World Journal of Emergency Medicine ›› 2021, Vol. 12 ›› Issue (1): 18-23.doi: 10.5847/wjem.j.1920-8642.2021.01.003
Special Issue: COVID-19
• Original Articles • Previous Articles Next Articles
Wei Guo1, Lin-yu Ran2, Ji-hong Zhu3, Qing-gang Ge4, Zhe Du1, Fei-long Wang2( ), Wei-bo Gao3(), Tian-bing Wang1()
), Wei-bo Gao3(), Tian-bing Wang1()
Received:2020-06-18
Accepted:2020-11-05
Online:2021-01-01
Published:2021-01-01
Contact:
Fei-long Wang,Wei-bo Gao,Tian-bing Wang
E-mail:dr.feilongwang@gmail.com;13699185078@163.com;wangtianbing@pkuph.edu.cn
Wei Guo, Lin-yu Ran, Ji-hong Zhu, Qing-gang Ge, Zhe Du, Fei-long Wang, Wei-bo Gao, Tian-bing Wang. Identifying critically ill patients at risk of death from coronavirus disease[J]. World Journal of Emergency Medicine, 2021, 12(1): 18-23.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2021.01.003
Table 1
Performance of variables for predicting in-hospital mortality in COVID-19 patients*
| Variables | AUC | 95% CI | Cut-off value | Sensitivity (%) | Specificity (%) | P |
|---|---|---|---|---|---|---|
| SOFA | 0.960 | 0.908-0.987 | 2 | 94.29 | 93.02 | <0.001 |
| Free triiodothyronine | 0.863 | 0.761-0.932 | 3.25 pmol/L | 94.44 | 75.93 | <0.001 |
| Neutrophil-to-lymphocyte ratio | 0.857 | 0.782-0.914 | 8.48 | 85.71 | 79.07 | <0.001 |
| Procalcitonin | 0.850 | 0.771-0.910 | 0.38 ng/mL | 84.85 | 76.54 | <0.001 |
| Neutrophil count | 0.842 | 0.764-0.902 | 5.71×109/L | 82.86 | 77.91 | <0.001 |
| Prothrombin time | 0.828 | 0.748-0.891 | 15.2 seconds | 71.43 | 85.88 | <0.001 |
| White blood cell count | 0.827 | 0.747-0.889 | 7.04×109/L | 85.71 | 70.93 | <0.001 |
| Ferritin | 0.827 | 0.744-0.892 | 862.7 μg/L | 94.12 | 58.44 | <0.001 |
| Direct bilirubin | 0.826 | 0.746-0.889 | 5.2 μmol/L | 80.00 | 74.12 | <0.001 |
| High sensitive C-reactive protein | 0.824 | 0.742-0.889 | 131.1 mg/L | 68.57 | 85.00 | <0.001 |
| Albumin | 0.811 | 0.730-0.877 | 31.9 g/L | 94.29 | 61.63 | <0.001 |
| High sensitive troponin I | 0.808 | 0.722-0.877 | 33.4 ng/mL | 73.53 | 86.84 | <0.001 |
| Total bilirubin | 0.794 | 0.711-0.862 | 10.1 μmol/L | 85.71 | 61.63 | <0.001 |
| Lactate dehydrogenase | 0.794 | 0.710-0.862 | 425 U/L | 77.14 | 76.74 | <0.001 |
| NT-proBNP | 0.793 | 0.704-0.864 | 247 pg/mL | 96.97 | 56.58 | <0.001 |
| Creatine kinase muscle brain isoenzyme | 0.793 | 0.695-0.870 | 2.2 ng/mL | 70.37 | 87.69 | <0.001 |
| Fibrin degradation products | 0.792 | 0.701-0.866 | 8.9 μg/mL | 81.25 | 69.01 | <0.001 |
| D-dimer | 0.786 | 0.702-0.856 | 2.21 μg/mL | 80.00 | 68.24 | <0.001 |
| Aspartate aminotransferase | 0.763 | 0.677-0.836 | 33 U/L | 88.57 | 60.47 | <0.001 |
| Blood urea nitrogen | 0.761 | 0.675-0.834 | 5.2 μmol/L | 91.43 | 56.98 | <0.001 |
| Lymphocyte count | 0.734 | 0.646-0.811 | 0.65×109/L | 68.57 | 74.42 | <0.001 |
| qSOFA | 0.734 | 0.646-0.810 | 0 | 97.14 | 32.56 | <0.001 |
| Myohemoglobin | 0.726 | 0.622-0.814 | 87 ng/mL | 77.78 | 60.94 | <0.001 |
| Interleukin-2 receptor | 0.720 | 0.627-0.802 | 1,215 U/mL | 73.53 | 64.47 | <0.001 |
