
The Fear of Covid-19 Scale (FCV-19S) in Spain: Adaptation and Confirmatory Evidence of Construct and Concurrent Validity


Department of Behavioral Sciences Methodology, University of Valencia, 46010 Valencia, Spain
*
Author to whom correspondence should be addressed.
Mathematics 2021, 9(19), 2512; https://doi.org/10.3390/math9192512
Submission received: 18 August 2021
/
Revised: 1 October 2021
/
Accepted: 3 October 2021
/
Published: 7 October 2021
(This article belongs to the Special Issue Quantitative Methods for Social Sciences)
Abstract
:Fear of the coronavirus has important implications on mental health. In western countries, a significant degree of vaccination has been achieved, but in Spain, less than 75% of the population has received both doses. The current situation is still seen as a threat by many people. Therefore, it is important to have reliable and valid measurement instruments to assess the impact of COVID-19 on the population. In this study, the Fear of COVID-19 Scale has been adapted to Spain, and its psychometric properties have been studied in a Spanish sample using Structural Equation Modeling. This methodology allows obtaining more reliable estimates, regardless of the measurement scale of the variables. The unifactorial structure was confirmed. The correlations with Neuroticism were statistically significant, and the concurrent validity structural equation model yielded good fit indices. However, neither age nor belonging to a risk group directly predict fear of the coronavirus in this sample, but gender and neuroticism are direct predictors. Likewise, neuroticism mediates the relationship between age and fear of COVID-19, and between gender and fear of COVID-19. So being young and being a woman show high scores on neuroticism, leading to their most intense fear of COVID-19. With this reliable and valid measurement instrument, it will be possible to assess the degree of fear of the coronavirus in the Spanish population and improve psychological interventions.
1. Introduction
SARS-CoV-2 is a pathogen that emerged in China in 2019 and soon spread around the world, and the World Health Organization (WHO) declared it a global pandemic in March 2020 [1]. In the case of Spain, on March 14, 2020, a confinement was declared that lasted three months, followed by a slow de-escalation that has led us to a totally different life from the one we knew a little over a year ago, taking into account the changes in the measures and restrictions that are taken according to the evolution of the health alert. The COVID-19 pandemic has sparked fear and anxiety in many people. According to some authors, the current situation is seen as a threat by many people, influencing is decision-making and the feeling of control [2].
We constantly receive a lot of information about the current situation, leading to overexposure to the news since it reaches us from different channels (television, radio, social networks, physical and digital press, etc.). In addition, this information is constantly changing because the knowledge about the disease and its treatments advances according to science and research. Although a significant degree of vaccination has already been achieved in Western countries, at this time in Spain, less than 75% of the population has received both doses and now, with the appearance of the new variants, it is recommended to vaccinate at least 90% of the population with both doses. Furthermore, the vaccination rate has dropped in recent months. Likewise, the possibility of adding a third dose of the vaccine to those who received the first two is being considered, so uncertainty continues to exist in the population. This means that there are still many people with a significant fear of the coronavirus and its consequences, especially after verifying the existence of vaccinated people who have been infected, some of whom have had to go to the hospital due to the severity of their symptoms. All this uncertainty and perception of threat ends up causing anxiety in the population and deteriorates their psychological well-being. This anxiety can manifest itself individually through maladaptive behaviors (social isolation, obsession with disinfection, excessive fear of contagion) or in a more social way, generating mistrust and uncertainty on a large scale [3,4]. The current pandemic, in addition to the global quarantine that took place during 2020, has generated in some people a feeling of social isolation and a feeling of loneliness. These conditions, together with the anxiety generated by uncertainty, have been shown to cause psychiatric and even physical disorders in healthy people, including health professionals [5].
The COVID-19 outbreak and its pandemic nature has caused widespread worry, fear and anxiety, and excessive fear can lead to irrational thoughts [6]. The fear of COVID-19 that some people have can lead to stigmatize and socially exclude some coronavirus patients, people who have survived the disease and their families, and this can lead to the development of mental health problems, such as an adjustment disorder and depression [2,7]. In a study carried out in China at the beginning of 2020, with medical personnel treating patients with coronavirus, it was found that friends and family were able to give emotional support to these personnel, contributing to reduce their anxiety levels [8]. Family and community can serve as a key psychosocial protective factor that provides support in the context of stress and reduces vulnerability to concern about COVID-19. Therefore, people who lived with other family members showed a higher level of concern about COVID-19. Similar results have been found in other studies, in which women suffered a greater psychological impact with the appearance of the coronavirus, showing higher levels of stress and anxiety, among others [9,10,11]. This is likely to occur because women anticipate, to a greater extent than men, the negative impact of the disease both on oneself and on family members or loved ones, especially when it comes to childcare. This fact may be due to the fact that women are more aware of the negative impact of the disease on their own health, and on the health of family and friends. But since childcare continues to fall primarily on women, school and daycare closures have greatly increased childcare needs, especially impacting working mothers.
Regarding personality, it seems that only neuroticism or emotional instability is clearly and positively correlated with perceived stress [12]. These authors found that people with high levels of neuroticism tend to experience emotional imbalances more easily, since this personality trait showed negative correlations with problem-focused coping and positive with emotion-focused coping. In addition to external factors like work, family, and health, certain personality traits can affect the way people live and cope with COVID-19. A study conducted in Germany found that neuroticism was linked to a negative perception of the restrictions imposed by COVID-19, but openness to experience was associated with more positive perceptions of the situation. In a Slovenian study with adults, the authors found that resilience partially or fully mediated relationships between the five major personality traits, but neuroticism was the strongest predictor of less adaptive psychological functioning [13]. Regarding conscientiousness, agreeableness and openness to experience the results are confusing, finding some cases related to less stress and others finding no relationship [13]. Another study carried out with adults in Qatar showed that having a higher level of conscientiousness or neuroticism, being able to perceive risk and routinely implement personal hygiene measures, were good predictors of some social distancing. Gender differences were also found, as women reported a greater commitment to social distancing practices than men [14].
