
Therapy of Type 2 Diabetes in Patients with SARS-CoV-2 Infection


Department of Physiology, Pomeranian Medical University in Szczecin, 70-111 Szczecin, Poland
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2021, 22(14), 7605; https://doi.org/10.3390/ijms22147605
Submission received: 7 June 2021
/
Revised: 12 July 2021
/
Accepted: 13 July 2021
/
Published: 16 July 2021
(This article belongs to the Special Issue Pharmacological Strategies for Metabolic Diseases: New Evidence)
Abstract
:COVID-19 infection poses an important clinical therapeutic problem, especially in patients with coexistent diseases such as type 2 diabetes. Potential pathogenetic links between COVID-19 and diabetes include inflammation, effects on glucose homeostasis, haemoglobin deoxygenation, altered immune status and activation of the renin-angiotensin-aldosterone system (RAAS). Moreover, drugs often used in the clinical care of diabetes (dipeptidyl peptidase 4 inhibitors, glucagon-like peptide 1 receptor agonists, sodium-glucose cotransporter 2 inhibitors, metformin and insulin) may influence the course of SARS-CoV-2 infection, so it is very important to verify their effectiveness and safety. This review summarises the new advances in diabetes therapy and COVID-19 and provides clinical recommendations that are essential for medical doctors and for patients suffering from type 2 diabetes.
1. Introduction
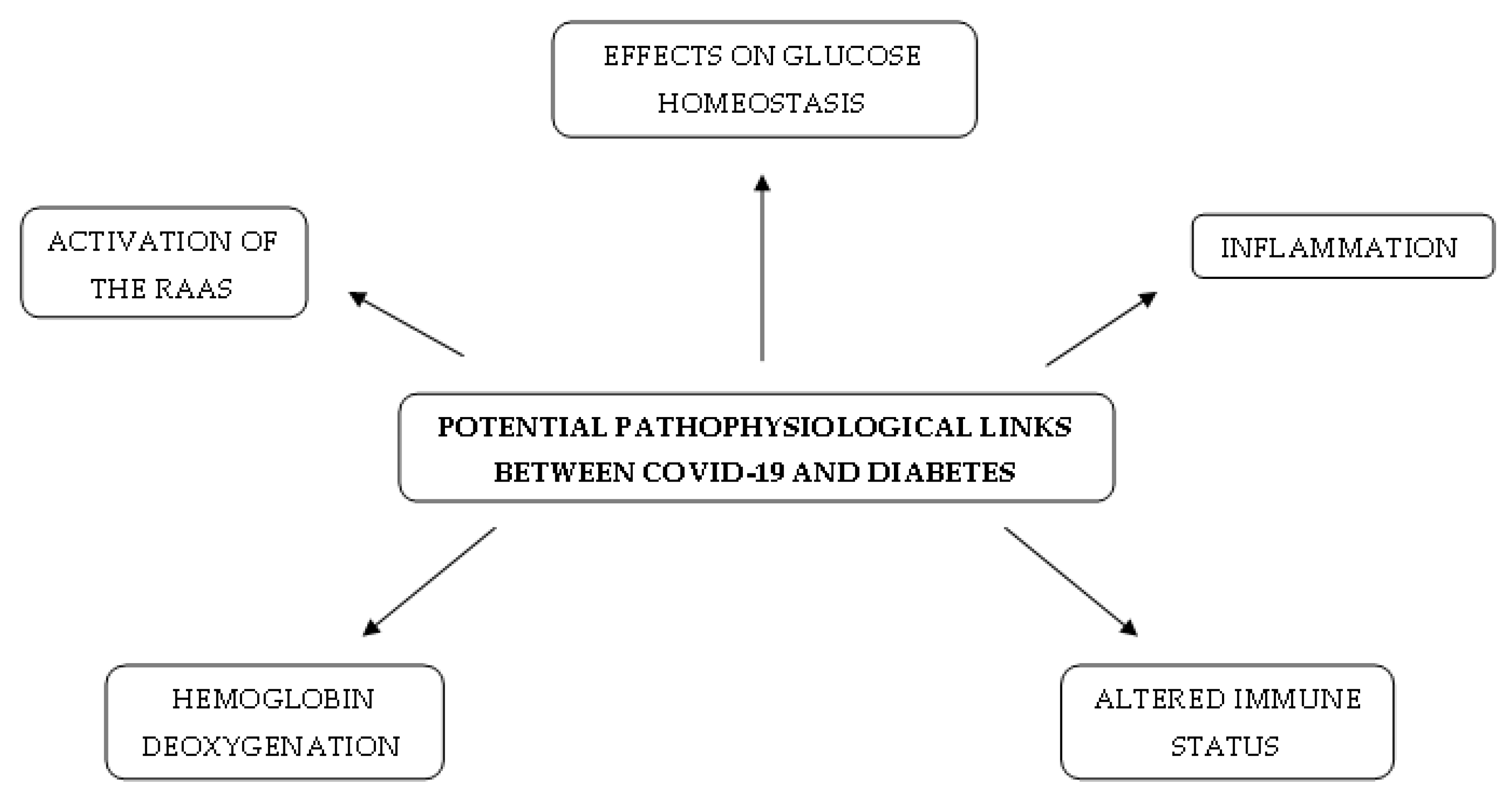
Coronavirus disease 2019 (COVID-19), caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), currently affects many people worldwide. Studies have found an increased severity of COVID-19 or a high risk of death in patients with advanced age, male sex, cardiovascular disease, obesity and type 1 (T1DM) or type 2 diabetes mellitus (T2DM) [1]. Both T2DM and COVID-19 infection are associated with ethnicity, socioeconomic status and metabolic factors such as metabolic syndrome [2]. Furthermore, COVID-19 infection might also create a predisposition to hyperglycaemia in people without impaired glucose tolerance [3]. The main entry receptor for SARS-CoV-2 in human cells is angiotensin-converting enzyme 2 (ACE2), which is highly expressed in lung alveolar cells, vascular endothelium, cardiac myocytes and many other cell types [4], although dipeptidyl peptidase 4 (DPP4) might also act as a binding target [5]. SARS-CoV-2 infection not only induces mild symptoms, but also has the potential to develop into systemic inflammatory response syndrome, acute respiratory distress syndrome (ARDS), multi-organ involvement and shock [6]. Potential pathogenetic links between COVID-19 and diabetes include inflammation, effects on glucose homeostasis, haemoglobin deoxygenation, altered immune status and activation of the renin-angiotensin-aldosterone system (RAAS) [3]. Moreover, drugs that are often used in the clinical care of type 2 diabetes (dipeptidyl peptidase 4 inhibitors, glucagon-like peptide 1 receptor agonists, sodium-glucose cotransporter 2 inhibitors, metformin and insulin) may influence the course of SARS-CoV-2 infection, so it is very important to verify their effectiveness and safety.
2. Potential Pathophysiological Mechanisms Existing in Diabetes and COVID-19
2.1. Effects on Glucose Homeostasis
The presence of hyperglycaemia or typical complications of diabetes increases COVID-19 severity and mortality [1]. An association exists between hyperglycaemia and dysregulation of the innate and humoral immune system. Hyperglycaemia may cause impaired phagocytosis and bactericidal activity, neutrophil chemotaxis, complement fixation and opsonisation of microorganisms, as well as altered chemokine production [7]. Moreover, elevated glucose concentrations and glycolysis support SARS-CoV-2 replication in human monocytes via the activation of hypoxia-inducible factor 1α (HIF-1α) and the production of mitochondrial reactive oxygen species [8]. Endothelial damage by inflammation, glucotoxicity, oxidative stress and cytokine production leads to an increased risk of thromboembolic complications and the risk of damage to vital organs in patients with diabetes [3]. A typical complication of COVID-19 in patients with diabetes is glycaemic deterioration, which causes the rapidly increasing need for high doses of insulin in patients requiring insulin treatment [9]. In patients with a severe course of COVID-19, viral-induced inflammation may affect the functions of the skeletal muscle and liver, which are the major organs responsible for insulin-mediated glucose uptake, thereby increasing insulin resistance [10]. Furthermore, ketoacidosis frequently occurs in patients with COVID-19, either T1DM or T2DM [11]. A study of 174 participants has demonstrated that patients with diabetic ketoacidosis and infectious shock were more likely to die of the virus [12].
2.2. Inflammation
In patients with COVID-19, IL-6, TNF-α and IFN-γ have been confirmed to be critical pathogenic cytokines involved in the inflammatory storm [13]. Blood levels of IL-6 and lactate dehydrogenase (LDH) are independent predictors of COVID-19 severity [14]. A retrospective study of 317 patients with laboratory-confirmed COVID-19 showed a correlation between these indicators of active inflammatory response within 24 h of hospitalisation and disease severity [14]. Moreover, blood levels of IL-6 might correlate with a pro-coagulant profile [15]. IL-6 may cause damage to lipids, proteins and DNA by increasing oxidative stress, which, as a consequence, leads to an impairment of the body’s structure and function and causes the rapid progression of COVID-19 in patients with diabetes [3]. The presence of other inflammatory markers, such as D-dimers and ferritin, might contribute to an increased risk of microvascular and macrovascular complications in patients with underlying diabetes [16]. In a French study, these complications were significantly associated with an increased risk of mortality in patients with diabetes and COVID-19 comorbidity [17]. On the other hand, in a Chinese study, patients with COVID-19 and elevated glucose levels showed promoted cytokine profiles and immune responses [18]. In that study, patients with coexisting diabetes had shorter hospitalisation times [18]. The possible explanation for this phenomenon is that increased blood glucose levels might be beneficial for some anti-inflammatory cytokines and for the process of eliminating the virus [18].
