An Online Cross-Sectional Survey on Oral Healthcare Among School-Age Children During COVID-19 Epidemic in Wuhan, China
 Zhen Li
Zhen Li Yuhong Li
Yuhong Li Chang Liu
Chang Liu Han Jiang
Han Jiang Chenzheng Zhang
Chenzheng Zhang Minquan Du
Minquan Du- The State Key Laboratory Breeding Base of Basic Science of Stomatology (Hubei-MOST) & Key Laboratory of Oral Biomedicine Ministry of Education, School and Hospital of Stomatology, Wuhan University, Wuhan, China
Background: Since the outbreak of Coronavirus disease 2019 (COVID-19), the government of China adopted many measures which changed people's lifestyle including oral health-related lifestyle to control the transmission. The aim of this study was to investigate oral health status, oral healthcare behaviors, and parental attitudes toward oral healthcare among school-age children in Wuhan during the COVID-19 outbreak and what the status would be when the outbreak is under control.
Methods: This study was an online cross-sectional survey facing elementary school students in Wuhan. The questionnaire was completed by children's parents or other family members. The information on demographic data, oral health status, oral healthcare behaviors, and parental attitudes toward oral healthcare was collected at the end of school closure. The chi-square test was used to test the association of different questionnaire items.
Results: A total of 18,383 subjects aged 6–13 years with complete data were included in this investigation, and 44.2% of them suffered pain or discomfort related to teeth and gums during the epidemic. While there might be an increasing need and concern of oral healthcare during the outbreak and even when the outbreak was controlled, the worry of infection made it difficult for people to meet their demands of dental attendance.
Conclusion: The risk of cross-infection during the treatment had a negative influence on parental attitudes toward dental attendance. Effective measures should be taken to meet people's demands of dental attendance.
Introduction
Coronavirus disease 2019 (COVID-19) is a respiratory disease caused by a novel coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The World Health Organization (WHO) officially recognized the outbreaks as a public health emergency of international concern on January 30, 2020 (1). As of June 8, 2020, a total of 6,931,000 confirmed cases and 400,857 deaths has been recognized in the whole world (2). This is a great challenge not only for China, but also for the world.
Oral disease is a major public health problem which affects children worldwide (3). Moreover, it would impact children's eating, speaking, emotional well-being, and general health when it happened to children (4). It is widely accepted that lifestyles are closely associated with oral disease (5), and great changes have happened on children's daily life since the outbreak of COVID-19.
Currently, the transmission of COVID-19 is regarded as starting with an animal-to-human transmission, followed by human-to-human spread. The modes of its interpersonal transmission include respiratory droplets, contact transmission, and aerosol routes. In addition, some asymptomatic spread cases were also reported (6). Considering these transmission characteristics of COVID-19, dentistry practices have a high risk of infection such as the frequent production of aerosols, constant presence of saliva, and the unavoidable touch of mouth, nose, and eyes (7). As a result, general non-emergency dental treatment was suspended and only emergency dental services were provided across China since January 2020 (8). Besides the limitation of dental attendance, many other measures, including lockdown for the whole Hubei province, quarantining infected and suspected people, restricting access to public spaces, and issuing a home quarantine order to all the residents, were adopted by the government of China to control the transmission efficiently. During this special domiciliary time, people have spent most of their time staying at home. For citizens in Wuhan, only online shopping provided by local supermarkets and markets was available and a narrow range of goods could be bought. This epidemic also has an indirect impact on people's lifestyle through psychology. It was reported that over half of Chinese suffered moderate-to-severe psychological impact during the initial phase of the COVID-19 outbreak (9).
With all of these changes, we hypothesized that the oral health status, the oral healthcare behaviors, and the attitudes toward oral healthcare of school-age children may have also changed. Wuhan, as the city facing the severest epidemic condition across China (10), may face more challenges than other cities on oral healthcare.