On the other hand, the World Health Organization (WHO), has indicated which are the groups of people with the highest risk of developing severe coronavirus disease. They are elderly people, with cardiovascular diseases and high blood pressure, diabetes, chronic obstructive pulmonary disease, cancer, immunosuppression, pregnancy and other chronic diseases [15,16,17]. In addition, it is considered that people who smoke or those who are obese, also seem to be at higher risk of suffering a serious illness due to the virus. However, the fact of including older people in the list of risk groups is based on the mortality due to the coronavirus, but this does not consider the cultural, social and contextual differences that could have a significant impact, both at physical and at psychological level, of the survivors after the outbreak, and does not take into account the resilience of these people. According to some authors [18] this is a discrimination process based on age-centered stereotypes. This is what is called age discrimination or ageism [19] and it continuous to exist today [20].
However, we have not found studies that evaluate the relationship between belonging to a risk group and fear of the coronavirus. It is reasonable to expect that if a person is at a higher risk of developing more severe symptoms of COVID-19, he/she will be more afraid of the coronavirus. Likewise, one of the variables that is considered a risk factor is advanced age. However, despite the fact that people of advanced chronological age have been the ones who have increased the number of deaths the most, especially at the beginning of the pandemic, in the studies carried out it is the youngest people, even adolescents, who show higher levels of anxiety in the face of the coronavirus.
In a study with parents and children up to 16 years old [7], poor physical health predicted anxiety about COVID-19 rather than fear of the consequences of the illness. This may be due, perhaps, to the fact that people with health problems are at higher risk of being hospitalized or even dying from the coronavirus. Thus, it is expected that they are more afraid of contracting COVID-19 than people without health problems. In addition, in the sample of parents, the authors found that women obtained significantly higher scores than men in anxiety about the disease, perhaps because the responsibility of caring for the children falls more on women. However, also in the adolescent sample, women obtained significantly higher scores than men in anxiety about the consequences of the coronavirus. Likewise, older adolescents also presented greater anxiety about the consequences, probably due to the uncertainties they perceive in their future both at an educational and economic level [21]. Likewise, other studies have analyzed the psychological impact on the uninfected community, revealing psychiatric comorbidities associated with a younger age and greater self-blame [22]. On the other hand, age and time spent focusing on COVID-19 are potential risks for developing psychological problems, and it has been observed that people under 30 years of age are more likely to develop anxiety and fear [23].
Based on what has been observed in different studies, some researchers have emphasized the need to carry out studies on possible prevention strategies to avoid major mental health problems, including suicidal thoughts due to fear of the coronavirus [24]. For this reason, assessment tools are needed to discover the mental health effects of COVID-19, to be able to prevent them. In 2020, the Fear of Covid-19 Scale (FCV-19S) was developed and validated in Iran [6]. These authors developed a short, valid and reliable instrument to assess fear of COVID-19, and it has already been adapted in many countries on different continents, such as Arabia [25], Bangladesh [26], China [27], Japan [28,29], Malaysia [30], Pakistan [31], Israel [32], New Zealand [33], Turkey [34], Ethiopia [35], Mozambique [36], Romania [37], Norway [38], Russia and Belarus [39], Italy [40], Poland [41], Portugal [42], Greece [43], United States [44], Brazil [45], Argentina [46], Perú [47], Cuba [10] o Paraguay [48]. In this study, the Cuban version has been adapted to Spain, and the psychometric properties of this scale are studied in a general sample from a confirmatory perspective using Structural Equation Modeling (SEM). The use of the SEM methodology to study the psychometric properties of the tests allows estimating both the error and the part of the true score contained in the observed scores. If not, psychometric properties (reliability and validity) will be underestimated. When calculated using an SEM, the error part is extracted from these correlations among the variables, which allows a more reliable estimate of them to be obtained. In addition, the SEM methodology allows variables with different measurement levels to be included in the model, which allows more information to be obtained. Finally, it is not necessary to perform an exploratory factor analysis since the structure of one factor has been supported in previous studies.
With this instrument, it will be possible to evaluate the fear of COVID-19 among Spaniards, which will allow one to know the psychological impacts of this disease in order to develop psychological interventions aimed at helping people to face the fear caused by this pandemic.
2. Materials and Methods
2.1. Procedure
Following the standards of the International Test Commission (ITC) [49], the items of the Cuban version of the scale have been adapted to the Spanish used in Spain. In addition to taking gender into account, the wording of item 3 has been slightly modified to be more intelligible in Spain. Items are shown in the Appendix A. The data was collected online through the LimeSurvey platform, an open-source survey tool installed on the University’s servers. The data collection was initiated on 22 February 2021, and closed on 15 April 2021. All respondents had to read and accept the data protection policy before responding. Furthermore, they were informed that the survey was completely voluntary, anonymous, and confidential. No person received money in exchange for responding. The survey was disseminated through personal contacts, who could also forward it to their contacts. On the other hand, the survey was also posted on social networks, where it could also be answered, shared and disseminated.
2.2. Participants
This is a non-probability or accidental sampling. The sample is made up of 397 participants. Among them, 29.5% are men, 7.3% are women, and 0.1% preferred not to indicate it. The participants are between 14 and 68 years of age, with a mean age of 31.16 years (SD = 13.62), distributed as follows: between 14–17 (3%), 18–25 (53.4%), 26–40 (15.6%), 41–55 (22.2%), and over 55 (5.8%). Regarding the level of studies completed, 5.5% have only primary studies or less, 6.8% have compulsory secondary studies, 52.4% have completed high school level, 1.9% have completed a university degree and 13.4% have a postgraduate or doctorate degree. On the other hand, 52.4% of the sample is single, 42.1% are married or have an intimate partner, 4.8% have been divorced and 0.8% are widowed. Regarding main activity, 3.8% are full-time students, 2.9% are students with sporadic or part-time jobs, 37.7% are employed or self-employed, 4.5% are unemployed, 1% are not working nor looking for a job, and 2% is retired.
