
Towards Smart Healthcare: UAV-Based Optimized Path Planning for Delivering COVID-19 Self-Testing Kits Using Cutting Edge Technologies

 , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction and Background
2. Techniques for Collecting COVID-19 Patient Samples
3. Method and Material
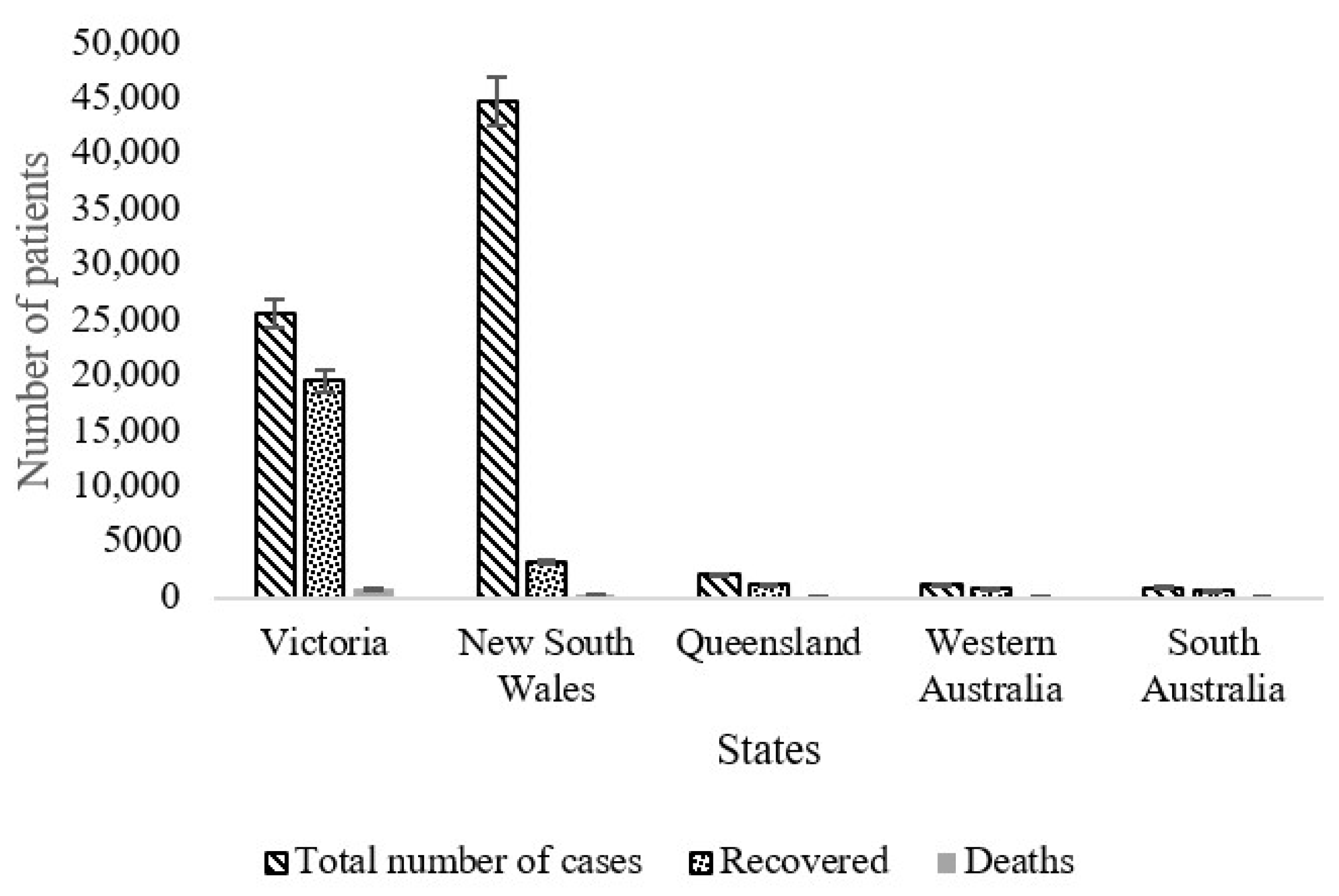
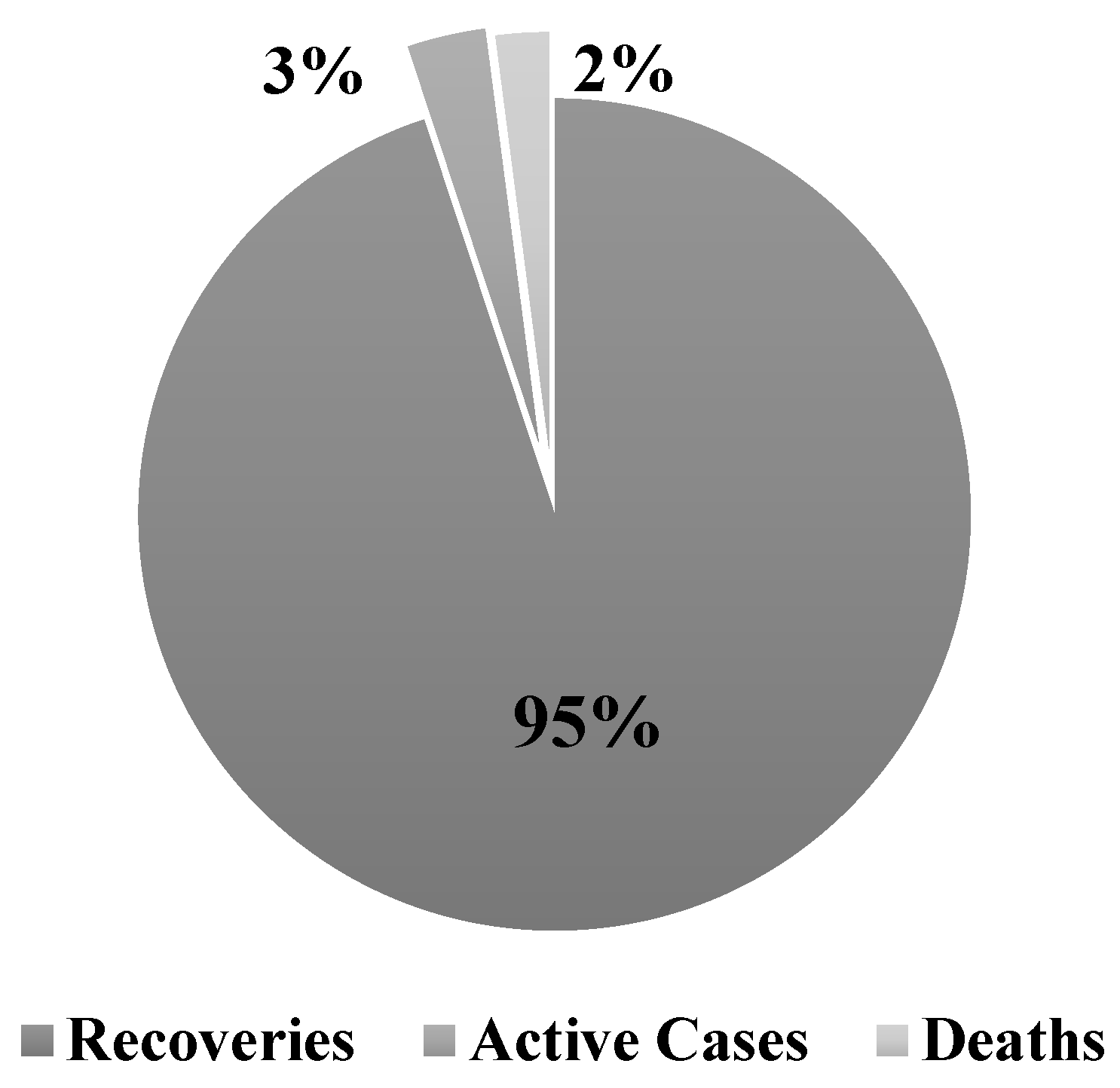
3.1. Case Study Area, Sample Delivery, and Collection
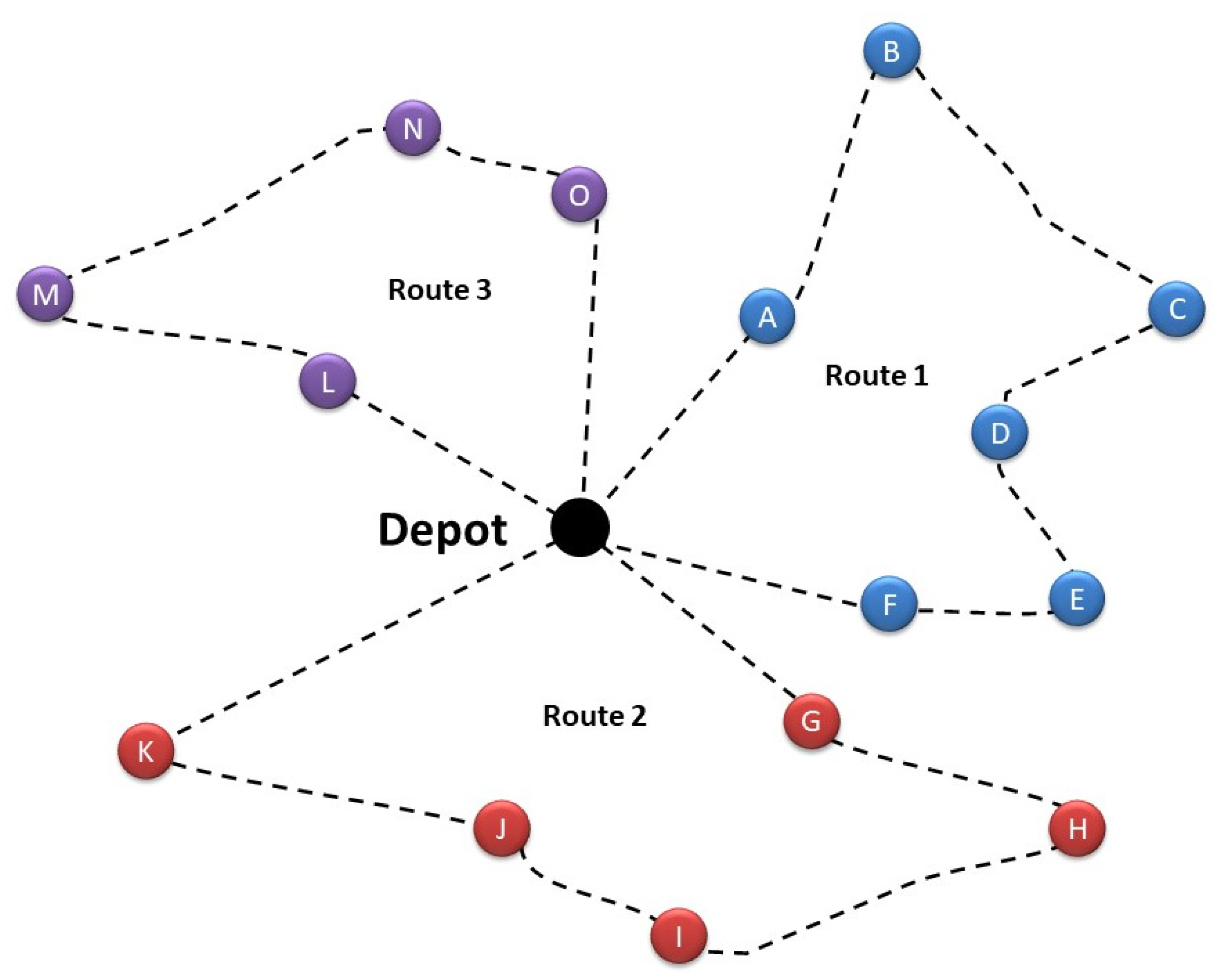
Proposed Model
- Each route starts and ends at the same location
- the depot and node 0, , i.e., and ⊆ N\{0}, and
- Each node is visited by one drone, i.e.,
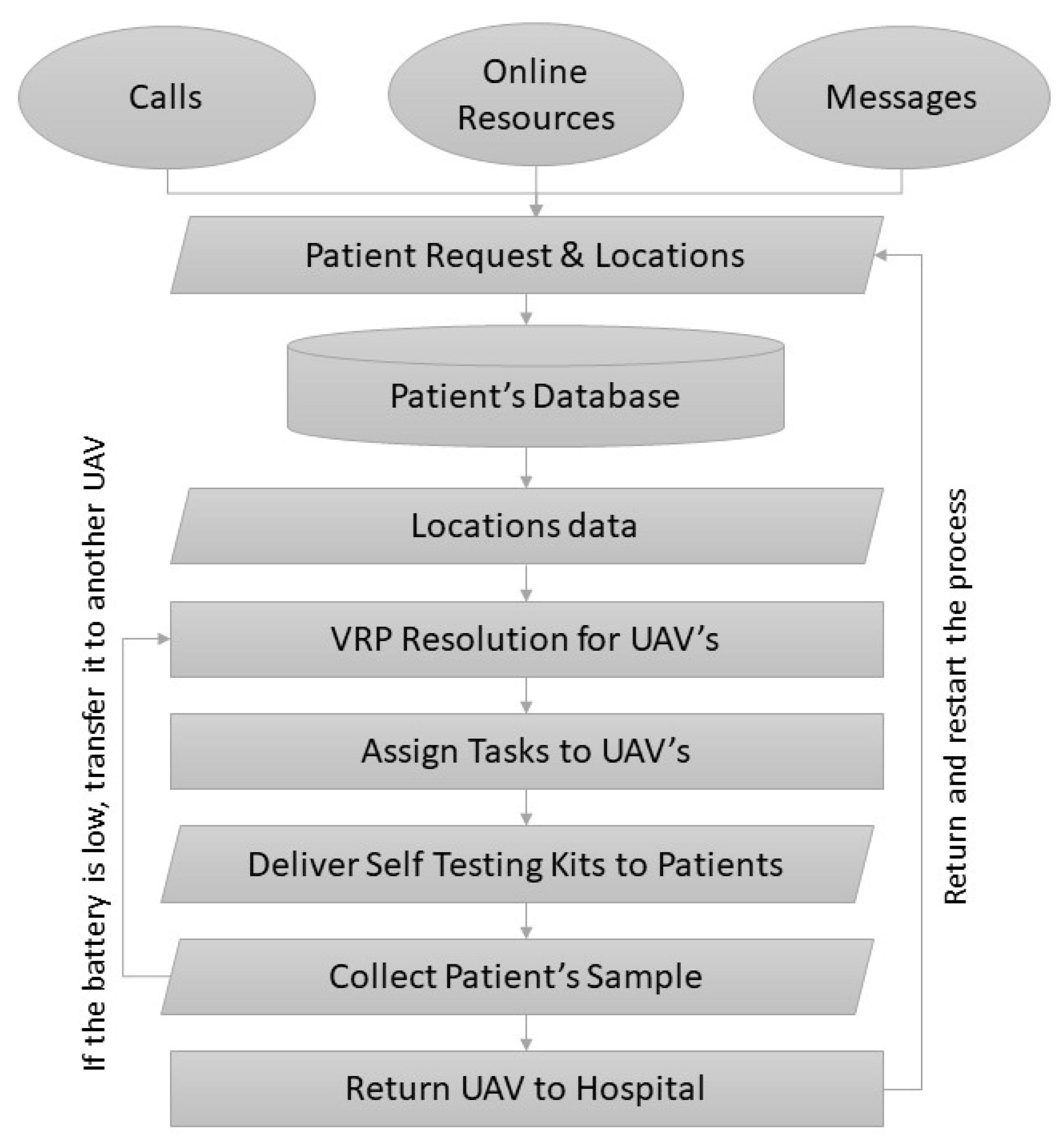
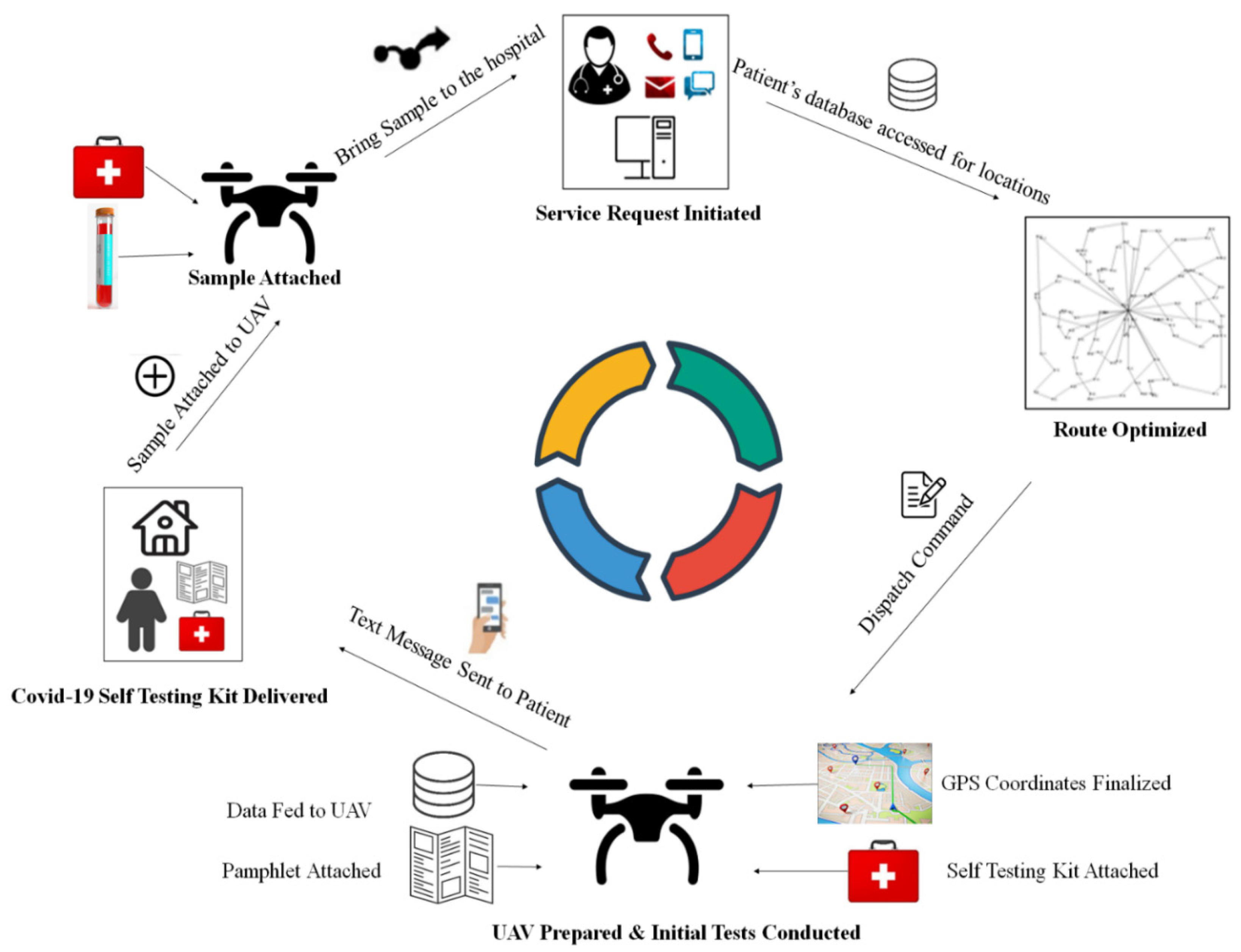
3.2. The Proposed UAV-Based COVID-19 Kit Dispatch and Collection System
3.2.1. Step 1
3.2.2. Step 2
3.2.3. Step 3
3.2.4. Step 4
3.2.5. Step 5
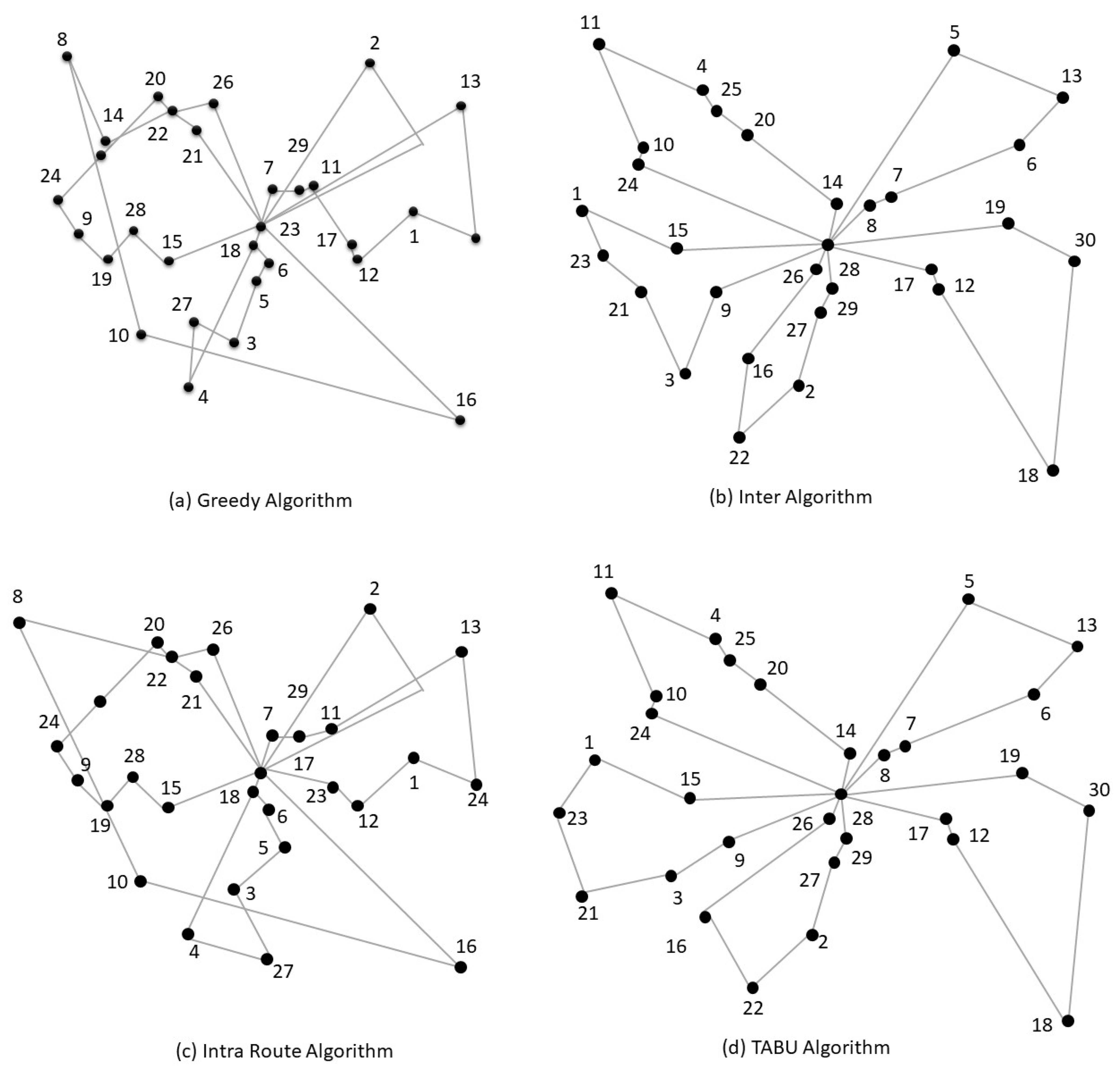
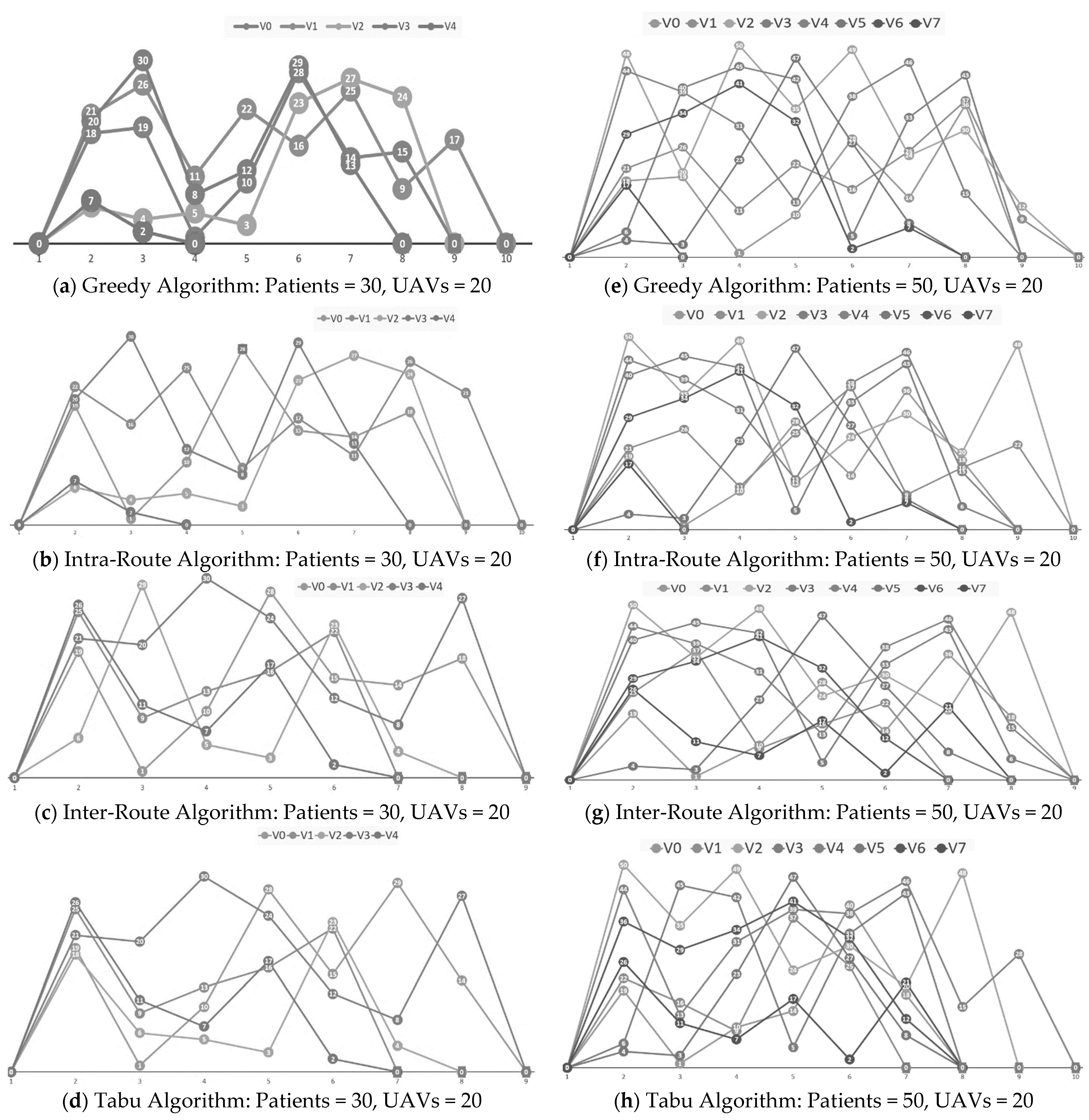
3.3. The Algorithms and Their Pseudocodes
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometers. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/?utm_campaign=homeAdvegas1?#countries (accessed on 24 October 2020).