Respiratory syncytial virus infections increase IFN-γ production, which, as a result, activates natural killer (NK) cells as a defensive mechanism and also causes insulin resistance in human muscle and adipose tissues [19]. A connection exists between NK cell activity and glycaemic deterioration in patients with impaired glucose metabolism [20]. NK cell activity is lower in patients with T2DM than in those with prediabetes or normal glucose tolerance [20]. Reduced NK cell activity might be one explanation for why patients with diabetes are more susceptible to COVID-19 and have a worse prognoses [3].
2.3. Activation of the RAAS
In a healthy human, an equilibrium exists between the action of angiotensin II and angiotensin (1–7). Angiotensin II is made by angiotensin-converting enzyme, ACE, from angiotensin I and has vasoconstrictory and pro-thrombotic properties [21]. On the other hand, ACE2 can hydrolyse angiotensin II to angiotensin (1–7), which causes vasodilatation and acts in an antithrombotic manner through the production of prostacyclin and nitric oxide [22,23]. Moreover, angiotensin II determines the overproduction of IL-6, TNF-α and other pro-inflammatory cytokines [24]. It has been suggested that the prevalence of angiotensin II during SARS-CoV-2 infection may lead to the exacerbation of the cytokine storm and cause acute respiratory distress syndrome and multi-organ dysfunction [21]. Furthermore, ACE2 may serve as an entry receptor for SARS-CoV-2 and is expressed in many human cells, including pancreatic islets [25,26]. Hyperglycaemia might lead to the induction of aberrant glycosylation of the ACE2 receptor, which promotes the binding of SARS-CoV-2 to the ACE2 receptor [27]. On the other hand, COVID-19 infection is able to cause hyperglycaemia in people without pre-existing diabetes [28]. This finding and the localisation of ACE2 expression in the endocrine pancreatic cells suggests that SARS-CoV-2 specifically damages pancreatic islets, potentially leading to hyperglycaemia [28]. There is a possibility that the damage of pancreatic beta cells and increased insulin resistance, as well as impaired glucose metabolism, caused by COVID-19 may lead to the occurrence of diabetes in the future [29].
2.4. Haemoglobin Deoxygenation
Glycosylated haemoglobin is a deoxygenated form of haemoglobin and its level is higher in diabetic patients than in people without hyperglycaemia. Deoxyhaemoglobin may be more easily attacked by the surface proteins of SARS-CoV-2. This observation suggests that there is an increased risk of COVID-19 infection for diabetic patients. The proteins bind to the 1-β chain of the haem in the haemoglobin of erythrocytes. As a consequence, iron is dissociated to form porphyrin. This phenomenon causes a loss of function of red blood cells in oxygen and carbon dioxide carrying, leading to respiratory distress symptoms [30].
2.5. Altered Immune Status
The accumulation of HIF-1α in the hyperglycaemic state leads to the upregulation of LDH activity [31]. In addition, in severe SARS-CoV-2 infection, LDH levels are frequently higher than usual [32]. Lactate may play an important role in the modulation of the inflammatory immune response. It inhibits the retinoic acid-inducible gene I-like receptor (RLR) by binding directly to the mitochondrial antiviral-signalling protein transmembrane domain. This, as a consequence, decreases IFN production and viral clearance [33]. In the aforementioned mechanism, increased lactate production in diabetes may attenuate RLR signalling and delay the clearance of SARS-CoV-2, causing severe outcomes in patients with COVID-19 and diabetes [34]. A short summary of potential pathophysiological mechanisms existing in diabetes and COVID-19 is presented in Figure 1.
3. Diabetes Treatment and COVID-19
3.1. Dipeptidyl Peptidase 4 Inhibitors in COVID-19
The aforementioned potential pathophysiological mechanisms existing in diabetes and COVID-19 are of crucial importance in the context of diabetes treatment during SARS-CoV-2 infection. Taking into consideration all types of antidiabetic drugs, dipeptidyl peptidase 4 (DPP4) inhibitors (DPP4is), gliptins, are our first focus of attention regarding their impact on the course of COVID-19.
Dipeptidyl peptidase 4 is an aminopeptidase which is expressed on the surface of various cell types. It also circulates in the blood as a soluble form (sDPP4), maintaining its activity as an enzyme there [35]. This peptidase contributes mainly to the regulation of glucose metabolism and the degradation of incretins—hormones that lead to lower blood glucose concentrations through, among other mechanisms, increasing insulin secretion after oral food intake [36]. Furthermore, DPP4 plays a major role in the immune system. Not only is it a marker of activated T lymphocytes, but it also cleaves many peptide hormones, chemokines and proteins which show immunomodulatory properties [35]. In addition, DPP4 possibly participates in the modification of acquired and innate immune responses [37,38]. The binding of adenosine deaminase to dipeptidyl peptidase 4 plays a vital role in providing co-stimulatory signals to T lymphocytes, by increasing the degradation of adenosine, a strong suppressor of T cells, and thus promoting the activation and proliferation of T cells [39]. Moreover, adenosine deaminase has been shown to block the binding of MERS-CoV to cell-bound DPP4 and thus protect it from entering into host cells [40]. Analogous properties of this deaminase have not been confirmed in COVID-19, but cannot be excluded. DPP4 also modulates the function of other immune cells and also stimulates the production of pro-inflammatory cytokines [41].
DPP4 is known to be the main entry receptor for the Middle East Respiratory Syndrome coronavirus (MERS-CoV) [42], but in silico modelling has shown that SARS-CoV-2 probably interacts with this enzyme as well as with ACE2 [5,43]. This could be an explanation for why the spread of SARS-CoV-2 infection in various tissues runs so easily and why the virus shows tropism to either the respiratory or gastrointestinal epithelium. Increased levels of DPP4 might promote the development of SARS-CoV-2 infections in patients with coexisting diabetes and obesity and may be responsible for the more severe course of the disease in this population because of the support of subclinical chronic inflammation and immune system dysregulation [44].
The soluble form of DPP4 might enhance the responsiveness of memory cells to antigens and stimulate the proliferative response of T lymphocytes, possibly through interfering with its form located in membranes and, eventually, protecting T cells from anergy or apoptosis [45]. It has been found that the level of plasma sDPP4 is lower in patients suffering from MERS and correlates with the severity of disease [46], suggesting a protective role for the soluble enzyme. A similar conclusion about decreased sDPP4 levels has been reached regarding patients with the severe course of COVID-19 [47]. A possible explanation for this advantageous feature of sDPP4 is that it may react with virus proteins, preventing their interactions with cell-bound DPP4 and thus making viruses unable to enter into targeted tissues.
Gliptins are commonly used antidiabetic medications, which are well tolerable and body-weight-neutral, and have a low risk of hypoglycaemia, thus showing a safe profile [48]. They are inhibitors of DPP4, and not only have an impact on lowering the glucose concentration in blood in patients with diabetes, but also influence other DPP4 properties, including immune effects. It is suggested that using DPP4is may offer some advantages, preventing coronaviruses from entering host cells [49,50] and eliciting an anti-inflammatory effect, as DPP4 is also involved in the development of inflammation [51]. This last claim is supported by some research which has demonstrated a beneficial role of sitagliptin in reducing the plasma concentrations of pro-inflammatory markers [52,53]. The direct effect of gliptins on DPP4, which could prevent MERS-CoV and SARS-CoV-2 from entering into cells, seems to be unlikely, as in silico modelling has shown that binding sites for viral proteins and gliptins are different [43,54]. However, an indirect effect of DPP4i treatment on the reduced invasion of SARS-CoV-2 into targeted cells may exist, which consists of modulating the interaction between dipeptidyl peptidase and caveolin-1, a protein that is essential for the formation of endosomes and entering cells [55]. In vitro studies have shown that treatment with sitagliptin, vildagliptin or saxagliptin did not prevent coronaviruses from entering into cells [42], but the protective role of teneligliptin regarding a mechanism associated with caveolin-1 has been confirmed in a rodent model [56]. So far, there are no clear data which could prove these assumptions regarding possible interactions between DPP4is and SARS-CoV-2 entry into host cells.
Regarding the beneficial role of dipeptidyl peptidase 4 in proper immune system functions, the question is raised whether the inhibition of DPP4 through DPP4is does not deteriorate the immune response and eventually increase the susceptibility to SARS-CoV-2 infection. A meta-analysis studying the overall risk of infections of DPP4is has not confirmed any association between DPP4i treatment and an increased risk of infections in comparison to placebo or another antidiabetic treatment [57]. Large preclinical studies of rodent models have confirmed that the selective inhibition of DPP4 does not impair T-dependent immune responses to antigenic challenges [58]. Furthermore, short periods of DPP4i treatment, as well as long-term use, did not unfavourably affect the lymphocytes and plasma levels of the main cytokines [59,60].
