
How Did COVID-19 Affect Suicidality? Data from a Multicentric Study in Lombardy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Methods
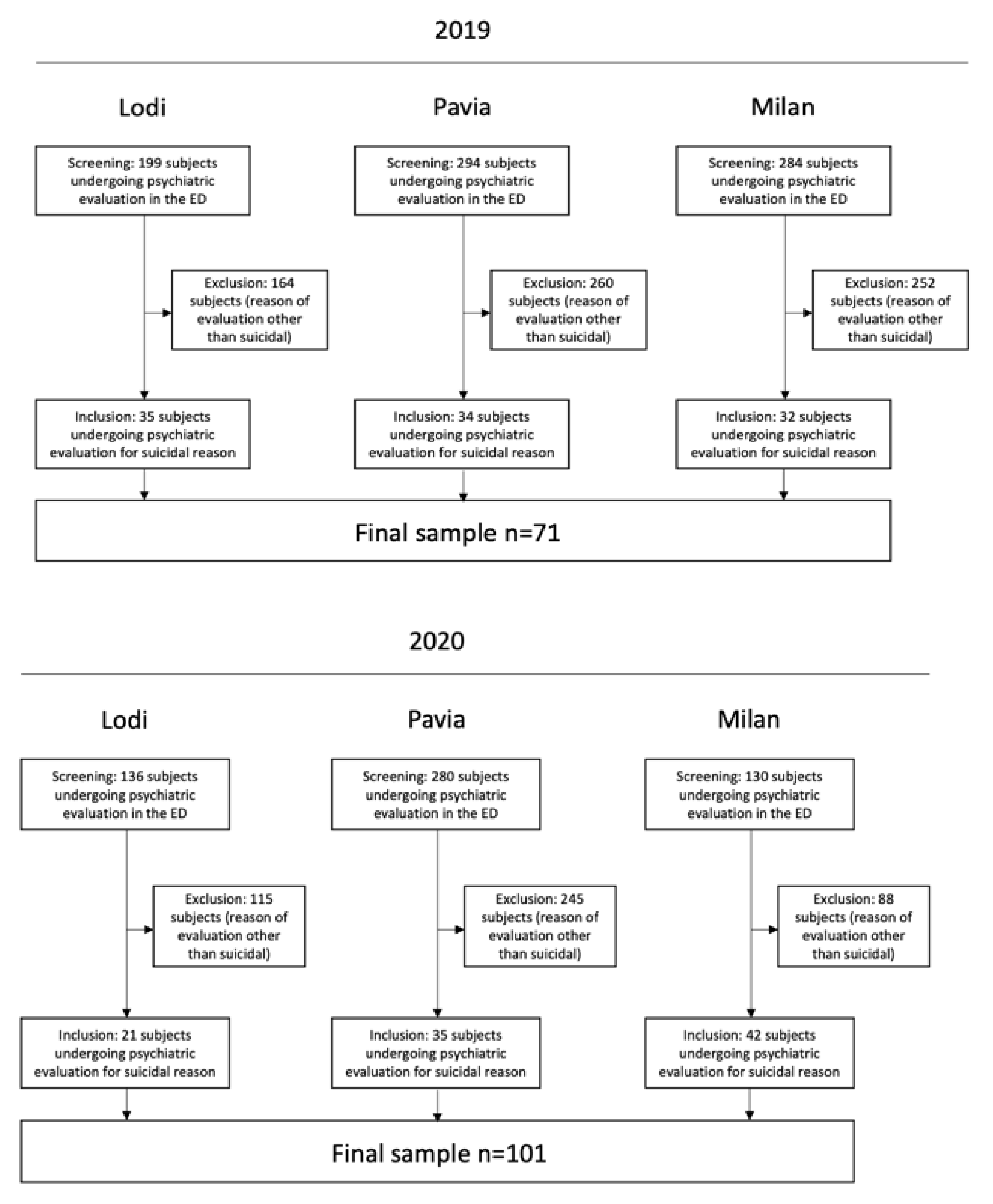
2.2. Study Population and Data Collection
2.3. Statistical Analyses
3. Results
3.1. Characteristics of Patients Accessing the ED for Suicidality during the First Wave of COVID-19 in 2020
3.2. Comparisons between 2020 and 2019
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Dates; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Bertolote, J.M.; Fleischmann, A. Suicide and psychiatric diagnosis: A worldwide perspective. World Psychiatry 2002, 1, 181–185. [Google Scholar]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D. Rebuilding the Tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, rationale, and methodology. Suicide Life Threat Behav. 2007, 37, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Hamza, C.A.; Stewart, S.L.; Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: A review of the literature and an integrated model. Clin. Psychol. Rev. 2012, 32, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, P.L.; Mutter, R.; Stocks, C. Mental Health and Substance Abuse-Related Emergency Department Visits among Adults, 2007: Statistical Brief #92. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006. Available online: https://www.ncbi.nlm.nih.gov/books/NBK52659/ (accessed on 7 May 2021).
