
An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan

 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Settings
4.2. Study Design
4.3. Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aldeyab, M.; López-Lozano, J.M.; Gould, I.M. Global Antibiotics Use and Resistance. In Global Pharmaceutical Policy; Babar, Z.U.D., Ed.; Palgrave Macmillan: Singapore, 2020; Available online: https://doi.org/10.1007/978-981-15-2724-1_13 (accessed on 7 June 2021).
- Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. The Review on Antimicrobial Resistance. Chaired by Jim O’Neill, December 2014. Available online: https://amr-review.org/Publications.html (accessed on 13 March 2021).
- Hayajneh, W.A.; Al-Azzam, S.; Yusef, D.; Lattyak, W.J.; Lattyak, E.A.; Gould, I.; López-Lozano, J.M.; Conway, B.R.; Conlon-Bingham, G.; Aldeyab, M.A. Identification of thresholds in relationships between specific antibiotic use and carbapenem-resistant Acinetobacter baumannii (CRAb) incidence rates in hospitalized patients in Jordan. J. Antimicrob. Chemother. 2021, 76, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Conlon-Bingham, G.M.; Aldeyab, M.; Scott, M.; Kearney, M.P.; Farren, D.; Gilmore, F.; McElnay, J. Effects of Antibiotic Cycling Policy on Incidence of Healthcare-Associated MRSA and Clostridioides difficile Infection in Secondary Healthcare Settings. Emerg. Infect. Dis. 2019, 25, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jirjees, F.J.; Al-Obaidi, H.J.; Sartaj, M.; ConlonBingham, G.; Farren, D.; Scott, M.G.; Gould, I.M.; López-Lozano, J.M.; Aldeyab, M.A. Antibiotic Use and Resistance in Hospitals: Time-Series Analysis Strategy for Determining and Prioritising Interventions. Hosp. Pharm. Eur. 2020, 13–19. Available online: https://hospitalpharmacyeurope.com/news/reviews-research/antibiotic-use-and-resistance-in-hospitals-time-series-analysis-strategy-for-determining-and-prioritising-interventions/ (accessed on 7 June 2021).
- Resolution WHA 68-7. Global action plan on antimicrobial resistance. In Proceedings of the Sixty-Eighth World Health Assembly, Geneva, Switzerland, 26 May 2015; Annex 3. WHO: Geneva, Switzerland, 2015. [Google Scholar]
- GLASS Guide for National Surveillance Systems for Monitoring Antimicrobial Consumption in Hospitals; Licence: CC BY-NC-SA 3.0 IGO; accessed on 7 June 2021; World Health Organization: Geneva, Switzerland, 2020.
- WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation; World Health Organization: Geneva, Switzerland, 2018.
- Aldeyab, M.A.; McElnay, J.C.; Scott, M.G.; Lattyak, W.J.; Darwish Elhajji, F.W.; Aldiab, M.A.; Magee, F.A.; Conlon, G.; Kearney, M.P. A modified method for measuring antibiotic use in healthcare settings: Implications for antibiotic stewardship and benchmarking. J. Antimicrob. Chemother. 2014, 69, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusef, D.; Hayajneh, W.; Bond, S.; Lee-Milner, J.; Al-Azzam, S.; Bani Issa, A.; Jaradat, S.; Gould, I.; Conway, B.R.; Hasan, S.; et al. Analysis of hospital antimicrobial consumption to identify targets for antimicrobial stewardship. Infect. Control Hosp. Epidemiol. 2021, 1–3. [Google Scholar] [CrossRef]
- Yusef, D.; Hayajneh, W.A.; Bani Issa, A.; Haddad, R.; Al-Azzam, S.; Lattyak, E.A.; Lattyak, W.J.; Gould, I.; Conway, B.R.; Bond, S.; et al. Impact of an antimicrobial stewardship programme on reducing broad-spectrum antibiotic use and its effect on carbapenem-resistant Acinetobacter baumannii (CRAb) in hospitals in Jordan. J. Antimicrob. Chemother. 2021, 76, 516–523. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 16–24 February 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 9 March 2021).