The role of DPP4 inhibitors in the course of COVID-19 remains unknown and the current knowledge clearly supports neither a favourable nor an adverse effect of gliptins during the infection, mainly because of the small groups of patients included in the research and treated with DPP4is, the lack of some data for all patients and the different outcomes taken into consideration. In an Italian multicentre retrospective study of 338 hospitalised patients with COVID-19 and coexisting type 2 diabetes—the “Sitagliptin in Type 2 Diabetes and COVID-19 (SIDIACO)” study—treatment with sitagliptin added to the standard of care was associated with a reduction in mortality, an improvement in clinical outcomes and an increase in hospital discharges [61]. A similar conclusion about the association between DPP4i treatment and reduced mortality was made in a case series study from an academic hospital in Italy [62]. Another retrospective study including 904 diabetic patients with a moderate–severe course of SARS-CoV-2 infection showed that treatment consisting of gliptins had no significant influence on mortality and clinical outcomes [63]. Similar conclusions regarding the lack of a significant influence of DPP4is on the course of COVID-19 came from a retrospective epidemiological study including 85 hospitalised patients with type 2 diabetes [64] and from the large-scale French “Coronavirus SARS-CoV-2 and Diabetes Outcomes (CORONADO)” study) including 1317 diabetic patients [65]. In contrast, in a retrospective, observational cohort study of 717 hospitalised patients, treatment with DPP4is was associated with worse outcomes in diabetic patients, increasing the risk of intensive care unit admission [66]. In the latest meta-analysis it has been reported that DPP4 inhibitor treatment during hospitalisation is associated with lower mortality, but there is no similar correlation when infected patients used DPPis prior to admission [67]. Further research is required to define an exact role of DPPis in the course of COVID-19 in people with coexisting diabetes.
3.2. Glucagon-Like Peptide 1 Receptor Agonists in COVID-19
Glucagon-like peptide 1 (GLP1) receptor agonists (GLP1RAs) belong to another type of antidiabetic medications which affect the incretin axis.
Glucagon-like peptide 1 is a protein secreted from the intestinal L cells after oral glucose intake and immediately degraded by dipeptidyl peptidase 4. It exerts its actions through the glucagon-like peptide 1 receptor (GLP1R), expressed in various tissues—the pancreas, kidney, heart, central nervous system, gastrointestinal tract, lung, muscle or adipose tissue [68]. A reduction in the plasma levels of inflammatory markers, such as interleukin 6, intracellular adhesion molecule 1 and biomarkers of oxidative stress, has been reported during the infusion of native GLP1 in patients suffering from type 2 diabetes [69], which indicates a possible beneficial effect of incretins during inflammation.
Glucagon-like peptide 1 receptor agonists seem to have systemic anti-inflammatory properties, which might potentially play a supportive role during SARS-CoV-2 infection. They may interfere with nuclear factor-kappa B (NF-ĸB) signalling pathways [70] and inhibit the release of cytokines, attenuating pulmonary inflammation [71,72]. Moreover, treatments based on GLP1 have been confirmed to reduce not only the production of inflammatory cytokines, but also the infiltration of immune cells in organs such as the liver, kidney and lungs [36,73,74]. Treatment based on these medications shows a reduction in the production of inflammatory cytokines in the respiratory epithelium in a murine model infected with respiratory syncytial virus [75]. Furthermore, in animal studies regarding sepsis, it has been confirmed that the administration of liraglutide improved survival, vascular dysfunction and inflammation, as well as haemostatic indicators [76]. Some research has highlighted a potential positive effect of GLP1RAs in chronic inflammatory diseases, for instance, neurodegenerative disorders [77] or non-alcoholic fatty liver disease [78], probably through a reduction of inflammatory pathway activity [73]. However, it remains unknown whether such effects exerted on low-grade inflammation translate into anti-inflammatory properties during infection with SARS-CoV-2, and further research should be conducted.
The fact that liraglutide has been reported to probably increase the expression of ACE2 in the heart and lungs raised doubts about the safe long-term use of GLP1RAs in patients with diabetes under the conditions of the COVID-19 pandemic as it could increase susceptibility to infection [79,80]. However, studies have not proved this initial belief. In addition, ACE2 has been showed to have a protective role in acute respiratory distress syndrome (ARDS) in lung diseases, partly because of restoring the production of angiotensin (1–7) [81], and the under-expression of ACE2 has been confirmed to be an indicator of infection progression [80,82]. It has also been suggested that the course of SARS-CoV infection may be favourably modulated by ACE2 [83]. Moreover, in animal studies, the overexpression of ACE2 caused by the administration of liraglutide has been associated with negative effects on inflammatory and fibrotic processes [84]. Liraglutide treatment may also stimulate the synthesis of the surfactant proteins A and B by type II pneumocytes [84,85]. SARS-CoV-2 has a confirmed ability to damage type II pneumocytes, leading to a loss of surfactant and alveolar collapse [21]. It is suggested that the ability of glucagon-like peptide 1 receptor agonists to increase the expression of ACE2, and consequently to stimulate the production of surfactant, may protect the type II pneumocytes and prevent ARDS [86].
Because of the advantageous effects of GLP1RA treatment, such as a reduction in cardiovascular events [73], the prevention of cardiovascular disease and kidney disease [87,88], lowering body mass, as well as a reduction of the risk of hypoglycaemia and glucose variability in the setting of the intensive care unit [89], these drugs seem to be a good choice for patients who are at risk of a severe course of COVID-19. However, the initiation of such therapies is not recommended during acute or critical conditions because of the fact that GLP1RAs show a delayed onset of action and might cause nausea or vomiting at the beginning of treatment [90]. Presently, there are no clinical-epidemiological studies which directly indicate a beneficial effect of GLP1RA treatment on the course of COVID-19.
3.3. Sodium-Glucose Cotransporter 2 Inhibitors in COVID-19
Sodium-glucose cotransporter 2 (SGLT2) inhibitors (SGLT2is), or gliflozins, are oral antidiabetic drugs which mainly act on the kidneys and inhibit renal glucose reuptake in proximal renal tubes, inducing glucosuria and a decrease in glycaemia.
SGLT2is have been shown to increase the expression of ACE2 in the kidney, similar to GLP1RAs, so an assumption that they may increase susceptibility to infection has been made [79]. On the other hand, the upregulation of ACE2 leads to an increase in the production of angiotensin (1–7), a vasodilator showing anti-oxidative as well as anti-fibrotic properties, and preventing the development of ARDS [91]. These drugs have also been reported to reduce cardiovascular and renal complications, as well as to show anti-inflammatory properties in animal models [92]. In some studies, treatment based on SGLT2 inhibitors in T2DM patients decreased the mRNA expression levels of tumour necrosis factor, IL-6 or monocyte chemoattractant protein 1 [93,94]. Moreover, one of the SGLT2is, dapagliflozin, has been reported to potentially decrease lactic acidosis through various mechanisms and influence the acid–base balance inside a cell under conditions of hypoxia, which could eventually prevent cell injury during the course of COVID-19 [95]. Furthermore, dapagliflozin, by lowering the cytosolic pH and decreasing the viral load, may protect against the severe course of SARS-CoV-2 infection [95].
A large-scale analysis has shown that patients who suffer from cardiometabolic or renal diseases have susceptibility to worse outcomes of COVID-19 [96]. Other pleiotropic effects of gliflozins, such as cardioprotective and nephroprotective properties [97], mean that the attention of scientists and clinicians is turned to SGLT2is as a treatment which could potentially prevent the adverse course of the infection. Currently, no clinical research has investigated an advantageous effect of treatment based on sodium-glucose cotransporter 2 inhibitors in COVID-19. A series from Italy has reported the lack of an influence of empagliflozin on clinical outcomes in severe pneumonia caused by SARS-CoV-2 in three nondiabetic patients [98]. Another retrospective analysis has shown that prior treatment with gliflozins in diabetic patients is associated with a lower risk of mechanical ventilation [66]. The benefits of SGLT2i treatment during COVID-19 remain unknown and are currently being investigated in the Dapagliflozin in Respiratory Failure in Patients with COVID-19 (DARE-19) trial [99].
However, SGLT2 inhibitors may cause euglycaemic diabetic ketoacidosis (DKA), especially in patients with severe acute disorder, dehydration or acute kidney injury [100], and are therefore not recommended for diabetic patients with a moderate or severe course of COVID-19 [101]. In addition, SARS-CoV-2 infection may cause acidosis, ketoacidosis and diabetic ketoacidosis for patients with diabetes [102]. The possible risk of DKA during gliflozin treatment should not be ignored, and some caution is necessary. The results of the aforementioned DARE-19 trial will provide a better understanding of the clinical consequences of the use of sodium-glucose cotransporter 2 inhibitors during COVID-19.
3.4. Metformin in COVID-19
Metformin is one of the most commonly used antidiabetic drugs; because of its widespread use, the impact of metformin therapy on the course of COVID-19 is particularly important.
It has been confirmed that metformin has some anti-inflammatory [103] and anti-thrombotic [104] properties, which may prevent the development of cytokine storms or thromboembolic events. This last claim is supported by research, in which metformin treatment was associated with a reduced risk of deep-vein thrombosis in type 2 diabetes [105], or by studies which have proved the ability of metformin to protect platelets against activation and to prevent extracellular mitochondrial DNA from being released [106]. Furthermore, this molecule shows protective properties towards the endothelium, reducing oxidative stress and inflammation [107]. Moreover, it is suggested that metformin might stop the virus from entering target cells by activating AMPK or via the PI3K/Akt signalling pathway [108].
Metformin use has been reported to decrease mortality in T2DM patients with COVID-19 [17,109,110,111]. In the CORONADO trial, regarding all available antidiabetic medications, only metformin treatment showed a reduced rate of death [17]. In a multicentre retrospective study, it has been shown that metformin treatment prior to admission to hospital was correlated with a decreased intensive care unit admission rate in a dose-dependent fashion [112]. In contrast, in a retrospective study, it was indicated that metformin therapy is associated with an increased severity of COVID-19 infection and with a higher number of life-threatening complications [113]; however, in another systematic review, it was shown that metformin might improve the clinical outcomes in diabetic patients with a mild to severe course of COVID-19 [114]. Treatment with metformin has also been proven to promote acidosis, but not mortality, in diabetic patients infected with SARS-CoV-2 [115] and it was initially suggested to avoid metformin treatment in patients suffering from COVID-19 with coexisting DM [101,116,117]. However, researchers have since pointed out the potential benefits of this method for diabetes management [118]. Of note, metformin is still contraindicated in patients with a high risk of acidosis [119] or acute respiratory distress syndrome [116] and watchfulness is required during the continuation of therapy. Unclear evidence should be investigated in further trials to clarify the exact role of metformin in COVID-19.
