
Acceptance Rates of COVID-19 Vaccine Highlight the Need for Targeted Public Health Interventions


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Factors Associated with COVID-19 Vaccine Acceptance
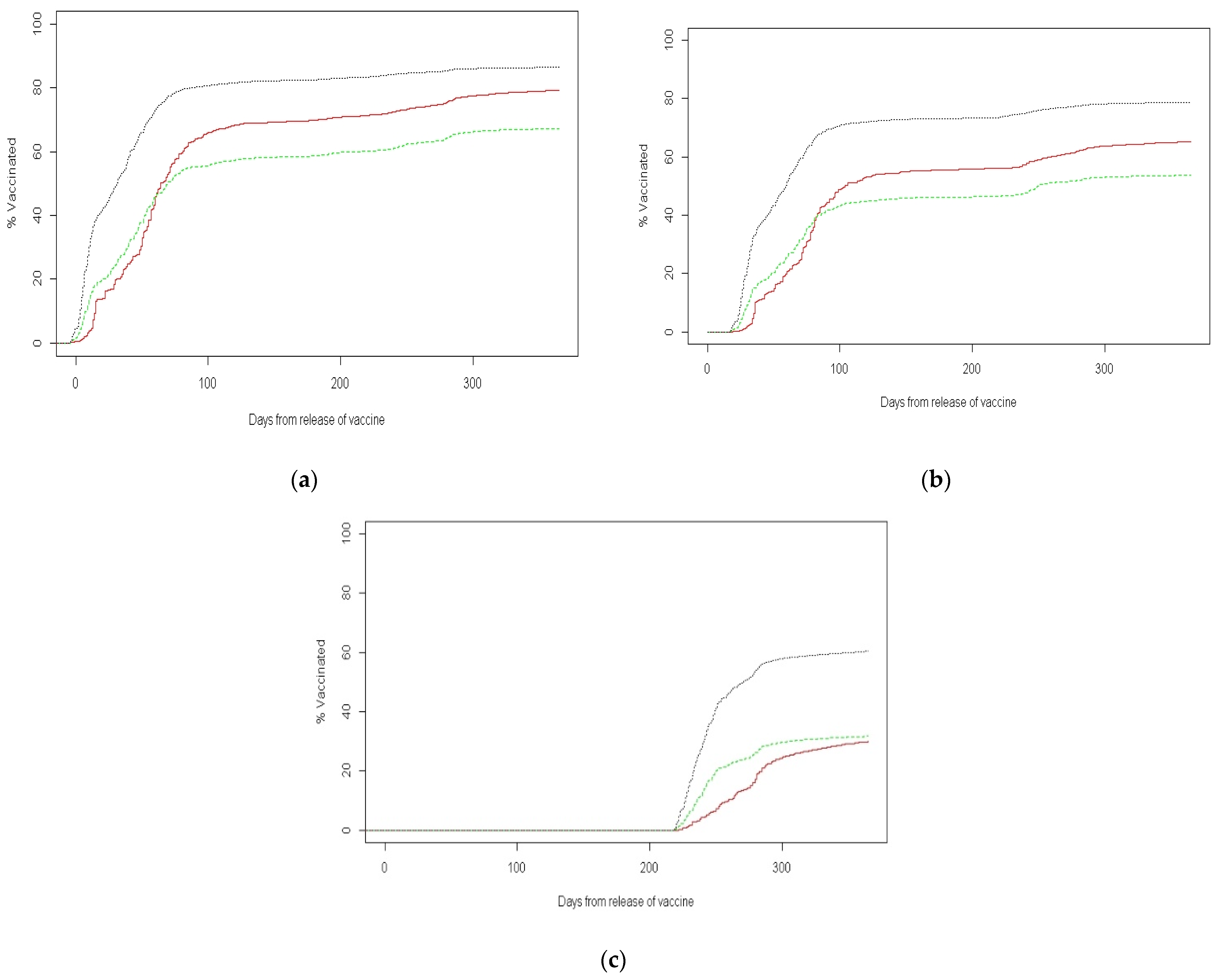
3.2. Analysis by Number of Vaccine Doses Received
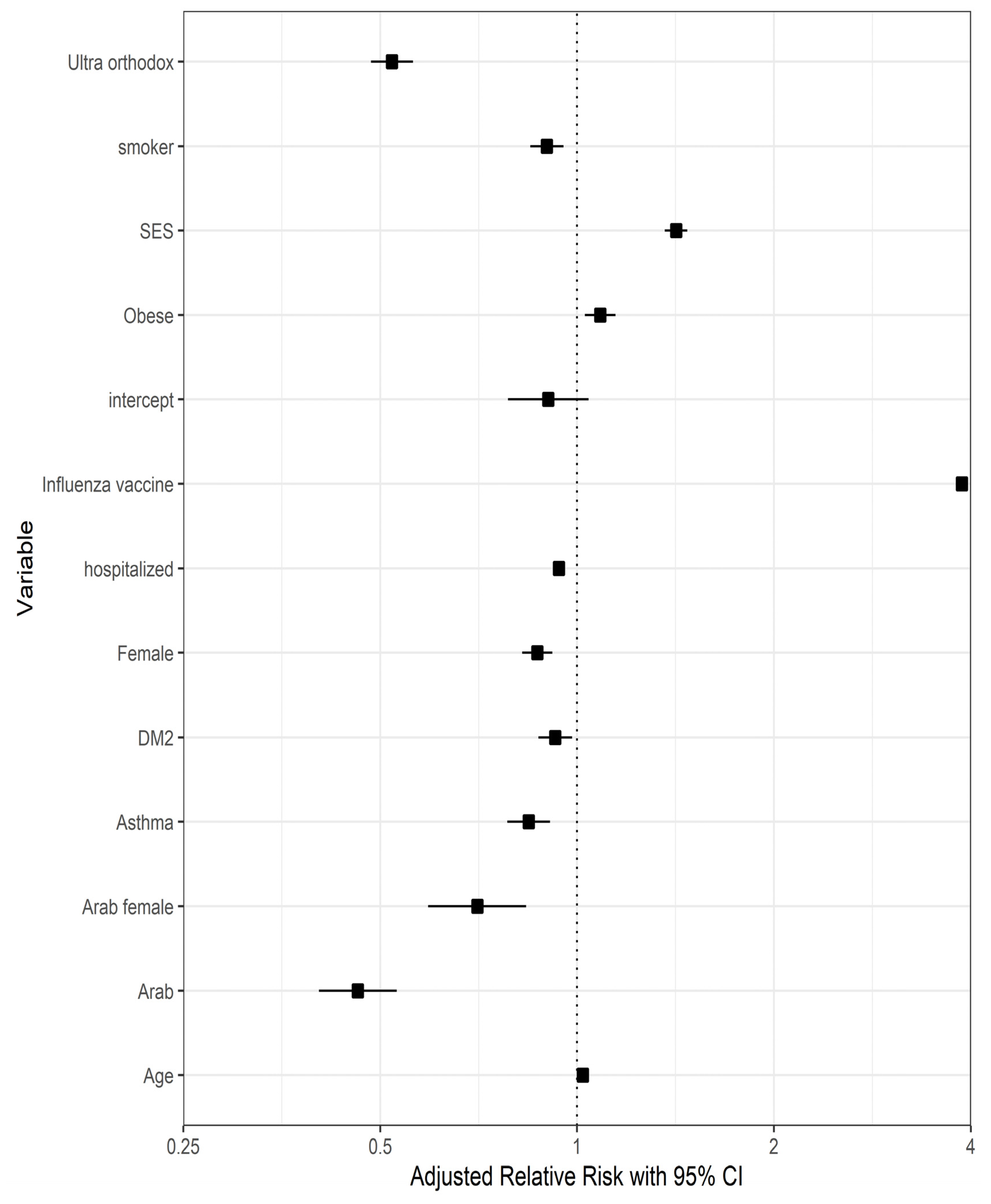
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 25 February 2022).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 April 2022).
- Joshee, S.; Vatti, N.; Chang, C. Long-term effects of COVID-19. Mayo Clin. Proc. 2022, 97, 579–599. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Pfizer Manufacturing Belgium NV. Pfizer-BioNTech COVID-19 Vaccine: Fact Sheet for Healthcare Providers Administering Vaccine (Vaccination Providers). 2021. Available online: http://labeling.pfizer.com/ShowLabeling.aspx?id=16073&format=pdf (accessed on 9 June 2022).