- Warsi, I.; Khurshid, Z.; Shazam, H.; Umer, M.F.; Imran, E.; Khan, M.O.; Slowey, P.D.; Goodson, J.M. Saliva Exhibits High Sensitivity and Specificity for the Detection of SARS-COV-2. Diseases 2021, 9, 38. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef]
- Martinez-Guerra, B.A.; Gonzalez-Lara, M.F.; de-Leon-Cividanes, N.A.; Tamez-Torres, K.M.; Roman-Montes, C.M.; Rajme-Lopez, S.; Villalobos-Zapata, G.I.; Lopez-Garcia, N.I.; Martínez-Gamboa, A.; Sifuentes-Osornio, J.; et al. Antimicrobial Resistance Patterns and Antibiotic Use during Hospital Conversion in the COVID-19 Pandemic. Antibiotics 2021, 10, 182. [Google Scholar] [CrossRef]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of Antimicrobial Consumption During the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef]
- Rawson, T.M.; Ming, D.; Ahmad, R.; Moore, L.S.P.; Holmes, A.H. Antimicrobial use, drug-resistant infections and COVID-19. Nat. Rev. Microbiol. 2020, 18, 409–410. [Google Scholar] [CrossRef]
- Lucien, M.A.B.; Canarie, M.F.; Kilgore, P.E.; Jean-Denis, G.; Fénélon, N.; Pierre, M.; Cerpa, M.; Joseph, G.A.; Maki, G.; Zervos, M.J.; et al. Antibiotics and antimicrobial resistance in the COVID-19 era: Perspective from resource-limited settings. Int. J. Infect. Dis. 2021, 104, 250–254. [Google Scholar] [CrossRef]
- World Bank. Drug-Resistant Infections: A Threat to Our Economic Future; World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Tomson, G.; Vlad, I. The need to look at antibiotic resistance from a health systems perspective. Upsala J. Med. Sci. 2014, 119, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Hamidi, A.; Yılmaz, Ş. Antibiotic consumption in the hospital during COVID-19 pandemic, distribution of bacterial agents and antimicrobial resistance: A single-center study. J. Surg. Med. 2021, 5, 124–127. [Google Scholar] [CrossRef]
- Ul Mustafa, Z.; Salman, M.; Aldeyab, M.; Kow, C.S.; Hasan, S.S. Antimicrobial consumption among hospitalized patients with COVID-19 in Pakistan. SN Compr. Clin. Med. 2021. [Google Scholar] [CrossRef]
- Gonzalez-Zorn, B. Antibiotic use in the COVID-19 crisis in Spain. Clin. Microbiol. Infect. 2021, 27, 646–647. [Google Scholar] [CrossRef]
- Elhajji, F.D.; Al-Taani, G.M.; Anani, L.; Al-Masri, S.; Abdalaziz, H.; Qabba’h, S.H.; Al Bawab, A.Q.; Scott, M.; Farren, D.; Gilmore, F.; et al. Comparative point prevalence survey of antimicrobial consumption between a hospital in Northern Ireland and a hospital in Jordan. BMC Health Serv. Res. 2018, 18, 849. [Google Scholar] [CrossRef] [Green Version]
- King, L.M.; Lovegrove, M.C.; Shehab, N.; Tsay, S.; Budnitz, D.S.; Geller, A.I.; Lind, J.N.; Roberts, R.; Hicks, L.A.; Kabbani, S. Trends in U.S. outpatient antibiotic prescriptions during the COVID-19 pandemic. Clin. Infect. Dis. 2020, ciaa1896. [Google Scholar] [CrossRef]
- De Lusignan, S.; Joy, M.; Sherlock, J.; Tripathy, M.; van Hecke, O.; Gbinigie, O.; Williams, J.; Butler, C.; Hobbs, F.D.R. PRINCIPLE trial demonstrates scope for in-pandemic improvement in primary care antibiotic stewardship. medRxiv 2021. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef] [PubMed]