| Glucose | 0.717 | 0.626-0.797 | 6.39 mmol/L | 77.14 | 65.43 | <0.001 |
| AT3 | 0.710 | 0.611-0.796 | 78% | 45.16 | 87.14 | <0.001 |
| Free thyroxine | 0.693 | 0.573-0.796 | 19.35 pmol/L | 83.33 | 55.56 | 0.003 |
| Alanine aminotransferase | 0.677 | 0.586-0.759 | 50 U/L | 42.86 | 88.37 | 0.001 |
| Creatine kinase | 0.664 | 0.569-0.750 | 207 U/L | 53.57 | 84.88 | 0.012 |
| Platelet count | 0.650 | 0.558-0.734 | 239×109/L | 85.71 | 44.19 | 0.008 |
| Age | 0.626 | 0.534-0.712 | 56 | 88.57 | 31.40 | 0.021 |
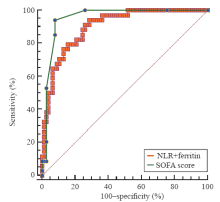
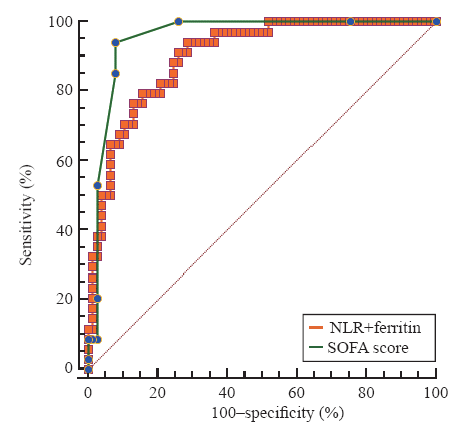
Figure 1.
Receiver operating characteristic curve for the combination of neutrophil-to-lymphocyte ratio (NLR) and ferritin as compared with Sequential Organ Failure Assessment (SOFA) score in predicting in-hospital mortality in COVID-19 patients.
| 1 |
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020; 382(8):727-33.
doi: 10.1056/NEJMoa2001017 pmid: 31978945 |
| 2 |
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020; 323(11):1061-9.
doi: 10.1001/jama.2020.1585 pmid: 32031570 |
| 3 |
Chang D, Lin M, Wei L, Xie L, Zhu G, Cruz CS, et al. Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA. 2020; 323(11):1092-3.
doi: 10.1001/jama.2020.1623 pmid: 32031568 |
| 4 |
Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020; 382(10):929-36.
doi: 10.1056/NEJMoa2001191 pmid: 32004427 |
| 5 |
Allione A, Giamello JD, Bernardi S, Paglietta G, Cavalot GLM, Dutto LA, et al. Coronavirus disease 2019 (COVID-19) and prosthetic heart valve: An additional coagulative challenge. World J Emerg Med. 2020; 11(4):258-9.
doi: 10.5847/wjem.j.1920-8642.2020.04.009 pmid: 33014223 |
| 6 | WHO. Coronavirus disease 2019 (COVID-19) situation report - 55. March 15, 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200315-sitrep-55-covid-19.pdf?sfvrsn=33daa5cb_6. Accessed March 16, 2020. |
| 7 |
Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Intensive Care Med. 2018; 44(6):925-8.
pmid: 29675566 |
| 8 |
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395(10223):497-506.
doi: 10.1016/S0140-6736(20)30183-5 pmid: 31986264 |
| 9 |
Force AD, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E. Acute respiratory distress syndrome. JAMA. 2012; 307(23):2526-33.
doi: 10.1001/jama.2012.5669 pmid: 22797452 |
| 10 |
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012; 120(4):c179-84.
pmid: 22890468 |
| 11 | Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016; 18(8):891-975. |
| 12 |
Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016; 315(8):762-74.
doi: 10.1001/jama.2016.0288 pmid: 26903335 |
| 13 |
Mackinnon A, Mulligan R. Combining cognitive testing and informant report to increase accuracy in screening for dementia. Am J Psychiatry. 1998; 155(11):1529-35.
pmid: 9812113 |
| 14 |
Hanley JA, McNeil BJ. A method of comparing the areas under ROC curves derived from same cases. Radiology. 1983; 148(3):839-43.
