
Mortality Prediction of COVID-19 Patients Using Radiomic and Neural Network Features Extracted from a Wide Chest X-ray Sample Size: A Robust Approach for Different Medical Imbalanced Scenarios

 , , , , , , ,
, , , , , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
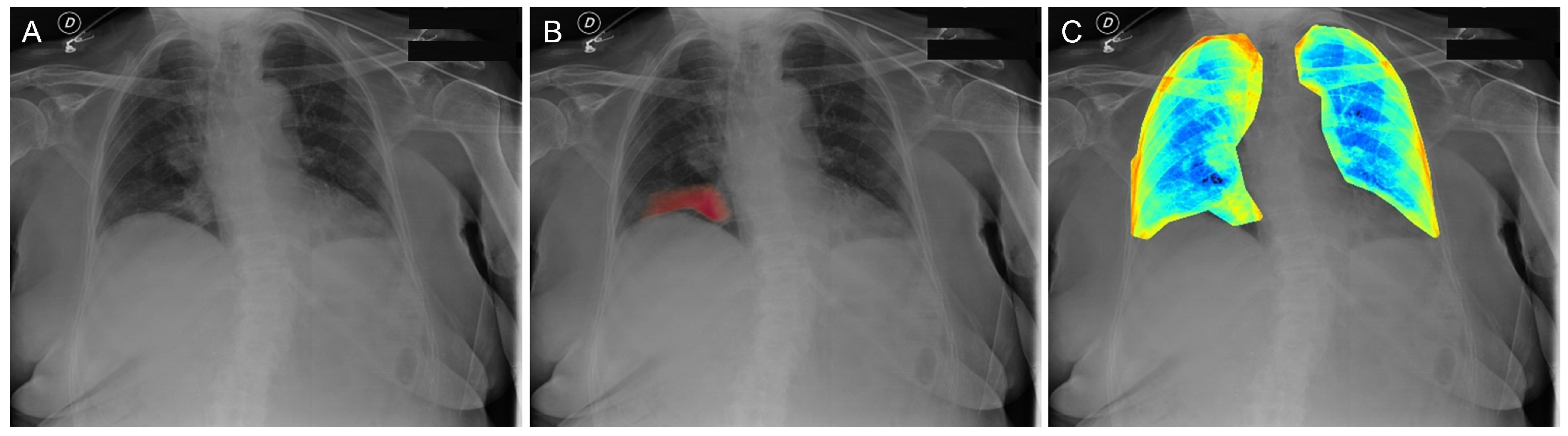
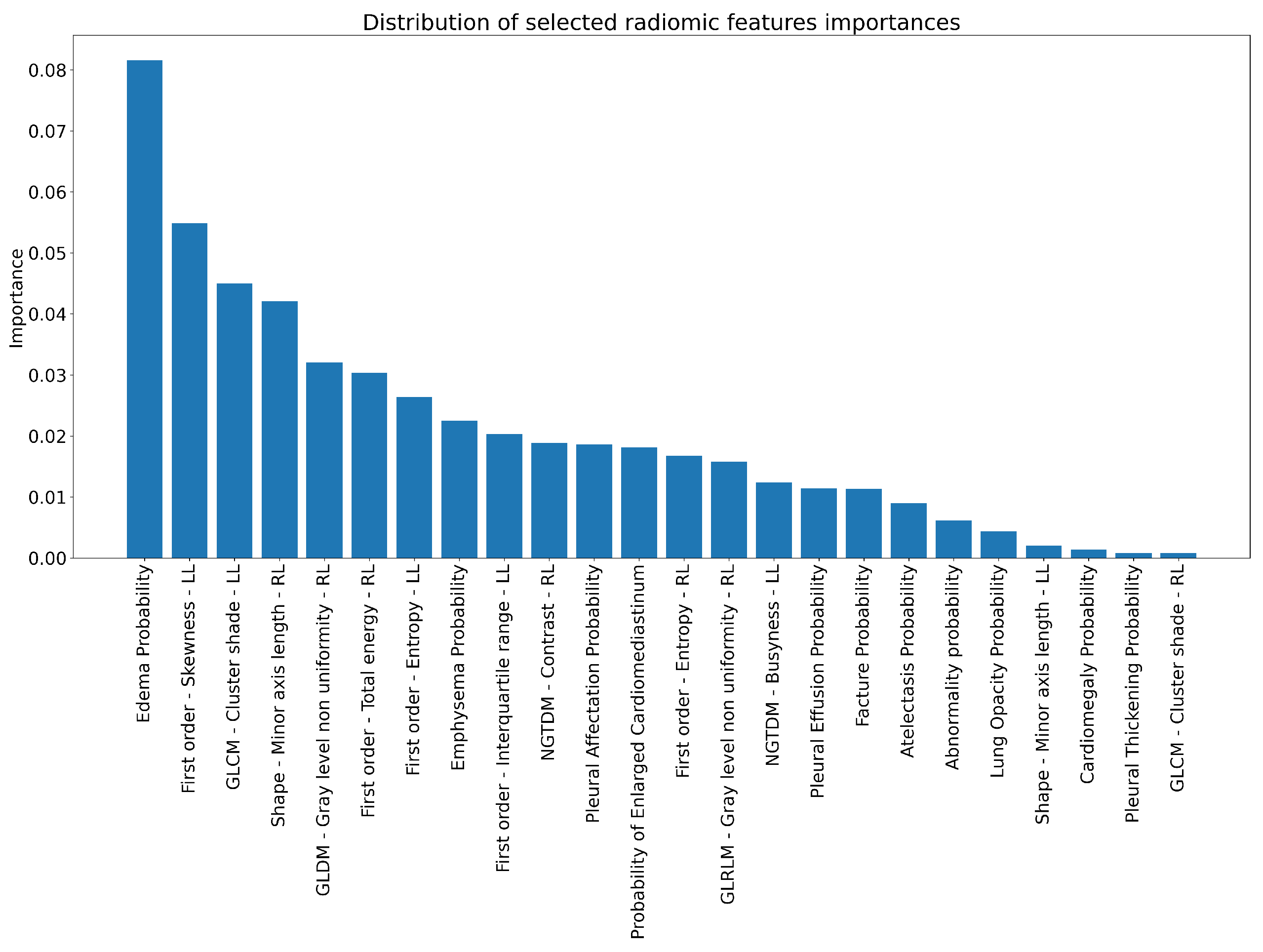
2.2. Radiomic Features Collection and Neural Network Findings
2.3. Pipeline
3. Results
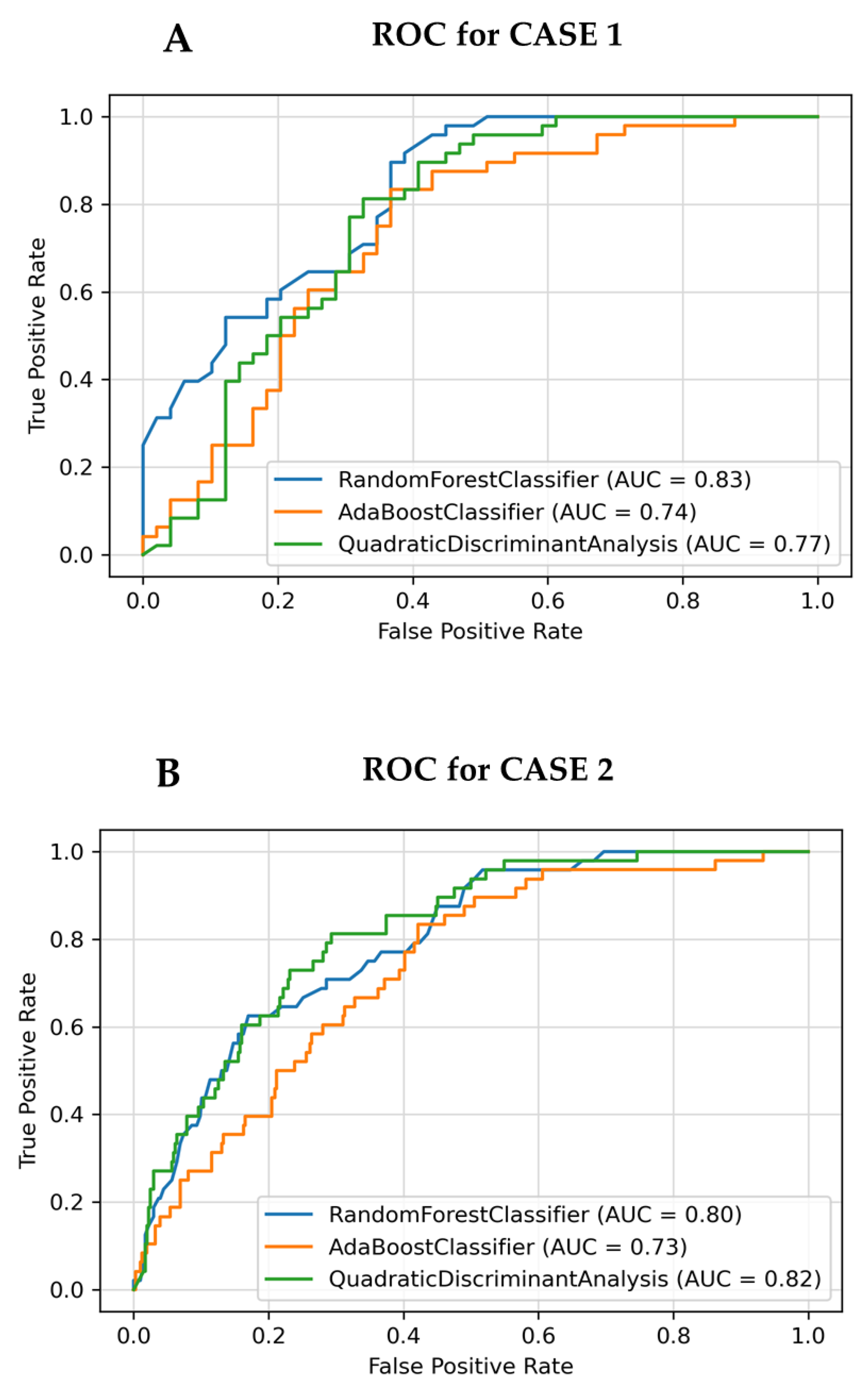
3.1. Case 1: Testing on Balanced Case
3.2. Case 2: Testing on Imbalanced Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China. N. Engl. J. Med. 2019, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, Z.; Wang, G.; Lau, J.Y.N.; Zhang, K.; Li, W. COVID-19 in early 2021: Current status and looking forward. Signal Transduct. Target. Ther. 2021, 6, 114. [Google Scholar] [CrossRef] [PubMed]
- Soda, P.; Natascha, C.D.; Tessadori, J.; Giovanni, V.; Valerio, G.; Chandra, B.; Muhammad, U.A.; Rosa, S.; Ermanno, C.; Deborah, F.; et al. AIforCOVID: Predicting the clinical outcomes in patients with COVID-19 applying AI to chest-X-rays. An Italian multicentre study. Med. Image Anal. 2021, 74, 102216. [Google Scholar] [CrossRef] [PubMed]
- Laino, M.E.; Ammirabile, A.; Posa, A.; Cancian, P.; Shalaby, S.; Savevski, V.; Neri, E. The Applications of Artificial Intelligence in Chest Imaging of COVID-19 Patients: A Literature Review. Diagnostics 2021, 11, 1317. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.; Chouhan, R.S.; Shahdeo, D.; Shrikrishna, N.S.; Kesarwani, V.; Horvat, M.; Gandhi, S. A Recent Update on Advanced Molecular Diagnostic Techniques for COVID-19 Pandemic: An Overview. Front. Immunol. 2021, 12, 5316. [Google Scholar] [CrossRef]