- Hasell, J.E.; Mathieu, D.; Beltekian, B.; Macdonald, C.; Giattino, E.; Roser, O.-O.M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 1–7. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [Green Version]
- Homolak, J.; Kodvanj, I.; Virag, D. Preliminary analysis of COVID-19 academic information patterns: A call for open science in the times of closed borders. Scientometrics 2020, 124, 2687–2701. [Google Scholar] [CrossRef] [PubMed]
- Smith, P. Covid-19 in Australia: Most infected health workers in Victoria’s second wave acquired virus at work. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Zhu, S.; Wu, Y.; Zhu, C.-Y.; Hong, W.-C.; Yu, Z.-X.; Chen, Z.-K.; Chen, Z.-l.; Jiang, D.-G.; Wang, Y.-G. The im-mediate mental health impacts of the COVID-19 pandemic among people with or without quarantine managements. Brain Behav. Immun. 2020, 87, 56. [Google Scholar] [CrossRef]
- Government of Pakistan. Pakistan Cases Details. Available online: http://covid.gov.pk/stats/pakistan?locale=en (accessed on 24 October 2020).
- Farooq, F.; Khan, J.; Khan, M.U.G. Effect of Lockdown on the spread of COVID-19 in Pakistan. arXiv 2020, arXiv:2005.09422. [Google Scholar]