3.5. Thiazolidinediones in COVID-19
Pioglitazone, an example of thiazolidinediones, is an agonist of a nuclear peroxisome proliferator-activated receptor-γ (PPARγ), which is involved in the regulation of the transcription of genes related to glucose and lipid metabolism [120]. It has shown anti-inflammatory activity [121]. Pioglitazone may reduce the secretion of some proinflammatory cytokines in leukocytes, such as monocytes or macrophages [122], as well as it exhibiting the property of blocking caspase recruitment domain-containing protein 9 in macrophages, thus weakening cytokine storms [123]. Moreover, bioinformatic analysis carried out by Wu et al. has shown that pioglitazone probably inhibits RNA synthesis and the replication of SARS-CoV-2 by affecting 3-chymotrypsin-like protease [124]. However, therapy based on pioglitazone was associated with weight gain, fluid retention, oedema and aggravation of heart failure, so it is not recommended for critically ill patients, including patients with COVID-19 [125,126].
3.6. Insulin in COVID-19
Insulin treatment has been suggested as a preferable method of diabetes management during the COVID-19 pandemic for critically ill diabetic patients with the infection [71]. Insulin has been reported to downregulate ACE2 receptors in a diabetic mouse model [127], which may hypothetically reduce the risk of infection of SARS-CoV-2. Furthermore, treatment based on intravenous insulin infusion, leading to optimal glycaemia control in patients with T2DM and COVID-19, seems to have a positive effect on inflammation and coagulation, and may be an effective method for achieving specified glycaemic targets [128]. Of note, patients suffering from SARS-CoV-2 infection require significantly higher insulin doses [101], which may be explained by the dysfunction of beta-cells or the high inflammatory process induced by the virus.
It has been reported that patients with COVID-19 who use insulin have a higher risk of poor prognosis than noninsulin users [63]. Moreover, insulin treatment in hospitalised patients has been linked to increased invasive ventilation [112]. However, it should be noted that these groups might have been incomparable, as insulin is usually the only recommended treatment in the severe course of infections and because in an advanced stage of diabetes with some comorbidities other glucose-lowering medications are contraindicated [63]. On the other hand, in the aforementioned CORONADO study, therapy based on insulin was not associated with death [17]. Treatment with subcutaneous insulin has also shown favourable results in uncomplicated diabetic ketoacidosis during the COVID-19 pandemic [129]. Further research is needed to define the exact role of insulin in the course of COVID-19.
A summary of antidiabetic drugs, their mechanisms of action and their possible influence on the course of COVID-19 is presented in Table 1.
4. Recommendations on Diabetes Treatment during the Pandemic
It has been proven that poor glycaemic control has a negative impact on prognosis and on the risk of any infections for both uninfected and infected people; thus, the strict management of diabetes is vital [130]. Although there is a lot of consideration about hypothetically increased susceptibility to COVID-19 during particular antidiabetic treatments in uninfected patients, no evidence confirming these assumptions is available, so treatment based on the usual glucose-lowering medications taken previously is recommended [117,131]. It is of crucial importance to intensify the metabolic control of diabetes by uninfected people as a method of the primary prevention of COVID-19 [101]. According to the guidelines of the American Diabetes Association for the year 2021, HbA1c <7% (53 mmol/mol) without significant hypoglycaemia is recommended. For patients with limited life expectancy or in a situation when the harms of treatment are greater than the benefits, HbA1c <8% (64 mmol/mol) may be appropriate. The use of continuous glucose monitoring devices should be also considered in patients with type 2 diabetes with multiple daily injections and other forms of insulin therapy, especially in those with a high risk of hypoglycaemia. Because an increased time in range is associated with the risk of microvascular complications, a goal is a time in range >70% (70–180 mg/dL, 3.9–10.0 mmol/L) with time below target <4% (<70 mg/dL, <3.9 mmol/L). Patients with cardiovascular disease and type 2 diabetes benefit from glucose-lowering therapies with an SGLT2 inhibitor or a GLP-1 receptor agonist. Moreover, in the current situation, people with diabetes should be a priority population for vaccinations. Routine vaccinations for SARS-CoV-2 infection and influenza prevent morbidity and reduce hospitalisations and are strongly recommended [132].
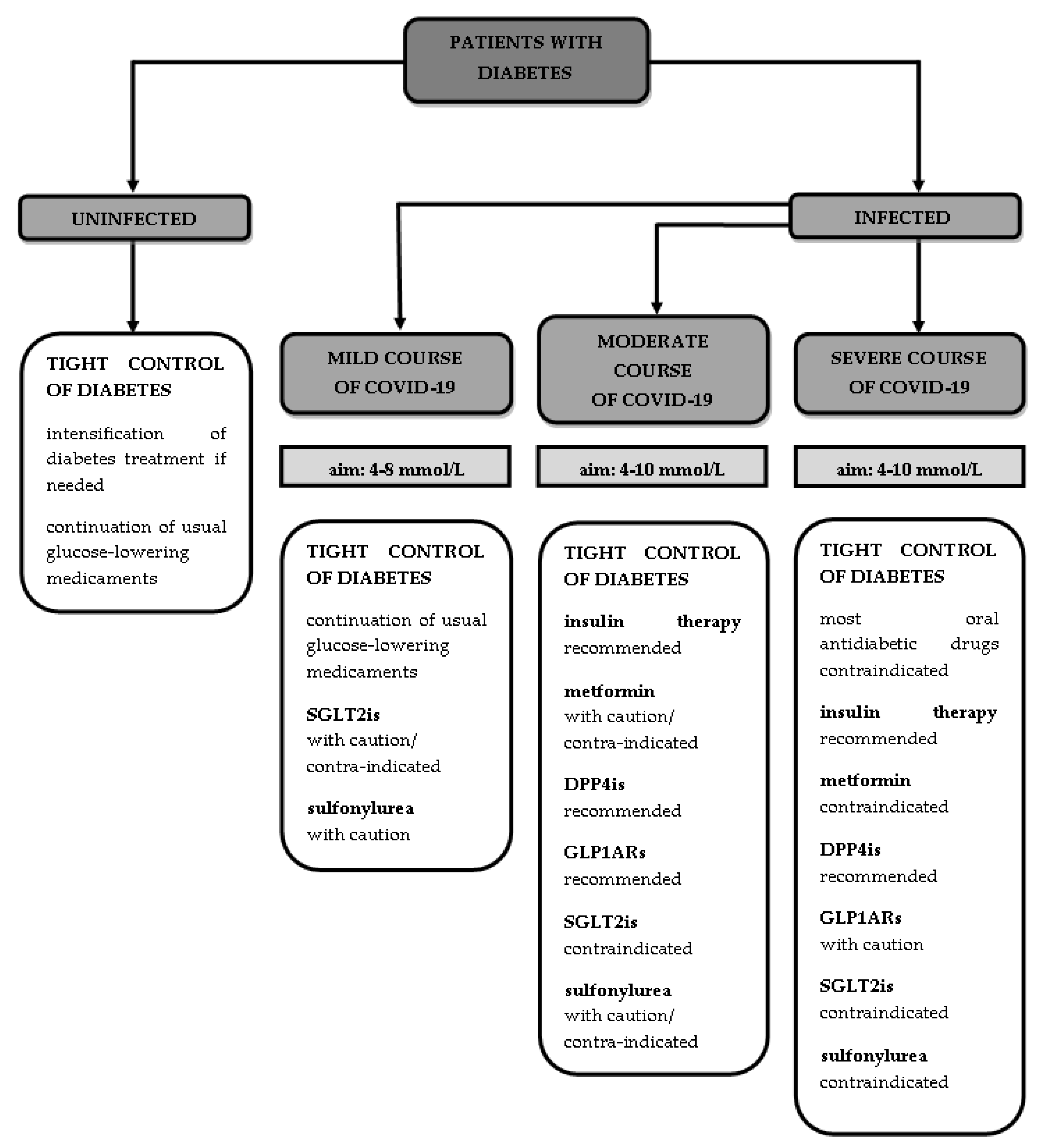
It is also important to monitor glucose levels and to treat worsening hyperglycaemia in patients with COVID-19. According to a Chinese retrospective study, fasting glucose levels ≥126 mg/dL at admission were an independent predictor of increased mortality in patients with SARS-CoV-2 infection and without diabetes [133]. A retrospective exploratory study using continuous glucose monitoring has shown that patients with diabetes and COVID-19 have an increased risk of adverse outcomes and prolonged hospitalisation with glucose levels >160 mg/dL and <70 mg/dL and a high coefficient of variation [134]. Regarding diabetic patients infected with SARS-CoV-2 who are at risk of metabolic decompensation in the form diabetic ketoacidosis or a hyperosmolar hyperglycaemic state, clinicians should take notice of the tight control of diabetes [116]. The therapeutic aims in terms of plasma glucose concentrations during the infection are 4–8 mmol/L (72–144 mg/dL) in patients under ambulatory control and 4–10 mmol/L (72–180 mg/dL) in hospitalised patients [101].