- Dhar, B.C. Diagnostic assay and technology advancement for detecting SARS-CoV-2 infections causing the COVID-19 pandemic. Anal. Bioanal. Chem. 2022, 414, 2903–2934. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Chen, Q.; Li, J.; Liu, Z. Diagnostic techniques for COVID-19: A mini-review. J. Virol. Methods 2022, 301, 114437. [Google Scholar] [CrossRef]
- Neri, E.; Miele, V.; Coppola, F.; Grassi, R. Use of CT and artificial intelligence in suspected or COVID-19 positive patients: Statement of the Italian Society of Medical and Interventional Radiology. La Radiol. Med. 2020, 125, 505–508. [Google Scholar] [CrossRef]
- Grassi, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Giacobbe, G.; Fusco, R.; Granata, V.; Petrillo, A.; Sacco, P.; et al. COVID-19 pneumonia: Computer-aided quantification of healthy lung parenchyma, emphysema, ground glass and consolidation on chest computed tomography (CT). La Radiol. Med. 2020, 126, 3. [Google Scholar] [CrossRef]
- Islam, N.; Ebrahimzadeh, S.; Salameh, J.P.; Kazi, S.; Fabiano, N.; Treanor, L.; Absi, M.; Hallgrimson, Z.; Leeflang, M.; Hooft, L.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2021, 9, CD013639. [Google Scholar]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, I.; Arabi, H.; Salimi, Y.; Sanaat, A.H.; Akhavanalaf, A.; Hajianfar, G.; Askari, D.; Moradi, S.; Mansouri, Z.; Pakbin, M.; et al. COLI-NET: Fully Automated COVID-19 Lung and Infection Pneumonia Lesion Detection and Segmentation from Chest CT Images. medRxiv 2021. [Google Scholar] [CrossRef]
- Calderon-Ramirez, S.; Yang, S.; Moemeni, A.; Elizondo, D.; Colreavy-Donnelly, S.; Chavarría-Estrada, L.; Molina-Cabello, M. Correcting Data Imbalance for Semi-Supervised Covid-19 Detection Using X-ray Chest Images. arXiv 2020, arXiv:2008.08496. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Rajendra Acharya, U. Automated detection of COVID-19 cases using deep neural networks with Xray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Win, K.; Maneerat, N.; Sreng, S.; Hamamoto, K. Ensemble Deep Learning for the Detection of COVID-19 in Unbalanced Chest X-ray Dataset. Appl. Sci. 2021, 11, 10528. [Google Scholar] [CrossRef]
- Bridge, J.; Meng, Y.; Zhao, Y.; Du, Y.; Zhao, M.; Sun, R.; Zheng, Y. Introducing the GEV Activation Function for Highly Unbalanced Data to Develop COVID-19 Diagnostic Models. IEEE J. Biomed. Health Inform. 2020, 24, 2776–2786. [Google Scholar] [CrossRef]
- Bae, J.; Kapse, S.; Singh, G.; Gattu, R.; Ali, S.; Shah, N.; Marshal, C.; Pierce, J.; Phatak, T.; Gupta, A.; et al. Predicting Mechanical Ventilation and Mortality in COVID-19 Using Radiomics and Deep Learning on Chest Radiographs: A Multi-Institutional Study. Diagnostics 2021, 11, 1812. [Google Scholar] [CrossRef]
- Jiao, Z.; Choi, J.W.; Halsey, K.; Tran, T.M.L.; Hsieh, B.; Wang, D.; Eweje, F.; Wang, R.; Chang, K.; Wu, J.; et al. Prognostication of patients with COVID-19 using artificial intelligence based on chest x-rays and clinical data: A retrospective study. Lancet Digit. Health 2021, 3, e286–e294. [Google Scholar] [CrossRef]
- Varghese, B.A.; Shin, H.; Desai, B.; Gholamrezanezhad, A.; Lei, X.; Perkins, M.; Oberai, A.; Nanda, N.; Cen, S.; Duddalwar, V. Predicting clinical outcomes in COVID-19 using radiomics on chest radiographs. Br. J. Radiol. 2021, 94, 20210221. [Google Scholar] [CrossRef]
- An, C.; Lim, H.; Kim, D.; Chang, J.H.; Choi, Y.J.; Kim, S.W. Machine learning prediction for mortality of patients diagnosed with COVID-19: A nationwide Korean cohort study. Sci. Rep. 2020, 10, 18716. [Google Scholar] [CrossRef]
- Oladunni, T.; Tossou, S.; Haile, Y.; Kidane, A. COVID-19 County Level Severity Classification with Imbalanced Dataset: A NearMiss Under-sampling Approach. medRxiv 2021. [Google Scholar] [CrossRef]
