
Determinants of COVID-19 Vaccination Hesitancy among Romanian Pregnant Women

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Data
2.2. Surveys and Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Markowicz, I.; Rudawska, I. Struggling with COVID-19—A Framework for Assessing Health System Performance. Sustainability 2021, 13, 11146. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Tirnea, L.; Avram, V.; Marincu, I. Exploring Pregnancy Outcomes Associated with SARS-CoV-2 Infection. Medicina 2021, 57, 796. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Neamtu, R.; Sorop, V.-B.; Horhat, D.I.; Gorun, F.; Tudorache, E.; Gorun, O.M.; Boarta, A.; Tuta-Sas, I.; Citu, I.M. Assessing SARS-CoV-2 Vertical Transmission and Neonatal Complications. J. Clin. Med. 2021, 10, 5253. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [Green Version]
- Marbán-Castro, E.; Pons-Duran, C.; García-Otero, L.; Chen, H.; Herrera, L.B.; Gil, M.d.M.; Goncé, A.; Ferriols-Pérez, E.; Rodríguez, M.Á.; Toro, P.; et al. Acceptability of Clinical Trials on COVID-19 during Pregnancy among Pregnant Women and Healthcare Providers: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 10717. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19: Latest Safety Data Provide Reassurance about Use of mRNA Vaccines during Pregnancy. Available online: https://www.ema.europa.eu/en/news/covid-19-latest-safety-data-provide-reassurance-about-use-mrna-vaccines-during-pregnancy (accessed on 6 January 2022).
- The American College of Obstetricians and Gynecologists. COVID-19 Vaccination Considerations for Obstetric–Gynecologic Care. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/12/covid-19-vaccination-considerations-for-obstetric-gynecologic-care (accessed on 3 January 2022).
- Donders, G.G.G.; Grinceviciene, S.; Haldre, K.; Lonnee-Hoffmann, R.; Donders, F.; Tsiakalos, A.; Adriaanse, A.; Martinez de Oliveira, J.; Ault, K.; Mendling, W.; et al. ISIDOG Consensus Guidelines on COVID-19 Vaccination for Women before, during and after Pregnancy. J. Clin. Med. 2021, 10, 2902. [Google Scholar] [CrossRef]
- Simionescu, A.A.; Streinu-Cercel, A.; Popescu, F.-D.; Stanescu, A.M.A.; Vieru, M.; Danciu, B.M.; Miron, V.D.; Săndulescu, O. Comprehensive Overview of Vaccination during Pregnancy in Europe. J. Pers. Med. 2021, 11, 1196. [Google Scholar] [CrossRef]
- Bin Naeem, S.; Kamel Boulos, M.N. COVID-19 Misinformation Online and Health Literacy: A Brief Overview. Int. J. Environ. Res. Public Health 2021, 18, 8091. [Google Scholar] [CrossRef]
- Guvernul Romaniei. Actualizare Zilnică—Evidența Persoanelor Vaccinate Împotriva COVID-19. Available online: https://vaccinare-covid.gov.ro/actualizare-zilnica-20-12-evidenta-persoanelor-vaccinate-impotriva-covid-19/ (accessed on 4 January 2022).