- Javaid, M.; Haleem, A.; Vaishya, R.; Bahl, S.; Suman, R.; Vaish, A. Industry 4.0 technologies and their applications in fighting COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Esmaeili, S.; Tabbakh, S.R.K.; Shakeri, H. A priority-aware lightweight secure sensing model for body area networks with clinical healthcare applications in Internet of Things. Pervasive Mob. Comput. 2020, 69, 101265. [Google Scholar] [CrossRef] [PubMed]
- Ke, Y.-Y.; Peng, T.-T.; Yeh, T.-K.; Huang, W.-Z.; Chang, S.-E.; Wu, S.-H.; Hung, H.-C.; Hsu, T.-A.; Lee, S.-J.; Song, J.-S. Artificial intelligence approach fighting COVID-19 with repurposing drugs. Biomed. J. 2020, 43, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Alimadadi, A.; Aryal, S.; Manandhar, I.; Munroe, P.B.; Joe, B.; Cheng, X. Artificial intelligence and machine learning to fight COVID-19. Physiol. Genom. 2020, 52, 200–202. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Carin, L.; Dzau, V.; Wong, T.Y. Digital technology and COVID-19. Nat. Med. 2020, 26, 459–461. [Google Scholar] [CrossRef] [Green Version]
- Ullah, F.; Sepasgozar, S.M.; Wang, C. A systematic review of smart real estate technology: Drivers of, and barriers to, the use of digital disruptive technologies and online platforms. Sustainability 2018, 10, 3142. