
Opinion and Sentiment Analysis of Palliative Care in the Era of COVID-19
 , , ,
, , ,
Abstract
:1. Key Message
2. Introduction
Palliative Care during COVID-19 Pandemic
3. Methods
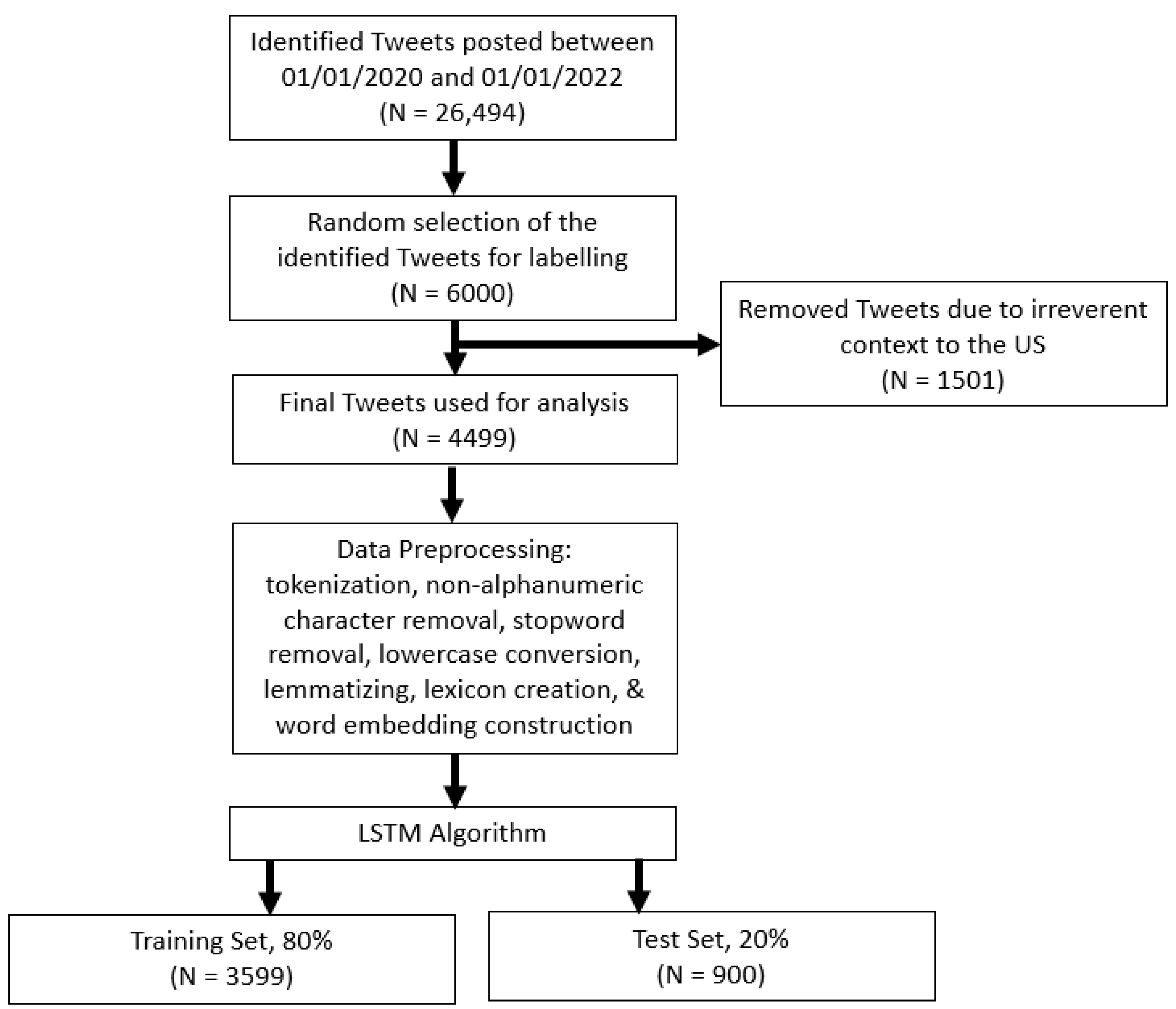
3.1. Tweet Collection and Filtering Based on Time, Keywords, and Location
3.2. Natural Language Processing to Create Word Embeddings, or Feature Vectors
3.3. LSTM Classification
4. Results
4.1. Theme Distributions of Manually Classified Data
4.2. Word Importance and Representative Tweets
4.2.1. Negative Impact of the Pandemic on Palliative Care
- (1)
- doctors and nurses are dealing hostility and threats from patients upset over hospital safety rules due to the #COVID19 pandemic. @kenceemd, hospitalist & palliative care physician, discusses her experience at #uofuhealth
- (2)
- such an emotionally draining week on placement, so many palliative cancer patients who were diagnosed late or had their surgery/chemo dates pushed back due to COVID
- (3)
- shortage of palliative care in usa could amplify suffering for coronavirus patients https://t.co/5nzcggqzie (accessed on 29 January 2023) via @usatoday
4.2.2. Positive Impact of the Pandemic on Palliative Care
- (1)
- long-haul #COVID renews push to expand #palliativecare
- (2)
- #telemedicine—it is saved so many chronically ill people from risking COVID to see their drs. it is also saves time & money—for me, it is often a 3 h one way drive to see my palliative care doctor. it is #somethingpositiveabout2020 that i hope will continue long after COVID
- (3)
- coronavirus may push more home health providers into palliative care
4.2.3. Recognized Benefits of Palliative Care
- (1)
- palliative care meets emotional needs during COVID-19
- (2)
- the demand for palliative care has grown substantially during the pandemic. our director of palliative care rhonda gaugh, do explains what palliative care is and how it helps COVID patients.
