
Factors Affecting Young Adults’ Decision Making to Undergo COVID-19 Vaccination: A Patient Preference Study


1
Department of Biomedical Technology, Czech Technical University in Prague, 272 01 Kladno, Czech Republic
2
Center for Health Research, Kaiser Permanente Northwest, Portland, OR 97227, USA
*
Author to whom correspondence should be addressed.
Vaccines 2022, 10(2), 265; https://doi.org/10.3390/vaccines10020265
Submission received: 1 December 2021
/
Revised: 14 January 2022
/
Accepted: 8 February 2022
/
Published: 9 February 2022
(This article belongs to the Special Issue COVID-19 Vaccination: Considerations for Public Health and Policy)
Abstract
:Young adults are a substantial driver of lagging vaccination against COVID-19 worldwide. We aimed to understand what vaccine or vaccination environment attributes may affect young adults’ vaccine inclination. We contacted a convenience sample of 1415 students to recruit a minimum of 150 individuals for a web-based discrete choice experiment. The respondents were asked to choose one of two hypothetical vaccines, defined by six attributes—vaccine efficacy, risk of mild side effects, protection duration, administration route, recommender, and travel time to the vaccination site. Individual preferences were calculated with the Markov chain Monte Carlo hierarchical Bayes estimation. A total of 445 individuals (mean age 24.4 years, 272 (61.1%) women) completed the survey between 22 March and 3 May 2021. Vaccine protection duration (28.3 (95% CI, 27.0–29.6)) and vaccine efficacy in preventing COVID-19 (27.5 (95% CI, 26.3–28.8)) were the most important, followed by the risk of vaccine side effects (17.3 (95% CI, 16.2–18.4)). Individuals reluctant or unsure about vaccination (21.1%) prioritized the potential for mild side effects higher and vaccine efficacy lower than the vaccine-inclined individuals. New vaccination programs that target young adults should emphasize the protection duration, low risk of vaccine side effects, and high efficacy.
1. Introduction
Coronavirus disease 2019 (COVID-19) is associated with all-cause and COVID-19-related mortality, morbidity, and increased healthcare utilization [1,2]. Although older adults are at a higher risk for these outcomes compared with younger adults [3], young persons, particularly those with multimorbidity, are also experiencing negative effects of the current pandemic [4,5,6,7,8,9]. In addition, young adults, who returned to in-person schooling after lifting the stay-at-home policy, are likely to contribute to the spread of the virus in older adults [7,10,11].
While many individuals from high-developed countries have already been vaccinated against COVID-19, unvaccinated persons, particularly young adults, are reluctant to take up the vaccine [12,13]. Because there is no mandatory vaccination for COVID-19 for the general population, the ability to control the COVID-19 pandemic relies heavily on the success of vaccination programs [14]. The success of rapid immunization, among other factors (e.g., vaccine availability, access, infrastructure), relies on individuals’ vaccine acceptance [15]. However, high worldwide vaccine hesitancy [16,17] is forecasted to be one of the main impediments to COVID-19 vaccine uptake [18] and perhaps subsequent re-vaccination. Governments, policymakers, and health systems are facing the task of developing effective vaccine-acceptance messaging to engage individuals in vaccination [19,20], so the population can gain herd immunity [15,21]. Research on how to promote vaccination for COVID-19 is still underdeveloped [15], particularly among young adults.
Relatively high COVID-19 vaccine hesitancy [22] is observed in the general population across various countries (e.g., the US [12,23,24,25], France [18,26], and the UK and Ireland [27,28]) and specific populations (e.g., Black and Hispanic individuals, persons with no college degree, younger age, women, low income, and persons with a history of avoiding the influenza vaccine) [12,16,29,30]. A systematic review [31] of COVID-19 vaccine receptivity studies from 31 countries has shown that vaccine acceptability declined from >70% to <50% between March and October 2020 in older and younger adults. A study of vaccine hesitancy and acceptance among American medical students toward a COVID-19 vaccine found that nearly a quarter of surveyed students are reluctant to undergo vaccination immediately upon the US Food and Drug Administration’s approval [25]. A Polish survey of 1284 students found that 40.6% (521) are unwilling to be vaccinated or undecided [32]. Similar results have been shown among Italian [26], Spanish [33], German [34], and Turkish [35] students. Among the main drivers for vaccine hesitancy in students are often-cited concerns regarding adverse reactions, mistrust in the vaccine information presented by public health authorities [25,32], and overall insufficient information about the vaccine [25].
Quantitative patient preference research has been used in Europe to inform marketing authorization, reimbursement, and pricing decisions [36]. Previous vaccine preference studies were either conducted when no authorized vaccines were available [30,37] or have not focused on preferences playing an essential role in young adults [38,39]. The purpose of this study was to understand what vaccine attributes might affect young adults’ decision to undergo vaccination and explore how this information can support governments, policymakers, and health systems in developing initiatives to improve vaccination against COVID-19. We also explored factors that might serve as predictors of individuals being reluctant to undergo vaccination against COVID-19.
2. Materials and Methods
The protocol of this study was reviewed and approved by the Institutional Review Board (IRB ID: B1/2021) at the Faculty of Biomedical Engineering at Czech Technical University in Prague (Prague, Czech Republic).
2.1. Study Design
The experiment was a cross-sectional, self-administered, web-based survey conducted with a convenience sample of students aged ≥18 years from a large university in the Czech Republic between 22 March 2021 and 3 May 2021. We used Conjont.ly software (Analytics Simplified, Sydney, Australia) to elicit participants’ preferences regarding vaccination against COVID-19. We followed the International Society for Pharmacoeconomics and Outcomes Research Good Research Practices for Conjoint Analysis Task Force’s guidance [40] to develop a discrete choice experiment (DCE). We used multivariable logistic regression to identify factors that might predict young adults’ reluctance to undergo vaccination.
2.2. Discrete Choice Experiment Design
2.2.1. Attributes and Levels
We reviewed peer-reviewed literature of previously conducted DCEs for any vaccines or earlier COVID-19 patient-preference vaccine studies to identify candidate attributes. The core set of attributes was retrieved from the two early DCE studies—conducted in the US and China—that analyzed factors associated with adults’ willingness to undergo vaccination against COVID-19 [30,41]. These studies were based on information about hypothetical vaccines. To develop levels for each attribute, we reviewed results of the first vaccine trials that had been published at the time of research design [42,43,44], websites of COVID-19 vaccine manufacturers (i.e., AstraZeneca PLC, Cambridge, UK, Moderna Inc., Cambridge, MA, USA, Pfizer Inc., New York, NY, USA) and their press releases [45,46,47], fact sheets published by the US Food and Drug Administration [48,49,50], and the World Health Organization report on vaccine development [51]. Overall, six attributes and their levels were included in the DCE (Table 1).
The “Vaccine efficacy in preventing COVID-19” attribute indicates the reduction in disease incidence in a vaccinated group compared with an unvaccinated group. The vaccine’s potential harms were grouped in the “Risk of mild side effects” attribute, which refers to the probability of short-term flu-like symptoms, for example, fatigue, headache, chills, and nausea after the vaccination. The “Protection duration” attribute reflects the time between vaccination and anticipated re-vaccination—when the vaccine provides protection against COVID-19. The “Vaccine administration route” attribute reflects the path by which a vaccine can be administered to a patient, either oral or in injections. The “Recommender of the vaccine” attribute reflects who recommended a vaccine to a respondent (i.e., family members or friends, practitioner or experts, or professional societies). The last attribute, “Time to the vaccination site,” presented an expected patient travel time to a vaccination site.