During the mild course of COVID-19, it is necessary to continue the anti-diabetic treatment prescribed before the infection with one exception—SGLT2is, which may potentially cause dehydration or lead to euglycaemic diabetic ketoacidosis [135], but some authors allow their use with caution in a mild ambulatory course [3]. It is possible to follow treatment based on sulfonylurea but careful adjustment of the patient’s actual food intake and risk of hypoglycaemia should be performed [117].
Regarding patients with a moderate or severe course of the infection, who should be hospitalised, treatment based on insulin seems to be a good option to maintain target glycaemia levels. Despite the fact that insulin therapy is correlated with a poor prognosis [63], it is still the main way to lower blood glucose levels in hospitalised patients, as most oral antidiabetic drugs are contraindicated [79,101] and tight diabetes control is required. It is not recommended to continue metformin treatment during the hospitalisation of patients with a moderate or severe course of COVID-19, because of the possibility of triggering lactic acidosis, especially under conditions of hypoxia [101]; however, some authors permit the use of metformin in hospitalised people with moderate disease with adequate caution, highlighting its anti-inflammatory properties [135]. The authors of a few guidelines propose continuing treatment based on DPP4 inhibitors, as there is no evidence of the need to discontinue the supply of this type of drug and they may be used safely in a broad spectrum of severity of the disease [101,135]. Similar recommendations have been made considering the use of GLP1 analogues [101,135]. During the hospitalisation of patients with moderate or severe COVID-19, SGLT2 inhibitors are strongly not recommended due to the risk of diabetic ketoacidosis, dehydration and acute kidney injury, as well as sulfonylurea because of the risk of severe hypoglycaemia, especially under in the presence of a loss of appetite or irregular food intake, which characterises the course of SARS-CoV-2 infection [101,135]. A short summary of the recommendations on diabetes treatment during the COVID-19 pandemic is presented in Figure 2.
5. Conclusions
COVID-19 is a new, not fully understood, disease which has affected a large number of people worldwide. The widespread occurrence of SARS-CoV-2 and its high infectiousness mean that the attention of scientists should be turned to better understanding the pathophysiology underlying COVID-19 and its impact on coexisting diseases. Antidiabetic drugs, used not only during asymptomatic or mild SARS-CoV-2 infection, but also within the severe course of the disease, can influence the pathophysiological mechanisms of COVID-19 and affect disease prognosis. Because of the high incidence of diabetes, it is of crucial importance to consider the relationship between SARS-CoV-2 infection and impaired glucose metabolism and to establish the most advantageous way to manage diabetes during the infection, which may prevent worse outcomes in these patients in the future.
Funding
The project was financed through the program of the Minister of Science and Higher Education under the name “Regional Initiative of Excellence” in 2019–2022 project number 002/RID/2018/19.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declare no conflict of interest.
References
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Chowdhury, T.A. Diabetes and COVID-19: Diseases of racial, social and glucose intolerance. World J. Diabetes 2021, 12, 198–205. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhang, Z.; Yang, L.; Lian, X.; Xie, Y.; Li, S.; Xin, S.; Cao, P.; Lu, J. The MERS-CoV Receptor DPP4 as a Candidate Binding Target of the SARS-CoV-2 Spike. iScience 2020, 23, 101160. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Codo, A.C.; Davanzo, G.G.; Monteiro, L.B.; de Souza, G.F.; Muraro, S.P.; Virgilio-da-Silva, J.V.; Prodonoff, J.S.; Carregari, V.C.; de Biagi Junior, C.A.O.; Crunfli, F.; et al. Elevated Glucose Levels Favor SARS-CoV-2 Infection and Monocyte Response through a HIF-1α/Glycolysis-Dependent Axis. Cell Metab. 2020, 32, 498–499. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Girgis, C.M.; Cheung, N.W. COVID-19 and diabetes: Insulin requirements parallel illness severity in critically unwell patients. Clin. Endocrinol. 2020, 93, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Groop, L.C.; Bonadonna, R.C.; DelPrato, S.; Ratheiser, K.; Zyck, K.; Ferrannini, E.; DeFronzo, R.A. Glucose and free fatty acid metabolism in non-insulin-dependent diabetes mellitus. Evidence for multiple sites of insulin resistance. J. Clin. Investig. 1989, 84, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Eketunde, A.O.; Mellacheruvu, S.P.; Oreoluwa, P. A Review of Postmortem Findings in Patients with COVID-19. Cureus 2020, 12, e9438. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, e3319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lew, T.W.; Kwek, T.K.; Tai, D.; Earnest, A.; Loo, S.; Singh, K.; Kwan, K.M.; Chan, Y.; Yim, C.F.; Bek, S.L.; et al. Acute respiratory distress syndrome in critically ill patients with severe acute respiratory syndrome. JAMA 2003, 290, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal changes of inflammatory parameters and their correlation with disease severity and outcomes in patients with COVID-19 from Wuhan, China. Crit. Care 2020, 24, 525. [Google Scholar] [CrossRef]
- Libby, P.; Simon, D.I. Inflammation and thrombosis: The clot thickens. Circulation 2001, 103, 1718–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheema, A.K.; Kaur, P.; Fadel, A.; Younes, N.; Zirie, M.; Rizk, N.M. Integrated Datasets of Proteomic and Metabolomic Biomarkers to Predict Its Impacts on Comorbidities of Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2020, 13, 2409–2431. [Google Scholar] [CrossRef] [PubMed]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef]
- Zheng, M.; Wang, X.; Guo, H.; Fan, Y.; Song, Z.; Lu, Z.; Wang, J.; Zheng, C.; Dong, L.; Ma, Y.; et al. The Cytokine Profiles and Immune Response Are Increased in COVID-19 Patients with Type 2 Diabetes Mellitus. J. Diabetes Res. 2021, 2021, 9526701. [Google Scholar] [CrossRef] [PubMed]
- Wensveen, F.M.; Jelenčić, V.; Valentić, S.; Šestan, M.; Wensveen, T.T.; Theurich, S.; Glasner, A.; Mendrila, D.; Štimac, D.; Wunderlich, F.T.; et al. NK cells link obesity-induced adipose stress to inflammation and insulin resistance. Nat. Immunol. 2015, 16, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, K.; Lee, S.B.; Kang, S.; Park, J.S.; Ahn, C.W.; Nam, J.S. Relationship between natural killer cell activity and glucose control in patients with type 2 diabetes and prediabetes. J. Diabetes Investig. 2019, 10, 1223–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection. Eur. J. Intern. Med. 2020, 76, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Stavrou, E.; Schmaier, A.A.; Grobe, N.; Morris, M.; Chen, A.; Nieman, M.T.; Adams, G.N.; LaRusch, G.; Zhou, Y.; et al. Angiotensin 1-7 and Mas decrease thrombosis in Bdkrb2−/− mice by increasing NO and prostacyclin to reduce platelet spreading and glycoprotein VI activation. Blood 2013, 121, 3023–3032. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/MAS Axis of the Renin-Angiotensin System: Focus on Angiotensin-(1-7). Physiol. Rev. 2018, 98, 505–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benigni, A.; Cassis, P.; Remuzzi, G. Angiotensin II revisited: New roles in inflammation, immunology and aging. EMBO Mol. Med. 2010, 2, 247–257. [Google Scholar] [CrossRef]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef]
- Wang, L.; Liang, J.; Leung, P.S. The ACE2/Ang-(1-7)/Mas Axis Regulates the Development of Pancreatic Endocrine Cells in Mouse Embryos. PLoS ONE 2015, 10, e0128216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brufsky, A. Hyperglycemia, hydroxychloroquine, and the COVID-19 pandemic. J. Med. Virol. 2020, 92, 770–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.K.; Lin, S.S.; Ji, X.J.; Guo, L.M. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol. 2010, 47, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Accili, D. Can COVID-19 cause diabetes? Nat. Metab. 2021, 3, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.Z.; Li, H.L. COVID-19: Attacks the 1-β chain of hemoglobin and captures the porphyrin to inhibit human heme metabolism. ChemRxiv 2020. [Google Scholar] [CrossRef]
- Cheng, L.; Qin, T.; Ma, J.; Duan, W.; Xu, Q.; Li, X.; Han, L.; Li, W.; Wang, Z.; Zhang, D.; et al. Hypoxia-inducible Factor-1α Mediates Hyperglycemia-induced Pancreatic Cancer Glycolysis. Anticancer Agents Med. Chem. 2019, 19, 1503–1512. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, G.; Xu, Z.G.; Tu, H.; Hu, F.; Dai, J.; Chang, Y.; Chen, Y.; Lu, Y.; Zeng, H.; et al. Lactate Is a Natural Suppressor of RLR Signaling by Targeting MAVS. Cell 2019, 178, 176–189.e15. [Google Scholar] [CrossRef]