Regarding the risk group 83.4% of the participants do not belong to any risk group, and 16.6% belong at least to one risk group. Specifically, only 6 people (1.5%) consider themselves to be elderly, 4.3% are people have hypertension or cardiovascular disease, 2% have diabetes, 3.3% have chronic obstructive pulmonary disease, 1.3% have cancer, only one person is pregnant and 4.2% have other chronic diseases. To estimate the structural equation model, the variable risk factor has been considered with these two categories (belong to any risk group or not belong to any risk group).
2.3. Measures
Ten Item Personality Inventory (TIPI) [50]. This scale is made up of 10 items in which each dimension of the Big-Five Questionnaire (Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness) is represented by two descriptors. One represents the positive pole of the dimension and the other represents the negative pole. For example, one item of the factor Extraversion is “Extraverted, enthusiastic”, and the other is “Reserved, quiet”. The items are answered using a Likert-type scale (from 1-strongly disagree to 7-strongly agree). The Spanish version has been used in this study [51].
Fear of COVID-19 Scale (FCV-19S) [6]. This scale is used to measure people’s fear of COVID-19. It has 7 items that are answered with a Likert scale that ranges from 1 (totally disagree) to 5 (totally agree). One example of item in the scale is “I am most afraid of coronavirus-19”. The higher the total score, the greater the fear. The version used in this study is the adaptation to Spain of the Cuban version [10].
2.4. Data Analysis
To confirm the one-factor structure of the questionnaire, a confirmatory factor analysis (CFA) was performed. Because the response scale to the items is ordinal, the Weighted Least Squares with Mean and Variance Adjusted (WLSMV) estimate was used [52]. In addition to χ2, the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), the Root-Mean-Square Error of Approximation (RMSEA), and the Standardized Root-Mean-Square Residual (SRMR) have been used to determine the fit of the model. CFI and TLI values of 0.90 and RMSEA values above 0.06 and below 0.08 are indicative of acceptable model fit [53]. CFI and TLI values of 0.95 or above and RMSEA values below 0.05 are indicative of good empirical fit, and SRMR values close to 0.08 are indicative of good model fit [54,55,56]. The factor measurement reliability [57] was evaluated with the Composite Reliability (CR) [58], which is identical to Omega coefficient [59] because standardized factor loadings have been used [60]. Then, the Average Variance Extracted (AVE) [61] was estimated to evidence factor measurement validity [60]. Values above 0.70 for the AVE are considered good, and values of 0.50 are considered acceptable. For the CR, values above 0.70 are considered good [60]. All values outside this range were considered not acceptable. The corrected item-total polyserial correlations for the items [56,62] have been calculated, as indicators of corrected homogeneity indices for items with ordinal response scales [63,64].
To study the validity of the FCV-19S, the correlations between the total score on the FCV-19S, the two items of the TIPI that measures Neuroticism (since it has been seen in most studies that it is the trait that predicts the highest levels of anxiety), and the variables age, gender, and risk group have been calculated. In addition, a structural equation model was specified considering these variables as direct predictors of fear of COVID-19. On the other hand, and as described above, some current studies indicate that women, especially younger, have shown higher levels of anxiety about the coronavirus, developing fear behaviors to a greater degree in the face of the pandemic. Since the Neuroticism items are indicators of trait anxiety, this factor has also been considered as a mediating variable between the descriptive variables and the total score on the FCV-19S. All these analyses have been carried out using the program Mplus 8.6 [65], taking into account the response scale of variable. To obtain descriptions of the sociodemographic variables, of the items of the FCV-19S and of the items of the TIPI, the IBM SPSS 26 statistical package was used.
3. Results
In Table 1 are shown the descriptive statistics for the items and for the total score of the FCV-19S, the corrected item-total polyserial correlations for the items with their standard errors, and the standardized factor loadings of the CFA. In Table 2 are shown the descriptive statistics for the items of the Ten-Item Personality Inventory.
The one-factor confirmatory factor model of the FCV-19S showed good fit indices (χ2(14) = 115.113, p < 0.001; CFI = 0.970; TLI = 0.955, SRMR = 0.049), except for the RMSEA index (0.135; 90% CI [0.113, 0.158]; PClose value < 0.001). Although the RMSEA and CFI values are inconsistent in this case, this can happen at times. These indices are commonly used to assess model fit, but CFI and RMSEA do not produce comparable qualitative assessments for any data set, as they are calculated differently. RMSEA is a non-standardized fit index, which makes it difficult to interpret, except if it is done using arbitrary cutoffs. But the CFI measures the relative improvement in fit [66]. When RMSEA and CFI offer different assessments of the fit of the model, some authors argue that this does not mean that the model is poorly specified or that there is a problem with the data, but rather that these indices may differ in their interpretation because they assess the fit of the model from different perspectives [67]. Other authors indicate that, compared to the RMSEA, the SRMR, that is a standardized fit index, shows higher power to reject models that present poor fit to the data with ordinal responses (as in this case), regardless of the number of parameters to be estimated and the sample size [68]. Therefore, the fit of the model can be evaluated, in this case, using the SRMR and the CFI. For these reasons, we consider that the one-factor model for the FCV-19S shows a good fit to the data in this sample. All the factor loadings were statistically significant (p < 0.001), ranging from 0.728 to 0.879 (see Table 1). Likewise, the Composite Reliability (CR = 0.954) and the Average Variance Extracted showed very good values (AVE = 0.645). Corrected item-total corrected polyserial correlations (see Table 1) showed very good values too, ranging from 0.642 to 0.779 (SE from 0.019 to 0.036).