The aim of this study was to investigate oral health status, oral healthcare behaviors, and parental attitudes toward oral healthcare among school-age children in Wuhan during the COVID-19 outbreak and what the status would be when the outbreak is under control, thereby providing guidance for the following preventive and therapeutic oral healthcare in Wuhan and other districts which are affected by the epidemic.
Materials and Methods
Ethical Clearance
This questionnaire survey was undertaken by the Department of Preventive Dentistry, School & Hospital of Stomatology of Wuhan University. The questionnaire was anonymous to ensure privacy protection. Ethical approval (Approval no. HGGC-035) for the study was obtained from the Ethics Committee of the School & Hospital of Stomatology of Wuhan University, and informed consent was obtained from the guardian of each subject.
Study Participants
This survey faces to elementary school students in Wuhan. In view of their age, parents or other family members are allowed to fill in the questionnaire instead.
Data collection was conducted from May 1 to 7, 2020. An online data collection was conducted because of the home quarantine order. The questionnaire was published on Wenjuanxing, and it was set as “per IP address and WeChat account can only submit the questionnaire once” through the platform to prevent double entry from participants. Then, we posted the link and the quick response code of the questionnaire, on WeChat groups and moments, attaching with a brief introduction, and asked people for passing on to their friends and relatives.
Questionnaire Survey
The questionnaire consisted of four parts: (1) demographic data; (2) oral health status; (3) oral healthcare behaviors; and (4) attitudes toward oral healthcare during and after the epidemic situation.
Demographic data was collected on gender, age, and living region, including each district in Wuhan and the other regions in China.
To understand oral health status, we listed options including dental caries, bleeding while brushing teeth, loss of restorative material, tooth trauma, bad breath, oral ulcer, and other oral discomfort (an open-ended option) for people to multiply choose. In addition, we also afforded “I don't know” and “I don't have any discomfort” options. A self-assessment regarding oral health status was required in the end of the questionnaire.
In the aspect of oral healthcare behaviors, questions were designed covering several areas: (1) the choices about using oral healthcare products for the home; (2) the choices about using oral health services toward prevention; (3) meal times; (4) frequency of having confectionery; (5) frequency of having sweet drinks; (6) frequency of having sugared drinks like milk, yogurts, milk powders, tea, soybean milk, and coffees; and (7) frequency of toothbrushing.
Attitudes toward oral healthcare were measured by questions for during and after the epidemic situation, respectively, including the level of concern on oral health, the level of concern on access to treatment, the level of worry on being infected in the process of oral treatment, and the attitudes toward dental attendance.
In this questionnaire, “before the epidemic” means the period when there is no outbreak of epidemic (before January 23, 2020); “during the epidemic” means during Wuhan lockdown (from January 23, 2020, to April 8, 2020); and “after the epidemic” means the period that the epidemic is under control.
Statistical Analysis
Data analysis was performed using the SPSS (PC version 23.0) software with the level of statistical significance set at P < 0.001. Subjects with missing data were excluded from the analysis.
The Optimal Binning method was used to select the optimal cutoff point of age. The chi-square test was used to test the association of different questionnaire items. McNemar's test was taken into account to find out the different attitudes toward oral healthcare in different epidemic situations.
Results
A total of 18,694 subjects took part in this investigation. Of these subjects, 159 children were excluded because their living region was out of Wuhan and 152 subjects were excluded because of their age. At last, 18,383 subjects (9,753 boys and 8,630 girls) between the ages of 6 and 13 years were included in this study. The age range of 9–10 is the cutoff point between younger and older school-age children in this study. The characteristics of the study group are shown in Table 1.
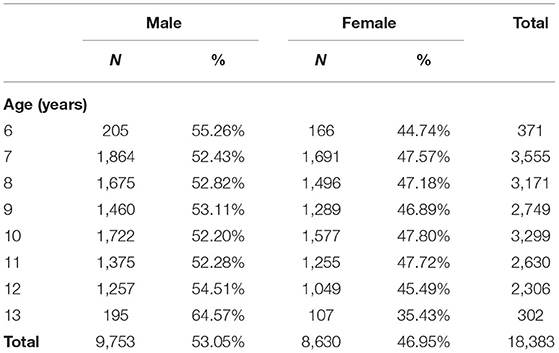
Table 1. General characteristics of the study group.
