
Acceptability of the Vaccine against COVID-19 in Spanish Health Sciences Students: A Cross-Sectional Study
 , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Tool
2.3. Procedure
2.4. Ethical Considerations
3. Results
3.1. Population Description
3.2. Variables Relating to the COVID-19 Disease
3.3. Variables Relating to the Acceptance of Vaccines in General and against COVID-19
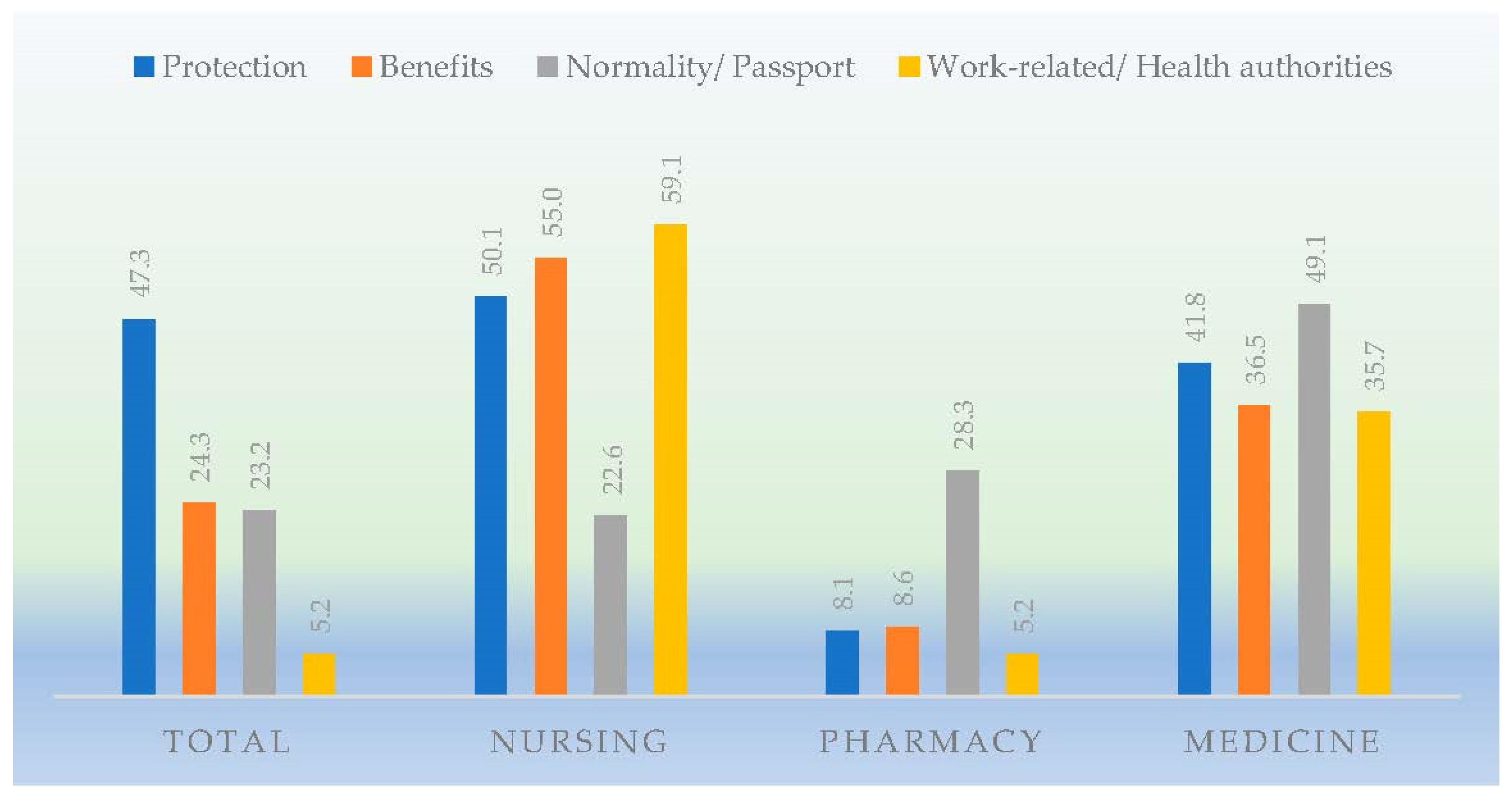
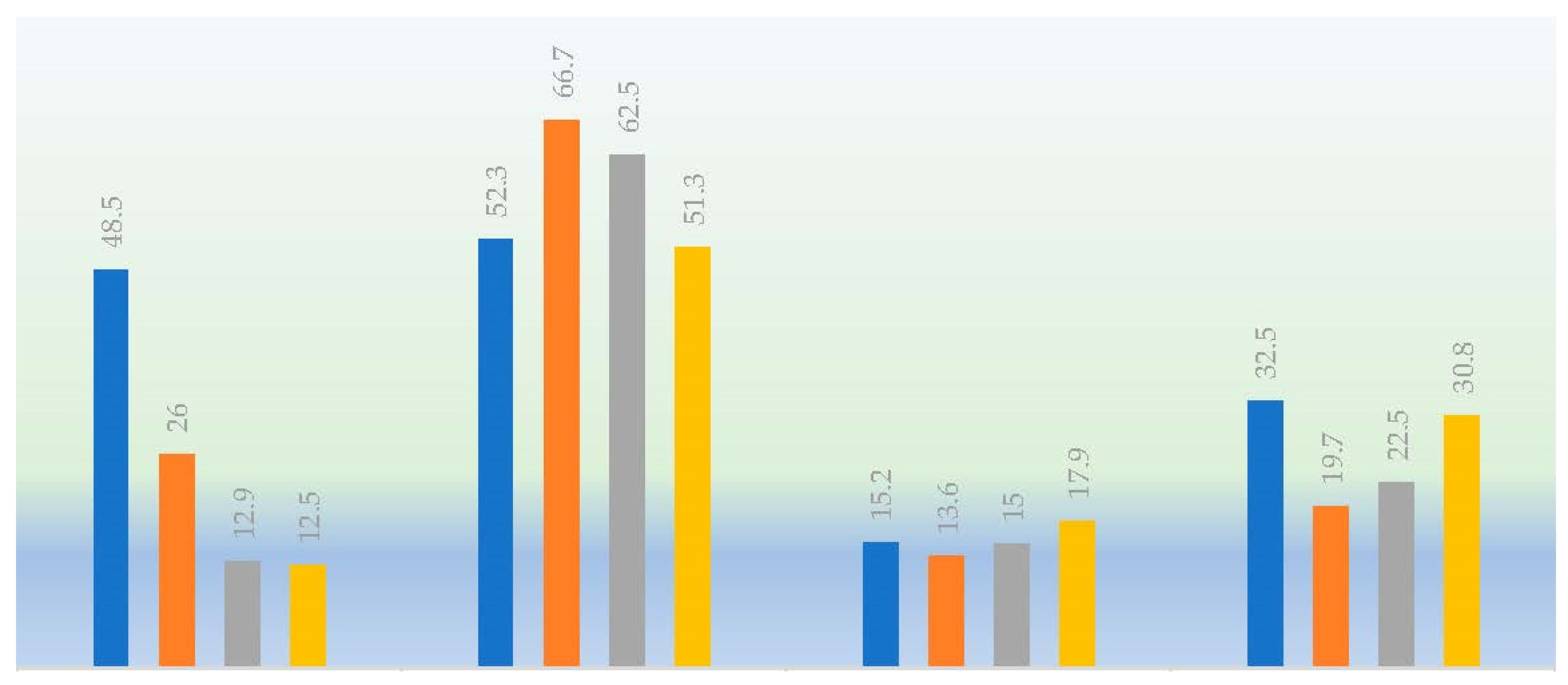
3.4. Justified Reasons for the Acceptance or Rejection of the Vaccines against COVID-19
3.5. Variables Relating to the Secondary Effects of the Vaccines against COVID-19
3.6. Multivariate Logistic Regression between the Administered Vaccines and the Declared Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Desmond, A.; Offit, P.A. On the Shoulders of Giants—From Jenner’s Cowpox to mRNA Covid Vaccines. N. Engl. J. Med. 2021, 384, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Marco, V. COVID-19 vaccines: The pandemic will not end overnight. Lancet Microbe 2020, 2, 30226-3. [Google Scholar] [CrossRef]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Reintjes, R.; Das, E.; Klemm, C.; Richardus, J.H.; Keßler, V.; Ahmad, A. “Pandemic Public Health Paradox”: Time Series Analysis of the 2009/10 Influenza A/H1N1 Epidemiology, Media Attention, Risk Perception and Public Reactions in 5 European Countries. PLoS ONE 2016, 11, e0151258. [Google Scholar] [CrossRef]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef]