2.2.2. Survey Development
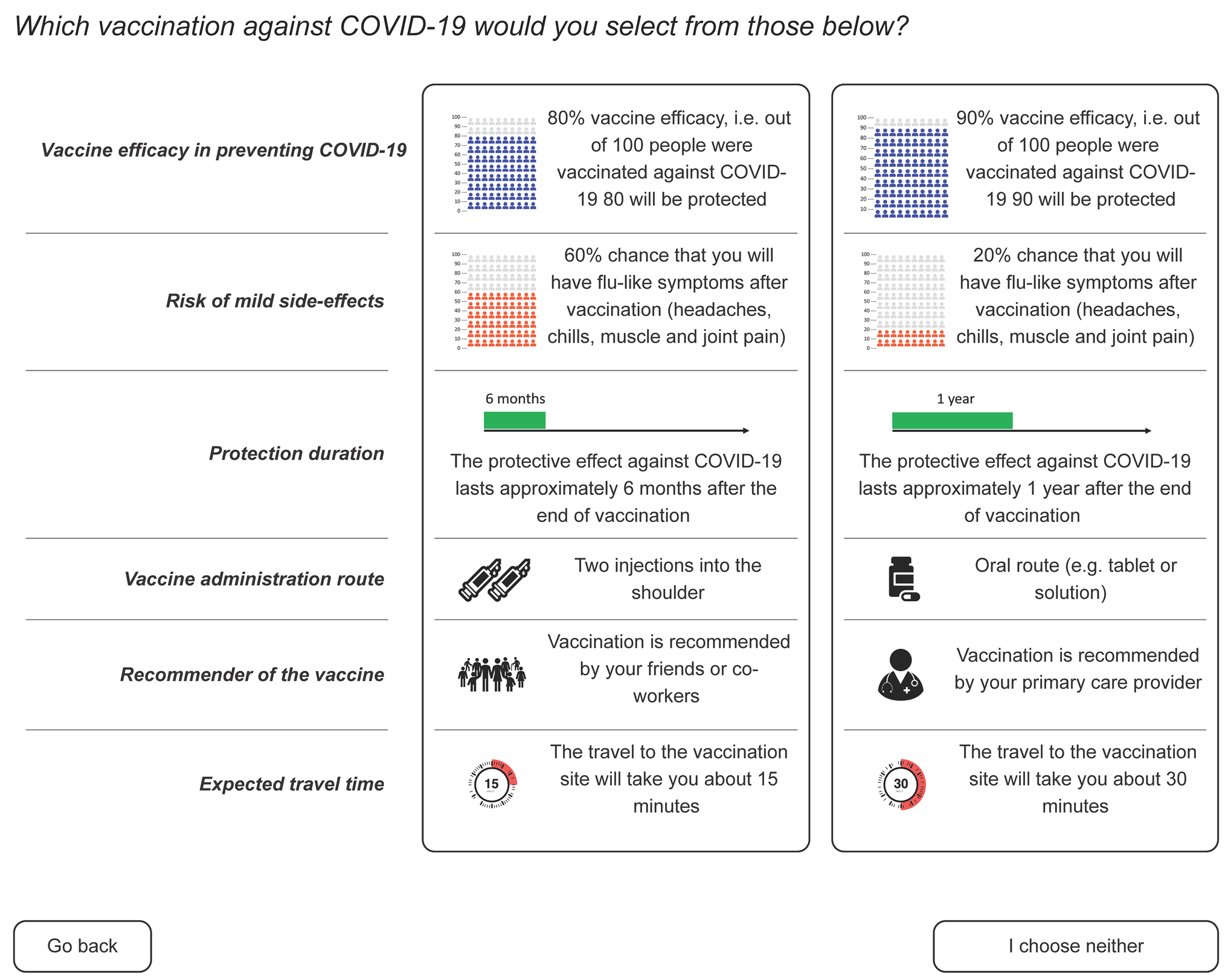
We used the International Patient Decision Aid Standards (IPDAS) Collaboration’s guidance [52,53] on presenting numerical data to patients and ensuring an appropriate literacy level to develop a visualization of DCE choices. We consulted additional resources on the best approaches to present risk estimates to patients [54]. Levels for each attribute were presented as text or pictograms accompanied by an explanation (Figure 1). The draft survey was piloted with five volunteers. As a result of this pilot testing, we updated instructions, reordered visual elements on a webpage, and redesigned some graphics.
2.3. Setting, Participants, and Recruitment
The sample size for DCE studies generally ranges between 100 and 1000 participants [55,56]. We identified a minimum sample size of 150 respondents based on a number of attributes and their levels [57].
Potential participants were 1415 students enrolled in bachelor’s and master’s programs during the 2020–2021 academic year at the Faculty of Biomedical Engineering at the Czech Technical University in Prague. All students were invited via university email on 22 March 2021. The invitation email contained a description of the research, the expected time to complete a survey, information about anonymization and confidentiality, and a link to the DCE questionnaire. A reminder was sent three weeks after the initial invitation. Overall, participants had six weeks to complete the experiment.
Participants were required to indicate that they were at least 18 years old and provide informed consent to enter the study. We had no other eligibility criteria. Participation was voluntary, and no incentives were offered.
2.4. Experimental Design and Variables
Before participants could start the DCE, they were presented with instructions on how to complete the experiment. They were also presented with an example of a DCE question design. In the experiment, individuals were asked, “Which vaccination against COVID-19 would you select from those below?” In each choice task, respondents were asked to compare two hypothetical vaccine/vaccination scenarios (A and B) and choose their preferred one or select an “I choose nothing” option. We used Conjoint.ly to create hypothetical vaccination profiles. This algorithm tends to produce D-efficient designs rather than maximize D-efficiency [57]. The order of questions and alternatives, and the placement of respondents into choice blocks, were randomized to avoid order bias. There were 56 blocks, and each survey respondent completed one of them.
Participants who completed the DCE were also asked to provide their age, gender, ethnicity, current or anticipated pregnancy, level of education, work experience in healthcare, employment status, household income and the size of their household, the count of risk factors for severe COVID-19 (e.g., chronic kidney disease, obesity, human immunodeficiency virus) [58], previous rejection of any recommended vaccination, current COVID-19 vaccination status, prior SARS-CoV-2 infection, and experience with any vaccine’s adverse events. We used a five-point Likert scale (Strongly agree, Agree, Unsure, Disagree, and Strongly disagree) to identify participants’ willingness to undergo vaccination for COVID-19 among those who did not undergo vaccination. All questions were optional and always included the option “Prefer not to say”.
2.5. Analysis
2.5.1. Discrete Choice Experiment
We processed the DCE choices of the respondents within the Conjoint.ly software that utilizes a Markov chain Monte Carlo hierarchical Bayes estimation to calculate individual-level preference coefficients. As the result of this analysis, relative importance scores and their 95% confidence intervals (CIs) were estimated for selected attributes, which measure how much each characteristic affects a participant’s decision to undergo vaccination. The relative importance scores were calculated as the average of each respondent attribute utility. We used McFadden’s pseudo R2 to assess how well our survey results describe the respondents’ answers [59]. We calculated level preference scores to understand which specific vaccination parameters were strongly preferred by the respondents.
We used participants’ self-reported sociodemographic data and stated willingness to undergo vaccination against COVID-19 to estimate attribute importance scores among subgroups. Our subgroup analyses were post hoc based on the number of respondents with a given characteristic. The subgroups were: age, gender, willingness to undergo vaccination, persons with at least one self-reported risk factor for severe COVID-19, and individuals with any experience with COVID-19 since the beginning of the pandemic (e.g., a personal history of COVID-19, a family member diagnosed with COVID-19).
2.5.2. Predictors of Vaccine Hesitancy
We explored factors that might predict participants’ reluctance to undergo vaccination against COVID-19. Participants who indicated that they strongly disagreed, disagreed, or were unsure about undergoing vaccination against COVID-19 when a vaccine is available were grouped as “reluctant to be vaccinated”.
