
‘I Live a Kind of Shadow Life’: Individual Experiences of COVID-19 Recovery and the Impact on Physical Activity Levels

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Analysis
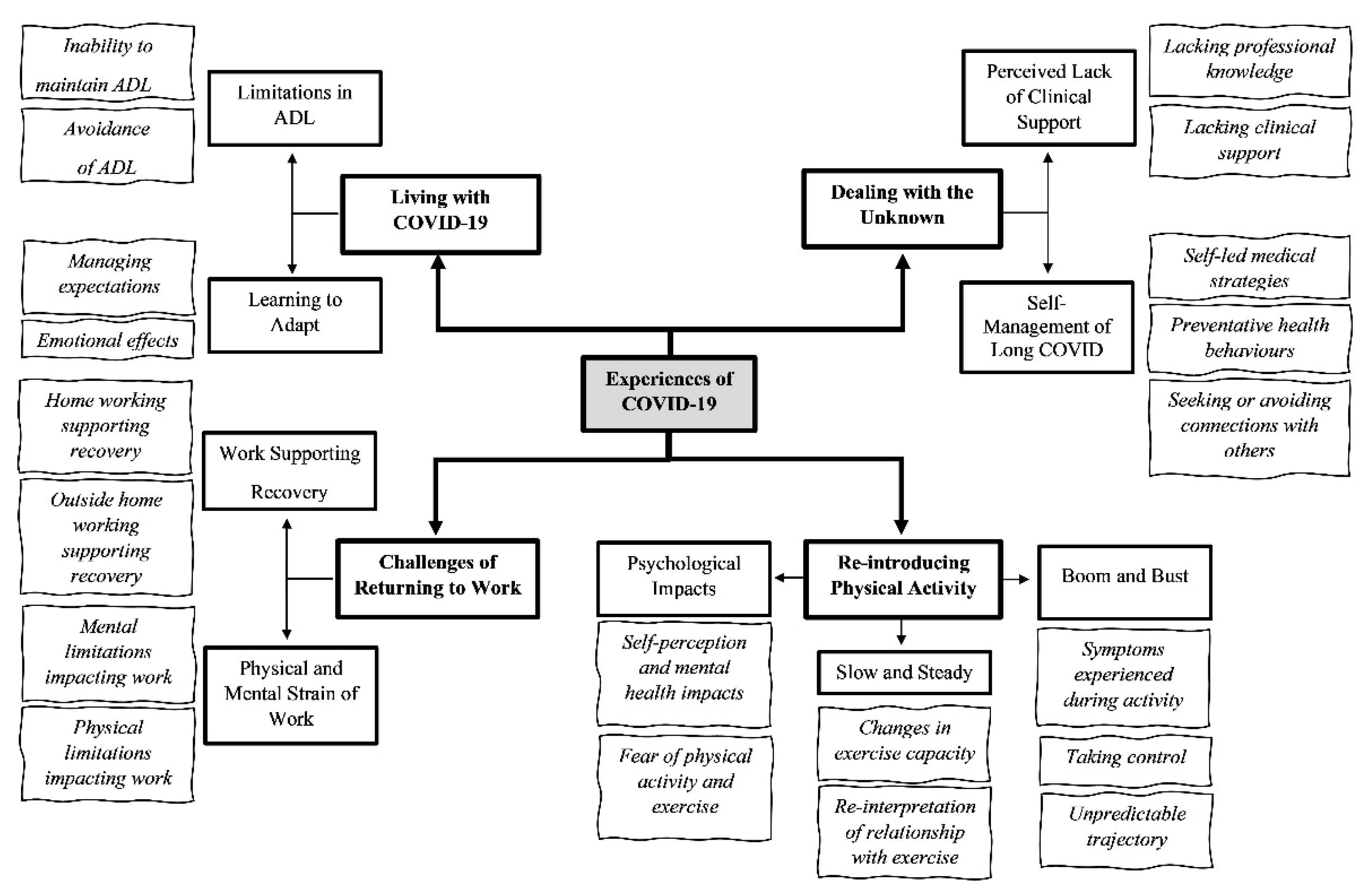
3. Results
3.1. Pre-COVID-19 Physical Activity
‘Prior to getting COVID, I would have put myself in a fit category’ (F01; 7 months post-infection)
‘I couldn’t live without it, yeah…I guess it’s the thing that gives me joy in life; it’s an inseparable part of me’ (F14; 10 months post-infection)
‘I have a medical condition anyway, which does cause some fatigue…I do think that having had the pre-existing health condition has helped me quite a bit because my ability to be patient and just try and accept things as they are and do what I can. I already had to do pacing, for example, whereas a lot of people have been having to get their heads around that for the first time ever, that have got ill with kind of long COVID symptoms’ (F09; 10 months post-infection)
3.2. ‘A Part of Our Everyday Lives’: Living with COVID-19
3.2.1. Limitations in Activities of Daily Living
‘Your body, it shuts down, you lift your arms up, every, everything you do, to go to the toilet, to make a cup of tea, is an effort’ (M02; 6 months post-infection)
‘…if I’m trying to move or do any activities, the breathlessness that’s the… problem’ (F05; 10 months post-infection)
‘Yeah, you are very, very, very tired and, for me to go to the shop… is, too much, couldn’t do it’ (M02; 6 months post-infection)
‘I haven’t made a cup of tea since March… I haven’t done anything, I haven’t made a meal, haven’t made a cup of tea, I tried, oh my gosh, I tried changing a pillowcase, oh my gosh, that’s hard, it’s so hard. No seriously, it’s really hard. I folded up four jumpers…I folded four and I was short of breath’ (F05; 10 months post-infection)
‘I’m worried about that in terms of doing any sort of strength work, I think that, if I go shopping and have heavy shopping, I, I worry if that’s like a, a kind of trigger…’ (F04; 7 months post-infection)
‘So, I mean I’ve been super cautious and although everyone has said “don’t worry you’ve had it”, I think I’ve probably been over cautious. I mean, because of that, I’ve hardly done any driving because I’ve just not been out and about and I’ve not done the usual, the shops or anything like that. I don’t think I’ve done a single supermarket shop. So, in that respect, I’m not doing the usual kind of everyday activities anyway because I don’t particularly want to go out.’ (F08; 10 months post-infection)
‘…yeah, I don’t know, it doesn’t, it doesn’t make sense this illness in terms of what the specific triggers are when I push it, whether that’s, you know, a physical thing… I know it’s physical because I know that, when I was pushing it early on, I would end up back in bed’ (F04; 7 months post-infection)
3.2.2. Learning to Adapt
‘It’s like, if you have the energy, you just, you suddenly find yourself doing more, but then you sort of do too much, so the pacing thing really has been quite crucial to, you know, being able to do most things’ (M13; 11 months post-infection)
‘It’s amazing how much you normalise avoiding stuff that you can’t handle’ (F05; 10 months post-infection)
‘I was so frustrated I just wasn’t able to do stuff’’ (F05; 10 months post-infection)
‘I think when you go for weeks and weeks and there’s no real difference you can put your finger on, in terms of improvement, you just think, “Well, is this it now? Is this just me now?”’ (F09; 10 months post-infection)
‘I fully expected, at some point, I’ll start to feel better and that this, you know, there may or may not be a long-term effect on the lungs but, if there is, then this is something I can deal with’ (F03; 7 months post-infection)
3.3. ‘So Frightening’: Dealing with the Unknown
3.3.1. Perceived Lack of Clinical Support
‘Whenever I speak to the [general practitioner] GP, the poor GPs have not been any help at all, and I think they’re quite open. They say “we don’t know what’s wrong” (F08; 10 months post-infection)