Table 2 presents children's oral health status during the epidemic. Almost half of the children (44.2%) suffered oral discomfort, and the younger group had a higher proportion than the older group (47.5 vs. 40.3%). Besides, more children aged 6–9 years had an increase in the severity of oral discomfort than the children aged 10–13 years during the epidemic (7.6 vs. 4.7%). No significant difference was found for gender in the items above. As for detailed experience of pain/discomfort the children suffered, the younger group had a higher rate of dental caries and loss of restorative material than the older group while more girls than boys suffered bleeding while brushing teeth.
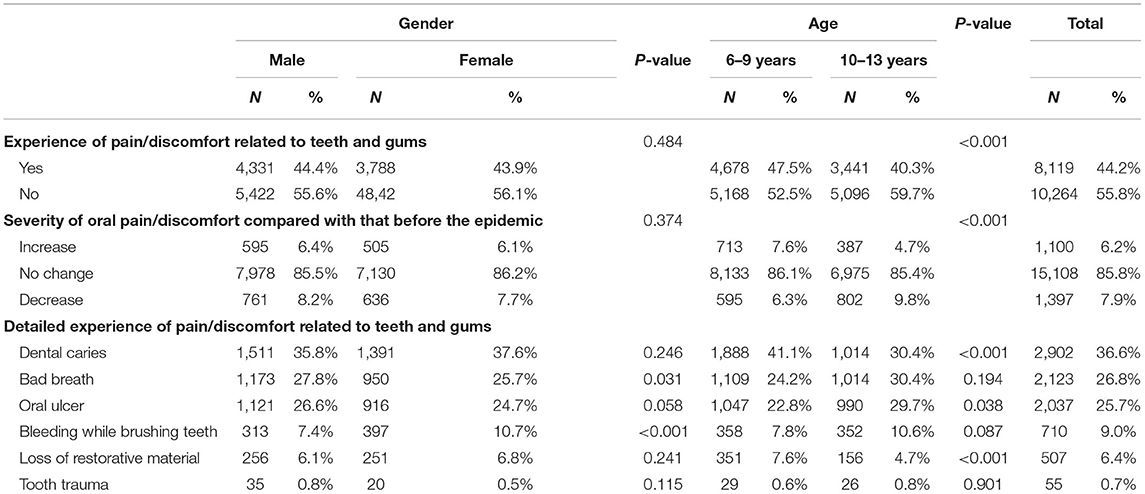
Table 2. Chi-square test for relationship of gender/age and oral health status during the epidemic.
Table 3 provides information on oral healthcare behaviors. As for the use of oral healthcare products for the home, the proportion of subjects who used electric toothbrush (33.1 vs. 30.2%), fluoride toothpaste (26.1 vs. 20.2%), mouth rinse (16.1 vs. 7.0%), and dental floss (8.8 vs. 8.0%) after the epidemic was higher than that during the epidemic. What is more, little difference was found for gender and significant difference was found for age in the use of oral healthcare products for the home. No matter the situation was during the epidemic or after the epidemic, the younger group had a higher rate of the usage of electric toothbrush and fluoride toothpaste while the older group had a higher rate of the usage of mouth rinse.