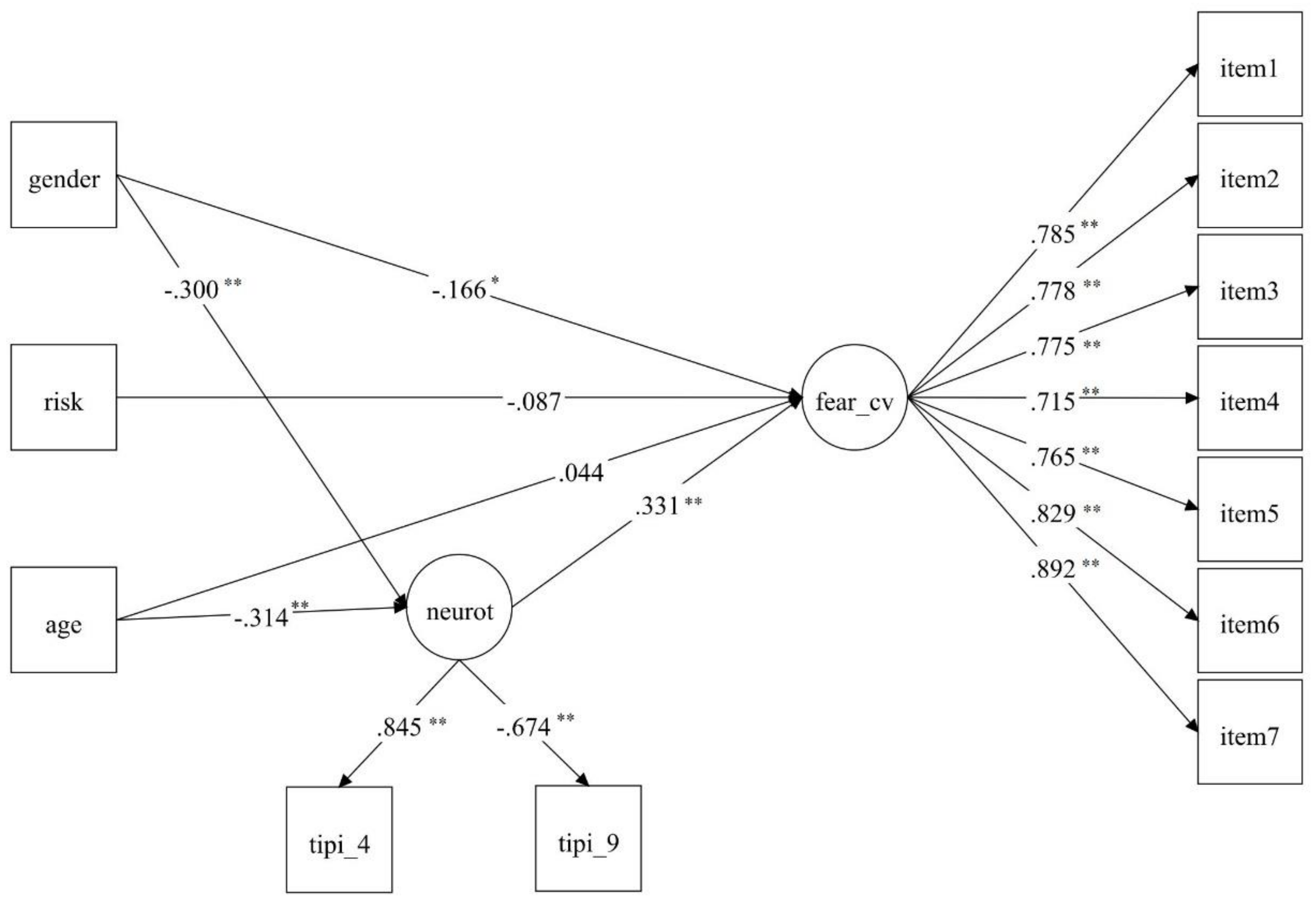
The correlations between the total score of the Fear of Covid-19 scale and the TIPI Neuroticism indicator items have been the following: 0.281 with Tipi_4 (Anxious, easily upset) and -.191 with Tipi_9 (Calm, emotionally stable), and −0.347 with Gender, all of them p < 0.01, an in the expected sense (being a woman correlates with fear of the coronavirus). The correlations between the total score of the Fear of Covid-19 scale with Risk Group (−0.071) and Age (−0.082) were not statistically significant. However, all the descriptive variables (age, gender and risk group) were included in the model to study the mediating effect of neuroticism between these variables and fear of the coronavirus. The fit indices indicated that the model did not fit the data very well: χ2 (50) = 288.678, p < 0.001; CFI = 0.933; TLI = 0.915, RSMEA = 0.110; RMSEA 90% CI = [0.098, 0.122], and SRMR = 0.083. Two high modification indices were observed: Neuroticism on Age (58.022) and Neuroticism on Gender (52.022). It makes sense that both age and gender can be considered predictors of neuroticism, since one of the indicators of this variable is anxiety (item 4: anxious, easily upset). For this reason, the model was re-estimated considering both age and gender as predictors of neuroticism. The new model showed better fit (see Figure 1): χ2 (48) = 184.628, p < 0.001; CFI = 0.961; TLI = 0.949, RSMEA = 0.085; RMSEA 90% CI = [0.072, 0.115], and SRMR = 0.054. Although RMSEA showed a slightly high value, it can be considered for the reasons mentioned above that the model showed good fit to the data.