We performed a multivariable logistic regression in R (v.4.0.5) software to test the potential predictors. We used age, education, presence of risk factors for severe COVID-19, ethnicity, previous COVID-19 infection, rejection of vaccination in the past, previous vaccine adverse events, and socioeconomic index as independent variables in the regression analysis. The socioeconomic index was a ratio of reported household income (numerator) and household size (denominator). The referent and comparison groups can be found in the results section. We used the chi-square test to understand whether the variables (participants’ characteristics) were distributed differently between respondents and non-respondents. We used complete case analysis because missing data of covariate did not depend on the outcome (Supplementary Table S1) and the small size of our sample [60,61].
3. Results
3.1. Study Population
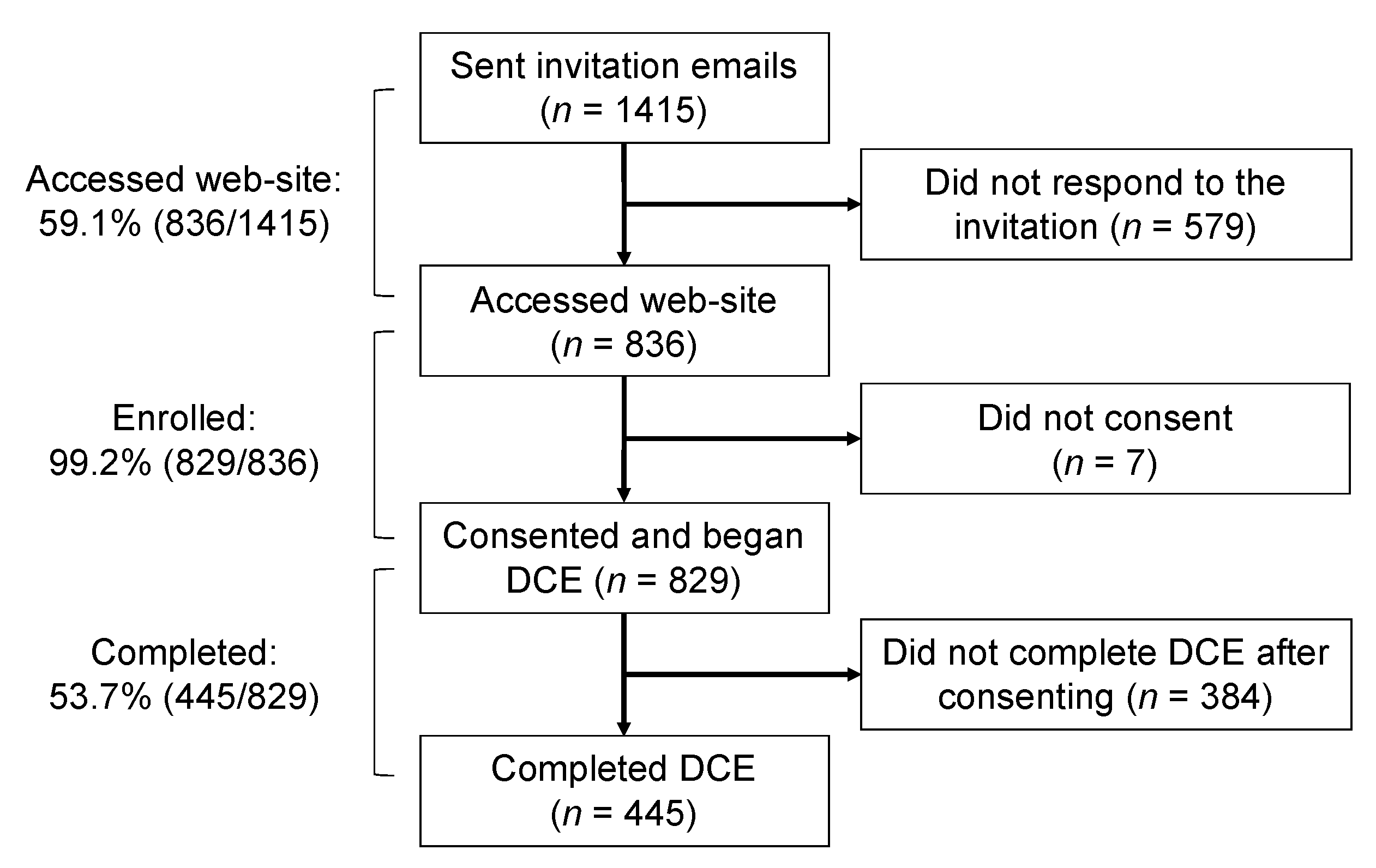
A total of 1415 individuals were invited to participate in the study. Of these, 836 (59.1%) opened the survey link, and 829 (99.2% of those who accessed the website) enrolled (i.e., completed the consent form) (Figure 2). Fifty-four percent (445/829) of those who were enrolled completed the DCE. Of the 445 who completed the DCE, 272 (61.1%) were women, with an estimated weighted mean age of 24.4 years; 360 (80.6%) were Czech, with or without multiple ethnic backgrounds; and 264 (59.3%) had a biomedical background. A total of 77 (17.3%) individuals reported one or more risk factors for severe COVID-19, 22 (4.9%) had rejected a recommended vaccination in the past, 79 (17.6%) reported one or more adverse events with previous vaccinations, and 96 (16.4%) reported a personal history of COVID-19 infection. Only one-fifth (86, 19.3%) of participants reported being fully or partially vaccinated against COVID-19 (Table 2). The study population was representative of the general Czech young adults and university student population with respect to age, gender, and education background (see Supplementary Table S2).
Among the respondents who had not received nor started vaccination, more than two-thirds (233, 70.4%) agreed with the statement, “I want to be vaccinated against COVID-19 as soon as the vaccine is available for me.” At the same time, more than a quarter of participants (94, 28.4%) strongly disagreed, disagreed, or were unsure about getting the vaccine (Table 2).