- Touret, F.; Gilles, M.; Barral, K.; Nougairède, A.; van Helden, J.; Decroly, E.; de Lamballerie, X.; Coutard, B. In vitro screening of a FDA approved chemical library reveals potential inhibitors of SARS-CoV-2 replication. Sci. Rep. 2020, 10, 13093. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.E.; Hinks, T.S.C. Azithromycin in viral infections. Rev. Med. Virol. 2020, 31, e2163. [Google Scholar] [CrossRef] [PubMed]
- Min, J.Y.; Jang, Y.J. Macrolide therapy in respiratory viral infections. Mediat. Inflamm. 2012, 2012, 649570. [Google Scholar] [CrossRef] [Green Version]
- PRINCIPLE Trial Collaborative Group. Azithromycin for community treatment of suspected COVID-19 in people at increased risk of an adverse clinical course in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet 2021, 397, 1063–1074. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Azithromycin in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 605–612. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.P.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Furtado, R.H.M.; Berwanger, O.; Fonseca, H.A.; Corrêa, T.D.; Ferraz, L.R.; Lapa, M.G.; Zampieri, F.G.; Veiga, V.C.; Azevedo, L.C.P.; Rosa, R.G.; et al. Azithromycin in addition to standard of care versus standard of care alone in the treatment of patients admitted to the hospital with severe COVID-19 in Brazil (COALITION II): A randomised clinical trial. Lancet 2020, 396, 959–967. [Google Scholar] [CrossRef]
- Mercuro, N.J.; Yen, C.F.; Shim, D.J.; Maher, T.R.; McCoy, C.M.; Zimetbaum, P.J.; Gold, H.S. Risk of QT Interval Prolongation Associated with Use of Hydroxychloroquine With or Without Concomitant Azithromycin Among Hospitalized Patients Testing Positive for Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1036–1041. [Google Scholar] [CrossRef]
- Roden, D.M.; Harrington, R.A.; Poppas, A.; Russo, A.M. Considerations for Drug Interactions on QTc Interval in Exploratory COVID-19 Treatment. J. Am. Coll. Cardiol. 2020, 75, 2623–2624. [Google Scholar] [CrossRef]
- Rodrigo, C.; Fernando, S.D.; Rajapakse, S. Clinical evidence for repurposing chloroquine and hydroxychloroquine as antiviral agents: A systematic review. Clin. Microbiol. Infect. 2020, 26, 979–987. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar]
- World Health Organization. WHO Discontinues Hydroxychloroquine and Lopinavir/Ritonavir Treatment Arms for COVID-19. 4 July 2020. Available online: https://www.who.int/news/item/04-07-2020-who-discontinues-hydroxychloroquine-and-lopinavir-ritonavir-treatment-arms-for-covid-19 (accessed on 14 March 2021).
- Letter from the, U.S. Food and Drug Administration re: Revocation of the Emergency Use Authorization (EUA) Letter of March 20, 2020. 15 June 2020. Available online: https://www.fda.gov/media/138945/download (accessed on 14 March 2021).
- World Health Organization. The 2019 WHO AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use. World Health Organization. License: CC BY-NC-SA 3.0 IGO. 2019. Available online: https://apps.who.int/iris/handle/10665/327957 (accessed on 7 June 2021).