pmid: 6878708 |
| 15 |
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395(10229):1054-62.
pmid: 32171076 |
| 16 |
Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020; 8(5):475-81.
pmid: 32105632 |
| 17 |
Faria SS, Fernandes Jr PC, Silva MJ, Lima VC, Fontes W, Freitas-Junior R, et al. The neutrophil-to-lymphocyte ratio: a narrative review. Ecancermedicalscience. 2016; 10:702.
doi: 10.3332/ecancer.2016.702 pmid: 28105073 |
| 18 |
Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014; 106(6):dju124.
doi: 10.1093/jnci/dju124 pmid: 24875653 |
| 19 |
Bhat T, Teli S, Rijal J, Bhat H, Raza M, Khoueiry G, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013; 11(1):55-9.
pmid: 23259445 |
| 20 |
Hwang SY, Shin TG, Jo IJ, Jeon K, Suh GY, Lee TR, et al. Neutrophil-to-lymphocyte ratio as a prognostic marker in critically-ill septic patients. Am J Emerg Med. 2017; 35(2):234-9.
doi: 10.1016/j.ajem.2016.10.055 pmid: 27806894 |
| 21 |
Knovich MA, Storey JA, Coffman LG, Torti SV, Torti FM. Ferritin for the clinician. Blood Rev. 2009; 23(3):95-104.
pmid: 18835072 |
| 22 |
Kell DB, Pretorius E. Serum ferritin is an important inflammatory disease marker, as it is mainly a leakage product from damaged cells. Metallomics. 2014; 6(4):748-73.
doi: 10.1039/c3mt00347g pmid: 24549403 |
| 23 | Rosário C, Zandman-Goddard G, Meyron-Holtz EG, D’Cruz DP, Shoenfeld Y. The hyperferritinemic syndrome: macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med. 2013; 11(1):185. |
| 24 |
Cohen LA, Gutierrez L, Weiss A, Leichtmann-Bardoogo Y, Zhang DL, Crooks DR, et al. Serum ferritin is derived primarily from macrophages through a nonclassical secretory pathway. Blood. 2010; 116(9):1574-84.
doi: 10.1182/blood-2009-11-253815 pmid: 20472835 |
| 25 | Lalueza A, Ayuso B, Arrieta E, Trujillo H, Folgueira D, Cueto C, et al. Elevation of serum ferritin levels for predicting a poor outcome in hospitalized patients with influenza infection. Clin Microbiol Infect. 2020; 26(11):1557.e9-1557.e15. |
| 26 |
van den Berghe G. The neuroendocrine response to stress is a dynamic process. Best Pract Res Clin Endocrinol Metab. 2001; 15(4):405-19.
pmid: 11800514 |
| 27 |
Wang F, Pan W, Wang H, Wang S, Pan S, Ge J. Relationship between thyroid function and ICU mortality: a prospective observation study. Crit Care. 2012; 16(1):R11.
doi: 10.1186/cc11151 pmid: 22257427 |
| 28 |
Warner MH, Beckett GJ. Mechanisms behind the non-thyroidal illness syndrome: an update. J Endocrinol. 2010; 205(1):1-3.
pmid: 20016054 |
| 29 |
Tisoncik JR, Korth MJ, Simmons CP, Farrar J, Martin TR, Katze MG. Into the eye of the cytokine storm. Microbiol Mol Biol Rev. 2012; 76(1):16-32.
doi: 10.1128/MMBR.05015-11 pmid: 22390970 |
| 30 |
Mehta P McAuley DF Brown M Sanchez M Tattersall RS Manson JJ, COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020 ; 395(10229):1033-4.