- (3)
- palliative care is an essential service to relieve pain and suffering related to COVID-19 and pre-existing health conditions
- (4)
- palliative care puts compassion into the COVID crisis, it adds the humanization, it put the patient in the center of the crisis and not other issues
4.2.4. Myths of Palliative Care
- (1)
- i wish hospitals would refuse to treat non vaccinated COVID patient, palliative care only or ivermectin/hydroxychloroquine if they like. why are we bothering with people who have chosen to become infected and suffer adverse results?
- (2)
- at this point when you ask a newly admitted patient if they have been vaxxed for COVID and they say “no”, just offer them palliative care and send them home.
- (3)
- “theoretically, a 90-year-old cancer patient already on palliative care could die but have coronavirus in their system at the time of death that could be recorded as a coronavirus death.”
4.2.5. Unrelated
- (1)
- Advertisement of webinars, YouTube videos, or journal articles, e.g., “today’s palliative care discussion series features guest xxx” or “visit the capc youtube channel for the latest videos on palliative care messaging…”
- (2)
- Palliative care was mentioned but not as its main point or focus, i.e., “over the past week my mother almost died from COVID. she was unvaccinated. she was hospitalized and didn’t want to be intubated, but managed to pull through and her oxygen levels rose, she’d planned to go palliative care. now she’ll live. please get the vaccine” or “trump touted hydroxychloroquine as a preventative treatment. the report states it was only helpful in severe cases when patients were on ventilators. so not preventive, palliative!”
- (3)
- Opinions or perceptions that are not uniquely associated with palliative care, i.e., opinions that are commonly shared in the settings other than palliative care, including “i work in a long term facility in the dementia and palliative care unit. we are COVID free but in full ppe gear every day because co-workers refused to get vaccinated. i am so disgusted”
4.3. Model Performance of LSTM
5. Discussion
“no one is trying to ‘cure’ me. i’m afraid to go to the hospital if i get sick or hurt right now because, my chart has been labeled, by the drs, as ‘palliative care’. not usually an issue, but now may be. the COVID death numbers are wrong, not counting all”.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- One input layer, which receives the vectorized words of the Tweet.
- One hidden layer, also referred to as a memory cell, with 256 nodes and a dropout rate of 0.3, with a rectified linear unit (ReLU) activation function. The 0.3 dropout rate means that 30% of nodes in this layer will be ignored during each training epoch. This improves the network’s stability by increasing resistance to noise in the data. This layer produces a hidden state at every time step.
- One dense layer with 256 nodes and a dropout rate of 0.3. This layer receives the hidden state generated by the memory cell and produces a class label.
- One output layer with a SoftMax activation function, which produces a probability distribution over the classes. The SoftMax function, softmax(zi) = exp(zi)/Ʃj exp(zj), used in the final layer, transforms the values (zi) to normalized exponential probabilities whose summation is one (i.e., Ʃi pi = 1). There are as many units in the output layer as there are classes. Each class is locally represented by a binary target vector with one non-zero component.