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Gupta, P.K.; Srivastava, A. A review of modern technologies for tackling COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Ullah, F.; Sepasgozar, S.M.; Shirowzhan, S.; Davis, S. Modelling users’ perception of the online real estate platforms in a digitally disruptive environment: An integrated KANO-SISQual approach. Telemat. Inform. 2021, 63, 101660. [Google Scholar] [CrossRef]
- Ullah, F.; Sepasgozar, S.M.; Thaheem, M.J.; Al-Turjman, F. Barriers to the digitalisation and innovation of Australian Smart Real Estate: A managerial perspective on the technology non-adoption. Environ. Technol. Innov. 2021, 22, 101527. [Google Scholar] [CrossRef]
- Ullah, F.; Sepasgozar, S.M.; Thaheem, M.J.; Wang, C.C.; Imran, M. It’s all about perceptions: A DEMATEL approach to exploring user perceptions of real estate online platforms. Ain Shams Eng. J. 2021, in press. [Google Scholar] [CrossRef]
- Hildmann, H.; Kovacs, E. Using Unmanned Aerial Vehicles (UAVs) as Mobile Sensing Platforms (MSPs) for Disaster Response, Civil Security and Public Safety. Drones 2019, 3, 59. [Google Scholar] [CrossRef] [Green Version]