3.2. Discrete Choice Experiment
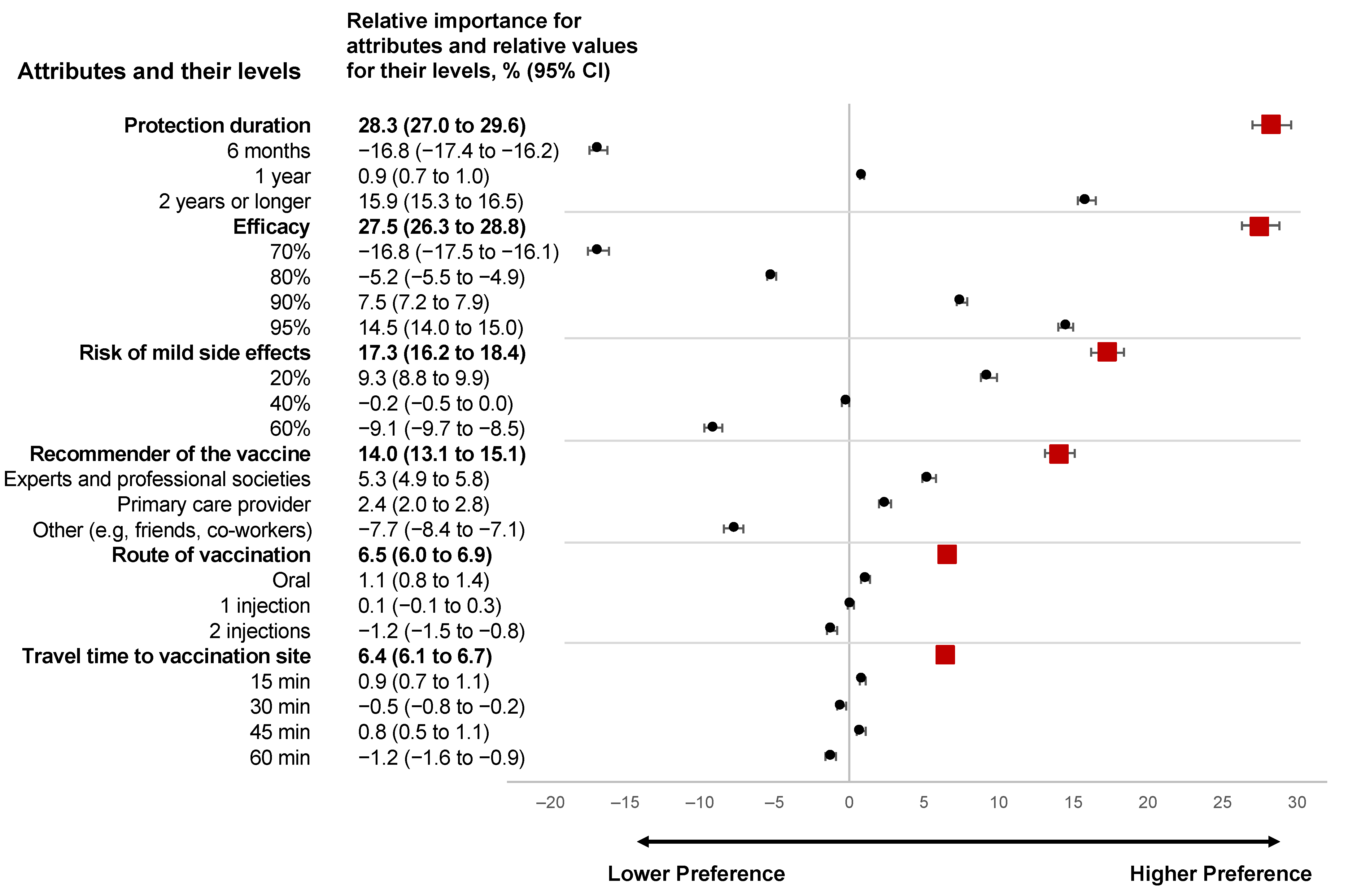
Figure 3 demonstrates the relative attribute importance scores, relative values of attribute levels, and their 95% confidence intervals. The most important attributes for the participants were vaccine protection duration (28.3 (95% CI, from 27.0 to 29.6)) and vaccine efficacy (27.5 (95% CI, from 26.3 to 28.8)). The increase in the protection duration from six months to two years was associated with higher importance: from −16.8 (95% CI, from −17.4 to −16.2) to 15.9 (95% CI, from 15.3 to 16.5), respectively. A vaccine with a higher efficacy was more preferable—the relative value increased from a negative preference of −16.8 (95% CI, from −17.5 to −16.1) for the vaccine with 70% efficacy to a positive preference of 7.5 (95%, CI, from 7.2 to 7.90) for the vaccine with 90% efficacy. The priority for vaccines with 95% efficacy has nearly doubled (14.5 (95% CI, from 14.0 to 15.0)) compared with vaccines with 90% efficacy.
The third most important attribute was the risk of vaccine mild side effects, with a relative importance of 17.3 (95% CI, from 16.2 to 18.4). A risk of mild side effects of 40% or higher was associated with lower vaccine preference. A vaccine with a 20% risk of mild side effects was shown to be the most preferable 9.3 (95% CI, from 8.8 to 9.9).
It was also important to the participants who recommended the vaccine (14.0 (95% CI, from 13.1 to 15.1)). Experts and representatives of professional societies (5.3 (95% CI, from 4.9 to 5.8)) and a primary care provider (2.4 (95% CI, from 2.0 to 2.8)) recommending vaccination were the most important source of advice and were associated with a higher likelihood of vaccine acceptance. Advice from a family member, coworkers, and friends demonstrated the lowest impact on the decision making (−7.7 (95% CI, from −8.4 to −7.1)).
The route of vaccine administration (i.e., oral or injection) and travel time to the vaccination site were the least important attributes, 6.5 (95% CI, from 6.0 to 6.9) and 6.4 (95% CI, from 6.1 to 6.7), respectively. The participants displayed a more favorable attitude toward the oral form of vaccine (1.1 (95% CI, from 0.8 to 1.4)), compared with one injection (0.1 (95% CI, from −0.1 to 0.3)). Two injections were associated with negative preferences (−1.2 (95% CI, from −1.5 to −0.8)). There was no consistency in preferences within the increase in the expected travel time to the vaccination time, suggesting that this attribute might not hold substantial importance for young adults.
The respondents had clear preferences for vaccination attributes (McFadden’s pseudo-R2 = 74.7%), meaning high goodness of fit for our model.
3.3. DCE Subgroup Analysis
Overall, we found that persons who were reluctant or unsure about undergoing vaccination prioritized risk for mild side effects substantially higher than other participants and also displayed lower priority for vaccine efficacy (Supplementary Table S3).
We observed that vaccine efficacy was substantially less important for individuals who were reluctant to undergo vaccination against COVID-19 (23.5 (95% CI, from 21.3 to 25.8); n = 94) than those inclined toward vaccination (28.7 (95% CI, from 26.9 to 30.5); n = 233), without risk factors for severe COVID-19 (27.9 (95% CI, from 26.4 to 29.3); n = 334), and with a biomedical background (28.2 (95% CI, from 26.6 to 30.1); n = 264).
Individuals reluctant or unsure about undergoing vaccination prioritized the risk for mild side effects (21.8 (95% CI, from 19.5 to 24.5)) substantially higher than individuals from other subgroups. For example, the relative attribute importance score was 16.3 (95% CI, from 14.9 to 17.7) for those who were willing to undergo vaccination (n = 233), 16.9 (95% CI, from 15.7 to 18.2) for those without risk factors for severe disease (n = 334), 16.9 (95% CI, from 15.7 to 18.2) for those with a personal history of COVID-19 (n = 96), and those with a biomedical background (17.3 (95% CI, from 15.8 to 18.8); n = 264).
3.4. Predictors of Vaccine Hesitancy
Overall, 238 persons contributed data for the analysis. Persons with missing responses (n = 89) were similar to those with complete responses for all characteristics, except for age. There was a smaller proportion of persons aged 18–24 years among those with complete data (Supplementary Table S1).
Individuals who reported rejecting any recommended vaccine in the past, before the COVID-19 pandemic, had a 3.30-fold (odds ratio, OR) increased risk (95% CI, from 1.06 to 10.31) of being reluctant to undergo vaccination against COVID-19 (Table 3). We have not observed differences among persons from different age groups, those reporting different gender, biomedical background, presence of risk factors for severe disease, a personal history of vaccine side effects, those with different socioeconomic indexes, or levels of education.
4. Discussion
Young adults are less likely to accept the COVID-19 vaccine than their older counterparts in many countries [16,17]. The vaccination rate against COVID-19 in young adults is already behind that in older adults [62]. New and innovative vaccination programs need to be developed to accelerate vaccination among vaccine-hesitant individuals. Our study provides insight into the vaccine and vaccination attributes important to young adults.
Our study demonstrated that a vaccine’s protective duration and efficacy are the most important parameters for young adults. Young adults who displayed a hesitancy to undergo vaccination against COVID-19 emphasized the risk of mild side effects and less on vaccine efficacy than those inclined to uptake vaccination. Even though some common factors affect younger and older adults’ decision making when deciding to undergo vaccination (i.e., vaccine efficacy, the risk of side effects), other factors and their importance differ from older adults.