- The cross-entropy cost function, applied in the network, is calculated as—Ʃc yc log(pc), where c represents a neuron (or class) in the output layer, yc represents the desired value (0 or 1) at that class, and pc is the predicted probability at that class. The network is trained using the Adam optimization algorithm [22], which is an extension to the stochastic gradient descent (SGD) approach, with a batch size of 256. In other words, at each training epoch, only 256 training samples were used. Unlike SGD, which maintains a single and fixed learning rate for all synaptic weight updates, Adam continually adjusts individual adaptive learning rates for each synaptic weight based on estimates of the first and second moments of the gradients. A five-epoch rule is applied to stop the training, i.e., the training is stopped if the validation accuracy does not improve for five consecutive epochs and the most accurate version of the model is stored. The validation accuracy is the percentage of validation Tweets (i.e., Tweets that have not been used for training) that are correctly classified.
References
- Radbruch, L.; De Lima, L.; Knaul, F.; Wenk, R.; Ali, Z.; Bhatnaghar, S.; Blanchard, C.; Bruera, E.; Buitrago, R.; Burla, C.; et al. Redefining Palliative Care—A New Consensus-Based Definition. J. Pain Symptom Manag. 2020, 60, 754–764. [Google Scholar] [CrossRef]
- Powell, V.D.; Silveira, M.J. Palliative Care for Older Adults with Multimorbidity in the Time of COVID 19. J. Aging Soc. Policy 2021, 33, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Heller, I.W.; Schaefer, N.; Salloum, R.G.; Kittelson, S.M.; Wilkie, D.J.; Huo, J. The health care cost of palliative care for cancer patients: A systematic review. Support. Care Cancer 2020, 28, 4561–4573. [Google Scholar] [CrossRef]
- May, P.; Garrido, M.M.; Cassel, J.B.; Kelley, A.S.; Meier, E.D.; Normand, C.; Smith, T.; Morrison, R.S. Cost analysis of a prospective multi-site cohort study of palliative care consultation teams for adults with advanced cancer: Where do cost-savings come from? Palliat. Med. 2017, 31, 378–386. [Google Scholar] [CrossRef]
- Evans, A.M.; Jonas, M.; Lantos, J. Pediatric Palliative Care in a Pandemic: Role Obligations, Moral Distress, and the Care You Can Give. Pediatrics 2020, 146, e20201163. [Google Scholar] [CrossRef]
- Scibetta, C.; Kerr, K.; McGuire, J.; Rabow, M.W. The Costs of Waiting: Implications of the Timing of Palliative Care Consultation among a Cohort of Decedents at a Comprehensive Cancer Center. J. Palliat. Med. 2016, 19, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Parajuli, J.; Tark, A.; Jao, Y.-L.; Hupcey, J. Barriers to palliative and hospice care utilization in older adults with cancer: A systematic review. J. Geriatr. Oncol. 2020, 11, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Taber, J.M.; Ellis, E.M.; Reblin, M.; Ellington, L.; Ferrer, R.A. Knowledge of and beliefs about palliative care in a nationally-representative U.S. sample. PLoS ONE 2019, 14, e0219074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flieger, S.P.; Chui, K.; Koch-Weser, S. Lack of Awareness and Common Misconceptions About Palliative Care Among Adults: Insights from a National Survey. J. Gen. Intern. Med. 2020, 35, 2059–2064. [Google Scholar] [CrossRef]
- Mallon, A.; Slater, P.; Hasson, F.; Casson, K.; McIlfatrick, S. What do young adults know about palliative care? A cross-sectional survey. Public Health 2021, 191, 78–84. [Google Scholar] [CrossRef]
- Radbruch, L.; Knaul, F.M.; de Lima, L.; de Joncheere, C.; Bhadelia, A. The key role of palliative care in response to the COVID-19 tsunami of suffering. Lancet 2020, 395, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.; Boundy, E.; Bowen, V.; Chow, N.; Cohn, A.; Dowling, N.; Ellington, S.; Gierke, R.; Hall, A.; MacNeil, J.; et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12–March 16, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef]
- Abbas, S.Q. P-46 Barriers towards providing effective spiritual care to palliative care patients. BMJ Support. Palliat. Care 2021, 11, A25–A26. [Google Scholar] [CrossRef]
- Wu, M.-P.; Tsao, L.-I.; Huang, S.-J.; Liu, C.-Y. Development of the Readiness for Home-Based Palliative Care Scale (RHBPCS) for Primary Family Caregivers. Healthcare 2021, 9, 608. [Google Scholar] [CrossRef] [PubMed]