- Sharland, M.; Gandra, S.; Huttner, B.; Moja, L.; Pulcini, C.; Zeng, M.; Mendelson, M.; Cappello, B.; Cooke, G.; Magrini, N.; et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use- the new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect. Dis. 2019, 19, 1278–1280. [Google Scholar] [CrossRef]
- Chen, C.; Huang, J.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; Luo, Y.; Zhang, J.; et al. Favipiravir versus arbidol for COVID-19: A randomized clinical trial. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhong, W.; Salam, A.; Tarning, J.; Zhan, Q.; Huang, J.A.; Weng, H.; Bai, C.; Ren, Y.; Yamada, K.; et al. Phase 2a, open-label, dose-escalating, multi-center pharmacokinetic study of favipiravir (T-705) in combination with oseltamivir in patients with severe influenza. EBioMedicine 2020, 62, 103125. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, G.; Salam, A.; Horby, P.; Hayden, F.G.; Chen, C.; Pan, J.; Zheng, J.; Lu, B.; Guo, L.; et al. Comparative Effectiveness of Combined Favipiravir and Oseltamivir Therapy Versus Oseltamivir Monotherapy in Critically Ill Patients with Influenza Virus Infection. J. Infect. Dis. 2020, 221, 1688–1698. [Google Scholar] [CrossRef]
- Strasfeld, L.; Chou, S. Antiviral drug resistance: Mechanisms and clinical implications. Infect. Dis. Clin. N. Am. 2010, 24, 413–437, Erratum in 2010, 24, 809–833. [Google Scholar] [CrossRef] [Green Version]
- Behillil, S.; May, F.; Fourati, S.; Luyt, C.E.; Chicheportiche, T.; Sonneville, R.; Tandjaoui-Lambiotte, Y.; Roux, D.; Guérin, L.; Mayaux, J.; et al. Oseltamivir Resistance in Severe Influenza A(H1N1)pdm09 Pneumonia and Acute Respiratory Distress Syndrome: A French Multicenter Observational Cohort Study. Clin. Infect. Dis. 2020, 71, 1089–1091. [Google Scholar] [CrossRef]
