, D.; Flad, B.; Ellebrecht, N.; Juen, B. Ethical and psychosocial considerations for hospital personnel in the COVID-19 crisis: Moral injury and resilience. PLoS ONE 2021, 16, e0249609. [Google Scholar] [CrossRef]
- Zerach, G.; Levi-Belz, Y. Moral injury and mental health outcomes among Israeli health and social care workers during the COVID-19 pandemic: A latent class analysis approach. Eur. J. Psychotraumatol. 2021, 12, 1945749. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Harold, K.G.; Tong, Y.; Wen, J.; Sui, M.; Liu, H.; Zaben, F.A.; Liu, G. Moral injury in Chinese health professionals during the COVID-19 pandemic. Psychol. Trauma. 2022, 14, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Pulakos, E.D.; Schmitt, N.; Dorsey, D.W.; Arad, S.; Borman, W.C.; Hedge, J.W. Predicting Adaptive Performance: Further Tests of a Model of Adaptability. Hum. Perform. 2002, 15, 299–323. [Google Scholar] [CrossRef]
- Ramos-Villagrasa, P.J.; Fernández-del-Río, E.; Barrada, J.R. Does Evil Prevail? The “Bright” and “Dark” Sides of Personality as Predictors of Adaptive Performance. Sustainability 2020, 12, 474. [Google Scholar] [CrossRef] [Green Version]
- Gray, K.; Waytz, A.; Young, L. The moral dyad: A fundamental template unifying moral judgment. Psychol. Inq. 2012, 2, 206–215. [Google Scholar] [CrossRef]
- Brüggemann, A.J.; Wijma, B.; Swahnberg, K. Abuse in health care: A concept analysis. Scand. J. Caring Sci. 2012, 26, 123–132. [Google Scholar] [CrossRef] [Green Version]
- Cook, R.D.; Weisberg, S. Residuals and Influence in Regression; Chapman and Hall: New York, NY, USA, 1982. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: Boston, MA, USA, 2013. [Google Scholar]

| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |||
|---|---|---|---|---|---|---|---|---|---|
| 1. | Autonomy thwarting | Pearson’s r | — | ||||||
| p-value | — | ||||||||
| 95% CI UL | — | ||||||||
| 95% CI LL | — | ||||||||
| 2. | Moral learning | Pearson’s r | −0.53 *** | — | |||||
| p-value | < 0.001 | — | |||||||
| 95% CI UL | −0.47 | — | |||||||
| 95% CI LL | −0.58 | — | |||||||
| 3. | Work motivation | Pearson’s r | −0.51 *** | 0.52 *** | — | ||||
| p-value | < 0.001 | <0.001 | — | ||||||
| 95% CI UL | −0.45 | 0.58 | — | ||||||
| 95% CI LL | −0.57 | 0.46 | — | ||||||
| 4. | Work satisfaction | Pearson’s r | −0.46 *** | 0.46 *** | 0.52 *** | — | |||
| p-value | < 0.001 | <0.001 | <0.001 | — | |||||
| 95% CI UL | −0.4 | 0.52 | 0.58 | — | |||||
| 95% CI LL | −0.52 | 0.4 | 0.46 | — | |||||
| 5. | Burnout | Pearson’s r | 0.49 *** | −0.48 *** | −0.53 *** | −0.42 *** | — | ||
| p-value | < 0.001 | <0.001 | <0.001 | <0.001 | — | ||||
| 95% CI UL | 0.55 | −0.42 | −0.48 | −0.35 | — | ||||
| 95% CI LL | 0.43 | −0.54 | −0.59 | −0.48 | — | ||||
| 6. | Adaptive performance | Pearson’s r | −0.59 *** | 0.64 *** | 0.69 *** | 0.6 *** | −0.59 *** | — | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | — | |||
| 95% CI UL | −0.54 | 0.68 | 0.73 | 0.65 | −0.53 | — | |||
| 95% CI LL | −0.64 | 0.59 | 0.65 | 0.55 | −0.64 | — | |||