- Qadir, Z.; Ullah, F.; Munawar, H.S.; Al-Turjman, F. Addressing disasters in smart cities through UAVs path planning and 5G communications: A systematic review. Comput. Commun. 2021, 168, 114–135. [Google Scholar] [CrossRef]
- Munawar, H.S.; Ullah, F.; Qayyum, S.; Khan, S.I.; Mojtahedi, M. UAVs in Disaster Management: Application of Integrated Aerial Imagery and Convolutional Neural Network for Flood Detection. Sustainability 2021, 13, 7547. [Google Scholar] [CrossRef]
- Ullah, F.; Samad Sepasgozar, P.; Ali, T.H. Real estate stakeholders technology acceptance model (RESTAM): User-focused big9 disruptive technologies for smart real estate management. In Proceedings of the 2nd International Conference on Sustainable Development in Civil Engineering (ICSDC 2019), Jamshoro, Pakistan, 5–7 December 2019. [Google Scholar]
- Qayyum, S.; Ullah, F.; Al-Turjman, F.; Mojtahedi, M. Managing smart cities through six sigma DMADICV method: A review-based conceptual framework. Sustain. Cities Soc. 2021, 72, 103022. [Google Scholar] [CrossRef]
- Ullah, F.; Al-Turjman, F. A conceptual framework for blockchain smart contract adoption to manage real estate deals in smart cities. Neural Comput. Appl. 2021, 1–22. Available online: https://link.springer.com/article/10.1007%2Fs00521-021-05800-6#citeas (accessed on 30 July 2021).