A few large population-based population preferences studies have been conducted in the US and the UK (n = 6457) [30,38,63]. These studies tested various attributes of vaccines and vaccination programs to understand what attributes might play an important role in patients’ decision making. Similar to our study, in two US- and UK-based studies, vaccine efficacy was shown to be the most critical attribute, and higher efficacy was associated with a higher probability of vaccination [30,38]. A large US-based study with 1971 adults also concluded that a longer vaccine protection time is seen as more preferable, and a lower risk for side effects increases the probability of vaccination [30]. Our study suggests that anticipated travel time to the vaccination site might not play an important role among young adults. None of the other known to us studies tested the importance of the anticipated travel time to the vaccination site. A less intensive vaccination (i.e., one injection vs. two, oral form of vaccination vs. injections) was preferable among our participants. Similarly, American adults demonstrated a substantial negative preference for an annual vaccine booster (i.e., increased vaccination intensity) rather than a one-time vaccination and for two vaccine doses rather than one dose [30,63]. Young adults displayed a similar trend, preferring oral vaccine administration rather than one or two injections. These studies also add a better understanding of the importance of other attributes not tested in our experiment. For example, one US-based study demonstrated that mandatory vaccination was less preferable than voluntary vaccination [63]. American adults are less likely to undergo vaccination if the vaccine was made outside of the US, particularly if it originated from China [30]. It has also been demonstrated that the vaccination site can be an important attribute. Thus, in two studies, participants displayed a higher likelihood of vaccine uptake if vaccination was conducted at their general provider’s office or a health facility rather than at a mass vaccination site or a mobile vaccination unit [38,63].
Our study demonstrated that personal history of ever rejecting a recommended vaccination is associated with higher odds of reluctance toward vaccination against COVID-19 (OR, 3.30 (95% CI, from 1.06 to 10.31)). This result was similar in two US studies with 3279 adults. In one study, a history of flu vaccination in the past was associated with a 4.70-fold (from 3.55 to 6.23) increased odds of willingness to undergo vaccination against COVID-19 [64]. In another study, not having an influenza vaccine in the past year was independently associated with vaccine hesitancy [23]. Personal history of previous influenza vaccination was associated with an increased likelihood of vaccination against COVID-19 (OR, 2.74 (95% CI, from 2.12 to 3.57)) in the Czech study with 3550 healthcare workers [65]. None of the other factors in our study (e.g., gender, risk factors for severe COVID, history of side effects associated with vaccination, socioeconomic status) were shown to predict vaccination hesitancy. The above-mentioned Czech study [65] has demonstrated that female gender (OR, 0.58 (95% CI, from 0.45 to 0.75)), presence of chronic health conditions (OR, 0.80 (95% CI, from 0.66 to 0.97)), and a personal history of COVID-19 (OR, 0.41 (95% CI, from 0.34 to 0.49)) were associated with lower odds of undergoing vaccination.
A broader literature has also shown that vaccination against COVID-19 was politicized, and belonging to a political party might affect individuals’ decision making for vaccination [30,63]. Conspiracy beliefs also play an important role in persons being reluctant to undergo vaccination [66].
4.1. Future Research
Vaccine hesitancy for COVID-19 in the Czech Republic and many other developed countries still remains understudied for children and adolescents, racial and ethnic minorities, socioeconomically disadvantaged individuals, individuals affected by a disability, those who experience homelessness, and representatives of other minority groups. More research is needed to understand individuals’ needs (e.g., information, infrastructure) to maximize the vaccination rate, particularly among underserved populations. We will target these special populations in our future population-based research.
4.2. Limitations
Our study has several limitations. First, we used a convenience sample of university students, which limits the generalizability of our findings to all Czech young adults. We demonstrated that the respondents were representative of the Czech young adults in terms of age, gender, and education (Supplementary Table S2). Second, not all information was known about the currently available vaccines when the DCE was designed. For example, a 20% risk of side effects and 95% vaccine effectiveness for two years could be unachievable. Third, this study was conducted early in the COVID-19 pandemic. Results from more recent studies might provide new information. Fourth, our results might differ from actual choices due to the nature of the DCE and the inability to account for real-life behavior. Finally, the subgroup analysis for vaccine preferences was ad hoc; the sample size of some subgroups was smaller than the calculated minimum for our DCE.
5. Conclusions
This study demonstrated that protection duration, vaccine efficacy, and the potential for mild side effects play an important role in deciding whether to undergo vaccination against COVID-19 among young adults. Expected travel time to the vaccination site might not be an important attribute. Individuals reluctant or unsure about vaccination prioritized the potential for mild side effects higher and vaccine efficacy lower than vaccine inclined individuals. Our results can be used to design vaccination strategies to increase the vaccination rate among young adults.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/vaccines10020265/s1, Table S1: Comparison of respondents with and without missing data for multivariable logistic regression, Table S2: The age, gender, and educational background of the study population and of the general Czech students’ population, Table S3: Subgroup estimates of relative attribute importance scores.
Author Contributions
Conceptualization, G.D., A.E. and I.I.; methodology, G.D. and I.I.; formal analysis, G.D. and I.I.; investigation, G.D. and A.E.; data curation, G.D.; writing—original draft preparation, G.D., A.E. and I.I.; writing—review and editing, G.D. and I.I.; visualization, G.D. and I.I.; supervision, G.D. and I.I.; project administration, A.E. All authors have read and agreed to the published version of the manuscript.
Funding
G.D. and A.E. were supported in part by the Grant Agency of the Czech Technical University in Prague, grant No. SGS20/144/OHK5/2T/17. I.I. was supported by a career-development award number K12HS026370 from the Agency for Healthcare Research and Quality (AHRQ).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Faculty of Biomedical Engineering at Czech Technical University in Prague (IRB ID: B1/2021, 5 March 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank Petra Hospodkova and Vojtech Kamensky for supporting the early study design (i.e., identification of attributes and their levels, preparing recruitment materials). The authors thank Jozef Rosina and Peter Kneppo for their help with recruiting participants. The authors also thank Martin Rozanek for covering the open access fee.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the study’s design, data collection, analyses, interpretation, or writing of the manuscript.
References
- Woolf, S.H.; Chapman, D.A.; Lee, J.H. COVID-19 as the Leading Cause of Death in the United States. JAMA 2020, 325, 123–124. [Google Scholar] [CrossRef]
- Panagiotou, O.A.; Kosar, C.M.; White, E.M.; Bantis, L.E.; Yang, X.; Santostefano, C.M.; Feifer, R.A.; Blackman, C.; Rudolph, J.L.; Gravenstein, S.; et al. Risk Factors Associated With All-Cause 30-Day Mortality in Nursing Home Residents With COVID-19. JAMA Intern. Med. 2021, 181, 439. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Axfors, C.; Contopoulos-Ioannidis, D.G. Population-Level COVID-19 Mortality Risk for Non-elderly Individuals Overall and for Non-elderly Individuals without Underlying Diseases in Pandemic Epicenters. Environ. Res. 2020, 188, 109890. [Google Scholar] [CrossRef]