- Albrecht, D. Vaccination, politics and COVID-19 impacts. BMC Public Health 2022, 22, 96. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Ali, M.; Hossain, A. What is the extent of COVID-19 vaccine hesitancy in Bangladesh? A cross-sectional rapid national survey. BMJ Open 2021, 11, e050303. [Google Scholar] [CrossRef]
- Secosan, I.; Virga, D.; Crainiceanu, Z.; Bratu, L.; Bratu, T. Infodemia: Another Enemy for Romanian Frontline Healthcare Workers to Fight during the COVID-19 Outbreak. Medicina 2020, 56, 679. [Google Scholar] [CrossRef]
- Gagneur, A.; Gosselin, V.; Dubé, È. Motivational interviewing: A promising tool to address vaccine hesitancy. Vaccine 2018, 36, 6553–6555. [Google Scholar] [CrossRef]
- Farooq, F.; Rathore, F.A. COVID-19 Vaccination and the Challenge of Infodemic and Disinformation. J. Korean Med. Sci. 2021, 36, e78. [Google Scholar] [CrossRef] [PubMed]
- Pérez Milena, A. El desafío de informar a la población como estrategia para la cobertura óptima de la vacunación contra la COVID-19. Comunidad 2021, 23, 1. [Google Scholar]
- Agencia Española del Medicamento y Productos Sanitarios. Vigilancia de la Seguridad de las Vacunas Frente a la COVID-19. [Internet] Madrid: Ministerio de Sanidad. 2021. Available online: https://www.aemps.gob.es/medicamentosUsoHumano/vacunas/docs/vigilancia_seguridad_vacunas_COVID-19.pdf? (accessed on 24 June 2022).