- Miller, I.W.; Camargo, C.A., Jr.; Arias, S.A.; Sullivan, A.F.; Allen, M.H.; Goldstein, A.B.; Manton, A.P.; Espinola, J.A.; Jones, R.; Hasegawa, K.; et al. Suicide Prevention in an Emergency Department Population: The ED-SAFE Study. JAMA Psychiatry 2017, 74, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claassen, C.A.; Larkin, G.L. Occult suicidality in an emergency department population. Br. J. Psychiatry 2005, 186, 352–353. [Google Scholar] [CrossRef] [Green Version]
- Boudreaux, E.D.; Cagande, C.; Kilgannon, H.; Kumar, A.; Camargo, C.A. A prospective study of depression among adult patients in an urban emergency department. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Brenner, J.M.; Marco, C.A.; Kluesner, N.H.; Schears, R.M.; Martin, D.R. Assessing psychiatric safety in suicidal emergency department patients. J. Am. Coll. Emerg. Physicians Open 2020, 1, 30–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratta, P.; Capanna, C.; Riccardi, I.; Carmassi, C.; Piccinni, A.; Dell’Osso, L.; Rossi, A. Suicidal intention and negative spiritual coping one year after the earthquake of L’Aquila (Italy). J. Affect. Disord. 2012, 136, 1227–1231. [Google Scholar] [CrossRef]
- Kõlves, K.; Kõlves, K.E.; De Leo, D. Natural disasters and suicidal behaviours: A systematic literature review. J. Affect. Disord. 2013, 146, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Stratta, P.; Calderani, E.; Bertelloni, C.A.; Menichini, M.; Massimetti, E.; Rossi, A.; Dell’Osso, L. Impact of Mood Spectrum Spirituality and Mysticism Symptoms on Suicidality in Earthquake Survivors with PTSD. J. Relig. Health 2016, 55, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide Rates in Evacuation Areas After the Fukushima Daiichi Nuclear Disaster. Crisis 2018, 39, 353–363. [Google Scholar] [CrossRef]
- Wasserman, D.; Iosue, M.; Wuestefeld, A.; Carli, V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry 2020, 19, 294–306. [Google Scholar] [CrossRef]
- Jafari, H.; Cheraghi, M.A.; Pashaeypoor, S.; Hoseini, A.S. Human death: A concept analysis study. J. Nurs. Midwifery Sci. 2020, 7, 170–179. [Google Scholar]
- Mamelund, S.E. Spanish Influenza Mortality of Ethnic Minorities in Norway 1918–1919. Eur. J. Popul. 2003, 19, 83–102. [Google Scholar] [CrossRef]
- Tzeng, T.T.; Chen, P.L.; Weng, T.C.; Tsai, S.Y.; Lai, C.C.; Chou, H.I.; Chen, P.W.; Lu, C.C.; Liu, M.T.; Sung, W.C.; et al. Development of high-growth influenza H7N9 prepandemic candidate vaccine viruses in suspension MDCK cells. J. Biomed. Sci. 2020, 27, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.C.; Yen, D.H.T.; Huang, H.H.; Kao, W.F.; Wang, L.M.; Huang, C.I.; Lee, C.H. Impact of severe acute respiratory syndrome (SARS) outbreaks on the use of emergency department medical resources. J. Chin. Med. Assoc. 2005, 68, 254–259. [Google Scholar] [CrossRef] [Green Version]
- Breitbart, W. A COVID-19 Obituary. Palliat. Supportive Care 2021, 19, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E., Jr. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [Green Version]
- Calati, R.; Ferrari, C.; Brittner, M.; Oasi, O.; Olié, E.; Carvalho, A.F.; Courtet, P. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. J. Affect. Disord 2019, 245, 653–667. [Google Scholar] [CrossRef]