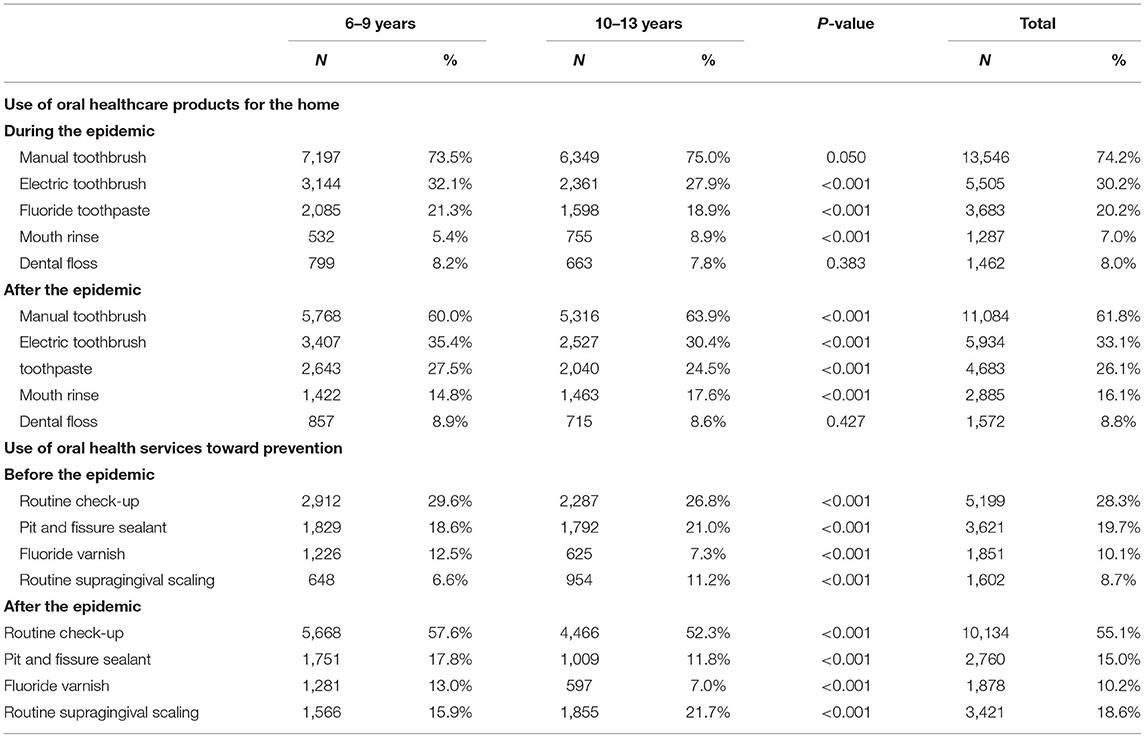
Table 3. Chi-square test for relationship of age and oral healthcare behaviors during the epidemic.
With regard to dental service utilization for preventive need, 28.3, 19.7, 10.1, and 8.7% of children took a routine check-up, pit and fissure sealant, fluoride varnish, and routine supragingival scaling before the epidemic, respectively. Moreover, the corresponding proportions were 55.1, 15.0, 10.2, and 18.6% when the epidemic was controlled. Children aged 6–9 years had a higher proportion of taking routine check-up (29.6 vs. 26.8%) and fluoride varnish (12.5 vs. 7.3%) than the older children and a lower proportion of taking pit and fissure sealant (18.6 vs. 21.0%) and routine supragingival scale (6.6 vs. 11.2%) before the epidemic. Besides, the parents of younger children had a higher willing of taking routine check-up (57.6 vs. 52.3%), fluoride varnish (13.0 vs. 7.0%), and pit and fissure sealant (17.8 vs. 11.8%) than the parents of older children and a lower willing of taking routine supragingival scale (15.9 vs. 21.7%) than the parents of older children after the epidemic. No dental service but routine check-up (26.4% for boys and 30.4% for girls before the epidemic; 54.0% for boys and 56.4% for girls after the epidemic) had a utilization difference for gender.