As can be seen in Figure 1, neither age nor belonging to a risk group directly predict fear of the coronavirus in this sample, but gender does. In this case, being a woman predicts more fear. On the other hand, neuroticism is not only a significant predictor of fear of coronavirus, but also acts as a mediating variable between age and fear of COVID-19, and between gender and fear of COVID-19. In this sample, the variables age and gender are negatively related to neuroticism, which means that younger people are more neurotic, which further leads to their more intense fear of COVID-19. Similarly, women show more neuroticism than men, leading them to feel more intense fear of COVID-19.
4. Discussion
The aim of this study has been to adapt the Cuban version of the Fear of Covid-19 Scale (FCV-19S) to Spain and study its psychometric properties using structural equation modeling. In this Spanish sample, the one-dimensional model obtained good fit indices except for the RMSEA index. However, although the RMSEA turned out to be a high value, sometimes this index shows inconsistent values with the other indices like CFI that, in this case, showed very good values. Therefore, the fit of the model can be evaluated using CFI and SRMR (a standardized fit index), which showed an adequate value. The other indicators of the reliability of the unifactorial model also showed very good values, both the Composite Reliability and the Average Variance Extracted. Likewise, the corrected item-total polyserial correlations showed very good values. Furthermore, all the factor loadings showed high values and were statistically significant.
Likewise, good evidence validity has been obtained. The correlations between the total score of the Fear of Covid-19 scale and the TIPI Neuroticism indicator items are statistically significant and in the expected sense. In other words, people with a higher level of anxiety (a higher degree of neuroticism) tend to have a greater fear of the coronavirus. Regarding gender, women also tend to have higher scores in fear of the coronavirus, as expected by previous studies. Regarding age and belonging to a risk group, they do not show significant correlations with fear of the coronavirus, contrary to expectations. However, when age is introduced into the model and neuroticism is considered as a mediating variable between age and fear of COVID-19, then age is statistically significant. This means that younger people who have high scores on neuroticism predict high scores on fear of the coronavirus. Neuroticism also appears as a mediating variable between gender and fear of the coronavirus. Being a woman seems to lead to more fear of the coronavirus, but if it is also about women with high neuroticism scores, this relationship increases. In addition, this model concludes that people with high neuroticism scores will be direct predictors of a greater fear of COVID-19, a relationship that has been demonstrated in other studies [12,13]. An interesting result is that neuroticism also appears as a mediating variable between age and fear of the coronavirus, and between gender and fear of the coronavirus.
These results are similar to those obtained in other studies that suggest a greater psychological vulnerability associated with COVID-19 in women [9,10,11]. Women suffer a greater psychological impact with the appearance of the coronavirus, showing higher levels of stress and anxiety, among others. This is likely to occur because women anticipate, to a greater extent than men, the negative impact of the disease both on oneself and on family members or loved ones, especially when it comes to childcare. In other studies, it has also been found that younger people show greater anxiety about the coronavirus [7,21]. Although age is not a direct predictor of fear of COVID-19 in our sample, it does present an effect on neuroticism as a mediating variable, so young people with higher scores in neuroticism will be more predictive of fear of COVID-19.
It is also interesting to note that in this sample belonging to a risk group is not a predictor of fear of the coronavirus. This may be because although this is a general sample, non-representative of the Spanish population most of the participants are young people, and old age is considered a significant risk factor. Although there are other risk factors related to other health problems, young people are more likely to have fewer such problems. As the sample of the study is composed mostly of young people, in the future, the psychometric properties of the scale and relationships among the variables of the model should be studied in a more representative sample of the population. Especially, it would be interesting to obtain data from an older sample, which could potentially also have other health problems that would carry a higher risk, and study again whether the variable “belong to a risk group” is a good predictor of fear of the coronavirus. As this study has been conducted with a non-representative sample of the Spanish population, these results should be interpreted with caution and try to replicate and expand this study with a representative sample of the population. There could also be some desirability in the participants’ responses, despite the fact that the survey is completely anonymous, and it is impossible to identify individuals. Men may need to show they are fearless due to gender mandates or other cultural influences. It might perhaps be appropriate in the future to assess the social desirability of people participating in studies on this topic.
5. Conclusions
As has been seen in various studies, the implications that fear of the coronavirus has on mental health are important. In this study, the Cuban version of the FCV-19S has been adapted in a general Spanish sample. The questionnaire has presented good psychometric properties, both in terms of validity and reliability. Having a measurement instrument that allows evaluating the fear of COVID-19 among Spaniards will allow one to better understand the psychological impacts of this disease, and in this way, it will be possible to develop psychological interventions that help people to face the fear caused. for this pandemic.
Author Contributions
Conceptualization, B.E.; methodology, B.E., I.C.; investigation, B.E., I.C.; data curation, B.E.; writing—original draft preparation, B.E., I.C.; writing—review and editing, B.E., I.C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of University of Valencia (protocol code 002, 8 May 2018)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Fear of Covid-19 Scale (Spain)
Por favor, responda las siguientes afirmaciones según su grado de conformidad con ellas, utilizando esta escala de respuesta (a más puntuación más acuerdo):
|
- Siento mucho miedo de la COVID-19
- Me hace sentir incómodo/a pensar acerca de la COVID-19
- Mis manos sudan cuando pienso en la COVID-19
- Tengo miedo a perder mi vida por la COVID-19
- Cuando veo las noticias y escucho historias sobre la COVID-19 en los medios de comunicación me pongo nervioso/a y ansioso/a
- No puedo dormir porque me preocupo por la posibilidad de contagiarme con la COVID-19
- Mi corazón se acelera cuando pienso que puedo contagiarme con la COVID-19
References
- WHO-Media-Briefing. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 13 May 2021).