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based COVID-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A.; et al. BNT162b2 vaccine induces neutralizing antibodies and poly-specific T cells in humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- FDA Takes Key Action in Fight against COVID-19 by Issuing Emergency Use Authorization for First COVID-19 Vaccine. News Release of the Food and Drug Administration, Silver Spring, MD. 11 December 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19 (accessed on 30 April 2022).
- World Health Organization. Available online: www.gov.il (accessed on 14 March 2021).
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Central Bureau of Statistics. Available online: https://www.cbs.gov.il/he/pages/default.aspx (accessed on 30 April 2022).
- Chernichovsky, D.; Bisharat, B.; Bowers, L.; Brill, A.; Sharony, C.; Taub Center for Social Policy Studies in Israel. The Health of the Arab Israeli Population. State of the Nation Report. 2017. Available online: https://www.taubcenter.org.il/wp-content/uploads/2020/12/healthofthearabisraelipopulation.pdf (accessed on 30 April 2022).
- Taub Center for Social Policy Studies in Israel. The Singer Series: State of the Nation Report, 2017. The Health of the Arab Israeli Population.pdf. Available online: https://taubcenter.org.il/state-of-the-nation-report-2017/ (accessed on 30 April 2022).
- Rosen, B.; Waitzberg, R.; Israeli, A.; Hartal, M.; Davidovitch, N. Addressing vaccine hesitancy and access barriers to achieve persistent progress in Israel’s COVID-19 vaccination program. Isr. J. Health Policy Res. 2021, 10, 43. [Google Scholar] [CrossRef]
- Cahaner, L.; Malach, G. The Yearbook of Ultraorthodox Society in Israel, 2019. Online. The Israel Democracy Institute. 2019. Available online: https://en.idi.org.il/media/14526/statistical-report-on-ultra-orthodox-haredi-society-in-israel-2019.pdf (accessed on 30 April 2022).
- Romem, A.; Pinchas-Mizrachi, R.; Zalcman, B.G. Utilizing the ACCESS model to understand communication with the ultraorthodox community in Beit Shemesh during the first wave of COVID-19. J. Transcult. Nurs. 2021, 32, 647–654. [Google Scholar] [CrossRef]
- Public Health England. Disparities in the Risk and Outcomes of COVID-19. 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/908434/Disparities_in_the_risk_and_outcomes_of_COVID_August_2020_update.pdf (accessed on 10 March 2022).
- Seligman, B.; Ferranna, M.; Bloom, D.E. Social determinants of mortality from COVID-19: A simulation study using NHANES. PLoS Med. 2021, 18, e1003490. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Goldblatt, P.; Herd, E.; Morrison, J. Build Back Fairer: The COVID-19 Marmot Review. 2020. Available online: https://www.health.org.uk/Publications/Build-Back-Fairer-the-Covid-19-Marmot-Review (accessed on 10 March 2022).