- Petousis-Harris, H. Assessing the Safety of COVID-19 Vaccines: A Primer. Drug Saf. 2020, 43, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Matić, Z.; Šantak, M. Current view on novel vaccine technologies to combat human infectious diseases. Appl. Microbiol. Biotechnol. 2021, 106, 25–56. [Google Scholar] [CrossRef]
- Azimi, M.; Dehzad, W.M.; Atiq, M.A.; Bahain, B.; Asady, A. Adverse Effects of the COVID-19 Vaccine Reported by Lecturers and Staff of Kabul University of Medical Sciences, Kabul, Afghanistan. Infect. Drug Resist. 2021, 14, 4077–4083. [Google Scholar] [CrossRef]
- Jeon, M.; Kim, J.; Oh, C.E.; Lee, J.-Y. Adverse Events Following Immunization Associated with Coronavirus Disease 2019 Vaccination Reported in the Mobile Vaccine Adverse Events Reporting System. J. Korean Med. Sci. 2021, 36, e114. [Google Scholar] [CrossRef]
- Working Group on Vaccine Hesitancy (SAGE). Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 26 December 2020).
- World Health Organization (WHO). Vaccination: European Commission and World Health Organization Join Forces to Promote the Benefits of Vaccines. Available online: https://www.who.int/news/item/12-09-2019-vaccination-european-commission-and-world-health-organization-join-forces-to-promote-the-benefits-of-vaccines (accessed on 4 December 2020).