‘I’m very lucky in that the GPs have been understanding, although not actually been able to provide any solutions, but they have been understanding and not dismissive’ (F10; 7 months post-infection)
‘I found it a struggle talking to my doctors, I felt like I wasn’t being believed, like I was just, you know, making stuff up or bigging things up’ (F14; 10 months post-infection)
‘…I then contacted my doctor because I thought that was an issue with my iron levels, who took the iron with thyroid issues, the thyroid was also fine. My doctor said that she can’t do anything else. I contacted another doctor, had, a full range of blood tests and they came back fine as well. I also had a chest X-ray, which was also okay and now, the latest doctor, after, after all the blood tests and chest X-ray, is sending me to a post-COVID clinic…’ (F14; 10 months post-infection)
3.3.2. ‘Like, Nobody’s Really Interested’: Self-Management of COVID-19
Self-Led Medical Strategies
‘...facial exercises and massages for your lymph areas and everything and that’s been proven to work with chronic fatigue, so for the last week, I’ve been trying to do that, you know with hot and cold complexes, compresses on your spine’ (F05; 10 months post-infection)
Preventative Health Behaviours
‘I’m taking some vitamins and I’ve got a, a sort of over-the-counter antihistamines, which seems to help, ah actually… when the breathing was at its worst, I, there’s a, an over the counter nasal spray for, I think it’s a steroid something you take for hay fever, I don’t really get hay fever but I get a touch of it when the pollution is bad’ (M13; 11 months post-infection)
‘…what am I in control of and what am I not in control of’ (F01; 7 months post-infection)
Avoiding or Connecting with Others
‘...that’s been really helpful in terms of, you know, a bit of support for other people that are going through the same thing, because at, at the beginning, the scary thing was, why’s this happening, why is this not written about, what, you know, people are going to think I’m putting this on…’ (F04; 7 months post-infection)
‘I’ve seen some comments by people about like, “Well, if I had to live with this fatigue for the rest of my life I’d kill myself”, and I think, “Well, I live with fatigue and I will do for the rest of my life, so thanks for that”’ (F01; 7 months post-infection)
‘I’ve built up a little network of friends and I walk with friends so that it takes my mind off what I don’t, what I’m so scared about it becoming too, I don’t want to start internalising. So rather than going out on my own and thinking about stuff I go out with friends and then I can just talk and do the exercise without…and take my mind off the illness really.’ (F08; 10 months post-infection)
3.4. ‘I Can’t Rest Anymore’: Re-Introducing Physical Activity
3.4.1. Boom and Bust
‘…the first time I went for a walk was probably only two miles and I ended up going to bed for two to three hours afterwards’ (F06; 10 months post-infection)
‘…and we walked one lunchtime and then I walked home from work, which was three miles and then the next day, I tried to walk home again and I got halfway home and thought I was going to fall over, like collapse’ (F04; 7 months post-infection)
‘I went for a swim and then I had heart palpitations for about twenty hours, it was really unnerving and uncomfortable, so I rang my GP, she sent me off for an ECG, which was fine and it’s been followed up since then and I have no long term or nothing that’s a big deal… I basically didn’t do anything again for two weeks after that and the heart palpitations went away but I’ve been much more gentle on myself with exercise since then’ (F03; 7 months post-infection)
‘I’ve never had a sustained period of feeling well enough for a long enough period of time that’s made me think that I’m ready to do that and I’m too scared that I take a step back again’ (F04; 7 months post-infection)
‘They told me to walk then for fifteen minutes and well, I tell you what, I struggled…walking down’s not so bad but walking up is, the hill, is like oh no, no, no, no, no, but I am improving and to what I was back in, I say, in May’ (M02; 6 months post-infection)