- De Souza, F.S.H.; Hojo-Souza, N.S.; Dos Santos, E.B.; Da Silva, C.M.; Guidoni, D.L. Predicting the Disease Outcome in COVID-19 Positive Patients Through Machine Learning: A Retrospective Cohort Study with Brazilian Data. Front. Artif. Intell. 2021, 4, 2624–8212. [Google Scholar] [CrossRef] [PubMed]
- Shiri, I.; Salimi, Y.; Pakbin, M.; Hajianfar, G.; Avval, A.H.; Sanaat, A.; Mo-stafaei, S.; Akhavanallaf, A.; Saberi, A.; Mansouri, Z.; et al. COVID-19 Prognostic Modeling Using CT Radiomic Features and Machine Learning Algorithms: Analysis of a Mul-ti-Institutional Dataset of 14,339 Patients. Physica A 2021, 145, 105467. [Google Scholar] [CrossRef]
- Shiri, I.; Sorouri, M.; Geramifar, P.; Nazari, M.; Abdollahi, M.; Salimi, Y.; Khosravi, B.; Askari, D.; Aghaghazvini, L.; Hajianfar, G.; et al. Machine learning-based prognostic modeling using clinical data and quantitative radiomic features from chest CT images in COVID-19 patients. Comput. Biol. Med. 2021, 132, 104304. [Google Scholar] [CrossRef] [PubMed]
- Bottino, F.; Tagliente, E.; Pasquini, L.; Napoli, A.; Lucignani, M.; Figà-Talamanca, L.; Napolitano, A. COVID Mortality Prediction with Machine Learning Methods: A Systematic Review and Critical Appraisal. J. Pers. Med. 2021, 11, 893. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Y.; Qian, Z.; Sun, Z.; Xu, K.; Wang, K.; Liu, S.; Fan, X.; Li, S.; Zhang, Z.; et al. A radiomic signature as a non-invasive predictor of progression-free survival in patients with lower-grade gliomas. Neuroimage Clin. 2018, 20, 1070–1077. [Google Scholar] [CrossRef]
- Forghani, R.; Savadjiev, P.; Chatterjee, A.; Muthukrishnan, N.; Reinhold, C.; Forghania, B. Radiomics and Artificial Intelligence for Biomarker and Prediction Model Development in Oncology. Comput. Struct. Biotechnol. J. 2019, 17, 995–1008. [Google Scholar] [CrossRef]