- Rostampour, S.; Cleveland, T.; White, H.; Haslam, P.; McCafferty, I.; Hamady, M. Response of UK interventional radiologists to the COVID-19 pandemic—Survey findings. CVIR Endovasc. 2020, 3, 41. [Google Scholar] [CrossRef] [PubMed]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Powers, D.M.W. Evaluation: From Precision, Recall and F-Measure to ROC, Informedness, Markedness & Correlation. J. Mach. Learn. Technol. 2011, 2, 37–63. [Google Scholar]
- Dunleavy, L.; Preston, N.; Bajwah, S.; Bradshaw, A.; Cripps, R.; Fraser, L.K.; Maddocks, M.; Hocaoglu, M.; Murtagh, F.E.; Oluyase, O.A.; et al. ‘Necessity is the mother of invention’: Specialist palliative care service innovation and practice change in response to COVID-19. Results from a multinational survey (CovPall). Palliat. Med. 2021, 35, 814–829. [Google Scholar] [CrossRef]
- Tang, M.; Reddy, A. Telemedicine and Its Past, Present, and Future Roles in Providing Palliative Care to Advanced Cancer Patients. Cancers 2022, 14, 1884. [Google Scholar] [CrossRef]
- Thomas, J.D.; Leiter, R.E.; Abrahm, J.L.; Shameklis, J.C.; Kiser, S.B.; Gelfand, S.L.; Sciacca, K.R.; Reville, B.; Siegert, C.A.; Zhang, H.; et al. Development of a Palliative Care Toolkit for the COVID-19 Pandemic. J. Pain Symptom Manag. 2020, 60, e22–e25. [Google Scholar] [CrossRef]
- Hoerger, M.; Perry, L.M.; Korotkin, B.D.; Walsh, L.E.; Kazan, A.S.; Rogers, J.L.; Atiya, W.; Malhotra, S.; Gerhart, J.I. Statewide Differences in Personality Associated with Geographic Disparities in Access to Palliative Care: Findings on Openness. J. Palliat. Med. 2019, 22, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar] [CrossRef]


{kind=link}
| Theme | Definition |
|---|---|
| Recognized Benefits of Palliative Care | Tweets acknowledge the importance or value of palliative care. |
| Positive Impact of the Pandemic on Palliative Care | Tweets state that something good happened or resulted from palliative care because of the pandemic, such as increasing recognition of palliative care in public and the development of toolkits to care for patients. |
| Negative Impact of the Pandemic on Palliative Care | Tweets voice concerns and difficulties in caring for palliative care patients, such as having overwhelmed medical staff, keeping patients isolated from their family members, and facing challenges to provide appropriate and timely treatment for palliative care patients. |
| Myths of Palliative Care | Tweets include misinformation and misconceptions, such as implying that palliative care means not providing appropriate treatment. |
| Theme | N | % |
|---|---|---|
| Negative Impact of the Pandemic on Palliative Care | 350 | 7.8 |
| Positive Impact of the Pandemic on Palliative Care | 254 | 5.6 |
| Recognized Benefits of Palliative Care | 329 | 7.3 |
| Myths of Palliative Care | 21 | 0.5 |
| Unrelated Tweets | 3631 | 80.7 |
| Outcome Variables/Theme | # of Test Samples | Size of the Positive (Class 1) | Size of the Negative (Class 0) | Recall | Precision | F1 Score |
|---|---|---|---|---|---|---|
| Negative Impact of the Pandemic | 900 | 70 | 830 | 0.97 | 0.95 | 0.96 |
| Positive Impact of the Pandemic | 900 | 51 | 849 | 0.41 | 0.68 | 0.51 |
| Recognized Benefits of Palliative Care | 900 | 66 | 834 | 0.27 | 0.55 | 0.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, M.; Li, M.-H.; Hashemi, M.; Yu, Y.; Jonnalagadda, J.; Kulkarni, R.; Kestenbaum, M.; Mohess, D.; Koizumi, N. Opinion and Sentiment Analysis of Palliative Care in the Era of COVID-19. Healthcare 2023, 11, 855. https://doi.org/10.3390/healthcare11060855
Inoue M, Li M-H, Hashemi M, Yu Y, Jonnalagadda J, Kulkarni R, Kestenbaum M, Mohess D, Koizumi N. Opinion and Sentiment Analysis of Palliative Care in the Era of COVID-19. Healthcare. 2023; 11(6):855. https://doi.org/10.3390/healthcare11060855
Chicago/Turabian StyleInoue, Megumi, Meng-Hao Li, Mahdi Hashemi, Yang Yu, Jahnavi Jonnalagadda, Rajendra Kulkarni, Matthew Kestenbaum, Denise Mohess, and Naoru Koizumi. 2023. "Opinion and Sentiment Analysis of Palliative Care in the Era of COVID-19" Healthcare 11, no. 6: 855. https://doi.org/10.3390/healthcare11060855