‘…lung specialist…she suggested that I shouldn’t get back in the water yet because she’s treating her patients as though they have a post-viral pneumonia and she said she would never suggest that somebody with post-viral pneumonia would swim’ (F08; 10 months post-infection)
‘Thought I can’t rest anymore and sleep all day and night so started pushing myself to do shorter runs, yoga and home exercise’ (F14; 10 months post-infection)
‘On Sunday I got a bit cocky and I let it [heart rate] creep up to a ‘massive’ 130 [beats per minute] and I think that’s what hammered me, to be honest, so when I go back I’ll keep it low. I don’t have any breathing difficulties doing that but obviously I haven’t got close to threshold or been anaerobic for nine months now’ (M12; 10 months post-infection)
‘…the last time I went around the block I was a little bit short of breath before I began, had been for a couple of days, a little bit short of breath. And it was awful, I didn’t think I was going to get home. I was in quite a state by the time I managed to walk home. Just walking like a zombie and barely able to breathe and trudging to get home really. Which has frightened me in doing activity like that’ (F10; 7 months post-infection)
3.4.2. Slow and Steady
‘I’m alright with endurance things, so I can run slow and steady, that’s fine. And I do a little bit of speedwork now, but I can’t get as fast as I was pre COVID’ (F06; 10 months post-infection)
‘…in terms of, you know, power, I mean I don’t have the strength back that I used to have, you know, physically lifting things, you know, I used to do a few weights and stuff, you know, a few times a week, just at home but I haven’t been able to do that, I can lift the weights now but it’s just, it’s still too painful’ (M13; 11 months post-infection)
‘If I run upstairs really quickly by the time I’ve got to the top of the stairs I have to sit down and I have to recover.’ (F08; 10 months post-infection)
‘bizarrely, my swimming has been great this year, I don’t know why, I think I’m a bit faster actually, that kind of helps but, but I think swimming is also a very measured breathing actually… you can’t sprint when you swim in open water because you can never get out of breath because that’s, ruins the whole style, so it’s a very measured breathing’ (F03; 7 months post-infection)
‘I sort of accept the fact that running is hard, it’s harder now, but, I guess, I’m, you know, I guess I get, I get better sense of achievement because despite feeling worse, I’m still doing it’ (F14; 10 months post-infection)
3.4.3. Psychological Impacts
‘With the germs [in gyms] today, you’ve got to be very cautious’ (M02; 6 months post-infection)
‘I stopped cycling, even though everybody seemed to take it up, because I was struggling with my breath after I experienced some symptoms and I also believed in my own head that if I was breathing more heavily by doing exercise around the other people I might be taking it in—whether that’s right or wrong I don’t know. That’s what I thought at the time and nobody else could tell me otherwise’ (M07; 10 months post-infection)
‘…tried walking, the same thing happened and they [the GP] said, what you need to do is go back to like a five-minute walk on the flat and try not to overdo it, so you can try and go every day because my mood was dipping, so severe, severe depression’ (F01; 7 months post-infection)
‘So, it’s almost like everything’s gone on a go slow. I feel that some days I wake up and I almost feel like I’ve kind of jumped forward 20 or 30 years and I feel like a little old lady instead of the active mum that I was six months ago’ (F08; 10 months post-infection)
3.5. ‘I Can’t Really Work’: Challenges of Returning to Work
3.5.1. Physical and Mental Strain of Work
‘…My stock-in-trade is writing and using and testing outdoor equipment, so suddenly I can’t… if you can’t walk up a hill, you can’t test a rucksack, you can’t test boots, you can’t use this stuff and if you can’t use your brain to write stuff...effectively, it’s rendered me incapable of working’ (M12; 10 months post-infection)
‘Months afterwards extremely fatigued and falling asleep at the desk/taking power naps’ (F14; 10 months post-infection)