- Faust, J.S.; Krumholz, H.M.; Du, C.; Mayes, K.D.; Lin, Z.; Gilman, C.; Walensky, R.P. All-Cause Excess Mortality and COVID-19-Related Mortality Among US Adults Aged 25–44 Years, March–July 2020. JAMA 2021, 325, 785–787. [Google Scholar] [CrossRef]
- Shiels, M.S.; Almeida, J.S.; García-Closas, M.; Albert, P.S.; Freedman, N.D.; de González, A.B. Impact of Population Growth and Aging on Estimates of Excess U.S. Deaths During the COVID-19 Pandemic, March to August 2020. Ann. Intern. Med. 2021, 174, 437–443. [Google Scholar] [CrossRef]
- Vestergaard, L.S.; Nielsen, J.; Richter, L.; Schmid, D.; Bustos, N.; Braeye, T.; Denissov, G.; Veideman, T.; Luomala, O.; Möttönen, T.; et al. Excess All-Cause Mortality during the COVID-19 Pandemic in Europe—Preliminary Pooled Estimates from The EuroMOMO Network, March to April 2020. Eurosurveillance 2020, 25, 2001214. [Google Scholar] [CrossRef]
- Boehmer, T.K.; DeVies, J.; Caruso, E.; van Santen, K.L.; Tang, S.; Black, C.L.; Hartnett, K.P.; Kite-Powell, A.; Dietz, S.; Lozier, M.; et al. Changing Age Distribution of the COVID-19 Pandemic—United States, May–August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1404–1409. [Google Scholar] [CrossRef]
- Salvatore, P.P.; Sula, E.; Coyle, J.P.; Caruso, E.; Smith, A.R.; Levine, R.S.; Baack, B.N.; Mir, R.; Lockhart, E.R.; Tiwari, T.S.; et al. Recent Increase in COVID-19 Cases Reported Among Adults Aged 18–22 Years—United States, May 31–September 5, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1419–1424. [Google Scholar] [CrossRef]
- Cunningham, J.W.; Vaduganathan, M.; Claggett, B.L.; Jering, K.S.; Bhatt, A.S.; Rosenthal, N.; Solomon, S.D. Clinical Outcomes in Young US Adults Hospitalized With COVID-19. JAMA Intern. Med. 2021, 181, 379. [Google Scholar] [CrossRef]
- Flasche, S.; Edmunds, W.J. The role of schools and schoolaged children in SARS-CoV-2 transmission. Lancet Infect. Dis. 2021, 21, 298–299. [Google Scholar] [CrossRef]
- Casini, L.; Roccetti, M. Reopening Italy’s schools in September 2020: A Bayesian estimation of the change in the growth rate of new SARS-CoV-2 cases. BMJ Open 2021, 11, e051458. [Google Scholar] [CrossRef]
- Daly, M.; Jones, A.; Robinson, E. Public Trust and Willingness to Vaccinate Against COVID-19 in the US From October 14, 2020, to March 29, 2021. JAMA 2021, 325, 2397–2399. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. Changes in COVID-19 Vaccine Intent From April/May to June/July 2021. JAMA 2021, 326, 1971–1974. [Google Scholar] [CrossRef]
- Mascola, J.R.; Graham, B.S.; Fauci, A.S. SARS-CoV-2 Viral Variants-Tackling a Moving Target. JAMA 2021, 325, 1261–1262. [Google Scholar] [CrossRef]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Danaee, M.; Ahmed, J.; Lachyan, A.; Cai, C.Z.; Lin, Y.; Hu, Z.; Tan, S.Y.; Lu, Y.; et al. COVID-19 Vaccination Intention and Vaccine Characteristics Influencing Vaccination Acceptance: A Global Survey of 17 Countries. Infect. Dis. Poverty 2021, 10, 122. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to Participate in a COVID-19 Vaccine Clinical Trial and to Get Vaccinated against COVID-19 in France during the Pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Weintraub, R.L.; Subramanian, L.; Karlage, A.; Ahmad, I.; Rosenberg, J. COVID-19 Vaccine To Vaccination: Why Leaders Must Invest In Delivery Strategies Now. Health Aff. 2021, 40, 33–41. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once We Have It, Will We Use It? A European Survey on Willingness to Be Vaccinated against COVID-19. Eur. J. Heal. Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of Intention to Vaccinate against COVID-19: Results of a Nationwide Survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 Vaccine Hesitancy among Medical Students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine Hesitancy’ among University Students in Italy during the COVID-19 Pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological Characteristics Associated with COVID-19 Vaccine Hesitancy and Resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards Vaccines and Intention to Vaccinate against COVID-19: Implications for Public Health Communications. Lancet Reg. Heal. Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 Related Medical Mistrust, Health Impacts, and Potential Vaccine Hesitancy Among Black Americans Living With HIV. JAIDS J. Acquir. Immune Defic. Syndr. 2021, 86, 200–207. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Tuells, J.; Egoavil, C.M.; Pena Pardo, M.A.; Montagud, A.C.; Montagud, E.; Caballero, P.; Zapater, P.; Puig-Barberá, J.; Hurtado-Sanchez, J.A. Seroprevalence Study and Cross-Sectional Survey on COVID-19 for a Plan to Reopen the University of Alicante (Spain). Int. J. Environ. Res. Public Health 2021, 18, 1908. [Google Scholar] [CrossRef]
- Grüner, S.; Krüger, F. The Intention to Be Vaccinated against COVID-19: Stated Preferences before Vaccines Were Available. Appl. Econ. Lett. 2021, 28, 1847–1851. [Google Scholar] [CrossRef]
- Kose, S.; Mandiracioglu, A.; Sahin, S.; Kaynar, T.; Karbus, O.; Ozbel, Y. Vaccine Hesitancy of the COVID-19 by Health Care Personnel. Int. J. Clin. Pract. 2021, 75, e13917. [Google Scholar] [CrossRef]
- Marsh, K.; van Til, J.A.; Molsen-David, E.; Juhnke, C.; Hawken, N.; Oehrlein, E.M.; Choi, Y.C.; Duenas, A.; Greiner, W.; Haas, K.; et al. Health Preference Research in Europe: A Review of Its Use in Marketing Authorization, Reimbursement, and Pricing Decisions—Report of the ISPOR Stated Preference Research Special Interest Group. Value Heal. 2020, 23, 831–841. [Google Scholar] [CrossRef]
- Hoogink, J.; Verelst, F.; Kessels, R.; van Hoek, A.J.; Timen, A.; Willem, L.; Beutels, P.; Wallinga, J.; de Wit, G.A. Preferential Differences in Vaccination Decision-Making for Oneself or One’s Child in the Netherlands: A Discrete Choice Experiment. BMC Public Health 2020, 20, 828. [Google Scholar] [CrossRef]
- McPhedran, R.; Toombs, B. Efficacy or Delivery? An Online Discrete Choice Experiment to Explore Preferences for COVID-19 Vaccines in the UK. Econ. Lett. 2021, 200, 109747. [Google Scholar] [CrossRef]
- Motta, M. Can a COVID-19 Vaccine Live up to Americans’ Expectations? A Conjoint Analysis of How Vaccine Characteristics Influence Vaccination Intentions. Soc. Sci. Med. 2021, 272, 113642. [Google Scholar] [CrossRef]
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health—A Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public Preference for COVID-19 Vaccines in China: A Discrete Choice Experiment. Heal. Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the chadox1 Ncov-19 Vaccine (AZD1222) Against SARS-CoV-2: An Interim Analysis of Four Random-Ised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford–AstraZeneca COVID-19 Vaccine Efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Pfizer and BioNTech Conclude Phase 3 Study of COVID-19 Vaccine Candidate, Meeting All Primary Efficacy Endpoints. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine (accessed on 24 August 2021).
- AstraZeneca AZD1222 Vaccine Met Primary Efficacy Endpoint in Preventing COVID-19. Available online: https://www.astrazeneca.com/content/astraz/media-centre/press-releases/2020/azd1222hlr.html (accessed on 24 August 2021).
- Moderna Moderna’s COVID-19 Vaccine Candidate Meets its Primary Efficacy Endpoint in the First Interim Analysis of the Phase 3 COVE Study. Available online: https://investors.modernatx.com/news-releases/news-release-details/modernas-covid-19-vaccine-candidate-meets-its-primary-efficacy (accessed on 24 August 2021).
- US Food and Drug Administration. Moderna COVID-19 Vaccine EUA Fact Sheet for Vaccination Providers. Available online: https://www.fda.gov/media/144637/download (accessed on 24 August 2021).
- US Food and Drug Administration. Pfizer-BioNTech COVID-19 Vaccine EUA Fact Sheet for Vaccination Providers. Available online: https://www.fda.gov/media/144413/download (accessed on 24 August 2021).
- US Food and Drug Administration. Janssen COVID-19 Vaccine EUA Fact Sheet for Vaccination Providers. Available online: https://www.fda.gov/media/146304/download (accessed on 24 August 2021).
- World Health Organization. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 24 August 2021).