Table 4 shows the frequency of eating and toothbrushing. A percentage of 20.2% of children had a change of meal times. The proportion of children who had an increase in the frequency of confectionery, sweet drinks, and sugared drinks like milk, yogurts, milk powders, tea, soybean milk, and coffees was 18.4, 10.3, and 22.9%, respectively. With 7.4% of children who had an increase in the frequency of toothbrushing, only 62.3% of children brushed their teeth more than twice a day during the epidemic. The proportion of girls who had a stable meal time (81.3 vs. 78.4%) and who brush their teeth more than twice a day (65.3 vs. 59.7%) were higher than that of boys. The proportion of the younger group who had an increase in the frequency of meal times (18.2 vs. 16.7%) and who brush their teeth more than twice a day (64.2 vs. 60.2%) was higher than that of the older group.
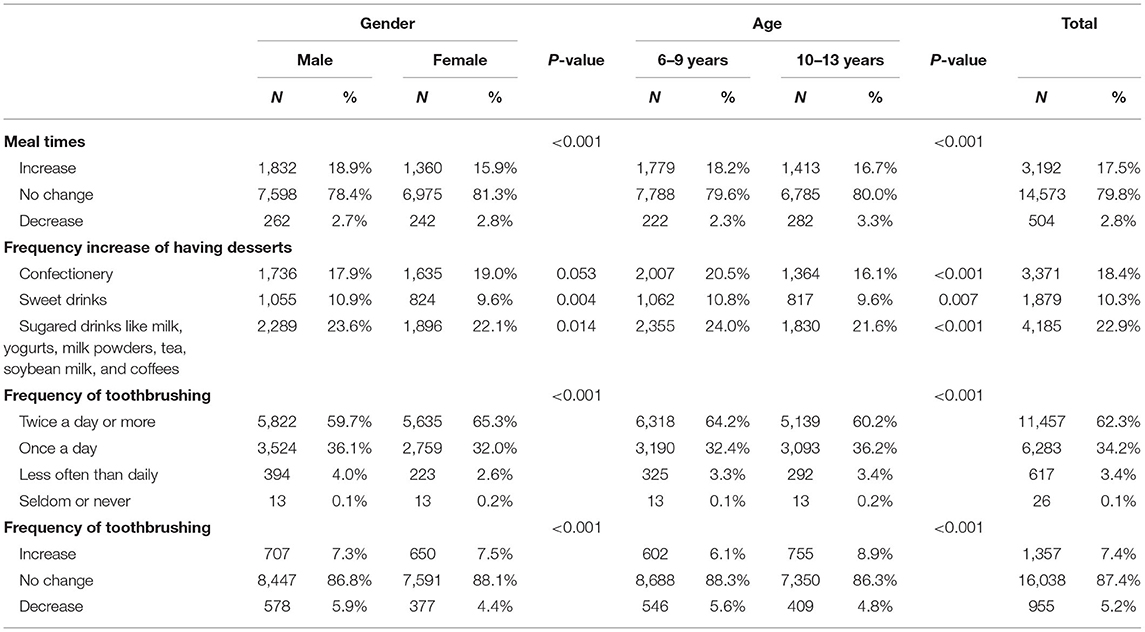
Table 4. Chi-square test for relationship of gender/age and oral healthcare behaviors during the epidemic.
Tables 5, 6 show parental attitudes toward oral healthcare during and after the epidemic situation. Table 5 shows a comparison of parental concern on oral health and access to oral treatment during the epidemic with that after the epidemic. A significant difference in the level of concern existed in different periods (P-value of McNemar's test <0.001). The levels of both concern on oral health and access to treatment after the epidemic were higher than those during the epidemic. Table 6 shows the relationship of worry on being infected in the process of oral treatment and the attitudes toward dental attendance after the epidemic. The overwhelming majority (93.8%) of the parents worried on being infected in the process of oral treatment after the epidemic, and half of the parents (53.4%) still avoided the dental attendance after the epidemic (no treatment for 9.8%, deal with it by oneself and avoid going to hospital for 13.4%, and avoid dental practice except for emergency cases for 30.2%).