- Alsukah, A.I.; Algadheeb, N.A.; Almeqren, M.A.; Alharbi, F.S.; Alanazi, R.A.; Alshehri, A.A.; Alsubie, F.N.; Ahajri, R.K. Individuals’ Self-Reactions Toward COVID-19 Pandemic in Relation to the Awareness of the Disease, and Psychological Hardiness in Saudi Arabia. Front. Psychol. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Knolle, F.; Ronan, L.; Murray, G.K. The impact of the COVID-19 pandemic on mental health in the general population: A comparison between Germany and the UK. BMC Psychol. 2021, 9, 60. [Google Scholar] [CrossRef]
- Effati-Daryani, F.; Zarei, S.; Mohammadi, A.; Hemmati, E.; Ghasemi Yngyknd, S.; Mirghafourvand, M. Depression, stress, anxiety and their predictors in Iranian pregnant women during the outbreak of COVID-19. BMC Psychol. 2020, 8, 99. [Google Scholar] [CrossRef]
- Moroianu, L.A.; Moroianu, M.; Toma, A.; Barbu, R.; Ardeleanu, V.; Nitoi, L.C. Psychopathology in Patients Diagnosed with Sars Cov 2: A Brief Report. Mediterr. J. Clin. Psychol. 2021, 9. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McElroy, E.; Patalay, P.; Moltrecht, B.; Shevlin, M.; Shum, A.; Creswell, C.; Waite, P. Demographic and health factors associated with pandemic anxiety in the context of COVID-19. Br. J. Health Psychol. 2020, 25, 934–944. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019(COVID-19) in January and February 2020 in China. Med. Sci. Monit. 2020, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Broche-Pérez, Y.; Fernández-Fleites, Z.; Jiménez-Puig, E.; Fernández-Castillo, E.; Rodríguez-Martin, B.C. Gender and Fear of COVID-19 in a Cuban Population Sample. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Agbaria, Q.; Mokh, A.A. Coping with Stress During the Coronavirus Outbreak: The Contribution of Big Five Personality Traits and Social Support. Int. J. Ment. Health Addict. 2021, 1–19. [Google Scholar] [CrossRef]
- Zager-Kocjan, G.; Kavčič, T.; Avsec, A. Resilience matters: Explaining the association between personality and psychological functioning during the COVID-19 pandemic. Int. J. Clin. Health Psychol. 2021, 21, 100198. [Google Scholar] [CrossRef]
- Abdelrahman, M. Personality Traits, Risk Perception, and Protective Behaviors of Arab Residents of Qatar During the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 13 May 2021).
- Risk Groups. Available online: https://www.phe.gov/s3/BioriskManagement/biosafety/Pages/Risk-Groups.aspx (accessed on 13 May 2021).
- Ministerio de Sanidad. Información Científica-Técnica COVID-19 en Distintos Entornos y Grupos de Personas. Ministerio de Sanidad: Madrid, Spain, 2021. [Google Scholar]
- Rahman, A.; Jahan, Y. Defining a ‘Risk Group’ and Ageism in the Era of COVID-19. J. Loss Trauma 2020, 25, 631–634. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.N. Why Survive? Being Old in America; Harper & Row: Oxford, UK, 1975. [Google Scholar]
- Sousa-São José, J.M.; Filipe-Amado, C.A.; Ilinca, S.; Buttigieg, S.C.; Taghizadeh-Larsson, A. Ageism in Health Care: A Systematic Review of Operational Definitions and Inductive Conceptualizations. Gerontologist 2019, 59, E98–E108. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Ahmed, N.; Pissarides, C.; Stiglitz, J. Why inequality could spread COVID-19. Lancet Public Health 2020, 5, e240. [Google Scholar] [CrossRef]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. Qjm Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatry 2020, 51, 102073. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 22–30. [Google Scholar] [CrossRef]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, M.A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric Validation of the Bangla Fear of COVID-19 Scale: Confirmatory Factor Analysis and Rasch Analysis. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Chen, S.; Chen, Y.; Chen, D.; Yu, Q.; Guo, T.; Cao, Q.; Zheng, X.; Huang, S.; Hossain, M.M.; et al. Psychometric Evaluation of the Fear of COVID-19 Scale Among Chinese Population. Int. J. Ment. Health Addict. 2021, 1–16. [Google Scholar] [CrossRef]
- Masuyama, A.; Shinkawa, H.; Kubo, T. Validation and Psychometric Properties of the Japanese Version of the Fear of COVID-19 Scale Among Adolescents. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wakashima, K.; Asai, K.; Kobayashi, D.; Koiwa, K.; Kamoshida, S.; Sakuraba, M. The Japanese version of the Fear of COVID-19 scale: Reliability, validity, and relation to coping behavior. PLoS ONE 2020, 15, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pang, N.T.P.; Kamu, A.; Hambali, N.L.B.; Mun, H.C.; Kassim, M.A.; Mohamed, N.H.; Ayu, F.; Rahim, S.S.S.A.; Omar, A.; Jeffree, M.S. Malay Version of the Fear of COVID-19 Scale: Validity and Reliability. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Mahmood, Q.K.; Jafree, S.R.; Qureshi, W.A. The Psychometric Validation of FCV19S in Urdu and Socio-Demographic Association with Fear in the People of the Khyber Pakhtunkhwa (KPK) Province in Pakistan. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Winter, T.; Riordan, B.C.; Pakpour, A.H.; Griffiths, M.D.; Mason, A.; Poulgrain, J.W.; Scarf, D. Evaluation of the English Version of the Fear of COVID-19 Scale and Its Relationship with Behavior Change and Political Beliefs. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its Association with Psychological Distress and Life Satisfaction in Turkey. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Elemo, A.S.; Satici, S.A.; Griffiths, M.D. The Fear of COVID-19 Scale: Psychometric Properties of the Ethiopian Amharic Version. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Formighieri-Giordani, R.C.; Giolo, S.R.; Muhl, C.; Estavela, A.J.; Mabuie-Gove, J.I. Validation of the FCV-19 scale and assessment of fear of COVID-19 in the population of Mozambique, East Africa. Psychol. Res. Behav. Manag. 2021, 14, 345–354. [Google Scholar] [CrossRef]