- Ullah, F.; Qayyum, S.; Thaheem, M.J.; Al-Turjman, F.; Sepasgozar, S.M. Risk management in sustainable smart cities governance: A TOE framework. Technol. Forecast. Soc. Chang. 2021, 167, 120743. [Google Scholar] [CrossRef]
- Tsouros, D.C.; Bibi, S.; Sarigiannidis, P.G. A review on UAV-based applications for precision agriculture. Information 2019, 10, 349. [Google Scholar] [CrossRef] [Green Version]
- Nikitas, A.; Michalakopoulou, K.; Njoya, E.T.; Karampatzakis, D. Artificial intelligence, transport and the smart city: Definitions and dimensions of a new mobility era. Sustainability 2020, 12, 2789. [Google Scholar] [CrossRef] [Green Version]
- Sethuraman, S.C.; Vijayakumar, V.; Walczak, S. Cyberattacks on healthcare devices using unmanned aerial vehicles. J. Med. Syst. 2020, 44, 9. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Ganguly, D. FANET based Emergency Healthcare Data Dissemination. In Proceedings of the 2020 Second International Conference on Inventive Research in Computing Applications (ICIRCA), Coimbatore, India, 15–17 July 2020. [Google Scholar]
- Euchi, J. Do drones have a realistic place in a pandemic fight for delivering medical supplies in healthcare systems problems. Chin. J. Aeronaut 2020, 34, 182–190. [Google Scholar] [CrossRef]
- Hossain, M.S.; Muhammad, G.; Guizani, N. Explainable AI and mass surveillance system-based healthcare framework to combat COVID-I9 like pandemics. IEEE Netw. 2020, 34, 126–132. [Google Scholar] [CrossRef]
- Wazid, M.; Bera, B.; Mitra, A.; Das, A.K.; Ali, R. Private blockchain-envisioned security framework for AI-enabled IoT-based drone-aided healthcare services. In Proceedings of the 2nd ACM MobiCom Workshop on Drone Assisted Wireless Communications for 5G and Beyond, London, UK, 25 September 2020. [Google Scholar]
- Siriwardhana, Y.; Gür, G.; Ylianttila, M.; Liyanage, M. The role of 5G for digital healthcare against COVID-19 pandemic: Opportunities and challenges. ICT Express 2020, 7, 244–252. [Google Scholar] [CrossRef]
- Ullah, H.; Nair, N.G.; Moore, A.; Nugent, C.; Muschamp, P.; Cuevas, M. 5G communication: An overview of vehicle-to-everything, drones, and healthcare use-cases. IEEE Access 2019, 7, 37251–37268. [Google Scholar] [CrossRef]
- Ullah, F.; Al-Turjman, F.; Qayyum, S.; Inam, H.; Imran, M. Advertising through UAVs: Optimized path system for delivering smart real-estate advertisement materials. Int. J. Intell. Syst. 2021, 36, 3429–3463. [Google Scholar] [CrossRef]
- IQAir. Air Quality and Pollution City Ranking. Available online: https://www.iqair.com/world-air-quality-ranking (accessed on 15 February 2021).
- Lee, I.; Wang, C.-C.; Lin, M.-C.; Kung, C.-T.; Lan, K.-C.; Lee, C.-T. Effective strategies to prevent coronavirus disease-2019 (COVID-19) outbreak in hospital. J. Hosp. Infect. 2020, 105, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buja, A.; Paganini, M.; Cocchio, S.; Scioni, M.; Rebba, V.; Baldo, V. Demographic and socio-economic factors, and healthcare resource indicators associated with the rapid spread of COVID-19 in Northern Italy: An ecological study. PLoS ONE 2020, 15, e0244535. [Google Scholar] [CrossRef] [PubMed]
- Hussain, R.; Dawoud, D.M. Drive-thru pharmacy services: A way forward to combat COVID-19 pandemic. Res. Soc. Adm. Pharm. 2020, 17, 1920–1924. [Google Scholar] [CrossRef]
- Nagura-Ikeda, M.; Imai, K.; Tabata, S.; Miyoshi, K.; Murahara, N.; Mizuno, T.; Horiuchi, M.; Kato, K.; Imoto, Y.; Iwata, M. Clinical evaluation of self-collected saliva by RT-qPCR, direct RT-qPCR, RT-LAMP, and a rapid antigen test to diagnose COVID-19. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef]
- Nomad. Coronavirus-Antibody-Self-Test-Kits. Available online: https://www.nomadtravel.co.uk/travel-store/coronavirus/coronavirus-antibody-self-test-kits (accessed on 24 October 2020).