- Trevena, L.J.; Zikmund-Fisher, B.J.; Edwards, A.; Gaissmaier, W.; Galesic, M.; Han, P.K.; King, J.; Lawson, M.L.; Linder, S.K.; Lipkus, I.; et al. Presenting Quantitative Information about Decision Outcomes: A Risk Communication Primer for Patient Decision Aid Developers. BMC Med. Inform. Decis. Mak. 2013, 13, S7. [Google Scholar] [CrossRef] [Green Version]
- McCaffery, K.J.; Holmes-Rovner, M.; Smith, S.K.; Rovner, D.; Nutbeam, D.; Clayman, M.L.; Kelly-Blake, K.; Wolf, M.S.; Sheridan, S.L. Addressing Health Literacy in Patient Decision Aids. BMC Med. Inform. Decis. Mak. 2013, 13, S10. [Google Scholar] [CrossRef] [Green Version]
- Veldwijk, J.; Lambooij, M.S.; van Til, J.A.; Groothuis-Oudshoorn, C.G.M.; Smit, H.A.; de Wit, G.A. Words or graphics to present a Discrete Choice Experiment: Does it matter? Patient Educ. Couns. 2015, 98, 1376–1384. [Google Scholar] [CrossRef] [Green Version]
- Orme, B.K. Sample Size Issues for Conjoint Analysis. In Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research; Research Publishers: Madison, WI, USA, 2020; pp. 57–66. ISBN 978-1-60147-115-4. [Google Scholar]
- de Bekker-Grob, E.W.; Donkers, B.; Jonker, M.F.; Stolk, E.A. Sample Size Requirements for Discrete-Choice Experiments in Healthcare: A Practical Guide. Patient 2015, 8, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Conjoint.ly. Technical Points on DCE with Conjoint.ly. Available online: https://conjointly.com/guides/conjoint-technical-notes/ (accessed on 24 August 2021).
- U.S. Centers for Disease Control and Prevention Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 24 March 2021).
- McFadden, D. Conditional logit analysis of qualitative choice behavior. In Frontiers in Economics; Zarembka, P., Ed.; Academic Press: New York, NY, USA, 1974; pp. 105–142. [Google Scholar]
- Hughes, R.A.; Heron, J.; Sterne, J.A.C.; Tilling, K. Accounting for missing data in statistical analyses: Multiple imputation is not always the answer. Int. J. Epidemiol. 2019, 48, 1294–1304. [Google Scholar] [CrossRef]
- White, I.R.; Carlin, J.B. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat. Med. 2010, 29, 2920–2931. [Google Scholar] [CrossRef]
- Diesel, J.; Sterrett, N.; Dasgupta, S.; Kriss, J.L.; Barry, V.; Esschert, K.V.; Whiteman, A.; Cadwell, B.L.; Weller, D.; Qualters, J.R.; et al. COVID-19 Vaccination Coverage Among Adults—United States, December 14, 2020–May 22, 2021. MMWR Recomm. Rep. 2021, 70, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Eshun-Wilson, I.; Mody, A.; Tram, K.H.; Bradley, C.; Sheve, A.; Fox, B.; Thompson, V.; Geng, E.H. Preferences for COVID-19 vaccine distribution strategies in the US: A discrete choice survey. PLoS ONE 2021, 16, e0256394. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.J.; Southwell, B.G.; McCormack, L.A.; Bann, C.M.; MacDonald, P.D.M.; Frasier, A.M.; Bevc, C.A.; Brewer, N.T.; Squiers, L.B. Correction to: Predictors of Willingness to Get a COVID-19 vaccine in the U.S. BMC Infect. Dis. 2021, 21, 383. [Google Scholar] [CrossRef] [PubMed]
- Štěpánek, L.; Janošíková, M.; Nakládalová, M.; Štěpánek, L.; Boriková, A.; Vildová, H. Motivation to COVID-19 Vaccination and Reasons for Hesitancy in Employees of a Czech Tertiary Care Hospital: A Cross-Sectional Survey. Vaccines 2021, 9, 863. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, J.; Ling, J. Predicting COVID-19 Vaccination Intention Using Protection Motivation Theory and Conspiracy Beliefs. Vaccine 2021, 39, 6269–6275. [Google Scholar] [CrossRef]
Figure 1.
An example choice card used in the discrete choice experiment survey. Participants could magnify the pictograms.
Figure 1.
An example choice card used in the discrete choice experiment survey. Participants could magnify the pictograms.

Figure 2.
Flow diagram. DCE—discrete choice experiment.

Figure 3.
The relative importance of attributes and relative values of attribute levels. Attributes are ordered from the most important to the least important. Squares correspond to the relative importance of attributes and the lines represent 95% confidence interval. Circles correspond to the relative values of attribute levels and the lines represent 95% confidence interval.
Figure 3.
The relative importance of attributes and relative values of attribute levels. Attributes are ordered from the most important to the least important. Squares correspond to the relative importance of attributes and the lines represent 95% confidence interval. Circles correspond to the relative values of attribute levels and the lines represent 95% confidence interval.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Attributes and levels for hypothetical COVID-19 vaccines and vaccination environment.
| Attributes | Levels |
|---|---|
| Efficacy in preventing COVID-19 | 70%; 80%; 90%; 95% |
| Risk of mild side effects | 20%; 40%; 60% |
| Protection duration | 6 months; 1 year; 2 years |
| Vaccine administration route | Oral; 1 injection; 2 injections |
| Recommender of the vaccine | Experts and professional societies; primary care provider; family or friends |
| Expected travel time to the vaccination site | 15 min; 30 min; 45 min; 60 min |
Table 2.
Participants’ characteristics.
| Characteristics | All Participants, n (%) n = 445 | Reluctant to Undergo Vaccination for COVID-19, n (%) a n = 94 | Inclined to Undergo Vaccination for COVID-19, n (%) b n = 233 |
|---|---|---|---|
| Age, years | |||
| 18–24 | 305 (68.5) | 71 (75.5) | 177 (76.0) |
| 25–34 | 83 (18.7) | 16 (17.0) | 41 (17.6) |
| ≥35 | 28 (6.3) | 7 (7.4) | 15 (6.4) |
| PNTS or no answer | 29 (6.5) | 0 (0.0) | 0 (0.0) |
| Gender | |||
| Woman | 272 (61.1) | 64 (68.1) | 151 (64.8) |
| Man | 142 (31.9) | 30 (31.9) | 79 (33.9) |
| PNTS or no answer | 31 (7.0) | 0 (0.0) | 3 (1.3) |
| Ethnicity c | |||
| Czech or multiple, including Czech | 370 (80.6) | 79 (80.6) | 212 (88.7) |
| Moravian | 17 (3.7) | 4 (4.1) | 7 (2.9) |
| Slovak | 19 (4.1) | 4 (4.1) | 11 (4.6) |
| Not listed | 12 (2.7) | 5 (5.1) | 4 (1.7) |
| PNTS or no answer | 41 (8.9) | 6 (6.1) | 5 (2.1) |
| Education background | |||
| Primary education | 1 (0.2) | 0 (0.0) | 1 (0.4) |
| Secondary education | 258 (58.0) | 62 (66.0) | 157 (67.4) |
| Post-secondary education | 7 (1.6) | 3 (3.2) | 3 (1.3) |
| Bachelor or equivalent | 137 (30.8) | 27 (28.7) | 63 (27.0) |
| Master’s or equivalent | 8 (1.8) | 2 (2.1) | 4 (1.7) |
| PhD or another doctorate | 5 (1.1) | 0 (0.0) | 4 (1.7) |
| PNTS or no answer | 29 (6.5) | 0 (0.0) | 1 (0.4) |
| Biomedical background | |||