- Stănculescu, E. Fear of COVID-19 in Romania: Validation of the Romanian Version of the Fear of COVID-19 Scale Using Graded Response Model Analysis. Int. J. Ment. Health Addict. 2021. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.M.; Norekvål, T.M.; Oterhals, K.; Fadnes, L.T.; Mæland, S.; Pakpour, A.H.; Breivik, K. Psychometric Properties of the Norwegian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2021. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 Fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Clari, M.; Arese, S.; Bandini, B.; Cavallaro, L.; Mozzone, S.; Vellone, E.; Frigerio, S.; Campagna, S. Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. Spinal Cord 2020, 58, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Pilch, I.; Kurasz, Z.; Turska-kawa, A. Experiencing fear during the pandemic. The Polish version of the Fear of Covid-19 Scale. PeerJ. 2020, 9. [Google Scholar] [CrossRef]
- Magano, J.; Vidal, D.; Sousa, H.; Pimienta, M. Leite  Validation and Psychometric Fear of COVID-19 Scale (FCV-19S) and Associations with Travel, Tourism and Hospitality. Int. J. Environ. Res. Public Health 2021, 18, 427. [Google Scholar] [CrossRef]
- Tsipropoulou, V.; Nikopoulou, V.A.; Holeva, V.; Nasika, Z.; Diakogiannis, I.; Sakka, S.; Kostikidou, S.; Varvara, C.; Spyridopoulou, E.; Parlapani, E. Psychometric Properties of the Greek Version of FCV-19S. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Perz, C.A.; Lang, B.A.; Harrington, R. Validation of the Fear of COVID-19 Scale in a US College Sample. Int. J. Ment. Health Addict. 2020, 1–11. [Google Scholar] [CrossRef]
- Cavalheiro, F.R.S.; Sticca, M.G. Adaptation and Validation of the Brazilian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Furman, H.; Griffiths, M.D.; Pakpour, A.H.; Simkin, H. Evidencias de Validez de la Escala de Miedo al COVID-19 (FCV-19S) en el contexto argentino. Psocial 2020, 6, 99–110. [Google Scholar]
- Caycho-Rodríguez, T.; Tomás, J.M.; Barboza-Palomino, M.; Ventura-León, J.; Gallegos, M.; Reyes-Bossio, M.; Vilca, L.W. Assessment of Fear of COVID-19 in Older Adults: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2021. [Google Scholar] [CrossRef]
- Barrios, I.; Rios-Gonzalez, C.; O’Higgins, M.; Gonzalez-Urbieta, I.; Garcia, O.; Almiron-Santacruz, J.; Navarro, R.; Melgarejo, O.; Ruiz Diaz, N.; Castaldelli-Maia, J.M.; et al. Psychometric properties of the Spanish version of the Fear of COVID-19 Scale in Paraguayan population. Ir. J. Psychol. Med. 2021. [Google Scholar] [CrossRef]
- Muñiz, J.; Elosúa, P.; Padilla, J.L.; Hambleton, R.K. Test adaptation standards for cross-lingual assessment. In Educational Measurement from Foundations to Future; Wells, C.S., Faulkner-Bond, M., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 291–304. [Google Scholar]
- Gosling, S.D.; Rentfrow, P.J.; Swann, W.B., Jr. A very brief measure of the Big-Five personality domains. J. Res. Personal. 2003, 37, 504–528. [Google Scholar] [CrossRef]
- Romero, E.; Villar, P.; Gómez-Fraguela, J.A.; López-Romero, L. Measuring personality traits with ultra-short scales: A study of the Ten Item Personality Inventory (TIPI) in a Spanish sample. Personal. Individ. Differ. 2012, 53, 289–293. [Google Scholar] [CrossRef]
- Finney, S.J.; DiStefano, C. Nonnormal and categorical data in structural equation modeling. In Structural Equation Modeling: A Second Course, 2nd ed.; Hancock, G.R., Mueller, R.O., Eds.; IAP Information Age Publishing: Charlotte, NC, USA, 2013; pp. 269–314. ISBN 9781623962449. [Google Scholar]
- Greiff, S.; Heene, M. Why Psychological Assessment Needs to Start Worrying About Model Fit. Eur. J. Psychol. Assess. 2017, 33, 313–317. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Evaluating model fit. In Structural Equation Modeling: Concepts, Issues, and Applications; Hoyle, R.H., Ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1995; Chapter xxii; p. 99. 289p. [Google Scholar]
- Marsh, H.W.; Balla, J.R.; Hau, K.-T. An evaluation of incremental fit indices: A clarification of mathematical and empirical properties. In Advanced Structural Equation Modeling: Issues and Techniques; Marcoulides, G.A., Schumacker, R.E., Eds.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1996; pp. 315–353. [Google Scholar]
- Raykov, T.; Marcoulides, G.A. A Direct Latent Variable Modeling Based Method for Point and Interval Estimation of Coefficient Alpha. Educ. Psychol. Meas. 2015, 75, 146–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Werts, C.E.; Linn, R.L.; Jöreskog, K.G. Intraclass Reliability Estimates: Testing Structural Assumptions. Educ. Psychol. Meas. 1974, 34, 25–33. [Google Scholar] [CrossRef]
- McDonald, R.P. Test Theory: A Unified Treatment; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999. [Google Scholar]
- Raykov, T. Estimation of composite reliability for congeneric measures. Appl. Psychol. Meas. 1997, 21, 173–184. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Raykov, T.; Marcoulides, G.A. Introduction to Psychometric Theory; Routledge Ltd: New York, NY, USA, 2011; ISBN 0415878225. [Google Scholar]
- Jöreskog, K.G. On the estimation of polychoric correlations and their asymptotic covariance matrix. Psychometrika 1994, 59, 381–389. [Google Scholar] [CrossRef]
- Muthén, B. A general structural equation model with dichotomous, ordered categorical, and continuous latent variable indicators. Psychometrika 1984, 49, 115–132. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Shi, D.; Lee, T.; Maydeu-Olivares, A. Understanding the Model Size Effect on SEM Fit Indices. Educ. Psychol. Meas. 2019, 79, 310–334. [Google Scholar] [CrossRef]
- Lai, K.; Green, S.B. The Problem with Having Two Watches: Assessment of Fit When RMSEA and CFI Disagree. Multivar. Behav. Res. 2016, 51, 220–239. [Google Scholar] [CrossRef]
- Shi, D.; Maydeu-Olivares, A.; Rosseel, Y. Assessing Fit in Ordinal Factor Analysis Models: SRMR vs. RMSEA. Struct. Equ. Modeling 2020, 27, 1–15. [Google Scholar] [CrossRef]
Figure 1.