- Breslin, G.; Dempster, M.; Berry, E.; Cavanagh, M.; Armstrong, N.C. COVID-19 vaccine uptake and hesitancy survey in Northern Ireland and Republic of Ireland: Applying the theory of planned behaviour. PLoS ONE 2021, 16, e0259381. [Google Scholar] [CrossRef]
- Martin, L.R.; Petrie, K.J. Understanding the Dimensions of Anti-Vaccination Attitudes: The Vaccination Attitudes Examination (VAX) Scale. Ann. Behav. Med. 2017, 51, 652–660. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J.G. A Proactive Approach for Managing COVID-19: The Importance of Understanding the Motivational Roots of Vaccination Hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 575950. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Bert, F.; Voglino, G.; Buttinelli, E.; D’Errico, M.M.; De Waure, C.; Di Giovanni, P.; Fantini, M.P.; Giuliani, A.R.; Marranzano, M.; et al. Attitudes towards compulsory vaccination in Italy: Results from the NAVIDAD multicentre study. Vaccine 2018, 36, 3368–3374. [Google Scholar] [CrossRef] [Green Version]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Heidari, S.; Palmer-Ross, A.; Goodman, T. A Systematic Review of the Sex and Gender Reporting in COVID-19 Clinical Trials. Vaccines 2021, 9, 1322. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Wang, J.; Ji, Q.; Dong, S.; Zhao, S.; Li, X.; Zhu, Q.; Long, S.; Zhang, J.; Jin, H. Factors Influencing Vaccine Hesitancy in China: A Qualitative Study. Vaccines 2021, 9, 1291. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Gorun, F.; Motoi, S.; Malita, D.; Navolan, D.B.; Nemescu, D.; Olariu, T.R.; Craina, M.; Vilibic-Cavlek, T.; Ciohat, I.; Boda, D.; et al. Cytomegalovirus seroprevalence in pregnant women in the western region of Romania: A large-scale study. Exp. Ther. Med. 2020, 20, 2439–2443. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Babicki, M.; Malchrzak, W.; Hans-Wytrychowska, A.; Mastalerz-Migas, A. Impact of Vaccination on the Sense of Security, the Anxiety of COVID-19 and Quality of Life among Polish. A Nationwide Online Survey in Poland. Vaccines 2021, 9, 1444. [Google Scholar] [CrossRef] [PubMed]
- Hudson, A.; Montelpare, W.J. Predictors of Vaccine Hesitancy: Implications for COVID-19 Public Health Messaging. Int. J. Environ. Res. Public Health 2021, 18, 8054. [Google Scholar] [CrossRef]