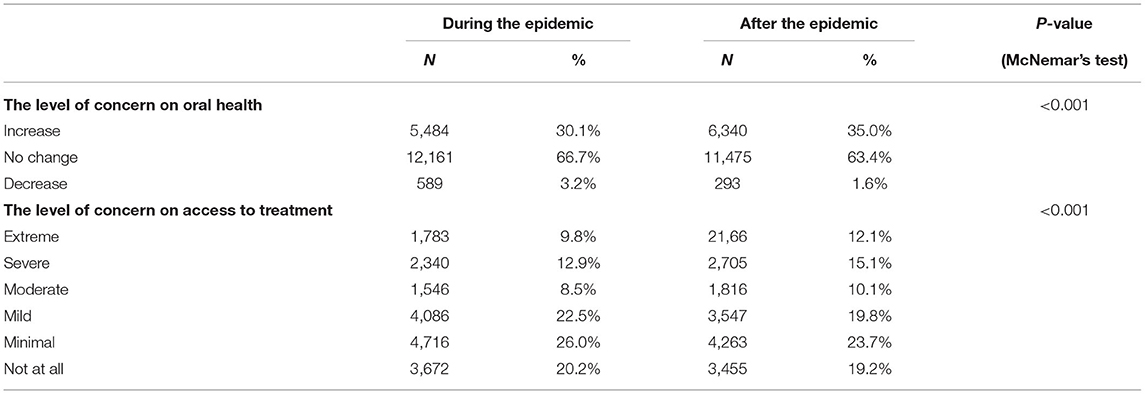
Table 5. Parental attitudes toward the oral health care compared with that before the epidemic.

Table 6. Chi-square test for relationship of the level of worry on being infected in the process of oral treatment and the attitudes toward dental attendance after the epidemic.
Discussion
This study based on a large sample size with unequal gender distribution, which was resulted from the snowball sampling techniques and consisted with sex ratio imbalance in Wuhan (11).
The results of this study show that some changes happened on children's oral health status, oral healthcare behaviors, and parental attitudes toward oral healthcare in Wuhan during the COVID-19 outbreak. Besides, significant differences were found in oral healthcare between different age groups. What is more, while there was an increasing necessity and concern of oral healthcare because of the epidemic, the outbreak of the epidemic brought lots of difficulties for people to have a dental visit even when the epidemic was controlled.
Oral Health Status
On the whole, the school-age children in Wuhan had a poor oral health and dental caries was the most common dental disease among this group. According to some recent reports on dental health among school-age children in China, the prevalence of dental caries was 46.88% for boys and 49.63% for girls among the children aged 6–12 years in Chengdu (12). In Shenzhen, the prevalence of dental caries was 55.7% for 6–9-year-old children and 31.9% for 10–13-year-old children (13). The prevalence of self-reported caries in this survey was 41.1% for children aged 6–9 years and 30.4% for children aged 10–13 years. It is relatively low compared with that in the previous study. A main explanation for this is that it is a result acquired in a self-reported way and it is difficult for people to distinguish whether it was caries or not.
Considering that studies on self-reported oral health and its correlation with clinical evaluation among school-age children were scarce, information about changes on self-reported oral health status during the epidemic was collected to identify what effect the epidemic had on oral health status.
Among the children who suffered pain/discomfort related to teeth and gums during the epidemic, the younger group had a higher proportion of subjects who had an increased severity than the older group. It indicated that the dental health status of the younger group was more susceptible to the epidemic than the older group. It could be partly explained by the fact that the younger group had a higher proportion of subjects who had a negative change on their diets during the epidemic than the older group.