- Qin, P.; Mehlum, L. National observation of death by suicide in the first 3 months under COVID-19 pandemic. Acta Psychiatr. Scand. 2021, 143, 92–93. [Google Scholar] [CrossRef]
- Olié, E.; Nogue, E.; Picot, M.; Courtet, P. Hospitalizations for suicide attempt during the first COVID-19 lockdown in France. Acta Psychiatr. Scand. 2021. [Google Scholar] [CrossRef]
- International Business Machines Corporation. IBM SPSS Statistics for Macintosh; Version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Butt, A.A.; Kartha, A.; Asaad, N.; Azad, A.M.; Bertollini, R.; Abou-Samra, A.B. Impact of COVID-19 upon changes in emergency room visits with chest pain of possible cardiac origin. BMC Res. Notes 2020, 13, 1–4. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding compliance and psychological impact of the SARS quarantine experience. Epidemiol. Infect. 2008, 136, 997–1007. [Google Scholar] [CrossRef]
- Conejero, I.; Nobile, B.; Olié, E.; Courtet, P. How Does COVID-19 Affect the Neurobiology of Suicide? Curr. Psychiatry Rep. 2021, 23, 16. [Google Scholar] [CrossRef] [PubMed]
- Hicks, B.M.; Blonigen, D.M.; Kramer, M.D.; Krueger, R.F.; Patrick, C.J.; Iacono, W.G.; McGue, M. Gender differences and developmental change in externalizing disorders from late adolescence to early adulthood: A longitudinal twin study. J. Abnorm. Psychol. 2007, 116, 433–447. [Google Scholar] [CrossRef] [Green Version]
- Crowley, M.S. Men’s Self-Perceived Adequacy as the Family Breadwinner: Implications for Their Psychological, Marital, and Work-Family Weil-Being. J. Fam. Econ. Issues 1998, 19, 7–23. [Google Scholar] [CrossRef]
- Lundin, A.; Lundberg, I.; Allebeck, P.; Hemmingsson, T. Unemployment and suicide in the Stockholm population: A register-based study on 771,068 men and women. Public Health 2012, 126, 371–377. [Google Scholar] [CrossRef]
- Deady, M.; Tan, L.; Kugenthiran, N.; Collins, D.; Christensen, H.; Harvey, S.B. Unemployment, suicide and COVID-19: Using the evidence to plan for prevention. Med. J. Aust. 2020, 213, 153–154. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year 2019 | Year 2020 | Chi Square | Sig. | |
|---|---|---|---|---|
| (n = 101) | (n = 94) | |||
| Sex | 0.035 | 0.852 | ||
| female | 61 (60.4) | 58 (61.7) | ||
| male | 40 (39.6) | 36 (38.3) | ||
| Nationality | 0.157 | 0.692 | ||
| Italian | 76 (75.2) | 73 (77.7) | ||
| Other | 25 (24.8) | 21 (22.3) | ||
| Occupation | 3.338 | 0.503 | ||
| employed | 17 (16.8) | 13 (13.8) | ||
| unemployed | 40 (39.6) | 41 (43.6) | ||
| student | 12 (11.9) | 6 (6.4) | ||
| retired | 10 (9.9) | 7 (7.4) | ||
| other/not known | 22 (21.8) | 27 (28.7) | ||
| Marital status | 3.955 | 0.412 | ||
| Married | 15 (14.9) | 18 (19.1) | ||
| unmarried | 54 (53.5) | 48 (51.1) | ||
| separated/divorced | 10 (9.9) | 14 (14.9) | ||
| widowed | 7 (6.9) | 7 (7.4) | ||
| other/unknown | 15 (14.9) | 7 (7.4) | ||
| Cohabitation status | 9.407 | 0.052 | ||
| partner/children | 25 (24.8) | 40 (42.6) | ||
| parents/siblings | 21 (20.8) | 20 (21.3) | ||
| alone | 24 (23.8) | 19 (20.2) | ||
| institution | 18 (17.8) | 9 (9.6) | ||
| other/unknown | 13 (12.9) | 6 (6.4) | ||
| Phase of access | 0.966 | 0.326 | ||
| 8 March–4 May | 66 (65.3) | −58.5 | ||