| Yes | 264 (59.3) | 56 (59.6) | 134 (57.5) |
| No | 139 (31.2) | 35 (37.2) | 88 (37.8) |
| PNTS or no answer | 42 (9.4) | 3 (3.2) | 11 (4.7) |
| Employment status | |||
| Student | 307 (69.0) | 74 (78.7) | 188 (80.7) |
| Employee | 87 (19.6) | 15 (16.0) | 31 (13.3) |
| Self-employed/Entrepreneur | 7 (1.6) | 2 (2.1) | 5 (2.1) |
| Unemployed | 7 (1.6) | 2 (2.1) | 5 (2.1) |
| Other | 5 (1.1) | 0 (0.0) | 3 (1.3) |
| PNTS or no answer | 32 (7.2) | 1 (1.1) | 1 (0.4) |
| Annual gross household income, EUR d | |||
| <6900 | 67 (15.1) | 19 (20.2) | 36 (15.5) |
| 6900–13,900 | 54 (12.1) | 11 (11.7) | 28 (12.0) |
| 13,900–20,800 | 66 (14.8) | 12 (12.8) | 36 (15.5) |
| 20,800–30,100 | 54 (12.1) | 11 (11.7) | 28 (12.0) |
| 30,100–37,000 | 44 (9.9) | 7 (7.4) | 33 (14.2) |
| 37,000–41,700 | 14 (3.1) | 3 (3.2) | 5 (2.1) |
| 41,700–46,300 | 9 (2.0) | 2 (2.1) | 4 (1.7) |
| >46,300 | 19 (4.3) | 4 (4.3) | 12 (5.2) |
| PNTS or no answer | 118 (26.5) | 25 (26.6) | 51 (21.9) |
| Socioeconomic index (SEI) e | |||
| <33rd percentile (lowest SEI) | 115 (25.8) | 61 (26.2) | 30 (31.9) |
| ≥33rd percentile (highest SEI) | 200 (44.9) | 114 (48.9) | 37 (39.4) |
| No answer | 130 (29.2) | 58 (24.9) | 27 (28.7) |
| Pregnancy (percent of women) | |||
| Yes | 2 (0.7) | 1 (1.6) | 1 (0.7) |
| Planning within one year | 9 (3.3) | 5 (7.8) | 2 (1.3) |
| No | 260 (95.6) | 58 (90.6) | 147 (97.4) |
| No answer | 1 (0.4) | 0 (0.0) | 1 (0.7) |
| Risk factors for severe COVID-19 f | |||
| One or more | 77 (17.3) | 13 (13.8) | 44 (18.9) |
| None | 334 (75.1) | 78 (83.0) | 187 (80.3) |
| PNTS or no answer | 34 (7.6) | 3 (3.2) | 2 (0.9) |
| Rejected any recommended vaccine in the past | |||
| Yes | 22 (4.9) | 12 (12.8) | 10 (4.3) |
| No | 387 (87.0) | 79 (84.0) | 221 (94.8) |
| PNTS or no answer | 36 (8.1) | 3 (3.2) | 2 (0.9) |
| Adverse events with any vaccine (not against COVID-19) c | |||
| Allergic reaction | 12 (2.7) | 5 (5.2) | 5 (2.1) |
| Other adverse events | 67 (14.9) | 17 (17.5) | 28 (11.9) |
| No or not sure | 339 (75.3) | 73 (75.3) | 201 (85.5) |
| PNTS or no answer | 32 (7.1) | 2 (2.1) | 1 (0.4) |
| History of COVID-19 c | |||
| Personal | 96 (16.4) | 21 (17.5) | 52 (16.6) |
| Relatives | 172 (29.4) | 34 (28.3) | 102 (32.5) |
| Other (e.g., friends, coworkers) | 203 (34.6) | 38 (31.7) | 113 (36.0) |
| No or not sure | 84 (14.3) | 24 (20.0) | 46 (14.6) |
| PNTS or no answer | 31 (5.3) | 3 (2.5) | 1 (0.3) |
| Vaccinated against COVID-19 | |||
| Yes, first dose or fully | 86 (19.3) | Not Applicable | Not Applicable |
| No | 331 (74.4) | 94 (100) | 233 (100) |
| PNTS or no answer | 28 (6.3) | Not Applicable | Not Applicable |
| Agreement with the statement “I want to be vaccinated against COVID-19 as soon as the vaccine is available for me.” g | |||
| Strongly agree | 140 (42.3) | Not Applicable | 140 (60.1) |
| Agree | 93 (28.1) | Not Applicable | 93 (39.9) |
| Not sure | 54 (16.3) | 54 (57.4) | Not Applicable |
| Disagree | 23 (6.9) | 23 (24.5) | Not Applicable |
| Strongly disagree | 17 (5.1) | 17 (18.1) | Not Applicable |
PNTS—prefer not to say. a Individuals who answered “Strongly disagree,” “Disagree,” or “Unsure” to the statement “I want to be vaccinated against COVID-19 as soon as the vaccine is available for me.” b Individuals who answered “Strongly agree” or “Agree” to the statement “I want to be vaccinated against COVID-19 as soon as the vaccine is available for me.” c Respondents could select several categories—the sum does not add to 100%. d We used the average Czech koruna to Euro exchange rate from the Czech national bank for April 2021, EUR 1 = CZK 25.924, rounded off to the nearest hundred. e A ratio of reported household income (numerator) and household size (denominator). f Any set of the following: cancer, chronic liver disease; chronic obstructive pulmonary disease; cardiovascular diseases (e.g., heart failure, ischemic heart disease, cardiomyopathy); weakened immune system (e.g., after organ transplantation, human immunodeficiency virus, etc.); obesity; sickle cell disease; smoking; type 2 diabetes mellitus. g Among those who have not started or completed vaccination against COVID-19.
Table 3.
Results of multivariable logistic regression for sociodemographic predictors of reluctance to undergo vaccination against COVID-19 (n = 238).
Table 3.
Results of multivariable logistic regression for sociodemographic predictors of reluctance to undergo vaccination against COVID-19 (n = 238).
| Participants’ Characteristics | Reluctance to Undergo Vaccination | |
|---|---|---|
| Adjusted Odds Ratio (95% CI) | p | |
| Age, years | ||
| 18–24 | 0.99 (0.43–2.28) | 0.975 |
| ≥25 | Referent | |
| Gender | ||
| Man | 1.06 (0.55–2.03) | 0.852 |
| Woman | Referent | |
| Biomedical background | ||
| No | 1.65 (0.89–3.10) | 0.114 |
| Yes, any | Referent | |
| Risk factors for severe COVID-19 a | ||
| ≥1 | 1.56 (0.72–3.65) | 0.282 |
| None | Referent | |
| Adverse events with any vaccine (not against COVID-19) | ||
| Yes | 1.62 (0.72–3.52) | 0.233 |
| No | Referent | |
| Rejected any recommended vaccination in the past (not against COVID-19) | ||
| Yes | 3.30 (1.06–10.31) | 0.037 |
| No | Referent | |
| Socioeconomic index (SEI) | ||
| <33rd percentile (lowest SEI) | 1.51 (0.81–2.80) | 0.191 |
| ≥33rd percentile (highest SEI) | Referent | |
| Education | ||
| Bachelor degree or higher | 0.75 (0.35–1.56) | 0.446 |
| Post-secondary or lower | Referent | |
a Any set of the following: cancer, chronic liver disease; chronic obstructive pulmonary disease; cardiovascular diseases (e.g., heart failure, ischemic heart disease, cardiomyopathy); weakened immune system (e.g., after organ transplantation, human immunodeficiency virus, etc.); obesity; sickle cell disease; smoking; type 2 diabetes mellitus.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Donin, G.; Erfányuková, A.; Ivlev, I. Factors Affecting Young Adults’ Decision Making to Undergo COVID-19 Vaccination: A Patient Preference Study. Vaccines 2022, 10, 265. https://doi.org/10.3390/vaccines10020265
AMA Style
Donin G, Erfányuková A, Ivlev I. Factors Affecting Young Adults’ Decision Making to Undergo COVID-19 Vaccination: A Patient Preference Study. Vaccines. 2022; 10(2):265. https://doi.org/10.3390/vaccines10020265
Chicago/Turabian StyleDonin, Gleb, Anna Erfányuková, and Ilya Ivlev. 2022. "Factors Affecting Young Adults’ Decision Making to Undergo COVID-19 Vaccination: A Patient Preference Study" Vaccines 10, no. 2: 265. https://doi.org/10.3390/vaccines10020265
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.