- Bera, K.; Braman, N.; Gupta, A.; Velcheti, V.; Madabhushi, A. Predicting cancer outcomes with radiomics and artificial intelligence in radiology. Nat. Rev. Clin. Oncol. 2021, 19, 132–146. [Google Scholar] [CrossRef]
- Ahmed, S.; Yap, M.H.; Tan, M.; Hasan, M.K. ReCoNet: Multi-level Preprocessing of Chest X-rays for COVID-19 Detection Using Convolutional Neural Networks. medRxiv 2020. [Google Scholar] [CrossRef]
- Rahman, M.; Davis, D.N. Addressing the Class Imbalance Problem in Medical Datasets. Int. J. Mach. Learn. Comput. 2013, 3, 224. [Google Scholar] [CrossRef]
- Thabtah, F.; Hammoud, S.; Kamalov, F.; Gonsalves, A. Data imbalance in classification: Experimental evaluation. Inf. Sci. 2020, 513, 429–441. [Google Scholar] [CrossRef]
- Dorn, M.; Grisci, B.; Narloch, P.; Feltes, B.C.; Avila, E.; Kahmann, A.; Alho, C. Comparison of machine learning techniques to handle imbalanced COVID-19 CBC datasets. PeerJ Comput. Sci. 2021, 7, e670. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Du, R.; Ho, J.; Pang, H.; Chiu, W.H.; Lee, E.; Vardhanabhuti, V. Effect of machine learning re-sampling techniques for imbalanced datasets in 18F-FDG PET-based radiomics model on prog-nostication performance in cohorts of head and neck cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2826–2835. [Google Scholar] [CrossRef]
- Nejatian, S.; Parvin, H.; Faraji, E. Using sub-sampling and ensemble clustering techniques to improve performance of imbalanced classification. Neurocomputing 2018, 276, 55–66. [Google Scholar] [CrossRef]