- Freed, G.L.; Clark, S.J.; Butchart, A.T.; Singer, D.C.; Davis, M.M. Sources and Perceived Credibility of Vaccine-Safety Information for Parents. Pediatrics 2011, 127, S107–S112. [Google Scholar] [CrossRef]
- Vorsters, A.; Tack, S.; Hendrickx, G.; Vladimirova, N.; Bonanni, P.; Pistol, A.; Metličar, T.; Pasquin, M.A.; Mayer, M.; Aronsson, B.; et al. A summer school on vaccinology: Responding to identified gaps in pre-service immunisation training of future health care workers. Vaccine 2010, 28, 2053–2059. [Google Scholar] [CrossRef]
- Siddiqui, M.; Salmon, D.A.; Omer, S.B. Epidemiology of vaccine hesitancy in the United States. Hum. Vaccines Immunother. 2013, 9, 2643–2648. [Google Scholar] [CrossRef]
- Kernéis, S.; Jacquet, C.; Bannay, A.; May, T.; Launay, O.; Verger, P.; Pulcini, C.; Abgueguen, P.; Ansart, S.; Bani-Sadr, F.; et al. Vaccine Education of Medical Students: A Nationwide Cross-sectional Survey. Am. J. Prev. Med. 2017, 53, e97–e104. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Gómez Marco, J.J.; Álvarez Pasquín, M.J.; Martín Martín, S. Efectividad y seguridad de las vacunas para el SARS-CoV-2 actualmente disponibles. FMC 2021, 28, 442–451. [Google Scholar] [CrossRef]
- Grupo de Trabajo Técnico de Vacunación COVID-19 de la Ponencia de Programa y Registro de Vacunaciones. Información Sobre las Vacunas en Tiempos de COVID-19. Consejo Interterritorial del SNS. Ministerio de Sanidad. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/covid19/ (accessed on 14 May 2022).
- Olmedo Lucerón, C.; Limia Sánchez, A.; García Gómez, M. La vacunación frente a la COVID-19 en colectivos laborales. Rev. Esp. Salud Pública 2021, 95, 1. [Google Scholar]
- Sharma, M.; Davis, R.; Wilkerson, A. COVID-19 Vaccine Acceptance among College Students: A Theory-Based Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4617. [Google Scholar] [CrossRef]
- Tavolacci, M.; Dechelotte, P.; Ladner, J. COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France. Vaccines 2021, 9, 654. [Google Scholar] [CrossRef]
- Mo, P.; Luo, S.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Xie, L.; Lau, J. Intention to Receive the COVID-19 Vaccination in China: Application of the Diffusion of Innovations Theory and the Moderating Role of Openness to Experience. Vaccines 2021, 9, 129. [Google Scholar] [CrossRef]
- Grech, V.; Gauci, C. WITHDRAWN: Vaccine hesitancy in the University of Malta Faculties of Health Sciences, Dentistry and Medicine vis-à-vis influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020, 12, 105258. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Qiao, S.; Tam, C.C.; Li, X. Risk Exposures, Risk Perceptions, Negative Attitudes Toward General Vaccination, and COVID-19 Vaccine Acceptance Among College Students in South Carolina. Am. J. Health Promot. 2021, 36, 175–179. [Google Scholar] [CrossRef]
- Qiao, S.; Friedman, D.B.; Tam, C.C.; Zeng, C.; Li, X. Vaccine acceptance among college students in South Carolina: Do information sources and trust in information make a difference? medRxiv 2020. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18, 2407. [Google Scholar] [CrossRef]