- Johns Hopkins Medicine. Self-Test for COVID-19: Instructions and FAQs. Available online: https://www.hopkinsmedicine.org/coronavirus/self-test.html (accessed on 24 October 2020).
- Kroger Health. COVID-19 Test Home Collection Kit. Available online: https://www.fda.gov/media/139682/download (accessed on 24 October 2020).
- Administration, T.G. Legal Supply of COVID-19 Test Kits. Available online: https://www.tga.gov.au/legal-supply-covid-19-test-kits (accessed on 23 October 2020).
- Çodur, M.K.; Yılmaz, M. A time-dependent hierarchical Chinese postman problem. Cent. Eur. J. Oper. Res. 2020, 28, 337–366. [Google Scholar] [CrossRef]
- Deng, W.; Xu, J.; Zhao, H. An improved ant colony optimization algorithm based on hybrid strategies for scheduling problem. IEEE Access 2019, 7, 20281–20292. [Google Scholar] [CrossRef]
- Gutierrez, A.; Dieulle, L.; Labadie, N.; Velasco, N. A multi-population algorithm to solve the VRP with stochastic service and travel times. Comput. Ind. Eng. 2018, 125, 144–156. [Google Scholar] [CrossRef]
- Munawar, H.S. Flood Disaster Management: Risks, Technologies, and Future Directions. In Machine Vision Inspection Systems: Image Processing, Concepts, Methodologies and Applications; Wiley: Hoboken, NJ, USA, 2020; Volume 1, pp. 115–146. [Google Scholar]
- Gocken, T.; Yaktubay, M. Comparison of different clustering algorithms via genetic algorithm for VRPTW. Int. J. Simul. Model 2019, 4, 574–585. [Google Scholar] [CrossRef]
- Zhou, Z.; Ma, X.; Liang, Z.; Zhu, Z. Multi-objective multi-factorial memetic algorithm based on bone route and large neighborhood local search for VRPTW. In Proceedings of the 2020 IEEE Congress on Evolutionary Computation (CEC), Glasgow, UK, 19–24 July 2020. [Google Scholar]
- Shen, Y.; Liu, M.; Yang, J.; Shi, Y.; Middendorf, M. A hybrid swarm intelligence algorithm for vehicle routing problem with time windows. IEEE Access 2020, 8, 93882–93893. [Google Scholar] [CrossRef]
- Dong, W.; Zhou, K.; Zhang, G.; Chao, H.-C. Modified discrete glowworm swarm optimization algorithm based on time window division for multi-objective vrptw. J. Internet Technol. 2018, 19, 001–013. [Google Scholar]
- Mat, N.A.; Benjamin, A.M.; Abdul-Rahman, S.; Wibowo, A. Nearest greedy for solving the waste collection vehicle routing problem: A case study. In AIP Conference Proceedings; AIP Publishing LLC: Langkawi, Malaysia, 2017. [Google Scholar]
- Mourad, B.; Chacher, A.A.; Cyril, F.; Hayder Ibrahim, H. Ontology-Based Reasoning System for Logistics Applications Deployment. In Proceedings of the Smart Application and Data Analysis for Smart Cities (SADASC’18), Casablanca, Morocco, 27–28 February 2018. [Google Scholar]
- Montané, F.A.T.; Galvao, R.D. A tabu search algorithm for the vehicle routing problem with simultaneous pick-up and delivery service. Comput. Oper. Res. 2006, 33, 595–619. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No | Method | Advantages | Risks and Limitations |
|---|---|---|---|
| 1 | Special Hospitals or Pop-Up Clinics | Qualified staff collecting samples; Reliable results | Risk of spread to other patients and staff; Long wait and queues |
| 2 | Drive through Clinics | Qualified staff collecting samples. Lower risk of spread from other patients; Reliable results | Long wait and queues; Potential infection from the collection staff |
| 3 | Self-Collections | No risk of spread from other patients. Speedy collection | The process may be tough to understand; Lack of qualifications of patients; Improper handling of test kits may result in public health risks |
| Collection Method | Kit Manufacturers and Name | Collection Process and Results | Location | Price |
|---|---|---|---|---|
| Nasal Swab | Everlywell COVID-19 Test Home Collection Kit | Kits shipped to patients with instructions; Return instructions mentioned; Results available online within 72 h when the lab receives the sample. | USA | $109 |
| Pixel by LabCorp COVID-19 Test | Test mailed out after the survey; Collection instructions mailed; Samples must be shipped back that same day; Results available within 24–48 h of the lab’s receipt of the sample. | USA | $119 | |
| LetsGetChecked Coronavirus Test | Online assessment marks eligibility; The patient will collect the sample and send it back to the lab; Results available on online accounts in 24 to 72 h. | USA | $119 | |
| Picture’s COVID-19 test by Fulgent Genetics | Eligibility assessment determines kit dispatch; samples are sent in a pre-labeled box; A digital report will be available in an online portal in 1 to 2 days; Optional telehealth consultation to discuss the results. | USA | $119 | |
| Kruger Health COVID-19 Test Home Collection Kit | Telehealth visits to determine eligibility; Test kit shipped; Collection and return explained; In-person drop-off available; Results available within 72 h of the lab receiving the sample. | USA | - | |
| Saliva-Based | For Hims & Hers Saliva Test Kit | Initial questionnaire to determine eligibility; Test kit shipped overnight; Collection and return explained; Results available within 3 to 5 days of the lab receiving the sample. | USA | $150 |
| Phosphorus COVID-19 PCR Test | Order test and complete online medical screening; At-home sample collection kit shipped; Test results available within 72 h from the lab’s receipt of the sample. | USA | $140 | |
| Vault COVID-19 Test Kit | Risk factors and symptoms described online; A test kit sent to the patient; An online telehealth provider guides sample collection; Sample sent back via overnight shipping; Test results available 48 to 72 h after the sample arrives at the lab. | USA | $150 | |