- Avanzo, M.; Trianni, A.; Botta, F.; Talamonti, C.; Stasi, M.; Iori, M. Artificial Intelligence and the Medical Physicist: Welcome to the Machine. Appl. Sci. 2021, 11, 1691. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Gabelloni, M.; De Vietro, F.; Mendola, V.; Cattabriga, A.; Cocozza, M.A.; Vara, G.; Piccinino, A.; Lo Monaco, S.; et al. Human, All Too Human? An All-Around Appraisal of the “Artificial Intelligence Revolution” in Medical Imaging. Front. Psychol. 2021, 12, 4296. [Google Scholar] [CrossRef]
- Liang, C.; Liu, Y.; Wu, M.; Garcia-Castro, F.; Alberich-Bayarri, A.; Wu, F. Identifying pulmonary nodules or masses on chest radiography using deep learning: External validation and strategies to improve clinical practice. Clin. Radiol. 2019, 38–45. [Google Scholar] [CrossRef] [Green Version]
- ISS. Available online: https://www.iss.it/en/web/guest/home (accessed on 14 September 2021).
- Infn. Available online: https://covid19.infn.it/iss/ (accessed on 17 September 2021).
- Scotland, P.H. Scottish Intensive Care Society Audit Group Report on COVID-19. Available online: https://publichealthscotland.scot/media/11407/2022-02-02_sicsag_report.pdf (accessed on 14 September 2021).
- Carbonell, R.; Urgelés, S.; Rodriguez, A.; Bodí, M.; Martin-Loeches, I.; Violán, J.; Diaz, E.; Gómez, J.; Trefler, S.; Vallverdú, M.; et al. Mortality comparison between the first and second/third waves among 3795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. Lancet Reg. Health Eur. 2021, 11, 100243. [Google Scholar] [CrossRef]
- ISS. Available online: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-analysis-of-deaths (accessed on 14 September 2021).
- Armstrong, R.; Kane, A.; Cook, T. Outcomes from intensive care in patients with COVID-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 16. [Google Scholar] [CrossRef] [Green Version]
- Nardin, M.D. Available online: https://www.med4.care/covid-19-mortalita-in-terapia-intensiva (accessed on 17 September 2021).