- Hayden, F.G.; Shindo, N. Influenza virus polymerase inhibitors in clinical development. Curr. Opin. Infect. Dis. 2019, 32, 176–186. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 9 March 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Bergman, U.; Popa, C.; Tomson, Y.; Wettermark, B.; Einarson, T.R.; Aberg, H.; Sjöqvist, F. Drug utilization 90%—A simple method for assessing the quality of drug prescribing. Eur. J. Clin. Pharmacol. 1998, 54, 113–118. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
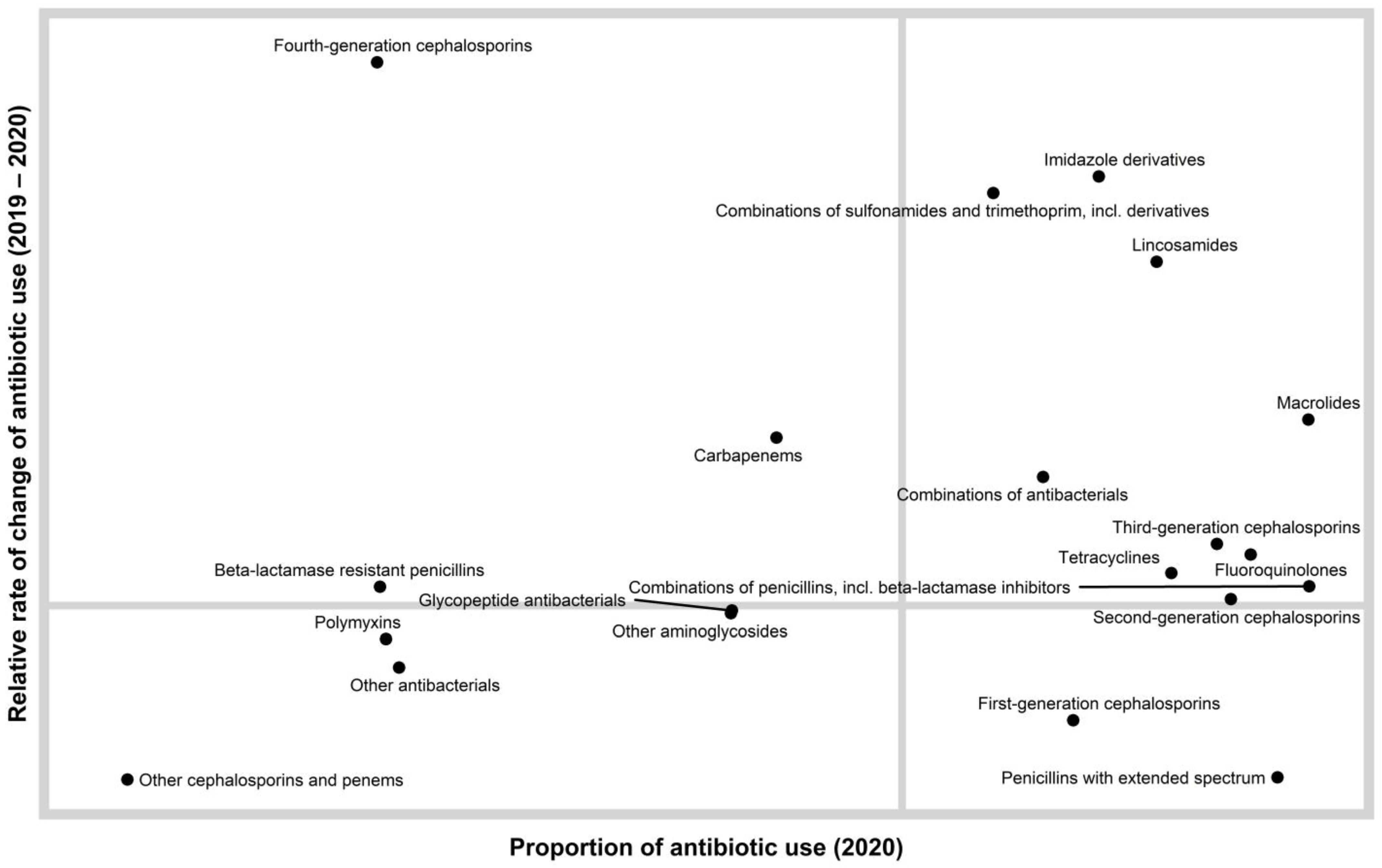
| Antimicrobial Class | National Antibiotic Use 2019 | National Antibiotic Use 2020 | Relative Rate of Change * | ||
|---|---|---|---|---|---|
| Total DDD per 1000 Inhabitants per Day | Class% | Total DDD per 1000 Inhabitants per Day | Class% | ||
| Tetracyclines | 1.508 | 5.312% | 1.5673 | 5.844% | 1.10 |
| Penicillins with extended spectrum | 8.396 | 29.574% | 3.7361 | 13.930% | 0.47 |
| Beta-lactamase resistant penicillins | 0.002 | 0.008% | 0.0024 | 0.009% | 1.06 |
| Combinations of penicillins, including beta-lactamase inhibitors | 4.843 | 17.059% | 4.8462 | 18.069% | 1.06 |
| First-generation cephalosporins | 1.147 | 4.042% | 0.7015 | 2.616% | 0.65 |
| Second-generation cephalosporins | 2.650 | 9.335% | 2.5534 | 9.520% | 1.02 |
| Third-generation cephalosporins | 2.024 | 7.128% | 2.2750 | 8.482% | 1.19 |
| Fourth-generation cephalosporins | 0.000 | 0.001% | 0.0023 | 0.009% | 9.35 |
| Carbapenems | 0.043 | 0.152% | 0.0618 | 0.230% | 1.52 |
| Other cephalosporins and penems | 0.001 | 0.003% | 0.0003 | 0.001% | 0.34 |
| Combinations of sulfonamides and trimethoprim, including derivatives | 0.170 | 0.598% | 0.3646 | 1.359% | 2.27 |
| Macrolides | 3.238 | 11.405% | 4.8133 | 17.947% | 1.57 |
| Lincosamides | 0.714 | 2.514% | 1.3892 | 5.180% | 2.06 |