- Pastorino, R.; Villani, L.; Mariani, M.; Ricciardi, W.; Graffigna, G.; Boccia, S. Impact of COVID-19 Pandemic on Flu and COVID-19 Vaccination Intentions among University Students. Vaccines 2021, 9, 70. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Lambert, P.-H.; Podda, A. Education in Vaccinology: An Important Tool for Strengthening Global Health. Front. Immunol. 2018, 9, 1134. [Google Scholar] [CrossRef]
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef]
- Le An, P.; Nguyen, H.T.N.; Nguyen, D.D.; Vo, L.Y.; Huynh, G. The intention to get a COVID-19 vaccine among the students of health science in Vietnam. Hum. Vaccines Immunother. 2021, 17, 4823–4828. [Google Scholar] [CrossRef]
- Wagner, A.L.; Masters, N.B.; Domek, G.J.; Mathew, J.L.; Sun, X.; Asturias, E.J.; Ren, J.; Huang, Z.; Contreras-Roldan, I.L.; Gebremeskel, B.; et al. Comparisons of Vaccine Hesitancy across Five Low- and Middle-Income Countries. Vaccines 2019, 7, 155. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020, 43, 445–449. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Rodríguez-Blanco, N.; Montero-Navarro, S.; Botella-Rico, J.; Felipe-Gómez, A.; Sánchez-Más, J.; Tuells, J. Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5272. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, N.; Singleton, J.A. COVID-19 vaccination intent, perceptions, and reasons for not vaccinating among groups prioritized for early vaccination—United States, September and December 2020. Am. J. Transplant. 2021, 21, 1650–1656. [Google Scholar] [CrossRef]
- Mascarenhas, A.K.; Lucia, V.C.; Kelekar, A.; Afonso, N.M. Dental students’ attitudes and hesitancy toward COVID-19 vaccine. J. Dent. Educ. 2021, 85, 1504–1510. [Google Scholar] [CrossRef]
- Van Der Weerd, W.; Timmermans, D.R.; Beaujean, D.J.; Oudhoff, J.; Van Steenbergen, J.E. Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health 2011, 11, 575. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Nursing n (%) | Pharmacy n (%) | Medicine n (%) | Total n (%) | IC 95% | p-Value | |
|---|---|---|---|---|---|---|
| 716 (52.0) | 124 (11.5) | 382 (36.5) | 1222 (100) | |||
| Sex | ||||||
| Male | 95 (13.3) | 46 (37.1) | 97 (25.4) | 238 (19.5) | (14.5–24.5) | <0.001 |
| Female | 621 (86.7) | 78 (62.9) | 285 (74.6) | 984 (80.5) | (78.0–82.9) | |
| Origin | ||||||
| Spanish | 697 (97.3) | 120 (96.8) | 373 (97.6) | 1190 (97.4) | (96.5–98.3) | 0.867 |
| Not Spanish | 19 (2.7) | 4 (3.2) | 9 (2.4) | 32 (2.6) | (0.0–8.1) | |
| Living arrangement | ||||||
| Alone | 487 (68.0) | 69 (55.6) | 266 (69.6) | 822 (67.3) | (64.1–70.5) | 0.013 |
| With a partner | 229 (32.0) | 55 (44.4) | 116 (30.4) | 400 (32.7) | (28.1–37.3) | |
| Age (years) | 22.2 ± 5.0 | 22.8 ± 5.2 * | 21.6 ± 4.1 † | 22.0 ± 4.8 | ||
| Academic year | ||||||
| Lower | 376 (52.5) | 47 (37.9) | 142 (37.2) | 565 (46.2) | (42.1–50.3) | <0.001 |
| Upper | 340 (47.5) | 77 (62.1) | 240 (62.8) | 657 (53.8) | (50.0–57.6) | |
| Chronic disease | ||||||
| No | 622 (86.9) | 113 (91.1) | 353 (92.4) | 1088 (89.0) | (87.1–90.8) | 0.015 |
| Yes | 94 (13.1) | 11 (8.9) | 29 (7.6) | 134 (11.0) | (5.7–16.3) | |