- Saban, M.; Myers, V.; Ben-Shetrit, S.; Wilf-Miron, R. Socioeconomic gradient in COVID-19 vaccination: Evidence from Israel. Int. J. Equity Health 2021, 20, 242. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.E.; Brown, J.; Shahab, L.; Steptoe, A.; Fancourt, D. COVID-19, smoking and inequalities: A study of 53,002 adults in the UK. Tob. Control 2021, 30, e111–e121. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, N.S.; Rossi, N.; El-Sayed Moustafa, J.; Laverty, A.A.; Quint, J.K.; Freidin, M.; Visconti, A.; Murray, B.; Modat, M.; Ourselin, S.; et al. Current smoking and COVID-19 risk: Results from a population symptom app in over 2.4 million people. Thorax 2021, 76, 714–722. [Google Scholar] [CrossRef]
- Ponsford, M.J.; Gkatzionis, A.; Walker, V.M.; Grant, A.J.; Wootton, R.E.; Moore, L.S.P.; Fatumo, S.; Mason, A.M.; Zuber, V.; Willer, C.; et al. Cardiometabolic traits, sepsis, and severe COVID-19: A Mendelian randomization investigation. Circulation 2020, 142, 1791–1793. [Google Scholar] [CrossRef]
- Jiménez-Ruiz, C.A.; López-Padilla, D.; Alonso-Arroyo, A.; Aleixandre-Benavent, R.; Solano-Reina, S.; de Granda-Orive, J.I. COVID-19 and smoking: A systematic review and meta-analysis of the evidence. Arch. Bronconeumol. 2021, 57, 21–34. [Google Scholar] [CrossRef]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1045–1056. [Google Scholar] [CrossRef]
- Gülsen, A.; Yigitbas, B.A.; Uslu, B.; Drömann, D.; Kilinc, O. The effect of smoking on COVID-19 symptom severity: Systematic review and meta-analysis. Pulm. Med. 2020, 2020, 7590207. [Google Scholar] [CrossRef]
- Treskova-Schwarzbach, M.; Haas, L.; Reda, S.; Pilic, A.; Borodova, A.; Karimi, K.; Koch, J.; Nygren, T.; Scholz, S.; Schönfeld, V.; et al. Pre-existing health conditions and severe COVID-19 outcomes: An umbrella review approach and meta-analysis of global evidence. BMC Med. 2021, 19, 212. [Google Scholar] [CrossRef]
- Hanna, J.; Tipparaju, P.; Mulherkar, T.; Lin, E.; Mischley, V.; Kulkarni, R.; Bolton, A.; Byrareddy, S.N.; Jain, P. Risk factors associated with the clinical outcomes of COVID-19 and its variants in the context of cytokine storm and therapeutics/vaccine development challenges. Vaccines 2021, 9, 938. [Google Scholar] [CrossRef]
- Huang, Y.; Lu, Y.; Huang, Y.M.; Wang, M.; Ling, W.; Sui, Y.; Zhao, H.L. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metabolism 2020, 113, 154378. [Google Scholar] [CrossRef]
- Tamara, A.; Tahapary, D.L. Obesity as a predictor for a poor prognosis of COVID-19: A systematic review. Diabetes Metab. Syndr. 2020, 14, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Cao, Y.; Du, T.; Zhi, Y. Prevalence of comorbid asthma and related outcomes in COVID-19: A systematic review and meta-analysis. J. Allergy Clin. Immunol. Pract. 2021, 9, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Xu, J.; Xiao, W.; Wang, Y.; Jin, Y.; Chen, S.; Duan, G.; Yang, H.; Wang, Y. Asthma in patients with coronavirus disease 2019: A systematic review and meta-analysis. Ann. Allergy Asthma Immunol. 2021, 126, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.D.; Heidel, R.E.; Dhand, R. Asthma in adult patients with COVID-19. Prevalence and risk of severe disease. Am. J. Respir. Crit. Care Med. 2021, 203, 893–905. [Google Scholar] [CrossRef]