- Wang, J.; Meng, W. COVID-19 and diabetes: The contributions of hyperglycemia. J. Mol. Cell Biol. 2021, 12, 958–962. [Google Scholar] [CrossRef]
- Lambeir, A.M.; Durinx, C.; Scharpé, S.; De Meester, I. Dipeptidyl-peptidase IV from bench to bedside: An update on structural properties, functions, and clinical aspects of the enzyme DPP IV. Crit. Rev. Clin. Lab. Sci. 2003, 40, 209–294. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. The biology of incretin hormones. Cell Metab. 2006, 3, 153–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassendine, M.F.; Bridge, S.H.; McCaughan, G.W.; Gorrell, M.D. COVID-19 and comorbidities: A role for dipeptidyl peptidase 4 (DPP4) in disease severity? J. Diabetes 2020, 12, 649–658. [Google Scholar] [CrossRef]
- Klemann, C.; Wagner, L.; Stephan, M.; von Hörsten, S. Cut to the chase: A review of CD26/dipeptidyl peptidase-4′s (DPP4) entanglement in the immune system. Clin. Exp. Immunol. 2016, 185, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Röhrborn, D.; Wronkowitz, N.; Eckel, J. DPP4 in Diabetes. Front. Immunol. 2015, 6, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raj, V.S.; Smits, S.L.; Provacia, L.B.; van den Brand, J.M.; Wiersma, L.; Ouwendijk, W.J.; Bestebroer, T.M.; Spronken, M.I.; van Amerongen, G.; Rottier, P.J.; et al. Adenosine deaminase acts as a natural antagonist for dipeptidyl peptidase 4-mediated entry of the Middle East respiratory syndrome coronavirus. J. Virol. 2014, 88, 1834–1838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, S.; Xu, Q.; Yu, X.; Pan, R.; Chen, Y. Dipeptidyl peptidase 4 inhibitors and their potential immune modulatory functions. Pharmacol. Ther. 2020, 209, 107503. [Google Scholar] [CrossRef] [PubMed]
- Raj, V.S.; Mou, H.; Smits, S.L.; Dekkers, D.H.; Müller, M.A.; Dijkman, R.; Muth, D.; Demmers, J.A.; Zaki, A.; Fouchier, R.A.; et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature 2013, 495, 251–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vankadari, N.; Wilce, J.A. Emerging WuHan (COVID-19) coronavirus: Glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26. Emerg. Microbes Infect. 2020, 9, 601–604. [Google Scholar] [CrossRef]
- Krejner-Bienias, A.; Grzela, K.; Grzela, T. DPP4 Inhibitors and COVID-19-Holy Grail or Another Dead End? Arch. Immunol. Ther. Exp. 2021, 69, 1. [Google Scholar] [CrossRef]
- Yu, D.M.; Slaitini, L.; Gysbers, V.; Riekhoff, A.G.; Kähne, T.; Knott, H.M.; De Meester, I.; Abbott, C.A.; McCaughan, G.W.; Gorrell, M.D. Soluble CD26/dipeptidyl peptidase IV enhances human lymphocyte proliferation in vitro independent of dipeptidyl peptidase enzyme activity and adenosine deaminase binding. Scand. J. Immunol. 2011, 73, 102–111. [Google Scholar] [CrossRef]
- Inn, K.S.; Kim, Y.; Aigerim, A.; Park, U.; Hwang, E.S.; Choi, M.S.; Kim, Y.S.; Cho, N.H. Reduction of soluble dipeptidyl peptidase 4 levels in plasma of patients infected with Middle East respiratory syndrome coronavirus. Virology 2018, 518, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Schlicht, K.; Rohmann, N.; Geisler, C.; Hollstein, T.; Knappe, C.; Hartmann, K.; Schwarz, J.; Tran, F.; Schunk, D.; Junker, R.; et al. Circulating levels of soluble Dipeptidylpeptidase-4 are reduced in human subjects hospitalized for severe COVID-19 infections. Int. J. Obes. 2020, 44, 2335–2338. [Google Scholar] [CrossRef] [PubMed]
- Gallwitz, B. Clinical Use of DPP-4 Inhibitors. Front. Endocrinol. 2019, 10, 389. [Google Scholar] [CrossRef]
- Krejner-Bienias, A.; Grzela, K.; Grzela, T. Do novel drugs for diabetes help in COVID-19? Another brick in the wall? J. Diabetes 2020, 12, 703–704. [Google Scholar] [CrossRef]
- Solerte, S.B.; Di Sabatino, A.; Galli, M.; Fiorina, P. Dipeptidyl peptidase-4 (DPP4) inhibition in COVID-19. Acta Diabetol. 2020, 57, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Trzaskalski, N.A.; Fadzeyeva, E.; Mulvihill, E.E. Dipeptidyl Peptidase-4 at the Interface between Inflammation and Metabolism. Clin. Med. Insights Endocrinol. Diabetes 2020, 13, 1179551420912972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsubara, J.; Sugiyama, S.; Akiyama, E.; Iwashita, S.; Kurokawa, H.; Ohba, K.; Maeda, H.; Fujisue, K.; Yamamoto, E.; Kaikita, K.; et al. Dipeptidyl peptidase-4 inhibitor, sitagliptin, improves endothelial dysfunction in association with its anti-inflammatory effects in patients with coronary artery disease and uncontrolled diabetes. Circ. J. 2013, 77, 1337–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh-Asahara, N.; Sasaki, Y.; Wada, H.; Tochiya, M.; Iguchi, A.; Nakagawachi, R.; Odori, S.; Kono, S.; Hasegawa, K.; Shimatsu, A. A dipeptidyl peptidase-4 inhibitor, sitagliptin, exerts anti-inflammatory effects in type 2 diabetic patients. Metabolism 2013, 62, 347–351. [Google Scholar] [CrossRef]
- Arulmozhiraja, S.; Matsuo, N.; Ishitsubo, E.; Okazaki, S.; Shimano, H.; Tokiwa, H. Comparative Binding Analysis of Dipeptidyl Peptidase IV (DPP-4) with Antidiabetic Drugs—An Ab Initio Fragment Molecular Orbital Study. PLoS ONE 2016, 11, e0166275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardaweel, S.K.; Hajjo, R.; Sabbah, D.A. Sitagliptin: A potential drug for the treatment of COVID-19? Acta Pharm. 2021, 71, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Takagaki, Y.; Shi, S.; Katoh, M.; Kitada, M.; Kanasaki, K.; Koya, D. Dipeptidyl peptidase-4 plays a pathogenic role in BSA-induced kidney injury in diabetic mice. Sci. Rep. 2019, 9, 7519. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Cai, X.; Han, X.; Ji, L. DPP-4 inhibitors and risk of infections: A meta-analysis of randomized controlled trials. Diabetes Metab. Res. Rev. 2016, 32, 391–404. [Google Scholar] [CrossRef] [Green Version]
- Vora, K.A.; Porter, G.; Peng, R.; Cui, Y.; Pryor, K.; Eiermann, G.; Zaller, D.M. Genetic ablation or pharmacological blockade of dipeptidyl peptidase IV does not impact T cell-dependent immune responses. BMC Immunol. 2009, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Price, J.D.; Linder, G.; Li, W.P.; Zimmermann, B.; Rother, K.I.; Malek, R.; Alattar, M.; Tarbell, K.V. Effects of short-term sitagliptin treatment on immune parameters in healthy individuals, a randomized placebo-controlled study. Clin. Exp. Immunol. 2013, 174, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Sromova, L.; Busek, P.; Posova, H.; Potockova, J.; Skrha, P.; Andel, M.; Sedo, A. The effect of dipeptidyl peptidase-IV inhibition on circulating T cell subpopulations in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2016, 118, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Solerte, S.B.; D’Addio, F.; Trevisan, R.; Lovati, E.; Rossi, A.; Pastore, I.; Dell’Acqua, M.; Ippolito, E.; Scaranna, C.; Bellante, R.; et al. Sitagliptin Treatment at the Time of Hospitalization Was Associated With Reduced Mortality in Patients With Type 2 Diabetes and COVID-19: A Multicenter, Case-Control, Retrospective, Observational Study. Diabetes Care 2020, 43, 2999–3006. [Google Scholar] [CrossRef]
- Mirani, M.; Favacchio, G.; Carrone, F.; Betella, N.; Biamonte, E.; Morenghi, E.; Mazziotti, G.; Lania, A.G. Impact of Comorbidities and Glycemia at Admission and Dipeptidyl Peptidase 4 Inhibitors in Patients With Type 2 Diabetes With COVID-19: A Case Series From an Academic Hospital in Lombardy, Italy. Diabetes Care 2020, 43, 3042–3049. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, D.; Cheng, B.; Chen, J.; Peng, A.; Yang, C.; Liu, C.; Xiong, M.; Deng, A.; Zhang, Y.; et al. Clinical Characteristics and Outcomes of Patients With Diabetes and COVID-19 in Association With Glucose-Lowering Medication. Diabetes Care 2020, 43, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Morieri, M.L.; Longato, E.; Bonora, B.M.; Pinelli, S.; Selmin, E.; Voltan, G.; Falaguasta, D.; Tresso, S.; Costantini, G.; et al. Exposure to dipeptidyl-peptidase-4 inhibitors and COVID-19 among people with type 2 diabetes: A case-control study. Diabetes Obes. Metab. 2020, 22, 1946–1950. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J.; Marre, M.; Thivolet, C. Prognostic factors in patients with diabetes hospitalized for COVID-19: Findings from the CORONADO study and other recent reports. Diabetes Metab. 2020, 46, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Dalan, R.; Ang, L.W.; Tan, W.Y.T.; Fong, S.W.; Tay, W.C.; Chan, Y.H.; Renia, L.; Ng, L.F.P.; Lye, D.C.; Chew, D.E.K.; et al. The association of hypertension and diabetes pharmacotherapy with COVID-19 severity and immune signatures: An observational study. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, e48–e51. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Mukherjee, S.; Bhogal, R.S.; Kaur, A.; Bhadada, S.K. Dipeptidyl peptidase-4 inhibitor use and mortality in COVID-19 patients with diabetes mellitus: An updated systematic review and meta-analysis. Ther. Adv. Endocrinol. Metab. 2021, 12, 2042018821996482. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.; Lund, A.; Knop, F.K.; Vilsbøll, T. Glucagon-like peptide 1 in health and disease. Nat. Rev. Endocrinol. 2018, 14, 390–403. [Google Scholar] [CrossRef]