- Cristina, I.O.M.; Nicoleta, C.; Cătălin, D.R.; Margareta, F. Regional Development in Romania: Empirical Evidence Regarding the Factors for Measuring a Prosperous and Sustainable Economy. Sustainability 2021, 13, 3942. [Google Scholar] [CrossRef]


{kind=link}
| Variables * | Pregnant (n = 184) | Non-Pregnant (n = 161) | p |
|---|---|---|---|
| Age | 30.6 ± 7.2 | 29.1 ± 7.8 | 0.064 |
| Place of Origin | 0.798 | ||
| Rural | 65 (35.3%) | 59 (36.6%) | |
| Urban | 119 (64.7%) | 102 (33.4%) | |
| Marital Status | 0.256 | ||
| Married/Concubinage | 169 (91.8%) | 142 (88.2%) | |
| Single/Divorced/Widowed | 15 (8.2%) | 19 (11.8%) | |
| Income | 0.023 | ||
| Below Average | 116 (63.0%) | 82 (50.9%) | |
| Above Average | 68 (37.0%) | 79 (49.1%) | |
| Education | 0.794 | ||
| ≤12 years | 40 (21.7%) | 38 (23.6%) | |
| >12 years | 124 (67.3%) | 123 (76.4%) | |
| Occupation | 0.012 | ||
| Employed/Self-Employed | 145 (78.9%) | 143 (88.8%) | |
| Unemployed | 39 (21.1%) | 18 (11.2%) | |
| Behavior | |||
| Frequent alcohol consumption | 11 (5.9%) | 16 (9.9%) | 0.171 |
| Frequent smoker | 20 (10.8%) | 39 (24.2%) | 0.001 |
| Trusting SARS-CoV-2 vaccine | 0.549 | ||
| Yes | 79 (42.9%) | 64 (39.7%) | |
| No | 105 (57.1%) | 97 (60.3%) | |
| Trusting other vaccines | 0.597 | ||
| Yes | 160 (86.9%) | 143 (88.8%) | |
| No | 24 (13.1%) | 18 (11.2%) |
| Survey Questions * | Pregnant (n = 184) | Non-Pregnant (n = 161) | p |
|---|---|---|---|
| VAX score, median (IQR) | 31 (8) | 26 (9) | <0.001 |
| Questions 1–3 (concerns about trusting vaccines), median (IQR) | 7 (3) | 5 (3) | <0.001 |
| Questions 4–6 (concerns about unpredictable effects), median (IQR) | 10 (5) | 9 (4) | 0.011 |
| Questions 7–9 (concerns about commercial profits), median (IQR) | 6 (3) | 4 (2) | <0.001 |
| Questions 10–12 (preference to natural immunity), median (IQR) | 8 (4) | 7 (3) | 0.016 |
| COVID-19 Vaccination Feeling | <0.001 | ||
| Confident | 63 (34.3%) | 39 (24.2%) | |
| Unsure | 25 (13.5%) | 57 (35.4%) | |
| Hesitant | 96 (52.2%) | 65 (40.3%) | |
| Other reasons for hesitancy | n = 96 | n = 65 | |
| Trusting rumors on social media | 75 (78.1%) | 41 (63.0%) | 0.036 |