| Tobacco | ||||||
| No | 609 (85.1) | 109 (87.9) | 345 (90.3) | 1063 (87.0) | (84.9–89.0) | 0.045 |
| Yes | 107 (14.9) | 15 (12.1) | 37 (9.7) | 159 (13.0) | (7.7–18.2) | |
| Alcohol | ||||||
| No | 643 (89.8) | 104 (83.9) | 348 (91.1) | 1095 (89.6) | (87.8–91.4) | 0.070 |
| Yes | 73 (10.2) | 20 (16.1) | 34 (8.9) | 127 (10.4) | (5.1–15.7) | |
| Psychoactive drugs | ||||||
| No | 705 (98.5) | 121 (97.6) | 375 (98.2) | 1201 (98.3) | (97.6–99.0) | 0.767 |
| Yes | 11 (1.5) | 3 (2.4) | 7 (1.8) | 21 (1.7) | (0.0–7.2) |
| Nursing n (%) | Pharmacy n (%) | Medicine n (%) | Total n (%) | IC 95% | p-Value | |
|---|---|---|---|---|---|---|
| Have you had COVID-19? (n = 1222) | ||||||
| Yes | 100 (14.0) | 15 (12.1) | 35 (9.2) | 150 (12.3) | (7.0–17.5) | 0.069 |
| No | 616 (86.0) | 109 (87.9) | 347 (90.8) | 1072 (87.7) | (85.7–89.6) | |
| Did you catch it at university? (n = 150) | ||||||
| Yes | 4 (4.0) | 0 (0) | 0 (0) | 4 (2.7) | (0–18.6) | 0.527 |
| No | 78 (78.0) | 13 (86.7) | 31 (88.6) | 122 (81.3) | (74.4–88.2) | |
| Don’t know | 18 (18.0) | 2 (13.3) | 4 (11.4) | 24 (16.0) | (1.3–30.6) | |
| Have you had to quarantine? (n = 1213) | ||||||
| Yes | 316 (44.4) | 50 (40.7) | 168 (44.3) | 534 (44.0) | (36.8–51.8) | 0.729 |
| No | 395 (55.6) | 73 (59.3) | 211 (55.7) | 679 (56.0) | (49.0–62.4) | |
| Have any of your family members or friends died from COVID-19? (n = 1222) | ||||||
| Yes | 118 (16.5) | 17 (13.7) | 68 (17.8) | 203 (16.6) | (11.5–21.7) | 0.562 |
| No | 598 (83.5) | 107 (86.3) | 314 (82.2) | 1019 (83.4) | (81.1–85.7) | |
| Have you taken a diagnostic test, antigen test or PCR? (n = 1222) | ||||||
| Yes | 526 (73.5) | 70 (56.5) | 269 (70.4) | 865 (70.8) | (67.7–73.8) | <0.001 |
| No | 190 (26.5) | 54 (43.5) | 113 (29.6) | 357 (29.2) | (24.5–34.0) | |
| What were the results of the antigen test or PCR? (n = 865) | ||||||
| Positive | 77 (14.6) | 13 (18.6) | 32 (11.9) | 122 (14.1) | (7.9–20.3) | 0.307 |
| Negative | 449 (85.4) | 57 (81.4) | 237 (88.1) | 743 (85.9) | (83.4–88.4) | |
| Nursing n (%) | Pharmacy n (%) | Medicine n (%) | Total n (%) | IC 95% | p-Value | |
|---|---|---|---|---|---|---|
| Would you vaccinate against COVID-19? (n = 1222) | ||||||
| Yes | 695 (97.1) | 120 (96.8) | 377 (98.7) | 1192 (97.5) | (96.6–98.4) | 0.214 |
| No | 21 (2.9) | 4 (3.2) | 5 (1.3) | 30 (2.5) | (0–8.0) | |
| Should there be a choice of COVID-19 vaccine? (n = 1222) | ||||||
| Yes | 434 (60.6) | 73 (58.9) | 208 (54.5) | 715 (58.5) | (54.8–62.1) | 0.142 |
| No | 282 (39.4) | 51 (41.1) | 174 (45.5) | 507 (41.5) | (37.2–45.8) | |
| Which vaccine would you like to be given? (n = 1222) | ||||||
| Comirnaty® | 542 (75.7) | 82 (66.1) | 291 (76.2) | 915 (74.9) | (72.1–77.7) | 0.043 |
| Spikevax® | 57 (8.0) | 13 (10.5) | 41 (10.7) | 111 (9.1) | (3.7–14.4) | |
| Vaxzevria® | 77 (10.8) | 15 (12.1) | 29 (7.6) | 121 (9.9) | (4.6–15.2) | |
| Jcovden® | 40 (5.6) | 14 (11.3) | 21 (5.5) | 75 (6.1) | (0.6–11.5) | |
| Have you received the COVID-19 vaccine? (n = 1222) | ||||||
| Yes | 433 (60.5) | 24 (19.4) | 149 (39.0) | 606 (49.6) | (45.6–53.6) | <0.001 |
| No | 283 (39.5) | 100 (80.6) | 233 (61.0) | 616 (50.4) | (46.5–54.3) | |