- Sunjaya, A.P.; Allida, S.M.; Di Tanna, G.L.; Jenkins, C.R. Asthma and COVID-19 risk: A systematic review and meta-analysis. Eur. Respir. J. 2022, 59, 2101209. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Xu, J.; Hou, H.; Yang, H.; Wang, Y. Impact of asthma on COVID-19 mortality in the United States: Evidence based on a meta-analysis. Int. Immunopharmacol. 2022, 102, 108390. [Google Scholar] [CrossRef]
- Gregory, J.M.; Slaughter, J.C.; Duffus, S.H.; Smith, T.J.; LeStourgeon, L.M.; Jaser, S.S.; McCoy, A.B.; Luther, J.M.; Giovannetti, E.R.; Boeder, S.; et al. COVID-19 severity is tripled in the diabetes community: A prospective analysis of the pandemic’s impact in type 1 and type 2 diabetes. Diabetes Care 2021, 44, 526–532. [Google Scholar] [CrossRef]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia: A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr. 2020, 14, 395–403. [Google Scholar] [CrossRef]
- Itelman, E.; Wasserstrum, Y.; Segev, A.; Avaky, C.; Negru, L.; Cohen, D.; Turpashvili, N.; Anani, S.; Zilber, E.; Lasman, N.; et al. Clinical Characterization of 162 COVID-19 patients in Israel: Preliminary report from a large tertiary center. Isr. Med. Assoc. J. 2020, 22, 271–274. [Google Scholar] [PubMed]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Wang, Y.; Dong, H.; Song, C.; Zheng, J.; Li, J.; Li, M.; Wang, J.; Yang, J.; Xu, J. The COVID-19 vaccination behavior and correlates in diabetic patients: A health belief model theory-based cross-sectional study in China, 2021. Vaccines 2022, 10, 659. [Google Scholar] [CrossRef] [PubMed]
- Benis, A.; Seidmann, A.; Ashkenazi, S. Reasons for Taking the COVID-19 Vaccine by US Social Media Users. Vaccines 2021, 9, 315. [Google Scholar] [CrossRef]
- Shah, S.; Gui, H.; Chua, P.E.Y.; Tan, J.B.; Suen, L.K.; Chan, S.W.; Pang, J. Factors associated with COVID-19 vaccination intent in Singapore, Australia and Hong Kong. Vaccine 2022, 40, 2949–2959. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total | Vaccinated (≥1 Dose) N (%) | Unvaccinated N (%) | p-Value |
|---|---|---|---|---|
| Study cohort | 246,543 | 207,911 (84%) | 38,632 (16%) | |
| Age, mean ± SD | 51.6 ± 19.7 | 53.2 ± 19.7 | 42.9 ± 17.3 | |
| Age category, years 20–39 | 84,364 | 63,967 (75.6%) | 20,667 (24.4%) | <0.001 |
| 40–59 | 71,433 | 60,576 (84.8%) | 10,857 (15.2%) | |
| 60–79 | 66,756 | 61,408 (92%) | 5348 (8%) | |
| ≥80 | 23,720 | 21,960 (92.6%) | 1760 (7.4%) | |
| Gender | ||||
| Male | 120,724 | 100,960 (83.6%) | 19,764 (16.4%) | <0.001 |
| Female | 125,819 | 106,961 (85%) | 18,868 (15%) | |
| Sector | ||||
| Non-ultra-Orthodox Jews | 193,035 | 169,259 (87.7%) | 23,766 (12.3%) | <0.001 |
| Ultra-Orthodox Jews | 37,511 | 25,771 (68.7%) | 11,740 (31.3%) | |
| Arabs | 15,997 | 12,881 (80.5%) | 3116 (19.5%) | |
| Socioeconomic status | ||||
| Low | 57,111 | 42,474 (74.4%) | 14,637 (25.6%) | <0.001 |
| Middle | 96,624 | 81,138 (84%) | 15,486 (16%) | |
| High | 92,808 | 84,229 (90.8%) | 8509 (9.2%) | |
| Previous influenza vaccination | ||||
| Vaccinated | 101,429 | 95,834 (94.5%) | 5595 (5.5%) | <0.001 |
| Unvaccinated | 145,114 | 112,077 (77.2%) | 33,037 (22.8%) | |
| Underlying Conditions | Total | Vaccinated (≥1 Dose) N (%) | Unvaccinated N (%) | p-Value |
|---|---|---|---|---|
| Obesity (BMI > 30) | 56,753 | 49,993 (88.1%) | 6760 (11.9%) | <0.001 |