| Previous unpleasant vaccine side effects | 3 (3.1%) | 2 (3.0%) | 0.986 |
| Insufficient information about vaccines | 25 (26.0%) | 20 (30.7%) | 0.511 |
| Not afraid of COVID-19 | 13 (13.5%) | 10 (15.3%) | 0.743 |
| Not believing in SARS-CoV-2 existence | 6 (6.2%) | 4 (6.1%) | 0.980 |
| Not believing in vaccines | 8 (8.3%) | 11 (16.9%) | 0.097 |
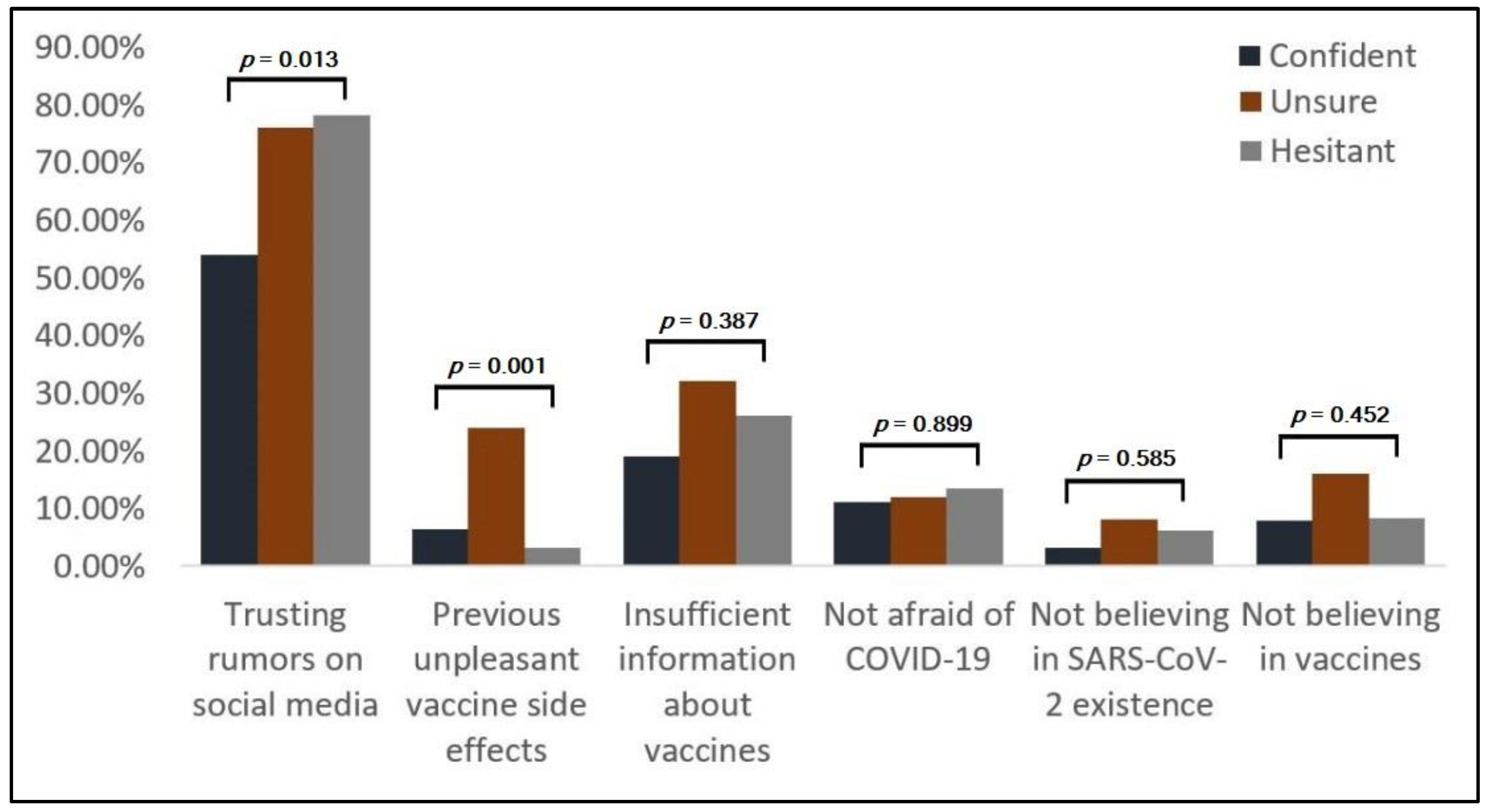
| Decision Factors * | Overall (n = 184) | Confident (n = 63) | Unsure (n = 25) | Hesitant (n = 96) | p |
|---|---|---|---|---|---|
| Trusting rumors on social media | 125 (67.9%) | 34 (53.9%) | 19 (76.0%) | 72 (78.1%) | 0.013 |
| Previous unpleasant vaccine side effects | 13 (7.1%) | 4 (6.3%) | 6 (24.0%) | 3 (3.1%) | 0.001 |
| Insufficient information about vaccines | 45 (24.4%) | 12 (19.0%) | 8 (32.0%) | 25 (26.0%) | 0.387 |
| Not afraid of COVID-19 | 23 (12.5%) | 7 (11.1%) | 3 (12.0%) | 13 (13.5%) | 0.899 |
| Not believing in SARS-CoV-2 existence | 10 (5.4%) | 2 (3.2%) | 2 (8.0%) | 6 (6.2%) | 0.585 |
| Not believing in vaccines | 17 (9.2%) | 5 (7.9%) | 4 (16.0%) | 8 (8.3%) | 0.452 |
| Factors | Pregnant Hesitancy (OR–95% CI) | p | Non-Pregnant Hesitancy (OR–95% CI) | p |
|---|---|---|---|---|
| Age | 1.00 (0.97–1.04) | 0.944 | 1.00 (0.96–1.03) | 0.913 |
| Place of Origin | 0.011 | 0.044 | ||
| Rural | 1.67 (1.27–2.38) | 1.52 (1.06–1.91) | ||
| Urban | 1.18 (0.74–1.89) | 1.03 (0.63–1.15) | ||
| Marital Status | 0.716 | 0.681 | ||
| Married/Concubinage ^ | 0.88 (0.36–1.44) | 0.94 (0.63–1.48) | ||
| Single/Divorced/Widowed | 1.06 (0.82–1.21) | 0.97 (0.71–1.09) | ||
| Income | 0.002 | 0.039 | ||
| Below Average | 2.52 (1.74–3.08) | 2.86 (1.72–3.76) | ||
| Above Average | 1.13 (0.93–1.42) | 1.05 (0.83–1.46) | ||
| Education | 0.573 | 0.418 | ||
| ≤12 years | 1.25 (1.04–1.62) | 1.30 (1.04–1.78) | ||
| >12 years | 0.92 (0.63–1.17) | 1.01 (0.85–1.22) | ||
| Occupation | 0.131 | 0.294 | ||
| Employed/Self-Employed ^ | 1.14 (0.86–1.34) | 0.90 (0.68–1.20) | ||
| Unemployed | 1.36 (0.97–1.59) | 1.33 (0.92–1.67) | ||
| Behavior | ||||
| Alcohol consumption | 0.82 (0.39–1.27) | 0.728 | 0.84 (0.32–1.31) | 0.661 |
| Smoking | 0.75 (0.30–1.14) | 0.842 | 0.78 (0.45–1.24) | 0.807 |