‘…with my team in work, I’ve got a lot of youngsters and, you know, where I’m normally, you, you know, in the front, come on, let’s go, not now…So it’s, I, I’m the one that’s trailing and it’s, and that’s not me, you know, alright you’ve got to allow for age, I know, but I’ve always been the first, let’s go for it, let’s go for it, you know and now, I’m, I’m saying, like let’s catch up all the time’ (M02; 6 months post-infection)
‘…with the brain fog, I… really am quite forgetful, like really badly, so I have to write everything down, so rather than stress about it... for work, I write everything and for every meeting, I’m just making notes on everything, so that has helped quite a lot’ (F11; 9 months post-infection)
3.5.2. Work Supporting Recovery
‘…the total hours I’m doing are probably about two thirds of what I would usually be doing and it’s all from home, so I don’t have the driving that I would usually have when I go to work, I don’t have the walking round an office that I would usually have, I’m not even going up and down the stairs more than once day and once I’m downstairs I stay downstairs, I’ve got my work laptop in the living room and I’m just doing what I can, very reduced workload’ (F09; 10 months post-infection)
‘I’ve started parking further away, to get a bit of exercise, so parking about a mile away from work, so I have a mile, two-mile walk, like a mile there and a mile back, just to try and gradually increase my fitness levels a bit’ (F04; 7 months post-infection)
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. COVID-19 Weekly Epidemiological Update 35; World Health Organization: Geneva, Switzerland, 2021; pp. 1–3. [Google Scholar]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rocke, J.; Hopkins, C.; Philpott, C.; Kumar, B.N. Is loss of sense of smell as a diagnostic marker in COVID-19: A Systematic Review and Meta-analysis. Authorea 2020, 45, 914–922. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence; Royal College of General Practitioners (RCGP); Healthcare Improvement Scotland. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19, NICE Guidelines; NICE: London, UK, 2020; pp. 1–35. [Google Scholar]
- Pope, C.; Ziebland, S.; Mays, N. Qualitative research in health care: Analysing qualitative data. BMJ 2000, 320, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Rooney, S.; Webster, A.; Paul, L. Systematic Review of Changes and Syndrome—Related Coronavirus Infection: Implications for COVID-19 Rehabilitation. Phys. Ther. 2020, 100, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, E.; Poole, R. Living with COVID-19 Second Review; NIHR: Twickenham, UK, 2021; p. 19. [Google Scholar]
- Delbressine, J.; Machado, F.; Goërtz, Y.; Van Herck, M.; Meys, R.; Houben-Wilke, S.; Burtin, C.; Franssen, F.; Spies, Y.; Vijlbrief, H.; et al. The Impact of Post-COVID-19 Syndrome on Self-Reported Physical Activity. Int. J. Environ. Res. Public Health 2021, 18, 6017. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, H.; Kilby, L.; Kudiersky, N.; Copeland, R. Long COVID and the role of physical activity: A qualitative study. BMJ Open 2021, 11, e047632. [Google Scholar] [CrossRef] [PubMed]
- Virginia, B.; Victoria, C. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar]
- Tracy, S.J. Qualitative quality: Eight a “big-tent” criteria for excellent qualitative research. Qual. Inq. 2010, 16, 837–851. [Google Scholar] [CrossRef] [Green Version]
- Francis, J.J.; Johnston, M.; Robertson, C.; Glidewell, L.; Entwistle, V.; Eccles, M.P.; Grimshaw, J. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health 2010, 25, 1229–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, M.H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post–COVID-19 Syndrome (Long Haul Syndrome): Description of a Multidisciplinary Clinic at Mayo Clinic and Characteristics of the Initial Patient Cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, M.; Kerai, G.; Ainslie, D. Coronavirus and the Social Impacts of ‘Long COVID’ on People’s Lives in Great Britain: 7 April to 13 June 2021; Office for National Statistics: Newport, Wales, 2021; pp. 1–21.