| 7. | Work experience | Pearson’s r | 0.06 | −0.02 | −0.03 | −0.11 ** | 0.01 | −0.06 | — |
| p-value | 0.149 | 0.679 | 0.48 | 0.006 | 0.732 | 0.155 | — | ||
| 95% CI UL | 0.14 | 0.06 | 0.05 | −0.03 | 0.09 | 0.02 | — | ||
| 95% CI LL | −0.02 | −0.1 | −0.11 | −0.19 | −0.07 | −0.14 | — | ||
| 8. | Age | Pearson’s r | 0.1 * | −0.05 | −0.08 * | −0.15 *** | 0.02 | −0.1 * | 0.83 *** |
| p-value | 0.013 | 0.245 | 0.04 | <0.001 | 0.56 | 0.012 | <0.001 | ||
| 95% CI UL | 0.18 | 0.03 | 0 | −0.07 | 0.1 | −0.02 | 0.85 | ||
| 95% CI LL | 0.02 | −0.13 | −0.16 | −0.22 | −0.06 | −0.18 | 0.8 |
| Variable | Group | Mean | SD | Welch’s t | df | p | Mean Difference | SE Difference | 95% CI | Cohen’s d | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||||
| Autonomy thwarting | M | 2.73 | 2.6 | 1.36 | 118 | 0.176 | 0.4 | 0.3 | −0.18 | 0.99 | 0.16 |
| F | 2.33 | 2.46 | |||||||||
| Moral learning | M | 2.71 | 1.37 | −3.4 | 126 | <0.001 | −0.54 | 0.16 | −0.85 | −0.22 | −0.38 |
| F | 3.25 | 1.45 | |||||||||
| Work motivation | M | −5.73 | 8.53 | −2.49 | 132 | 0.014 | −2.48 | 0.99 | −4.44 | −0.51 | −0.27 |
| F | −3.25 | 9.7 | |||||||||
| Work satisfaction | M | 17.78 | 5.28 | −1.96 | 126 | 0.052 | −1.19 | 0.61 | −2.4 | 0.01 | −0.22 |
| F | 18.97 | 5.63 | |||||||||
| Burnout | M | 35.91 | 8.04 | 1.96 | 129 | 0.053 | 1.82 | 0.93 | −0.02 | 3.67 | 0.22 |
| F | 34.09 | 8.86 | |||||||||
| Adaptive performance | M | 67.67 | 17.78 | −2.2 | 133 | 0.029 | −4.58 | 2.08 | −8.69 | −0.47 | −0.24 |
| F | 72.25 | 20.57 | |||||||||
| Variable | Group c | Mean | SD | Welch’s F | df1 | df2 | p | Games-Howell Post-Hoc Tests | p | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | t | df | |||||||||
| Autonomy thwarting | Post-Secondary | 2.39 | 2.5 | 0.08 | 2 | 37.5 | 0.922 | ||||
| Bachelor’s | 2.32 | 2.33 | |||||||||
| Masters’ | 2.57 | 2.25 | |||||||||
| Moral learning | Post-Secondary | 3.15 | 1.43 | 0.63 | 2 | 36.3 | 0.54 | ||||
| Bachelor’s | 3.45 | 1.59 | |||||||||
| Masters’ | 3.3 | 1.61 | |||||||||
| Work motivation | Post-Secondary | −3.8 a | 9.69 | 3.88 | 2 | 38.5 | 0.029 | M a − M b = −3.79 | −2.79 | 36 | 0.022 |
| Bachelor’s | −0.01 b | 7.2 | |||||||||
| Masters’ | −3.98 | 8.73 | |||||||||
| Work satisfaction | Post-Secondary | 18.78 | 5.62 | 0.77 | 2 | 37.4 | 0.472 | ||||
| Bachelor’s | 19.68 | 5.59 | |||||||||
| Masters’ | 17.87 | 5.01 | |||||||||
| Burnout | Post-Secondary | 34.38 | 8.85 | 0.09 | 2 | 37.9 | 0.914 | ||||
| Bachelor’s | 34.29 | 8.67 | |||||||||
| Masters’ | 33.74 | 6.99 | |||||||||
| Adaptive performance | Post-Secondary | 71.53 | 20.33 | 0.66 | 2 | 37.2 | 0.524 | ||||
| Bachelor’s | 74.65 | 18.02 | |||||||||
| Masters’ | 68.65 | 21.12 | |||||||||
| M | SD | Skew | Kurtosis | VIF | Tolerance | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Adaptive performance | 71.6 | 20.2 | 0.09 | −0.36 | — | — | — | |||||
| 2. Autonomy thwarting | 2.39 | 2.48 | −0.11 | −0.86 | 1.68 | 0.60 | −0.59 *** | — | ||||
| 3. Moral learning | 3.17 | 1.45 | 0.25 | −0.64 | 1.69 | 0.59 | 0.64 *** | −0.52 *** | — | |||