| Other aminoglycosides | 0.046 | 0.162% | 0.0425 | 0.158% | 0.98 |
| Fluoroquinolones | 2.745 | 9.669% | 3.0007 | 11.188% | 1.16 |
| Combinations of antibacterials | 0.416 | 1.464% | 0.5483 | 2.044% | 1.40 |
| Glycopeptide antibacterials | 0.046 | 0.162% | 0.0429 | 0.160% | 0.98 |
| Polymyxins | 0.003 | 0.010% | 0.0025 | 0.009% | 0.90 |
| Imidazole derivatives | 0.394 | 1.389% | 0.8657 | 3.228% | 2.32 |
| Other antibacterials | 0.004 | 0.013% | 0.0028 | 0.010% | 0.81 |
| Year | Access | Watch | Reserve |
|---|---|---|---|
| DDD per 1000 Inhabitants per Day (%) | |||
| National antimicrobial use (2019) | 16.79 (59.13) | 11.59 (40.83) | 0.011 (0.0376) |
| National antimicrobial use (2020) | 13.05 (48.67) | 13.76 (51.30) | 0.008 (0.0315) |
| Relative rate of change * | 0.82 | 1.26 | 0.84 |
| National Antimicrobial Use (2019) | National Antimicrobial Use (2020) | ||||
|---|---|---|---|---|---|
| Antimicrobials * | DID ** | DIDs% ** | Antimicrobials * | DID ** | DIDs% ** |
| Amoxicillin | 8.39 | 29.56% | Amoxicillin/clavulanic Acid | 4.83 | 17.99% |
| Amoxicillin/clavulanic Acid | 4.82 | 16.97% | Amoxicillin | 3.73 | 13.91% |
| Cefuroxime | 2.37 | 8.34% | Azithromycin | 2.55 | 9.49% |
| Azithromycin | 1.54 | 5.44% | Cefuroxime | 2.31 | 8.60% |
| Ciprofloxacin | 1.53 | 5.40% | Clarithromycin | 1.87 | 6.98% |
| Doxycycline | 1.38 | 4.87% | Ciprofloxacin | 1.85 | 6.89% |
| Cefixime | 1.25 | 4.40% | Cefixime | 1.51 | 5.63% |
| Clarithromycin | 1.21 | 4.26% | Doxycycline | 1.32 | 4.94% |
| Cefalexin | 1.11 | 3.90% | Clindamycin | 1.19 | 4.43% |
| Levofloxacin | 1.02 | 3.58% | Levofloxacin | 0.89 | 3.32% |
| Clindamycin | 0.43 | 1.52% | Metronidazole (IV) | 0.87 | 3.23% |
| Spiramycin/metronidazole | 0.42 | 1.46% | Cefalexin | 0.61 | 2.28% |
| Metronidazole (IV) | 0.39 | 1.39% | Spiramycin/metronidazole | 0.55 | 2.04% |