- Scharn, M.; Hengel, K.O.; Boot, C.R.L.; Burdorf, A.; Schuring, M.; Van Der Beek, A.J.; Robroek, S.J.W. Influence of chronic diseases on societal participation in paid work, volunteering and informal caregiving in Europe: A 12-year follow-up study. J. Epidemiol. Community Health 2018, 73, 136–141. [Google Scholar] [CrossRef] [PubMed]
- World Physiotherapy. World Physiotherapy Response to COVID-19 Briefing Paper 9. Safe. Rehabilitation Approaches for People Living with Long Covid: Physical Activity and Exercise; World Physiotherapy: London, UK, 2021. [Google Scholar]
- Smith, B. Generalizability in qualitative research: Misunderstandings, opportunities and recommendations for the sport and exercise sciences. Qual. Res. Sport Exerc. Health 2018, 10, 137–149. [Google Scholar] [CrossRef]


{kind=link}
| Criteria | Examples of Use within Current Research |
|---|---|
| (1) Worthy topic | The research is unquestionably timely, relevant, and important. |
| (2) Rich rigor | The sample is purposive and information-rich, producing dense accounts of their experiences. |
| (3) Sincerity | We reflected together as a research team on our own biases and shaped our analysis to acknowledge these; for instance, KAM acted as a critical friend to JH who conducted the main analysis, whilst JS and MAM reviewed suggested themes and representative quotations. This was enabled by, for instance, a transparent audit trail of the analysis maintained by JH and detailed transcriptions of interviews. |
| (4) Credibility | We present thick description and verbatim quotations, coupled with our triangulation through multiple analysts engaging with the data to present a credible account of the participants’ experiences. |
| (5) Ethical | Procedurally, our research adheres to ethical codes and processes, and we are also mindful of relational ethics by ensuring we authentically represent experiences of activity during recovery from COVID-19. |
| (6, 7, 8) Resonance, Significant Contribution, Meaningful Coherence | To a degree, these are discerned by the reader, but we aim to influence resonance and transferability through the use of evocative quotations, to present an interpretation of the practical and theoretical relevance of our findings in our Conclusion, and we present a clear and detailed account of our purpose, methods, and interpretation of findings for readers to assess meaningful coherence. |
| COVID; coronavirus disease | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shelley, J.; Hudson, J.; Mackintosh, K.A.; Saynor, Z.L.; Duckers, J.; Lewis, K.E.; Davies, G.A.; Berg, R.M.G.; McNarry, M.A. ‘I Live a Kind of Shadow Life’: Individual Experiences of COVID-19 Recovery and the Impact on Physical Activity Levels. Int. J. Environ. Res. Public Health 2021, 18, 11417. https://doi.org/10.3390/ijerph182111417
Shelley J, Hudson J, Mackintosh KA, Saynor ZL, Duckers J, Lewis KE, Davies GA, Berg RMG, McNarry MA. ‘I Live a Kind of Shadow Life’: Individual Experiences of COVID-19 Recovery and the Impact on Physical Activity Levels. International Journal of Environmental Research and Public Health. 2021; 18(21):11417. https://doi.org/10.3390/ijerph182111417
Chicago/Turabian StyleShelley, James, Joanne Hudson, Kelly A. Mackintosh, Zoe L. Saynor, Jamie Duckers, Keir E. Lewis, Gwyneth A. Davies, Ronan M. G. Berg, and Melitta A. McNarry. 2021. "‘I Live a Kind of Shadow Life’: Individual Experiences of COVID-19 Recovery and the Impact on Physical Activity Levels" International Journal of Environmental Research and Public Health 18, no. 21: 11417. https://doi.org/10.3390/ijerph182111417