| Vitagene COVID-19 Saliva Test Kit | After a questionnaire, a test kit is sent via express mail; Sample collected as per instructions; Sample returned via express mail; Results available within 72 h of the lab receiving the sample. | USA | $129 | |
| P23 Labs Unsupervised COVID-19 Test | Initial questionnaire to determine eligibility; Test shipped out; Patients should send back the sample within 24 h of collection; An email sent when test results are ready; An opportunity to talk to a physician about the result. | USA | $142 | |
| TMB Coronavirus Self-Test Kit | Receive an activation link for MyTMB; Visit the site and complete the request form; Sample collected as per instructions; Post your pre-addressed package in any post box; Patients contacted when results available. | Ireland | £160 | |
| Blood-Based | Nomad Coronavirus Antibody Home Test Kit | Kit ordered online; Video consultation with a physician to determine eligibility; Kit shipped; Sample collected through video assistance; The results are explained on a video call. | UK | £60 |
| HIVE Coronavirus COVID-19 Test-Home Self-Test Kit | Blood test kit ordered online; Test strips provide indications of COVID-19 biomarkers; Used for secondary diagnosis of COVID-19 | UK | £110 |
| S. No | Name | Characteristics | Link Official Website |
|---|---|---|---|
| 1 | Wing | It can deliver packages up to 3.3 pounds. Customers do not interact directly with the delivery drone. It hovers around 20 feet above the ground. It has conducted more than 100,000 flights across three continents | https://wing.com/ (accessed on 4 July 2021) |
| 2 | Amazon Prime Air | It can deliver packages up to 5 pounds in 30 min. In addition, customers can interact with it. | https://www.amazon.com/Amazon-Prime-Air/ (accessed on 4 July 2021) |
| 3 | UPS Flight Forward | It can deliver packages weighing more than 55 pounds. Suitable for delivering medical kits. UPS Flight Forward has teamed with Matternet, an autonomous drone logistics platform, to deliver medical supplies to WakeMed hospital in Raleigh, North Carolina. It can operate at night. | https://www.ups.com/us/en/services/shipping-services/flight-forward-drones.page (accessed on 4 July 2021) |
| 4 | Wingcopter | It provides services for commercial and humanitarian applications, including medical air services, logistics, and others. It can carry weights up to 6 kg. Its flight range is up to 110–120 km, the wind resistance is 15 m/s on average with 20 m/s gusts, and the cruise speed is between 100–240 km/h. | https://wingcopter.com/ (accessed on 4 July 2021) |
| 5 | Zipline | It has been used in global healthcare, retail and e-commerce, and defense and disaster responses. It can fly at any time of the day or night. Its cruise speed is 101 km/h and can carry up to 1.75 kg (3.9 lb) of cargo. The flight time is 45 min, and an altitude of 80–120 m can be attained above ground level. | https://flyzipline.com/ (accessed on 4 July 2021) |
| 6 | DHL Parcelcopter | It can carry a payload of up to 4.4 pounds and travel at speeds of around 43 miles per hour. | https://www.dhl.com/discover/business/business-ethics/parcelcopter-drone-technology (accessed on 4 July 2021) |
| Algorithm | Pseudocode |
|---|---|
| (a) Greedy Algorithm | Start
|
| (b) Tabu Algorithm | Start
|
| (c) Intra-Route Algorithm | Start
|
| (d) Inter-Route Algorithm | Start
|
| No. of Patients | Total UAVs | UAVs Utilized | Greedy Search | Tabu Search | Inter-Route | Intra-Route | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Runtime (ms) | Distance | Runtime (ms) | Distance | Runtime (ms) | Distance | Runtime (ms) | Distance | |||
| 30 | 10 | 5 | 343 | 39.65 | 100 | 31.85 | 114 | 32.2 | 117 | 38.05 |
| 20 | 5 | 355 | 39.65 | 53 | 31.85 | 35 | 32.2 | 48 | 38.05 | |
| 30 | 5 | 352 | 39.65 | 55 | 31.85 | 35 | 32.2 | 52 | 38.05 | |
| 50 | 5 | 412 | 39.65 | 39 | 31.85 | 42 | 32.2 | 59 | 38.05 | |
| 100 | 5 | 353 | 39.65 | 49 | 31.85 | 29 | 32.2 | 85 | 38.05 | |
| 50 | 10 | 8 | 525 | 58.95 | 204 | 51.1 | 111 | 51.8 | 110 | 56.8 |
| 20 | 8 | 383 | 58.95 | 161 | 51.4 | 61 | 51.8 | 66 | 56.8 | |
| 30 | 8 | 359 | 58.95 | 156 | 51.15 | 63 | 51.8 | 62 | 56.8 | |
| 50 | 8 | 406 | 58.95 | 188 | 51.2 | 78 | 51.8 | 78 | 56.8 | |
| 100 | 8 | 402 | 58.95 | 169 | 51.35 | 94 | 51.8 | 109 | 56.8 | |
| 100 | 10 | N/A | ||||||||
| 20 | 14 | 355 | 102.45 | 266 | 83.75 | 109 | 89.8 | 94 | 99.55 | |
| 30 | 14 | 360 | 102.45 | 274 | 85.05 | 79 | 89.8 | 78 | 99.55 | |
| 50 | 14 | 421 | 102.45 | 240 | 88.2 | 89 | 89.8 | 108 | 99.55 | |
| 100 | 14 | 391 | 102.45 | 249 | 85 | 110 | 89.8 | 94 | 99.55 | |
| 500 | 10 | N/A | ||||||||
| 20 | N/A | |||||||||
| 30 | N/A | |||||||||
| 50 | N/A | |||||||||
| 100 | 71 | 458 | 369.1 | 1148 | 349.15 | 366 | 349.4 | 203 | 361 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munawar, H.S.; Inam, H.; Ullah, F.; Qayyum, S.; Kouzani, A.Z.; Mahmud, M.A.P. Towards Smart Healthcare: UAV-Based Optimized Path Planning for Delivering COVID-19 Self-Testing Kits Using Cutting Edge Technologies. Sustainability 2021, 13, 10426. https://doi.org/10.3390/su131810426
Munawar HS, Inam H, Ullah F, Qayyum S, Kouzani AZ, Mahmud MAP. Towards Smart Healthcare: UAV-Based Optimized Path Planning for Delivering COVID-19 Self-Testing Kits Using Cutting Edge Technologies. Sustainability. 2021; 13(18):10426. https://doi.org/10.3390/su131810426
Chicago/Turabian StyleMunawar, Hafiz Suliman, Hina Inam, Fahim Ullah, Siddra Qayyum, Abbas Z. Kouzani, and M. A. Parvez Mahmud. 2021. "Towards Smart Healthcare: UAV-Based Optimized Path Planning for Delivering COVID-19 Self-Testing Kits Using Cutting Edge Technologies" Sustainability 13, no. 18: 10426. https://doi.org/10.3390/su131810426