| If you have received it, which vaccine did you receive? * (n = 606) | ||||||
| Comirnaty® | 221 (51.0) | 1 (4.2) | 61 (40.9) | 283 (46.7) | (40.9–52.5) | <0.001 |
| Spikevax® | 49 (11.3) | 1 (4.2) | 22 (14.7) | 72 (11.8) | (4.4–19.2) | |
| Vaxzevria® | 163 (37.6) | 22 (91.7) | 66 (44.3) | 251 (41.4) | (35.63–47.5) | |
| Do you have a complete childhood vaccination schedule? (n = 1222) | ||||||
| Yes | 705 (98.5) | 112 (90.3) | 374 (97.9) | 1191 (97.5) | (96.6–98.4) | <0.001 |
| No | 6 (0.8) | 6 (4.8) | 3 (0.8) | 15 (1.2) | (0–6.7) | |
| Don’t know | 5 (0.7) | 6 (4.8) | 5 (1.3) | 16 (1.3) | (0–6.8) | |
| Have you ever had a flu vaccination? (n = 1222) | ||||||
| Yes | 460 (64.2) | 50 (40.3) | 221 (57.9) | 731 (59.8) | (56.2–63.3) | <0.001 |
| No | 256 (35.8) | 74 (59.7) | 161 (42.1) | 491 (40.2) | (35.8–44.5) | |
| Nursing n (%) | Pharmacy n (%) | Medicine n (%) | Total n (%) | IC 95% | p-Value | |
|---|---|---|---|---|---|---|
| Does it produce more adverse effects than other vaccines? (n = 1204) | ||||||
| Yes | 61 (8.6) | 39 (15.4) | 16 (9.8) | 116 (9.6) | (4.2–15.0) | 0.132 |
| No | 487 (68.4) | 74 (60.2) | 239 (64.8) | 800 (66.4) | (63.1–69.7) | |
| Don’t know | 164 (23.0) | 30 (24.4) | 94 (25.5) | 288 (23.9) | (18.9–28.8) | |
| Do there exist unknown adverse effects of the COVID-19 vaccine? (n = 1222) | ||||||
| Yes | 266 (37.2) | 59 (47.6) | 136 (35.6) | 461 (37.7) | (33.3–42.1) | 0.026 |
| No | 99 (13.8) | 23 (18.5) | 62 (16.2) | 184 (15.1) | (9.9–20.3) | |
| Don’t know | 351 (49.0) | 42 (33.9) | 184 (48.2) | 577 (47.2) | (43.1–51.3) | |
| Do you trust in the recommendations of the health authorities? (n = 1219) | ||||||
| Yes | 651 (91.2) | 101 (82.1) | 335 (87.7) | 1087 (89.2) | (87.3–91.0) | 0.035 |
| No | 61 (8.5) | 21 (17.1) | 45 (11.8) | 127 (10.4) | (5.1–15.7) | |
| Don’t know | 2 (0.3) | 1 (0.8) | 2 (0.5) | 5 (0.4) | (0–5.9) | |
| After vaccination, have you suffered adverse effects? (n = 606) | ||||||
| Yes | 374 (86.4) | 22 (91.7) | 123 (82.6) | 519 (85.6) | (82.6–88.6) | 0.298 |
| No | 59 (13.6) | 2 (8.3) | 26 (17.4) | 87 (14.4) | (7.0–21.8) | |
| What adverse effects have you suffered? * n = 374, n = 22, n = 123, n = 519 | ||||||
| Pain at injection site | 291 (77.8) | 16 (72.7) | 84 (68.3) | 391 (75.3) | (71.0–79.6) | 0.101 |
| Tiredness | 205 (54.8) | 13 (59.1) | 62 (50.4) | 280 (53.9) | (48.1–59.7) | 0.616 |
| Fever | 174 (46.5) | 17 (77.3) | 62 (50.4) | 253 (48.7) | (42.5–54.8) | 0.018 |
| Generalized muscle pain | 174 (46.5) | 11 (50.0) | 57 (46.3) | 242 (46.6) | (40.3–52.9) | 0.948 |
| Headache | 186 (49.7) | 11 (50.0) | 38 (30.9) | 235 (45.3) | (38.9–51.6) | 0.001 |
| Shivering | 140 (37.4) | 14 (63.6) | 42 (34.1) | 196 (37.8) | (31.0–44.6) | 0.031 |
| Swollen glands | 28 (7.5) | 1 (4.5) | 14 (11.4) | 43 (8.3) | (0.1–15.5) | 0.321 |
| Vomiting | 22 (5.9) | 3 (13.6) | 10 (8.1) | 35 (6.7) | (0.0–15.0) | 0.290 |
| Other | 22 (5.9) | 1 (4.5) | 3 (2.4) | 26 (5.0) | (0.0–13.3) | 0.314 |
| Total | Vaxzevria® | Comirnaty® | Spikevax® | Chi2 | Vaxzevria® vs. Comirnaty® | p-Value | Vaxzevria® vs. Spikevax® | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| 519 (100) | 229 (44.1) | 221 (42.6) | 69 (13.3) | ||||||