| 4. Work motivation | −3.61 | 9.57 | −0.11 | −0.63 | 1.94 | 0.52 | 0.69 *** | −0.51 *** | 0.52 *** | — | ||
| 5. Work satisfaction | 18.8 | 5.59 | −0.15 | −0.62 | 1.58 | 0.63 | 0.60 *** | −0.46 *** | 0.46 *** | 0.52 *** | — | |
| 6. Burnout | 34.4 | 8.77 | 0.21 | −0.67 | 1.66 | 0.60 | −0.59 *** | 0.49 *** | −0.48 *** | −0.53 *** | −0.42 *** | — |
| 7. Experimental condition a | — | — | — | — | 1.46 | 0.69 | −0.52 *** | 0.33 *** | −0.40 *** | −0.50 *** | −0.41 *** | 0.44 *** |
| Paths a | Label | B d | SE | 95% CI b | z | p | Β e | H | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| Autonomy ← PMIE vs. SMT recall c | a | 1.58 | 0.2 | 1.19 | 1.96 | 8.08 | <0.001 | 0.32 | H2 |
| Autonomy ← Age | 0.02 | 0.01 | 0 | 0.04 | 1.6 | 0.109 | 0.07 | ||
| Work Motivation ← Autonomy | b | −1.44 | 0.14 | −1.71 | −1.18 | −10.68 | <0.001 | −0.38 | H3 |
| Work Motivation ← PMIE vs. SMT recall | −6.88 | 0.69 | −8.23 | −5.51 | −10.02 | <0.001 | −0.36 | ||
| Work Motivation ← Age | −0.01 | 0.04 | −0.08 | 0.06 | −0.33 | 0.744 | −0.01 | ||
| Work Motivation ← Gender | 1.87 | 0.92 | 0.04 | 3.71 | 2.03 | 0.043 | 0.07 | ||
| Moral Learning ← Work Motivation | c | 0.05 | 0.01 | 0.03 | 0.07 | 5.36 | <0.001 | 0.31 | H4 |
| Moral Learning ← Autonomy | −0.21 | 0.03 | −0.26 | −0.15 | −7.42 | <0.001 | −0.36 | ||
| Moral Learning ← PMIE vs. SMT recall | −0.41 | 0.14 | −0.68 | −0.13 | −2.98 | 0.003 | −0.14 | ||
| Moral Learning ← Gender | 0.33 | 0.13 | 0.06 | 0.58 | 2.49 | 0.013 | 0.08 | ||
| Work Satisfaction ← Work Motivation | e | 0.2 | 0.03 | 0.14 | 0.27 | 6.53 | <0.001 | 0.35 | |
| Work Satisfaction ← Autonomy | −0.57 | 0.1 | −0.77 | −0.38 | −5.79 | <0.001 | −0.25 | ||
| Work Satisfaction ← PMIE vs. SMT recall | j | −1.83 | 0.48 | −2.77 | −0.89 | −3.8 | <0.001 | −0.16 | |
| Work Satisfaction ← Age | −0.06 | 0.02 | −0.1 | −0.02 | −2.9 | 0.004 | −0.09 | ||
| Burnout ← Work Motivation | d | −0.3 | 0.05 | −0.4 | −0.21 | −6.17 | <0.001 | −0.33 | |
| Burnout ← Autonomy | 1.03 | 0.17 | 0.69 | 1.36 | 6.08 | <0.001 | 0.29 | ||
| Burnout ← PMIE vs. SMT recall | k | 3.35 | 0.77 | 1.79 | 4.81 | 4.33 | <0.001 | 0.19 | |
| Adaptive Performance ← Burnout | f | −0.33 | 0.08 | −0.49 | −0.18 | −4.2 | <0.001 | −0.14 | |
| Adaptive Performance ← Moral Learning | g | 3.19 | 0.52 | 2.2 | 4.23 | 6.13 | <0.001 | 0.23 | |
| Adaptive Performance ← Work Satisfaction | h | 0.7 | 0.15 | 0.41 | 0.99 | 4.69 | <0.001 | 0.19 | |
| Adaptive Performance ← Work Motivation | 0.56 | 0.1 | 0.36 | 0.77 | 5.42 | <0.001 | 0.26 | ||
| Adaptive Performance ← Autonomy | −1.14 | 0.31 | −1.73 | −0.52 | −3.68 | <0.001 | −0.14 | ||
| Adaptive Performance ← PMIE vs. SMT recall | i | −4.3 | 1.12 | −6.43 | −2.03 | −3.83 | <0.001 | −0.11 | |
| Adaptive Performance ← Age | −0.03 | 0.06 | −0.15 | 0.08 | −0.6 | 0.546 | −0.02 | ||
| Adaptive Performance ← Gender | −0.41 | 1.32 | −3.04 | 2.15 | −0.31 | 0.757 | −0.01 | ||