| 5 May–3 June | 35 (34.7) | −41.5 | ||
| T | Sig. | |||
| Age (mean, SD) | 42.5 ± 17.6 | 42.4 ± 15.4 | 0.051 | 0.959 |
| Year 2019 | Year 2020 | Chi2 | Sig. | |
|---|---|---|---|---|
| (n = 101) | (n = 94) | |||
| Usual care provider | 0.305 | 0.859 | ||
| None | 49 (48.5) | 48 (51.1) | ||
| Public/private MHS+ | 40 (39.6) | 37 (39.4) | ||
| Addiction Service | 12 (11.9) | 9 (9.6) | ||
| History of alcohol substance abuse | 26 (25.7) | 27 (28.7) | 0.219 | 0.64 |
| Triage priority level | 0.005 | 0.945 | ||
| high | 51 (50.5) | 47 (50) | ||
| low | 50 (49.5) | 47 (50) | ||
| Conflicts triggering suicidality | 47 (46.5) | 38 (40.4) | 0.739 | 0.39 |
| Suicidality * | ||||
| Suicidal thoughts | 16 (16) | 19 (20.2) | 0.582 | 0.446 |
| Suicide attempt | 1 (1) | 3 (3.2) | 1.174 | 0.279 |
| Self-injuring | 21 (21) | 14 (14.9) | 1.222 | 0.269 |
| Drug ingestion | 54 (54) | 49 (52.1) | 0.068 | 0.794 |
| Discharge diagnosis | ||||
| Anxiety disorder | 7 (6.9) | 6 (6.4) | 0.023 | 0.878 |
| Mood disorder | 38 (37.6) | 31 (33) | 0.459 | 0.498 |
| Psychotic disorder | 2 (2) | 7 (7.4) | 3.305 | 0.069 |
| Personality disorder | 49 (48.5) | 38 (43.7) | 1.289 | 0.256 |
| No mental disorders/harmful substance use | 5 (5) | 12 (12.8) | 3.737 | 0.05 |
| Admission to psychiatric inpatient care | 32 (31.7) | 30 (31.9) | 0.001 | 0.972 |
| Year 2019 (n = 101) | Year 2020 (n = 94) | Chi2 | Sig. | |
|---|---|---|---|---|
| Psychotropic treatment at the moment of ED consultation | ||||
| Any psychotropic treatment | 74 (73.3) | 56 (59.6) | 4.108 | 0.043 |
| Anxiolytics | 51 (50.5) | 31 (33) | 6.130 | 0.013 |
| Antidepressants | 43 (42.6) | 41 (43.6) | 0.022 | 0.883 |
| Antipsychotics | 33 (32.7) | 23 (24.5) | 1.601 | 0.206 |
| Mood stabilizers | 12 (11.9) | 9 (9.6) | 0.270 | 0.604 |
| Psychotropic treatment administered during ED consultation | ||||
| Anxiolytics | 12 (11.9) | 26 (27.7) | 7.725 | 0.005 |
| Antidepressants | 0 (0) | 1 (1.1) | 1.080 | 0.299 |
| Antipsychotics | 6 (5.9) | 5 (5.3) | 0.035 | 0.851 |
| Mood stabilizers | 0 (0) | 2 (2.1) | 2.171 | 0.141 |
| Psychotropic treatment prescribed at discharge from PES | ||||
| Anxiolytics | 17 (16.8) | 15 (16) | 0.027 | 0.869 |
| Antidepressants | 22 (21.8) | 19 (20.2) | 0.072 | 0.788 |
| Antipsychotics | 14 (13.9) | 12 (12.8) | 0.051 | 0.822 |
| Mood stabilizers | 5 (5) | 3 (3.2) | 0.383 | 0.536 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gesi, C.; Grasso, F.; Dragogna, F.; Vercesi, M.; Paletta, S.; Politi, P.; Mencacci, C.; Cerveri, G. How Did COVID-19 Affect Suicidality? Data from a Multicentric Study in Lombardy. J. Clin. Med. 2021, 10, 2410. https://doi.org/10.3390/jcm10112410
Gesi C, Grasso F, Dragogna F, Vercesi M, Paletta S, Politi P, Mencacci C, Cerveri G. How Did COVID-19 Affect Suicidality? Data from a Multicentric Study in Lombardy. Journal of Clinical Medicine. 2021; 10(11):2410. https://doi.org/10.3390/jcm10112410
Chicago/Turabian StyleGesi, Camilla, Federico Grasso, Filippo Dragogna, Marco Vercesi, Silvia Paletta, Pierluigi Politi, Claudio Mencacci, and Giancarlo Cerveri. 2021. "How Did COVID-19 Affect Suicidality? Data from a Multicentric Study in Lombardy" Journal of Clinical Medicine 10, no. 11: 2410. https://doi.org/10.3390/jcm10112410