| Diabetes mellitus | 34,877 | 31,722 (91%) | 3155 (9%) | <0.001 |
| Asthma | 19,434 | 16,594 (85.4%) | 2840 (14.6%) | <0.001 |
| COPD | 6619 | 5996 (90.6%) | 623 (9.4%) | <0.001 |
| Cystic fibrosis | 43 | 41 (95.3%) | 2 (4.7%) | 0.0754 |
| Cirrhosis | 707 | 621 (87.8%) | 86 (12.2%) | 0.0119 |
| Smoker | 65,410 | 54,092 (82.7%) | 11,318 (17.3%) | <0.001 |
| Former smoker | 48,134 | 42,245 (87.8%) | 5889 (12.2%) | <0.001 |
| Cardiac disease 1 | 25,065 | 23,164 (92.4%) | 1901 (7.6%) | <0.001 |
| Hypertension | 55,685 | 51,516 (92.5%) | 4169 (7.5%) | <0.001 |
| CVA | 10,803 | 9851 (91.2%) | 952 (8.8%) | <0.001 |
| Malignancy 2 | 22,772 | 20,965 (92.1%) | 1807 (7.9%) | <0.001 |
| Chronic renal failure | 7869 | 7136 (90.7%) | 733 (9.3%) | <0.001 |
| Solid organ transplantation | 8344 | 7900 (94.7%) | 444 (5.3%) | <0.001 |
| Bone marrow transplantation | 318 | 279 (87.7%) | 39 (12.3%) | 0.1108 |
| Down syndrome | 1681 | 1466 (87.2%) | 215 (12.8%) | 0.0013 |
| Hematologic diseases 3 | 57 | 51 (89.5%) | 6 (10.5%) | 0.376 |
| Neurologic diseases 4 | 7753 | 7102 (91.6%) | 651 (8.4%) | <0.001 |
| Depression | 18,813 | 16,466 (87.5%) | 2347 (12.5%) | <0.001 |
| Rheumatologic diseases 5 | 4799 | 4323 (90.1%) | 476 (9.9%) | <0.001 |
| Biological therapy 6 | 1036 | 962 (92.9%) | 74 (7.1%) | <0.001 |
| Steroid therapy 7 | 485 | 439 (90.5%) | 46 (9.5%) | <0.001 |
| Variable | Total | No. of Vaccinations Received | |||
|---|---|---|---|---|---|
| One Dose N (%) | Two Doses N (%) | Three Doses N (%) | p-Value | ||
| Study cohort | 207,911 | 15,715 (7.5%) | 34,242 (16.5%) | 157,954 (76%) | <0.001 |
| Age, mean ± SD | 44.0 ± 19.9 | 36.0 ± 18.6 | 36.1 ± 18.3 | 46.5 ± 19.7 | |
| Age category, years | |||||
| 20–39 | 63,967 | 7547 (11.8%) | 16,183 (25.3%) | 40,237 (62.9%) | <0.001 |
| 40–59 | 60,576 | 4863 (8%) | 10,759 (17.8%) | 44,954 (74.2%) | |
| 60–79 | 61,408 | 2170 (3.5%) | 5178 (8.4%) | 54,060 (88%) | |
| ≥80 | 21,960 | 1135 (5.2%) | 2122 (9.7%) | 18,703 (85.1%) | |
| Gender | |||||
| Male | 100,960 | 7352 (7.3%) | 16,893 (16.7%) | 76,715 (76%) | 0.0098 |
| Female | 106,951 | 8363 (7.8%) | 17,349 (16.2%) | 81,239 (76%) | |
| Sector | |||||
| Non-ultra-Orthodox Jews | 169,259 | 8939 (5.3%) | 23,528 (13.9%) | 136,792 (80.8%) | <0.001 |
| Ultra-Orthodox Jews | 25,771 | 4730 (18.4%) | 6413 (24.9%) | 14,628 (56.7%) | |
| Arabs | 12,881 | 2046 (15.9%) | 4301 (33.4%) | 6534 (50.7%) | |
| Socioeconomic status | |||||
| Low | 42,474 | 6036 (14.2%) | 9867 (23.2%) | 26,571 (62.6%) | <0.001 |
| Middle | 81,138 | 6484 (8%) | 15,137 (18.7%) | 59,517 (73.3%) | |
| High | 84,299 | 3195 (3.8%) | 9238 (11%) | 71,866 (85.2%) | |
| Previous influenza vaccination | |||||
| Vaccinated | 95,836 | 4359 (4.5%) | 9662 (10.1%) | 81,813 (85.4%) | <0.001 |
| Unvaccinated | 112,077 | 11,356 (10.1%) | 24,580 (21.9%) | 76,141 (68%) | |
| Underlying Conditions | Total | Received Only One Vaccine Dose N (%) | Received Two Vaccine Doses N (%) | Received Three Vaccine Doses N (%) | p-Value |
|---|---|---|---|---|---|
| Obesity (BMI > 30) | 49,993 | 3742 (7.5%) | 7020 (14%) | 39,231 (78.5%) | <0.001 |
| Diabetes mellitus | 31,722 | 1761 (5.5%) | 3704 (11.7%) | 26,257 (82.8%) | <0.001 |