| Variable | n (%) | n (%) | n (%) | n (%) | OR (95% CI) | OR (95% CI) | |||
| Pain at injection site | |||||||||
| No (R) | 128 (24.7) | 62 (27.1) | 52 (23.5) | 14 (20.3) | 0.454 | 1 | 1 | 1 | 1 |
| Yes | 391 (75.3) | 167 (72.9) | 169 (76.5) | 55 (79.7) | 1.59 (0.92–2.73) | 0.095 | 2.40 (1.11–5.18) | 0.026 | |
| Tiredness | |||||||||
| No (R) | 239 (46.1) | 77 (33.6) | 119 (53.8) | 43 (62.3) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 280 (53.9) | 152 (66.4) | 102 (46.2) | 26 (37.7) | 1.04 (0.60–1.78) | 0.892 | 0.71 (0.34–1.49) | 0.361 | |
| Fever | |||||||||
| No (R) | 266 (51.3) | 55 (24.0) | 162 (73.3) | 49 (71.0) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 253 (48.7) | 174 (76.0) | 59 (26.7) | 20 (29.0) | 0.18 (0.11–0.28) | <0.001 | 0.27 (0.13–0.54) | <0.001 | |
| Generalized muscle pain | |||||||||
| No (R) | 277 (53.4) | 86 (37.6) | 144 (65.2) | 47 (68.1) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 242 (46.6) | 143 (62.4) | 77 (34.8) | 22 (31.9) | 0.70 (0.42–1.16) | 0.168 | 0.79 (0.39–1.61) | 0.513 | |
| Headache | |||||||||
| No (R) | 284 (54.7) | 94 (41.0) | 143 (64.7) | 47 (68.1) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 235 (45.3) | 135 (59.0) | 78 (35.3) | 22 (31.9) | 0.68 (0.41–1.13) | 0.140 | 0.62 (0.31–1.25) | 0.183 | |
| Shivering | |||||||||
| No (R) | 323 (62.2) | 97 (42.4) | 168 (76.0) | 58 (84.1) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 196 (37.8) | 132 (57.6) | 53 (24.0) | 11 (15.9) | 0.58 (0.35–0.99) | 0.044 | 0.29 (0.13–0.67) | 0.003 | |
| Swollen glands | |||||||||
| No (R) | 476 (91.7) | 211 (921) | 203 (91.9) | 62 (89.9) | 0.829 | 1 | 1 | 1 | 1 |
| Yes | 43 (8.3) | 18 (7.9) | 18 (8.1) | 7 (10.1) | 2.49 (1.06–5.85) | 0.056 | 3.12 (1.05–9.29) | 0.052 | |
| Vomiting | |||||||||
| No (R) | 484 (93.3) | 197 (86.0) | 219 (99.1) | 68 (98.6) | <0.001 | 1 | 1 | 1 | 1 |
| Yes | 35 (6.7) | 32 (14.0) | 2 (0.9) | 1 (1.4) | 0.09 (0.02–0.45) | 0.003 | 0.17 (0.02–1.49) | 0.110 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Blanco, N.; Vicente-Alcalde, N.; Cubero-Plazas, L.; Sánchez-Más, J.; Montagud, E.; Moragues, R.; Gabaldón-Bravo, E.; Hurtado-Sanchez, J.A.; Tuells, J. Acceptability of the Vaccine against COVID-19 in Spanish Health Sciences Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12244. https://doi.org/10.3390/ijerph191912244
Rodríguez-Blanco N, Vicente-Alcalde N, Cubero-Plazas L, Sánchez-Más J, Montagud E, Moragues R, Gabaldón-Bravo E, Hurtado-Sanchez JA, Tuells J. Acceptability of the Vaccine against COVID-19 in Spanish Health Sciences Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12244. https://doi.org/10.3390/ijerph191912244
Chicago/Turabian StyleRodríguez-Blanco, Noelia, Nancy Vicente-Alcalde, Laura Cubero-Plazas, Jesús Sánchez-Más, Emilia Montagud, Raul Moragues, Eva Gabaldón-Bravo, Jose Antonio Hurtado-Sanchez, and José Tuells. 2022. "Acceptability of the Vaccine against COVID-19 in Spanish Health Sciences Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12244. https://doi.org/10.3390/ijerph191912244