- Tamal, M.; Alshammari, M.; Alabdullah, M.; Hourani, R.; Alola, H.; Hegazi, T. An integrated framework with machine learning and radiomics for accurate and rapid early diagnosis of COVID-19 from Chest X-ray. Expert Syst. Appl. 2021, 180, 115152. [Google Scholar] [CrossRef] [PubMed]
- Thanh Noi, P.; Kappas, M. Comparison of Random Forest, k-Nearest Neighbor, and Support Vector Machine Classifiers for Land Cover Classification Using Sentinel-2 Imagery. Sens. Basel 2017, 18, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donini, B.; Rivetti, S.; Lanconelli, N.; Bertolini, M. Free software for performing physical analysis of systems for digital radiography and mammography. Med. Phys. 2014, 41, 051903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitrosi, A.; Bertolini, M.; Borasi, G.; Botti, A.; Barani, A.; Rivetti, S.; Pierotti, L. Application of QC_DR Software for Acceptance Testing and Routine Quality Control of Direct Digital Radiography Systems: Initial Experiences using the Italian Association of Physicist in Medicine Quality Control Protocol. J. Digit. Imaging 2009, 22, 656Y666. [Google Scholar] [CrossRef] [Green Version]
- Classifier, Q.C.X.R. Available online: https://quibim.com/biomarker/chest-xray-classifier/ (accessed on 30 November 2021).
- Awal, M.A.; Masud, M.; Hossain, M.S.; Bulbul, A.A.M.; Mahmud, S.M.H.; Bairagi, A.K. A Novel Bayesian Optimization-Based Machine Learning Framework for COVID-19 Detection From Inpatient Facility Data. IEEE Access 2021, 9, 10263–10281. [Google Scholar] [CrossRef]
- Matthew, S. Available online: https://towardsdatascience.com/guide-to-classification-on-imbalanced-datasets-d6653aa5fa23 (accessed on 1 November 2021).
- Laurikkala, J. Improving Identification of Difficult Small Classes by Balancing Class Distribution. In Proceedings of the Conference on Artificial Intelligence in Medicine in Europe, Cascais, Portugal, 1–4 July 2001; Volume 2101, pp. 63–66. [Google Scholar]
- Chawla, N.; Japkowicz, N.; Kołcz, A. Editorial: Special issue on learning from imbalanced data sets, SIGKDD Explorations Special Issue on Learning from Imbalanced Datasets. ACM SIGKDD Explor. Newsl. 2004, 6, 1–6. [Google Scholar] [CrossRef]
- Sun, Y.; Wong, A.; Kamel, M.S. Classification of imbalanced data: A review. Int. J. Pattern Recognit. Artif. Intell. 2009, 23, 687–719. [Google Scholar] [CrossRef]
- Van Hulse, J.; Khoshgoftaar, T.M.; Napolitano, A. An Empirical Comparison of Repetitive Undersampling Techniques. In Proceedings of the 2009 IEEE International Conference on Information Reuse & Integration, Las Vegas, NV, USA, 10–12 August 2009; pp. 29–34. [Google Scholar]
- An, C.; Park, Y.W.; Ahn, S.; Han, K.; Kim, H.; Lee, S.K. Radiomics machine learning study with a small sample size: Single random training-test set split may lead to unreliable results. PLoS ONE 2021, 16, e0256152. [Google Scholar] [CrossRef]
- Zhang, J.; Mani, I. KNN Approach to Unbalanced Data Distributions: A Case Study Involving Information Extraction. Proc. ICML 2003, 126, 1–7. [Google Scholar]
- Xie, Y.; Qiu, M.; Zhang, H.; Peng, L.; Chen, Z. Gaussian Distribution Based Oversampling for Imbalanced Data Classification. IEEE Trans. Knowl. Data Eng. 2022, 34, 667–679. [Google Scholar] [CrossRef]