| Reasons for hesitancy | ||||
| Trusting rumors on social media | 3.01 (1.84–4.66) | <0.001 | 2.47 (1.79–3.05) | <0.001 |
| Previous unpleasant vaccine side effects | 1.12 (1.01–1.48) | 0.057 | 1.29 (1.07–1.68) | 0.040 |
| Insufficient information about vaccines | 1.24 (0.90–1.33) | 0.146 | 1.16 (0.84–1.21) | 0.243 |
| Not afraid of COVID-19 | 2.33 (1.29–3.17) | <0.001 | 2.64 (1.30–3.09) | <0.001 |
| Not believing in SARS-CoV-2 existence | 3.43 (2.18–4.51) | <0.001 | 3.06 (2.11–3.94) | <0.001 |
| Not believing in vaccines | 4.05 (2.07–6.42) | <0.001 | 5.11 (3.27–7.70) | <0.001 |
| Trusting SARS-CoV-2 vaccine | 0.042 | 0.066 | ||
| Yes ^ | 0.64 (0.21–0.86) | 0.79 (0.54–1.04) | ||
| No | 1.74 (1.13–2.58) | 1.66 (1.05–2.83) | ||
| Trusting other vaccines | 0.094 | 0.172 | ||
| Yes ^ | 0.73 (0.49–1.11) | 0.92 (0.41–1.43) | ||
| No | 1.27 (1.04–1.76) | 1.30 (0.91–1.86) |
| Factors | Adjusted OR | 95% CI | p |
|---|---|---|---|
| By rural place of origin | 1.11 | 1.01–1.35 | 0.062 |
| By below average level of income | 2.06 | 1.74–2.71 | 0.004 |
| By trusting rumors on social media | 2.38 | 1.90–2.94 | <0.001 |
| By not being afraid of COVID-19 | 1.89 | 1.54–2.27 | 0.020 |
| By not believing in SARS-CoV-2 existence | 2.67 | 2.12–3.04 | <0.001 |
| By not believing in vaccines | 3.15 | 2.80–3.49 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, I.M.; Citu, C.; Gorun, F.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Tudorache, E.; Margan, M.-M.; Hosin, S.; et al. Determinants of COVID-19 Vaccination Hesitancy among Romanian Pregnant Women. Vaccines 2022, 10, 275. https://doi.org/10.3390/vaccines10020275
Citu IM, Citu C, Gorun F, Motoc A, Gorun OM, Burlea B, Bratosin F, Tudorache E, Margan M-M, Hosin S, et al. Determinants of COVID-19 Vaccination Hesitancy among Romanian Pregnant Women. Vaccines. 2022; 10(2):275. https://doi.org/10.3390/vaccines10020275
Chicago/Turabian StyleCitu, Ioana Mihaela, Cosmin Citu, Florin Gorun, Andrei Motoc, Oana Maria Gorun, Bogdan Burlea, Felix Bratosin, Emanuela Tudorache, Madalin-Marius Margan, Samer Hosin, and et al. 2022. "Determinants of COVID-19 Vaccination Hesitancy among Romanian Pregnant Women" Vaccines 10, no. 2: 275. https://doi.org/10.3390/vaccines10020275