What interested us is that a significant difference existed in the percentage of subjects who suffered discomfort related to teeth between different groups when the group was divided by age but not gender, while it was quite the opposite in the percentage of subjects who suffered discomfort related to gums. The former result that the younger group had a lower proportion of subjects who suffered discomfort related to teeth than the older group can be explained by the specific timing of tooth replacement (14). The latter result showing that the boys had a lower percentage of subjects who suffered discomfort related to gums than the girls was consistent with some of the previous studies (15), but it was difficult to explain combining the oral healthcare behaviors shown in this study. In this study, girls were more interested in adhering to the oral hygiene behaviors and their parents paid more attention to their children than the boys, which were reflected in the higher prevalence of routine check-up, recommended frequency of toothbrushing, and stable meal times. All of these results indicated that the girls might have a better oral hygiene level than boys. This difference in behaviors was consistent with previous studies. Furthermore, in most of such studies, boys had a worse gum health status (16–19). The result in this study was probably caused by physiological character difference in gender, such as the specific timing of teeth replacement and the fluctuation of hormone levels with stress events (20). Further researches are needed on it.
Oral Healthcare Behaviors
The willingness to use oral healthcare products for the home and oral health services toward prevention had an increase when the epidemic was controlled. Generally, the younger group had a higher proportion of using recommended oral healthcare products and oral health services than the older group during and after the epidemic. It might be because parents tend to put more concern on the younger children.
Parental Attitudes Toward Oral Healthcare
The changes on oral health status and oral healthcare behaviors indicated that there is an increase in the demand for oral healthcare after the epidemic. Besides, a large proportion of parents had an increased level of concern on oral health during and after the epidemic according to the results from parental attitudes toward oral healthcare.
However, 53.4% of them still have a tendency to avoid going to the hospital and the proportion of people who had concern on access to treatment after the epidemic was 80.8%. It can be partly explained by the positive correlation between the level of worry on being infected in the process of oral treatment and the attitudes toward dental attendance considering the large proportion of people who had worry on being infected in the process of oral treatment after the epidemic (93.8%).
Taking all these factors into account, more attention should be paid to spread information about the measures that have been taken to reduce the risk of cross-infection during the treatment.
Strengths and Limitations
This study has both strengths and limitations. A major strength of the current study is that it is the first study to report the oral healthcare of school-age children in Wuhan during the COVID-19 outbreak. Wuhan has its specificity for it was the most serious district in China and has been under the strictest management for the longest time. Besides, it has a large sample size and the data was obtained before the epidemic passed.
There are also some limitations. Firstly, selection bias exists because of the snowballing sampling strategy and the use of an online survey. Secondly, recall bias exists as the oral health condition was reported by the parents. Thirdly, to attract more subjects to fill the questionnaire, the number of the questions was limited. As a result, many items were not able to have a further discussion.
Conclusions
In conclusion, children's oral health status was affected by the epidemic, especially 6–9-year-old children. More attention should be paid on the eating habits of children aged 6–9 and toothbrushing habits of boys. Parents in Wuhan had more concerns on oral healthcare during and after the epidemic than before the epidemic state. Besides, the findings from this study show a high amount of dental treatment needed among school-age children in Wuhan after the epidemic. However, the worry on being infected in the process of oral treatment after the epidemic might be a major factor which would stop people from dental attendance. Effective measures should be taken to meet people's demands of oral healthcare. What is more, age-specific strategies in prevention are necessary for school-age children.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the School & Hospital of Stomatology of Wuhan University. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Statement on the second meeting of the International Health Regulations 2005 Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). (2020). Available online at: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-2005-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed June 10, 2020).
2. World Health Organization. Coronavirus Disease 2019. (COVID-19) Situation Report-140. (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed June 10, 2020).
3. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century–the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. (2003) 31(Suppl. 1):3–23. doi: 10.1046/j.2003.com122.x
4. Hescot P. The new definition of oral health and relationship between oral health and quality of life. Chin J Dent Res. (2017) 20:189–92. doi: 10.3290/j.cjdr.a39217
5. Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. (2016) 22:609–19. doi: 10.1111/odi.12428
6. General Office of National Health Commission of People's Republic of China Office of National Administration of Traditional Chinese Medicine. Diagnosis and treatment of corona virus disease-19(7th trial edition). China Med. (2020) 15:801–5. doi: 10.3760/j.issn.1673-4777.2020.06.001
7. Yang ZZ. Nosocomial infection risk through aerosol of corona virus disease-19 and preventive measure. China Med. (2020) 15:812–5. doi: 10.3760/j.issn.1673-4777.2020.06.003
8. Yang Y, Zhou Y, Liu X, Tan J. Health services provision of 48 public tertiary dental hospitals during the COVID-19 epidemic in China. Clin Oral Investig. (2020) 24:1861–4. doi: 10.1007/s00784-020-03267-8
9. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019. Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
10. National Health Commission of the People's Republic of China. Distribution of the COVID-19 Outbreak. (2020). Available online at: http://2019ncov.chinacdc.cn/2019-nCoV/ (accessed June 10, 2020).