- Du, G.; Zhang, J.; Jiang, M.; Long, J.; Lin, Y.; Li, S.; Tan, K.C. Graph-Based Class-Imbalance Learning with Label Enhancement. IEEE Trans. Neural Netw. Learn. Syst. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Cao, W.; Gao, Z.; Bian, J.; Chen, H.; Chang, Y.; Liu, T.Y. Self-paced Ensemble for Highly Imbalanced Massive Data Classification. In Proceedings of the 2020 IEEE 36th International Conference on Data Engineering (ICDE), Dallas, TX, USA, 20–24 April 2020; pp. 841–852. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population Features | Number |
|---|---|
| Total patients | 1816 |
| Survived patients | 1622 (89%) |
| Dead patients | 194 (11%) |
| Mean Age ± sd [min–max] | 63 ± 16 [18–100] |
| Mean Survived Age ± sd [min–max] | 61 ± 16 [18–99] |
| Mean Dead Age ± sd [min–max] | 80 ± 10 [45–100] |
| Women | 799 (44%) |
| Dead women | 60 (8%) |
| Men | 1017 (56%) |
| Dead men | 134 (13%) |
| Case 1 | Case 2 | |||||
|---|---|---|---|---|---|---|
| Testing on Balanced | Testing on Imbalanced | |||||
| RF | ADA | QDA | RF | ADA | QDA | |
| ACC | 0.72 ± 0.01 | 0.63 ± 0.01 | 0.71 ± 0.01 | 0.70 ± 0.04 | 0.64 ± 0.05 | 0.79 ± 0.04 |
| AUC | 0.82 ± 0.02 | 0.64 ± 0.03 | 0.74 ± 0.03 | 0.79 ± 0.03 | 0.68 ± 0.05 | 0.78 ± 0.04 |
| AP | 0.77 ± 0.06 | 0.58 ± 0.05 | 0.65 ± 0.05 | 0.27 ± 0.04 | 0.16 ± 0.05 | 0.22 ± 0.05 |
| SENS | 0.84 ± 0.04 | 0.68 ± 0.06 | 0.65 ± 0.07 | 0.76 ± 0.06 | 0.58 ± 0.08 | 0.45 ± 0.08 |
| SPEC | 0.60 ± 0.01 | 0.57 ± 0.01 | 0.75 ± 0.01 | 0.70 ± 0.06 | 0.65 ± 0.06 | 0.83 ± 0.06 |
| TN (%) | 33.9 | 38.5 | 38.5 | 63.2 | 62.8 | 74.0 |
| FN (%) | 12.3 | 15.4 | 21.6 | 2.3 | 3.0 | 3.3 |
| TP (%) | 40.0 | 36.9 | 30.8 | 7.9 | 7.6 | 6.9 |
| FP (%) | 13.9 | 9.2 | 9.2 | 26.6 | 26.6 | 15.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iori, M.; Di Castelnuovo, C.; Verzellesi, L.; Meglioli, G.; Lippolis, D.G.; Nitrosi, A.; Monelli, F.; Besutti, G.; Trojani, V.; Bertolini, M.; et al. Mortality Prediction of COVID-19 Patients Using Radiomic and Neural Network Features Extracted from a Wide Chest X-ray Sample Size: A Robust Approach for Different Medical Imbalanced Scenarios. Appl. Sci. 2022, 12, 3903. https://doi.org/10.3390/app12083903
Iori M, Di Castelnuovo C, Verzellesi L, Meglioli G, Lippolis DG, Nitrosi A, Monelli F, Besutti G, Trojani V, Bertolini M, et al. Mortality Prediction of COVID-19 Patients Using Radiomic and Neural Network Features Extracted from a Wide Chest X-ray Sample Size: A Robust Approach for Different Medical Imbalanced Scenarios. Applied Sciences. 2022; 12(8):3903. https://doi.org/10.3390/app12083903
Chicago/Turabian StyleIori, Mauro, Carlo Di Castelnuovo, Laura Verzellesi, Greta Meglioli, Davide Giosuè Lippolis, Andrea Nitrosi, Filippo Monelli, Giulia Besutti, Valeria Trojani, Marco Bertolini, and et al. 2022. "Mortality Prediction of COVID-19 Patients Using Radiomic and Neural Network Features Extracted from a Wide Chest X-ray Sample Size: A Robust Approach for Different Medical Imbalanced Scenarios" Applied Sciences 12, no. 8: 3903. https://doi.org/10.3390/app12083903