| Sulfamethoxazole/trimethoprim | 0.36 | 1.36% | |||
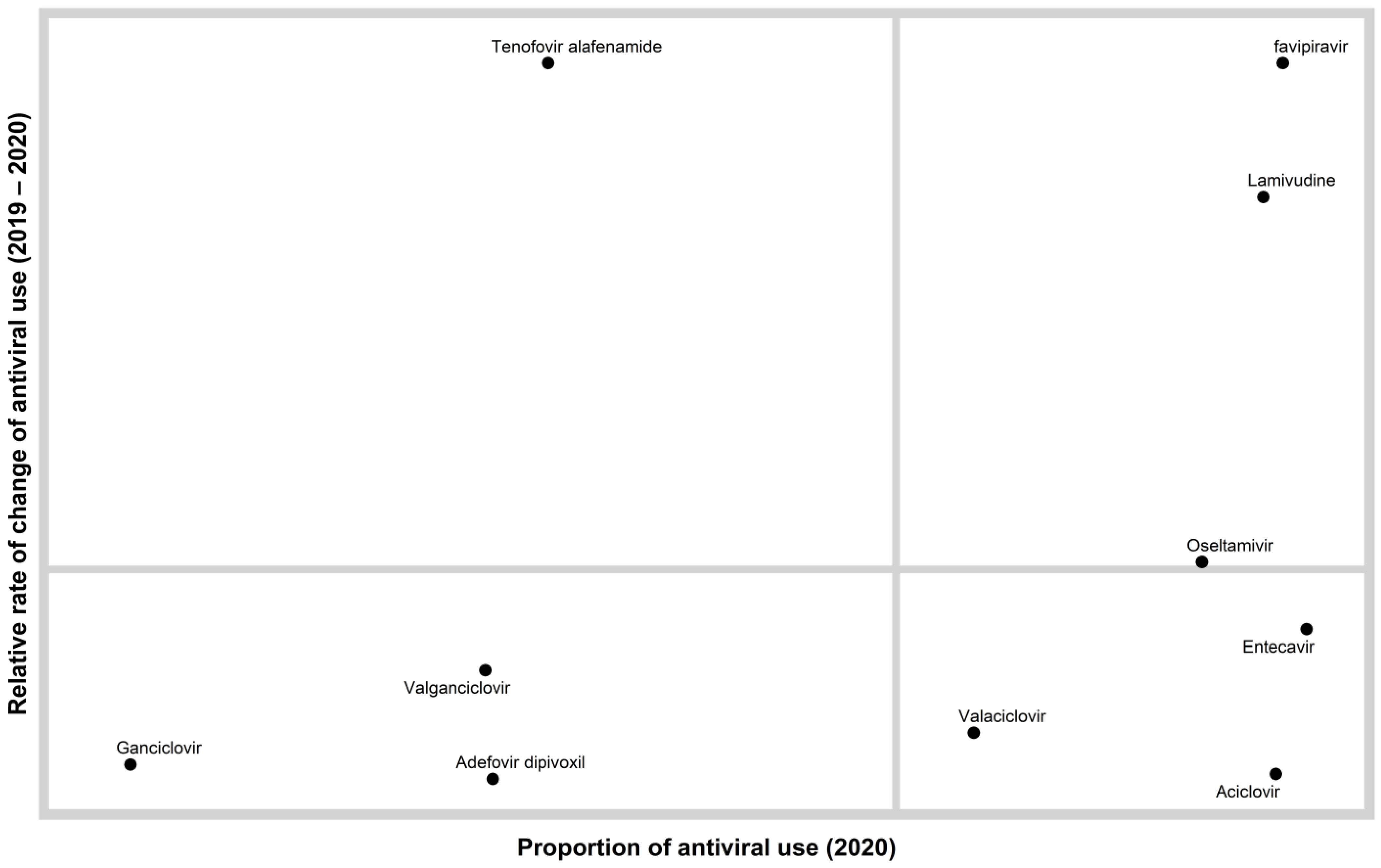
| Antiviral Agent | National Antibiotic Use 2019 | National Antibiotic Use 2020 | Relative Rate of Change * | ||
|---|---|---|---|---|---|
| Total DDD per 1000 Inhabitants per Day | Class% | Total DDD per 1000 Inhabitants per Day | Class% | ||
| Aciclovir | 0.058 | 38.87% | 0.039 | 18.99% | 0.49 |
| Ganciclovir | 0.000 | 0.31% | 0.000 | 0.16% | 0.51 |
| Valaciclovir | 0.014 | 9.12% | 0.011 | 5.40% | 0.59 |
| Valganciclovir | 0.001 | 0.94% | 0.001 | 0.70% | 0.75 |
| Lamivudine | 0.014 | 9.32% | 0.037 | 18.01% | 1.93 |
| Adefovir dipivoxil | 0.003 | 1.98% | 0.001 | 0.73% | 0.37 |
| Entecavir | 0.038 | 25.37% | 0.044 | 21.57% | 0.85 |
| Tenofovir alafenamide | 0.001 | 0.39% | 0.002 | 0.92% | 2.34 |
| Oseltamivir | 0.020 | 13.70% | 0.029 | 13.95% | 1.02 |
| Favipiravir | 0.000 | 0.00% | 0.040 | 19.56% | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Azzam, S.; Mhaidat, N.M.; Banat, H.A.; Alfaour, M.; Ahmad, D.S.; Muller, A.; Al-Nuseirat, A.; Lattyak, E.A.; Conway, B.R.; Aldeyab, M.A. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics 2021, 10, 690. https://doi.org/10.3390/antibiotics10060690
Al-Azzam S, Mhaidat NM, Banat HA, Alfaour M, Ahmad DS, Muller A, Al-Nuseirat A, Lattyak EA, Conway BR, Aldeyab MA. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics. 2021; 10(6):690. https://doi.org/10.3390/antibiotics10060690
Chicago/Turabian StyleAl-Azzam, Sayer, Nizar Mahmoud Mhaidat, Hayaa A. Banat, Mohammad Alfaour, Dana Samih Ahmad, Arno Muller, Adi Al-Nuseirat, Elizabeth A. Lattyak, Barbara R. Conway, and Mamoon A. Aldeyab. 2021. "An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan" Antibiotics 10, no. 6: 690. https://doi.org/10.3390/antibiotics10060690