11. National Bureau of Statistics of China. Tabulation on the 2010 Population Census of the Prople's Republic of China. (2012). Available online at: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm (accessed June 10, 2020).
12. Peng R, Li S, Zhang H, Zeng H, Jiang B, Liu Y, et al. Weight status is associated with blood pressure, vital capacity, dental decay, and visual acuity among school-age children in Chengdu, China. Ann Nutr Metab. (2016) 69:237–45. doi: 10.1159/000454888
13. Cheng YH, Liao Y, Chen DY, Wang Y, Wu Y. Prevalence of dental caries and its association with body mass index among school-age children in Shenzhen, China. BMC Oral Health. (2019) 19:270. doi: 10.1186/s12903-019-0950-y
14. Nelson SJ, Ash MM. Wheeler's Dental Anatomy, Physiology, and Occulsion. 9th ed. Philadelphia: W.B. Saunders Co (2010). p. 36.
15. Gopinath VK, Rahman B, Awad MA. Assessment of gingival health among school children in Sharjah, United Arab Emirates. Eur J Dent. (2015) 9:36–40. doi: 10.4103/1305-7456.149636
16. Bashirian S, Seyedzadeh-Sabounchi S, Shirahmadi S, Soltanian AR, Karimi-Shahanjarini A, Vahdatinia F. Socio-demographic determinants as predictors of oral hygiene status and gingivitis in schoolchildren aged 7-12 years old: a cross-sectional study. PLoS ONE. (2018) 13:e0208886. doi: 10.1371/journal.pone.0208886
17. Tomazoni F, Vettore MV, Zanatta FB, Tuchtenhagen S, Moreira CH, Ardenghi TM. The associations of socioeconomic status and social capital with gingival bleeding among schoolchildren. J Public Health Dent. (2017) 77:21–9. doi: 10.1111/jphd.12166
18. Shiau HJ, Reynolds MA. Sex differences in destructive periodontal disease: a systematic review. J Periodontol. (2010) 81:1379–89. doi: 10.1902/jop.2010.100044
19. Natto ZS, Abu Ahmad RH, Alsharif LT, Alrowithi HF, Alsini DA, Salih HA, et al. Chronic periodontitis case definitions and confounders in periodontal research: a systematic assessment. Biomed Res Int. (2018) 2018:4578782. doi: 10.1155/2018/4578782
Keywords: Wuhan, school-age children, oral health, epidemic, COVID-19
Citation: Li Z, Li Y, Liu C, Jiang H, Zhang C and Du M (2021) An Online Cross-Sectional Survey on Oral Healthcare Among School-Age Children During COVID-19 Epidemic in Wuhan, China. Front. Med. 8:572217. doi: 10.3389/fmed.2021.572217
Received: 13 June 2020; Accepted: 17 May 2021;
Published: 22 June 2021.
Edited by:
Colman McGrath, The University of Hong Kong, Hong Kong, SAR ChinaReviewed by:
Chun Hung Chu, The University of Hong Kong, Hong Kong, SAR ChinaGuohui Liu, Huazhong University of Science and Technology, China
Copyright © 2021 Li, Li, Liu, Jiang, Zhang and Du. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chenzheng Zhang, zhangchenzheng@foxmail.com; Minquan Du, duminquan@whu.edu.cn