- Ceriello, A.; Novials, A.; Ortega, E.; Canivell, S.; La Sala, L.; Pujadas, G.; Esposito, K.; Giugliano, D.; Genovese, S. Glucagon-like peptide 1 reduces endothelial dysfunction, inflammation, and oxidative stress induced by both hyperglycemia and hypoglycemia in type 1 diabetes. Diabetes Care 2013, 36, 2346–2350. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Jun, H.S. Anti-Inflammatory Effects of GLP-1-Based Therapies beyond Glucose Control. Mediat. Inflamm. 2016, 2016, 3094642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drucker, D.J. Coronavirus Infections and Type 2 Diabetes-Shared Pathways with Therapeutic Implications. Endocr. Rev. 2020, 41, bnaa011. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Puccio, L.; Foti, D.P.; Brunetti, A. Potential Benefits and Harms of Novel Antidiabetic Drugs During COVID-19 Crisis. Int. J. Environ. Res. Public Health 2020, 17, 3664. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Kim, K.M.; Nauck, M.A. Glucagon-like Peptide-1 Receptor Agonists and Cardiovascular Events: Class Effects versus Individual Patterns. Trends Endocrinol. Metab. 2018, 29, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Dear, A.E.; Knudsen, L.B.; Simpson, R.W. A long-acting glucagon-like peptide-1 analogue attenuates induction of plasminogen activator inhibitor type-1 and vascular adhesion molecules. J. Endocrinol. 2009, 201, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Bloodworth, M.H.; Rusznak, M.; Pfister, C.C.; Zhang, J.; Bastarache, L.; Calvillo, S.A.; Chappell, J.D.; Boyd, K.L.; Toki, S.; Newcomb, D.C.; et al. Glucagon-like peptide 1 receptor signaling attenuates respiratory syncytial virus-induced type 2 responses and immunopathology. J. Allergy Clin. Immunol. 2018, 142, 683–687.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steven, S.; Hausding, M.; Kröller-Schön, S.; Mader, M.; Mikhed, Y.; Stamm, P.; Zinßius, E.; Pfeffer, A.; Welschof, P.; Agdauletova, S.; et al. Gliptin and GLP-1 analog treatment improves survival and vascular inflammation/dysfunction in animals with lipopolysaccharide-induced endotoxemia. Basic Res. Cardiol. 2015, 110, 6. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Rashidy-Pour, A.; Atkin, S.L.; Jamialahmadi, T.; Sahebkar, A. GLP-1 mimetics and cognition. Life Sci. 2021, 264, 118645. [Google Scholar] [CrossRef]
- Carbone, L.J.; Angus, P.W.; Yeomans, N.D. Incretin-based therapies for the treatment of non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Bhadada, S.K. Should anti-diabetic medications be reconsidered amid COVID-19 pandemic? Diabetes Res. Clin. Pract. 2020, 163, 108146. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.V.; Pfeffer, M.A.; Solomon, S.D. Renin-Angiotensin-Aldosterone System Inhibitors in Patients with Covid-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Wösten-van Asperen, R.M.; Lutter, R.; Specht, P.A.; Moll, G.N.; van Woensel, J.B.; van der Loos, C.M.; van Goor, H.; Kamilic, J.; Florquin, S.; Bos, A.P. Acute respiratory distress syndrome leads to reduced ratio of ACE/ACE2 activities and is prevented by angiotensin-(1-7) or an angiotensin II receptor antagonist. J. Pathol. 2011, 225, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Jiang, C.; Penninger, J.M. Lessons from SARS: Control of acute lung failure by the SARS receptor ACE2. J. Mol. Med. 2006, 84, 814–820. [Google Scholar] [CrossRef]
- Romaní-Pérez, M.; Outeiriño-Iglesias, V.; Moya, C.M.; Santisteban, P.; González-Matías, L.C.; Vigo, E.; Mallo, F. Activation of the GLP-1 Receptor by Liraglutide Increases ACE2 Expression, Reversing Right Ventricle Hypertrophy, and Improving the Production of SP-A and SP-B in the Lungs of Type 1 Diabetes Rats. Endocrinology 2015, 156, 3559–3569. [Google Scholar] [CrossRef] [PubMed]
- Fandiño, J.; Vaz, A.A.; Toba, L.; Romaní-Pérez, M.; González-Matías, L.; Mallo, F.; Diz-Chaves, Y. Liraglutide Enhances the Activity of the ACE-2/Ang(1-7)/Mas Receptor Pathway in Lungs of Male Pups from Food-Restricted Mothers and Prevents the Reduction of SP-A. Int. J. Endocrinol. 2018, 2018, 6920620. [Google Scholar] [CrossRef] [PubMed]
- Monda, V.M.; Porcellati, F.; Strollo, F.; Gentile, S. ACE2 and SARS-CoV-2 Infection: Might GLP-1 Receptor Agonists Play a Role? Diabetes Ther. 2020, 11, 1909–1914. [Google Scholar] [CrossRef]
- Nauck, M.A.; Meier, J.J.; Cavender, M.A.; Abd El Aziz, M.; Drucker, D.J. Cardiovascular Actions and Clinical Outcomes With Glucagon-Like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors. Circulation 2017, 136, 849–870. [Google Scholar] [CrossRef] [PubMed]
- Prattichizzo, F.; La Sala, L.; Rydén, L.; Marx, N.; Ferrini, M.; Valensi, P.; Ceriello, A. Glucose-lowering therapies in patients with type 2 diabetes and cardiovascular diseases. Eur. J. Prev. Cardiol. 2019, 26, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, O.G.; Whyte, M.B. The use of GLP-1 receptor agonists in hospitalised patients: An untapped potential. Diabetes Metab. Res. Rev. 2019, 35, e3191. [Google Scholar] [CrossRef] [Green Version]
- Nauck, M.A.; Meier, J.J. MANAGEMENT OF ENDOCRINE DISEASE: Are all GLP-1 agonists equal in the treatment of type 2 diabetes? Eur. J. Endocrinol. 2019, 181, R211–R234. [Google Scholar] [CrossRef]
- Cure, E.; Cumhur Cure, M. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may be harmful in patients with diabetes during COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 349–350. [Google Scholar] [CrossRef]
- Bonnet, F.; Scheen, A.J. Effects of SGLT2 inhibitors on systemic and tissue low-grade inflammation: The potential contribution to diabetes complications and cardiovascular disease. Diabetes Metab. 2018, 44, 457–464. [Google Scholar] [CrossRef]
- Dekkers, C.C.J.; Petrykiv, S.; Laverman, G.D.; Cherney, D.Z.; Gansevoort, R.T.; Heerspink, H.J.L. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes. Metab. 2018, 20, 1988–1993. [Google Scholar] [CrossRef] [Green Version]
- Garvey, W.T.; Van Gaal, L.; Leiter, L.A.; Vijapurkar, U.; List, J.; Cuddihy, R.; Ren, J.; Davies, M.J. Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type 2 diabetes. Metabolism 2018, 85, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Cure, E.; Cumhur Cure, M. Can dapagliflozin have a protective effect against COVID-19 infection? A hypothesis. Diabetes Metab. Syndr. 2020, 14, 405–406. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minze, M.G.; Will, K.J.; Terrell, B.T.; Black, R.L.; Irons, B.K. Benefits of SGLT2 Inhibitors Beyond Glycemic Control—A Focus on Metabolic, Cardiovascular and Renal Outcomes. Curr. Diabetes Rev. 2018, 14, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Bossi, A.C.; Forloni, F.; Colombelli, P.L. Lack of Efficacy of SGLT2-i in Severe Pneumonia Related to Novel Coronavirus (nCoV) Infection: No Little Help from Our Friends. Diabetes Ther. 2020, 11, 1605–1606. [Google Scholar] [CrossRef] [PubMed]
- Kosiborod, M.; Berwanger, O.; Koch, G.G.; Martinez, F.; Mukhtar, O.; Verma, S.; Chopra, V.; Javaheri, A.; Ambery, P.; Gasparyan, S.B.; et al. Effects of dapagliflozin on prevention of major clinical events and recovery in patients with respiratory failure because of COVID-19: Design and rationale for the DARE-19 study. Diabetes Obes. Metab. 2021, 23, 886–896. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.; Ejaz, A.A.; Kanbay, M.; Lanaspa, M.A.; Johnson, R.J. Acute kidney injury from SGLT2 inhibitors: Potential mechanisms. Nat. Rev. Nephrol. 2016, 12, 711–712. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Rubino, F.; Khunti, K.; Mingrone, G.; Hopkins, D.; Birkenfeld, A.L.; Boehm, B.; Amiel, S.; Holt, R.I.; Skyler, J.S.; et al. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol. 2020, 8, 546–550. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Zuo, X.; Zhang, H.; Deng, A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes. Metab. 2020, 22, 1935–1941. [Google Scholar] [CrossRef]
- Cameron, A.R.; Morrison, V.L.; Levin, D.; Mohan, M.; Forteath, C.; Beall, C.; McNeilly, A.D.; Balfour, D.J.; Savinko, T.; Wong, A.K.; et al. Anti-Inflammatory Effects of Metformin Irrespective of Diabetes Status. Circ. Res. 2016, 119, 652–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, P.J. The effects of metformin on the fibrinolytic system in diabetic and non-diabetic subjects. Diabete Metab. 1991, 17, 168–173. [Google Scholar] [PubMed]