| Asthma | 16,594 | 1247 (7.5%) | 2728 (16.4%) | 12,619 (76.1%) | 0.966 |
| COPD | 5996 | 312 (5.2%) | 723 (12.1%) | 4961 (82.7%) | <0.001 |
| Cystic fibrosis | 41 | 4 (9.8%) | 4 (9.8%) | 33 (80.5%) | <0.001 |
| Cirrhosis | 621 | 45 (7.2%) | 80 (12.8%) | 496 (80%) | <0.001 |
| Smoker | 54,092 | 3120 (5.8%) | 9944 (18.4%) | 41,028 (75.8%) | <0.001 |
| Former smoker | 42,245 | 2126 (5%) | 5648 (13.4%) | 34,471 (81.6%) | <0.001 |
| Cardiac disease 1 | 23,164 | 1161 (5%) | 2450 (10.6%) | 19,553 (84.4%) | <0.001 |
| Hypertension | 51,516 | 2408 (4.7%) | 5001 (9.7%) | 44,107 (85.6%) | <0.001 |
| CVA | 9851 | 636 (6.5%) | 1241 (12.6%) | 7974 (80.9%) | <0.001 |
| Malignancy 2 | 20,965 | 906 (4.3%) | 2111 (10.1%) | 17,948 (85.6%) | <0.001 |
| Chronic renal failure | 7136 | 442 (6.2%) | 951 (13.3%) | 5743 (80.5%) | <0.001 |
| Solid organ transplantation | 7900 | 287 (3.6%) | 687 (8.7%) | 6926 (87.7) | <0.001 |
| Bone marrow transplantation | 279 | 13 (4.7%) | 32 (11.4%) | 234 (83.9%) | 0.0081 |
| Down syndrome | 1466 | 92 (6.3%) | 244 (16.6%) | 1130 (77.1%) | <0.001 |
| Hematologic diseases 3 | 51 | 7 (13.7%) | 11 (21.6%) | 33 (64.7%) | <0.001 |
| Neurologic diseases 4 | 7102 | 598 (8.4%) | 1069 (15.1%) | 5435 (76.5%) | <0.001 |
| Depression | 16,466 | 965 (5.9%) | 2270 (13.8%) | 13,231 (80.3%) | <0.001 |
| Rheumatologic diseases 5 | 4323 | 205 (4.7%) | 519 (12%) | 3599 (83.3%) | <0.001 |
| Biological therapy 6 | 962 | 45 (4.7%) | 107 (11.1%) | 810 (84.2%) | <0.001 |
| Steroid therapy 7 | 145 | 23 (15.9%) | 27 (18.6%) | 95 (65.5%) | <0.001 |
| Variable | Odds Ratio | Lower 95% CI | Upper 95% CI | p-Value |
|---|---|---|---|---|
| Age | 1.02 | 1.019 | 1.022 | <0.001 |
| Female | 0.842 | 0.791 | 0.895 | <0.001 |
| Arab | 0.453 | 0.394 | 0.52 | <0.001 |
| Arab female | 0.728 | 0.611 | 0.868 | <0.001 |
| Ultra-Orthodox Jews | 0.484 | 0.438 | 0.536 | <0.001 |
| Ultra-Orthodox female | 1.136 | 1.007 | 1.282 | 0.038 |
| Low SES | 1.418 | 1.363 | 1.475 | <0.001 |
| Previous influenza vaccination | 3.88 | 3.663 | 4.11 | <0.001 |
| Smoking | 0.901 | 0.85 | 0.955 | <0.001 |
| Asthma | 0.843 | 0.782 | 0.909 | <0.001 |
| Diabetes mellitus | 0.926 | 0.873 | 0.983 | 0.011 |
| Obesity | 1.086 | 1.029 | 1.145 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shkalim Zemer, V.; Grossman, Z.; Cohen, H.A.; Hoshen, M.; Gerstein, M.; Yosef, N.; Cohen, M.; Ashkenazi, S. Acceptance Rates of COVID-19 Vaccine Highlight the Need for Targeted Public Health Interventions. Vaccines 2022, 10, 1167. https://doi.org/10.3390/vaccines10081167
Shkalim Zemer V, Grossman Z, Cohen HA, Hoshen M, Gerstein M, Yosef N, Cohen M, Ashkenazi S. Acceptance Rates of COVID-19 Vaccine Highlight the Need for Targeted Public Health Interventions. Vaccines. 2022; 10(8):1167. https://doi.org/10.3390/vaccines10081167
Chicago/Turabian StyleShkalim Zemer, Vered, Zachi Grossman, Herman Avner Cohen, Moshe Hoshen, Maya Gerstein, Noga Yosef, Moriya Cohen, and Shai Ashkenazi. 2022. "Acceptance Rates of COVID-19 Vaccine Highlight the Need for Targeted Public Health Interventions" Vaccines 10, no. 8: 1167. https://doi.org/10.3390/vaccines10081167