Structural equation model with standardized factor loadings. Reference group for gender: Male. Reference group for risk: Not belong to any risk group. Note: risk = risk group; neurot = Neuroticism; fear_cv = Fear of Covid-19; tipi_4 = anxious, easily upset; tipi_9 = calm, emotionally stable. * p < 0.002; ** p < 0.001.
Figure 1.
Structural equation model with standardized factor loadings. Reference group for gender: Male. Reference group for risk: Not belong to any risk group. Note: risk = risk group; neurot = Neuroticism; fear_cv = Fear of Covid-19; tipi_4 = anxious, easily upset; tipi_9 = calm, emotionally stable. * p < 0.002; ** p < 0.001.


{kind=link}
Table 1.
Descriptive statistics for the items on the Fear of Covid-19 Scale and for the total score on the scale, corrected item-total polyserial correlations with standard errors (SE), and standardized factor loadings of the confirmatory factor analysis.
Table 1.
Descriptive statistics for the items on the Fear of Covid-19 Scale and for the total score on the scale, corrected item-total polyserial correlations with standard errors (SE), and standardized factor loadings of the confirmatory factor analysis.
| Mean | Standard Deviation | Skewness | Kurtosis | Corrected Item-Total Correlation | SE for the Corrected ITEM-Total Correlation | Standardized Loadings | |
|---|---|---|---|---|---|---|---|
| Item 1 | 2.66 | 1.14 | 0.069 | −0.801 | 0.717 | 0.019 | 0.800 |
| Item 2 | 2.97 | 1.26 | −0.026 | −1.06 | 0.685 | 0.023 | 0.775 |
| Item 3 | 1.41 | 0.749 | 2.12 | 4.95 | 0.642 | 0.036 | 0.769 |
| Item 4 | 2.45 | 1.34 | 0.481 | −1.02 | 0.659 | .024 | 0.728 |
| Item 5 | 2.85 | 1.29 | −0.028 | −1.18 | 0.682 | .022 | 0.753 |
| Item 6 | 1.46 | 0.773 | 1.81 | 3.14 | 0.687 | .032 | 0.818 |
| Item 7 | 1.83 | 1.15 | 1.16 | 0.243 | 0.779 | .022 | 0.879 |
| Total score | 15.92 | 5.78 | 0.592 | −0.153 |
Table 2.
Descriptive statistics for the items on the Ten Item Personality Inventory (TIPI).
| Mean | Standard Deviation | Skewness | Kurtosis | |
|---|---|---|---|---|
| TIPI1 (Extraversion) Extraverted, enthusiastic | 4.76 | 1.809 | −0.609 | −0.742 |
| TIPI2 (Agreeableness) Critical, quarrelsome | 2.93 | 1.787 | 0.583 | −0.806 |
| TIPI3 (Conscientiousness) Dependable, self-disciplined | 5.90 | 1.292 | −1.418 | 1.888 |
| TIPI4 (Emotional Stability) Anxious, easily upset | 3.94 | 1.884 | −0.009 | −1.215 |
| TIPI5 (Openness) Open to new experiences, complex | 5.49 | 1.388 | −0.961 | 0.626 |
| TIPI6 (Extraversion) Reserved, quiet | 4.07 | 2.088 | −0.106 | −1.393 |
| TIPI7 (Agreeableness) Sympathetic, warm | 6.21 | 0.900 | −1.417 | 3.487 |
| TIPI8 (Conscientiousness) Disorganized, careless | 3.27 | 1.976 | 0.328 | −1.264 |
| TIPI9 (Emotional Stability) Calm, emotionally stable | 4.62 | 1.777 | −.547 | −0.665 |
| TIPI10 (Openness) Conventional, uncreative | 2.98 | 1.776 | 0.630 | −0.754 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Espejo, B.; Checa, I. The Fear of Covid-19 Scale (FCV-19S) in Spain: Adaptation and Confirmatory Evidence of Construct and Concurrent Validity. Mathematics 2021, 9, 2512. https://doi.org/10.3390/math9192512
AMA Style
Espejo B, Checa I. The Fear of Covid-19 Scale (FCV-19S) in Spain: Adaptation and Confirmatory Evidence of Construct and Concurrent Validity. Mathematics. 2021; 9(19):2512. https://doi.org/10.3390/math9192512
Chicago/Turabian StyleEspejo, Begoña, and Irene Checa. 2021. "The Fear of Covid-19 Scale (FCV-19S) in Spain: Adaptation and Confirmatory Evidence of Construct and Concurrent Validity" Mathematics 9, no. 19: 2512. https://doi.org/10.3390/math9192512
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.