| Effects | Label | B b | SE | 95% CI c | z | p | β d | H | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| Indirect Effect PMIE vs. SMT recall a to Adaptive Performance through Burnout | a*b*d*f | −0.23 | 0.07 | −0.4 | −0.11 | −3.05 | 0.002 | −0.01 | H5 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Burnout | i | −4.3 | 1.12 | −6.43 | −2.03 | −3.83 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Burnout | i + a*b*d*f | −4.53 | 1.12 | −6.67 | −2.24 | −4.03 | <0.001 | −0.11 | |
| Indirect Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | a*b*c*g | −0.34 | 0.1 | −0.55 | −0.18 | −3.54 | <0.001 | −0.01 | H7 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | i | −4.3 | 1.12 | −6.43 | −2.03 | −3.83 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Moral Learning | i + a*b*c*g | −4.64 | 1.13 | −6.77 | −2.37 | −4.11 | <0.001 | −0.12 | |
| Indirect Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | a*b*e*h | −0.32 | 0.09 | −0.53 | −0.17 | −3.46 | 0.001 | −0.01 | H6 |
| Direct Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | i | −4.3 | 1.12 | −6.43 | −2.03 | −3.83 | <0.001 | −0.11 | |
| Total Effect PMIE vs. SMT recall to Adaptive Performance through Work Satisfaction | i + a*b*e*h | −4.62 | 1.13 | −6.75 | −2.36 | −4.1 | <0.001 | −0.11 | |
| Indirect Effect PMIE vs. SMT recall to Burnout | a*b*d | 0.69 | 0.16 | 0.41 | 1.04 | 4.3 | <0.001 | 0.04 | H5 |
| Direct Effect PMIE vs. SMT recall to Burnout | k | 3.35 | 0.77 | 1.79 | 4.81 | 4.34 | <0.001 | 0.19 | |
| Total Effect PMIE vs. SMT recall to Burnout | k + a*b*d | 4.04 | 0.73 | 2.55 | 5.42 | 5.53 | <0.001 | 0.23 | |
| Indirect Effect PMIE vs. SMT recall to Work Satisfaction | a*b*e | −0.46 | 0.1 | −0.68 | −0.29 | −4.59 | <0.001 | −0.04 | H6 |
| Direct Effect PMIE vs. SMT recall to Work Satisfaction | j | −1.83 | 0.48 | −2.77 | −0.89 | −3.81 | <0.001 | −0.16 | |
| Total Effect PMIE vs. SMT recall to Work Satisfaction | j + a*b*e | −2.3 | 0.46 | −3.2 | −1.4 | −5.03 | <0.001 | −0.21 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherman, M.A.; Arhiri, L.; Holman, A.C.; Soponaru, C. The Moral Impact of the COVID-19 Pandemic on Nurses’ Burnout, Work Satisfaction and Adaptive Work Performance: The Role of Autobiographical Memories of Potentially Morally Injurious Events and Basic Psychological Needs. Int. J. Environ. Res. Public Health 2022, 19, 7645. https://doi.org/10.3390/ijerph19137645
Gherman MA, Arhiri L, Holman AC, Soponaru C. The Moral Impact of the COVID-19 Pandemic on Nurses’ Burnout, Work Satisfaction and Adaptive Work Performance: The Role of Autobiographical Memories of Potentially Morally Injurious Events and Basic Psychological Needs. International Journal of Environmental Research and Public Health. 2022; 19(13):7645. https://doi.org/10.3390/ijerph19137645
Chicago/Turabian StyleGherman, Mihaela Alexandra, Laura Arhiri, Andrei Corneliu Holman, and Camelia Soponaru. 2022. "The Moral Impact of the COVID-19 Pandemic on Nurses’ Burnout, Work Satisfaction and Adaptive Work Performance: The Role of Autobiographical Memories of Potentially Morally Injurious Events and Basic Psychological Needs" International Journal of Environmental Research and Public Health 19, no. 13: 7645. https://doi.org/10.3390/ijerph19137645