- Lu, D.Y.; Huang, C.C.; Huang, P.H.; Chung, C.M.; Lin, S.J.; Chen, J.W.; Chan, W.L.; Leu, H.B. Metformin use in patients with type 2 diabetes mellitus is associated with reduced risk of deep vein thrombosis: A non-randomized, pair-matched cohort study. BMC Cardiovasc. Disord. 2014, 14, 187. [Google Scholar] [CrossRef] [Green Version]
- Xin, G.; Wei, Z.; Ji, C.; Zheng, H.; Gu, J.; Ma, L.; Huang, W.; Morris-Natschke, S.L.; Yeh, J.L.; Zhang, R.; et al. Metformin Uniquely Prevents Thrombosis by Inhibiting Platelet Activation and mtDNA Release. Sci. Rep. 2016, 6, 36222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triggle, C.R.; Ding, H. Metformin is not just an antihyperglycaemic drug but also has protective effects on the vascular endothelium. Acta Physiol. 2017, 219, 138–151. [Google Scholar] [CrossRef]
- Flory, J.H.; Hennessy, S.; Bailey, C.J.; Inzucchi, S.E. Reports of Lactic Acidosis Attributed to Metformin, 2015–2018. Diabetes Care 2020, 43, 244–246. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Metformin use is associated with reduced mortality rate from coronavirus disease 2019 (COVID-19) infection. Obes. Med. 2020, 19, 100290. [Google Scholar] [CrossRef] [PubMed]
- Lukito, A.A.; Pranata, R.; Henrina, J.; Lim, M.A.; Lawrensia, S.; Suastika, K. The Effect of Metformin Consumption on Mortality in Hospitalized COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2020, 14, 2177–2183. [Google Scholar] [CrossRef]
- Luo, P.; Qiu, L.; Liu, Y.; Liu, X.L.; Zheng, J.L.; Xue, H.Y.; Liu, W.H.; Liu, D.; Li, J. Metformin Treatment Was Associated with Decreased Mortality in COVID-19 Patients with Diabetes in a Retrospective Analysis. Am. J. Trop. Med. Hyg. 2020, 103, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Xin, S.; Chen, Y.; Li, L.; Chen, W.; Li, W.; Zhou, B.; Li, C.; Gong, Y.; Li, F.; et al. Effects of metformin, insulin on COVID-19 patients with pre-existed type 2 diabetes: A multicentral retrospective study. Life Sci. 2021, 275, 119371. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Liu, T.; Zhong, W.; Liu, R.; Zhou, H.; Huang, W.; Zhang, W. Risk of Metformin in Patients With Type 2 Diabetes With COVID-19: A Preliminary Retrospective Report. Clin. Transl. Sci. 2020, 13, 1055–1059. [Google Scholar] [CrossRef]
- Zangiabadian, M.; Nejadghaderi, S.A.; Zahmatkesh, M.M.; Hajikhani, B.; Mirsaeidi, M.; Nasiri, M.J. The Efficacy and Potential Mechanisms of Metformin in the Treatment of COVID-19 in the Diabetics: A Systematic Review. Front. Endocrinol. 2021, 12, 645194. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Liu, Y.M.; Li, H.; Zhang, X.; Lei, F.; Qin, J.J.; Chen, Z.; Deng, K.Q.; Lin, L.; Chen, M.M.; et al. Metformin Is Associated with Higher Incidence of Acidosis, but Not Mortality, in Individuals with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020, 32, 537–547.e3. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.; Dhatariya, K.; Burr, O.; Nagi, D.; Higgins, K.; Hopkins, D.; Patel, M.; Kar, P.; Gooday, C.; Howarth, D.; et al. Guidelines for the management of diabetes in care homes during the Covid-19 pandemic. Diabet. Med. 2020, 37, 1090–1093. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gupta, R.; Ghosh, A.; Misra, A. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab. Syndr. 2020, 14, 303–310. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R. Is metformin ahead in the race as a repurposed host-directed therapy for patients with diabetes and COVID-19? Diabetes Res. Clin. Pract. 2020, 165, 108268. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Ray, A.; Sadasivam, B. Metformin in COVID-19: A possible role beyond diabetes. Diabetes Res. Clin. Pract. 2020, 164, 108183. [Google Scholar] [CrossRef]
- Yki-Järvinen, H. Thiazolidinediones. N. Engl. J. Med. 2004, 351, 1106–1118. [Google Scholar] [CrossRef]
- Radwan, R.R.; Hasan, H.F. Pioglitazone ameliorates hepatic damage in irradiated rats via regulating anti-inflammatory and antifibrogenic signalling pathways. Free Radic. Res. 2019, 53, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Bassaganya-Riera, J.; Song, R.; Roberts, P.C.; Hontecillas, R. PPAR-gamma activation as an anti-inflammatory therapy for respiratory virus infections. Viral Immunol. 2010, 23, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Erol, A. Role of oxidized LDL-induced “trained macrophages” in the pathogenesis of COVID-19 and benefits of pioglitazone: A hypothesis. Diabetes Metab. Syndr. 2020, 14, 713–714. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhang, J.; Sun, X.; Wang, L.; Xu, Y.; Zhang, Y.; Liu, X.; Dong, C. Influence of diabetes mellitus on the severity and fatality of SARS-CoV-2 (COVID-19) infection. Diabetes Obes. Metab. 2020, 22, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Alam, F.; Islam, M.A.; Mohamed, M.; Ahmad, I.; Kamal, M.A.; Donnelly, R.; Idris, I.; Gan, S.H. Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Sci. Rep. 2019, 9, 5389. [Google Scholar] [CrossRef] [Green Version]
- Kernan, W.N.; Viscoli, C.M.; Furie, K.L.; Young, L.H.; Inzucchi, S.E.; Gorman, M.; Guarino, P.D.; Lovejoy, A.M.; Peduzzi, P.N.; Conwit, R.; et al. Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. N. Engl. J. Med. 2016, 374, 1321–1331. [Google Scholar] [CrossRef]
- Roca-Ho, H.; Riera, M.; Palau, V.; Pascual, J.; Soler, M.J. Characterization of ACE and ACE2 Expression within Different Organs of the NOD Mouse. Int. J. Mol. Sci. 2017, 18, 563. [Google Scholar] [CrossRef] [Green Version]
- Sardu, C.; D’Onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 2020, 43, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Palermo, N.E.; Sadhu, A.R.; McDonnell, M.E. Diabetic Ketoacidosis in COVID-19: Unique Concerns and Considerations. J. Clin. Endocrinol. Metab. 2020, 105, dgaa360. [Google Scholar] [CrossRef] [PubMed]
- Kosinski, C.; Zanchi, A.; Wojtusciszyn, A. Diabète et infection à COVID-19 [Diabetes and COVID-19 infection]. Rev. Med. Suisse 2020, 16, 939–943. [Google Scholar] [PubMed]
- Wang, W.; Lu, J.; Gu, W.; Zhang, Y.; Liu, J.; Ning, G. Care for diabetes with COVID-19: Advice from China. J. Diabetes 2020, 12, 417–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ma, P.; Zhang, S.; Song, S.; Wang, Z.; Ma, Y.; Xu, J.; Wu, F.; Duan, L.; Yin, Z.; et al. Fasting blood glucose at admission is an independent predictor for 28-day mortality in patients with COVID-19 without previous diagnosis of diabetes: A multi-centre retrospective study. Diabetologia 2020, 63, 2102–2111. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.M.; Slaughter, J.C.; Duffus, S.H.; Smith, T.J.; LeStourgeon, L.M.; Jaser, S.S.; McCoy, A.B.; Luther, J.M.; Giovannetti, E.R.; Boeder, S.; et al. COVID-19 Severity Is Tripled in the Diabetes Community: A Prospective Analysis of the Pandemic’s Impact in Type 1 and Type 2 Diabetes. Diabetes Care 2021, 44, 526–532. [Google Scholar] [CrossRef]
- Doupis, J.; Avramidis, K. Managing Diabetes during the COVID-19 Pandemic. Eur. Endocrinol. 2020, 16, 85–87. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Potential pathophysiological links between COVID-19 and diabetes.

Figure 2.
Recommendations pertaining to diabetes treatment during COVID-19 pandemic.


{kind=link}
{kind=link}
Table 1.
A summary of antidiabetic drugs, their mechanisms of action, their possible influence on the course of COVID-19 and current reports regarding impact of these drugs on the course of SARS-CoV-2 infection in patients with diabetes.
Table 1.
A summary of antidiabetic drugs, their mechanisms of action, their possible influence on the course of COVID-19 and current reports regarding impact of these drugs on the course of SARS-CoV-2 infection in patients with diabetes.
| Antidiabetic Drug | Mechanism of Drug Action | Possible Influence on the Course of COVID-19 | Current Reports on Outcomes in SARS-CoV-2 Infection in Patients with Diabetes |
|---|---|---|---|
| DPP4is |
|
|
|
| GLP1RAs | Lack of data | ||
| SGLT2is | |||
| Metformin |
|
| |
| Pioglitazone |
|
| Lack of data |
| Insulin |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bielka, W.; Przezak, A.; Pawlik, A. Therapy of Type 2 Diabetes in Patients with SARS-CoV-2 Infection. Int. J. Mol. Sci. 2021, 22, 7605. https://doi.org/10.3390/ijms22147605
AMA Style
Bielka W, Przezak A, Pawlik A. Therapy of Type 2 Diabetes in Patients with SARS-CoV-2 Infection. International Journal of Molecular Sciences. 2021; 22(14):7605. https://doi.org/10.3390/ijms22147605
Chicago/Turabian StyleBielka, Weronika, Agnieszka Przezak, and Andrzej Pawlik. 2021. "Therapy of Type 2 Diabetes in Patients with SARS-CoV-2 Infection" International Journal of Molecular Sciences 22, no. 14: 7605. https://doi.org/10.3390/ijms22147605
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.