doi: 10.1016/S0140-6736(20)30628-0 pmid: 32192578 |
| [1] | Wen-qiang Jiang, Xu-sheng Li, Wen-hong Zhong, Lin-qiang Huang, Xiao-jun Lin, Miao-yun Wen, Yu-jun Deng, Xin Li, Hong-ke Zeng. Comparison of clinical characteristics in patients with coronavirus disease and influenza A in Guangzhou, China [J]. World Journal of Emergency Medicine, 2021, 12(4): 287-292. |
| [2] | Ren-qi Yao, Chao Ren, Di Ren, Jin-xiu Li, Ying Li, Xue-yan Liu, Lei Huang, Yong Liu, Mian Peng, Yong-wen Feng, Yong-ming Yao. Development of septic shock and prognostic assessment in critically ill patients with coronavirus disease outside Wuhan, China [J]. World Journal of Emergency Medicine, 2021, 12(4): 293-298. |
| [3] | Gui-long Feng, Miao-miao Zheng, Shi-hong Yao, Yin-qi Li, Shao-jun Zhang, Wei-jing Wen, Kai Fan, Jia-li Zhang, Xiao Zhang. Risk factors and predictive model of adrenocortical insufficiency in patients with traumatic brain injury [J]. World Journal of Emergency Medicine, 2021, 12(3): 179-184. |
| [4] | Yu-qing Cui, Xian-fei Ding, Huo-yan Liang, Dong Wang, Xiao-juan Zhang, Li-feng Li, Quan-cheng Kan, Le-xin Wang, Tong-wen Sun. Efficacy and safety of low-dose corticosteroids for acute respiratory distress syndrome: A systematic review and meta-analysis [J]. World Journal of Emergency Medicine, 2021, 12(3): 207-213. |
| [5] | Wen Gao, Yu-ping Zhang, Jing-fen Jin. Poor outcomes of delirium in the intensive care units are amplified by increasing age: A retrospective cohort study [J]. World Journal of Emergency Medicine, 2021, 12(2): 117-123. |
| [6] | Hao-tian Chen, Jian-feng Xu, Xiao-xia Huang, Ni-ya Zhou, Yong-kui Wang, Yue Mao. Blood eosinophils and mortality in patients with acute respiratory distress syndrome: A propensity score matching analysis [J]. World Journal of Emergency Medicine, 2021, 12(2): 131-136. |
| [7] | Tian Xu, Ya Li, Li-ding Zhao, Guo-sheng Fu, Wen-bin Zhang. Predictors of recurrent angina in patients with no need for secondary revascularization [J]. World Journal of Emergency Medicine, 2021, 12(1): 42-47. |
| [8] | Rui-xue Sun, Priscilla Song, Joseph Walline, He Wang, Ying-chun Xu, Hua-dong Zhu, Xue-zhong Yu, Jun Xu. Morbidity and mortality risk factors in emergency department patients with Acinetobacter baumannii bacteremia [J]. World Journal of Emergency Medicine, 2020, 11(3): 164-168. |
| [9] | Shao-hua Liu, Huo-yan Liang, Hong-yi Li, Xian-fei Ding, Tong-wen Sun, Jing Wang. Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies [J]. World Journal of Emergency Medicine, 2020, 11(2): 109-116. |
| [10] | Wei He, Yue-yang You, Kai Sun, Chen Xie, Yue Ming, Li-na Yu, Feng-jiang Zhang, Min Yan. Admission delay is associated with worse surgical outcomes for elderly hip fracture patients: A retrospective observational study [J]. World Journal of Emergency Medicine, 2020, 11(1): 27-32. |
| [11] | Chang Pan, Xiao-ran Huang, Jiao-jiao Pang, Kai Cheng, Feng Xu, Yu-guo Chen. Trends in mortality of emergency departments patients in China [J]. World Journal of Emergency Medicine, 2019, 10(3): 152-155. |
| [12] | Yuzeng Shen, Yee Chien Tay, Edward Wee Kwan Teo, Nan Liu, Shao Wei Lam, Marcus Eng Hock Ong. Association between the elderly frequent attender to the emergency department and 30-day mortality: A retrospective study over 10 years [J]. World Journal of Emergency Medicine, 2018, 9(1): 20-25. |
| [13] | Kasim Turgut, Mehmet Ediz Sarihan, Cemil Colak, Taner Güven, Ali Gür, Sükrü Gürbüz. Falls from height: A retrospective analysis [J]. World Journal of Emergency Medicine, 2018, 9(1): 46-50. |
| [14] | Youichi Yanagawa, Kouhei Ishikawa, Kei Jitsuiki, Toshihiko Yoshizawa, Yasumasa Oode, Kazuhiko Omori, Hiromichi Ohsaka. Fibrinogen degradation product levels on arrival for trauma patients requiring a transfusion even without head injury [J]. World Journal of Emergency Medicine, 2017, 8(2): 106-109. |
| [15] | Egemen Küçük, İbrahim Kocayiğit, Candan Günel, Hasan Düzenli. Neutrophil-to-lymphocyte ratio in occlusive vascular diseases: the literature review of the past 10 years [J]. World Journal of Emergency Medicine, 2016, 7(3): 165-172. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
