 Ales Janda1
Ales Janda1 Corinna Engel2Jonathan Remppis3Sigrid Enkel4
Corinna Engel2Jonathan Remppis3Sigrid Enkel4 Andreas Peter5
Andreas Peter5 Sebastian Hörber5
Sebastian Hörber5 Tina Ganzenmueller6Sarah Schober3Christof Weinstock7,8,9
Tina Ganzenmueller6Sarah Schober3Christof Weinstock7,8,9 Eva-Maria Jacobsen1Dorit Fabricius1Maria Zernickel1
Eva-Maria Jacobsen1Dorit Fabricius1Maria Zernickel1 Thomas Stamminger10Andrea Dietz10Hans-Jürgen Groß11
Thomas Stamminger10Andrea Dietz10Hans-Jürgen Groß11 Sebastian F. N. Bode1
Sebastian F. N. Bode1 Anneke D. M. Haddad12
Anneke D. M. Haddad12 Roland Elling12,13Maximilian Stich14
Roland Elling12,13Maximilian Stich14 Burkhard Tönshoff14
Burkhard Tönshoff14 Philipp Henneke12,13
Philipp Henneke12,13 Klaus-Michael Debatin1Axel R. Franz2,3
Klaus-Michael Debatin1Axel R. Franz2,3 Hanna Renk3*
Hanna Renk3*
- 1Department of Pediatrics and Adolescent Medicine, Ulm University Medical Center, Ulm University, Ulm, Germany
- 2Center for Pediatric Clinical Studies, University Children’s Hospital Tübingen, Tübingen, Germany
- 3University Children’s Hospital Tübingen, Tübingen, Germany
- 4Center for Clinical Transfusion Medicine Tübingen, Tübingen, Germany
- 5Institute for Clinical Chemistry and Pathobiochemistry, University Hospital Tübingen, Tübingen, Germany
- 6Institute for Medical Virology and Epidemiology of Viral Diseases, University Hospital Tübingen, Tübingen, Germany
- 7Department of Transfusion Medicine, Ulm University, Ulm, Germany
- 8Institute for Clinical Transfusion Medicine and Immunogenetics, Ulm, Germany
- 9Red Cross Blood Service Baden-Württemberg-Hessen, Ulm, Germany
- 10Institute of Virology, Ulm University Medical Center, Ulm, Germany
- 11Institute of Clinical Chemistry, Ulm University Medical Center, Ulm, Germany
- 12Center for Pediatrics and Adolescent Medicine, Medical Center Freiburg, Germany and Faculty of Medicine, University of Freiburg, Freiburg, Germany
- 13Institute for Immunodeficiency, Medical Center Freiburg, Germany and Faculty of Medicine, University of Freiburg, Freiburg, Germany
- 14Department of Pediatrics I, University Children’s Hospital Heidelberg, Heidelberg, Germany
An association between certain ABO/Rh blood groups and susceptibility to SARS-CoV-2 infection has been proposed for adults, although this remains controversial. In children and adolescents, the relationship is unclear due to a lack of robust data. Here, we investigated the association of ABO/Rh blood groups and SARS-CoV-2 in a multi-center study comprising 163 households with 281 children and 355 adults and at least one SARS-CoV-2 seropositive individual as determined by three independent assays as a proxy for previous infection. In line with previous findings, we found a higher frequency of blood group A (+ 6%) and a lower frequency of blood group O (−6%) among the SARS-CoV-2 seropositive adults compared to the seronegative ones. This trend was not seen in children. In contrast, SARS-CoV-2 seropositive children had a significantly lower frequency of Rh-positive blood groups. ABO compatibility did not seem to play a role in SARS-CoV-2 transmission within the families. A correction for family clusters was performed and estimated fixed effects of the blood group on the risk of SARS-CoV-2 seropositivity and symptomatic infection were determined. Although we found a different distribution of blood groups in seropositive individuals compared to the reference population, the risk of SARS-CoV-2 seropositivity or symptomatic infection was not increased in children or in adults with blood group A or AB versus O or B. Increasing age was the only parameter positively correlating with the risk of SARS-CoV-2 infection. In conclusion, specific ABO/Rh blood groups and ABO compatibility appear not to predispose for SARS-CoV-2 susceptibility in children.
Introduction
Susceptibility to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and severity of coronavirus disease 2019 (COVID-19) are heterogeneous across different populations. This heterogeneity has been attributed to various individual risk factors (Williamson et al., 2020; Goel et al., 2021; Ng et al., 2021). The ABO blood group is a suspected candidate because of its known role in other infectious diseases (Cooling, 2015). Early in the pandemic, a report from China showed an association of blood group A with increased risk of SARS-CoV-2 infection and lower risk for individuals with group O (Li et al., 2020). A first large-scale genome-wide study reported similar results with respect to COVID-19 severity (Ellinghaus et al., 2020). Others demonstrated a protective role of blood group O compared to A regarding disease susceptibility or severity (Golinelli et al., 2020; Wu et al., 2020). However, current results are conflicting and several high-quality studies did not support ABO-dependent intrinsic susceptibility to SARS-CoV-2 infection or COVID-19 severity (Boudin and Dutasta, 2020; Zhang et al., 2020; Zietz et al., 2020; Anderson et al., 2021). One of the possible explanations could be an over-recruitment of individuals with blood group O in blood banks due to their universal donor status. Thus, studies using blood donors as a reference group would find that the frequency of blood group O is lower among their COVID-19 cases than in the blood bank reference population (Dzik et al., 2020; Pendu et al., 2021).
Several underlying mechanisms have been proposed to explain the association between ABO blood group and SARS-CoV-2 infection: First, genetic histo-blood group polymorphisms can lead to variable viral attachment. Second, it has been hypothesized that the SARS-CoV-2 receptor-binding domain (RBD) may act as a lectin and preferentially bind to blood group A glycoprotein expressed on respiratory epithelial cells of blood group A individuals, favoring SARS-CoV-2 infection, though this has been recently contradicted in vitro (Wu et al., 2021; Boukhari et al., 2022). Third, the interaction of the SARS-CoV-1 and -2 spike protein with the cellular angiotensin-converting enzyme 2 (ACE2) receptor is inhibited by anti-A natural antibodies (Guillon et al., 2008; Le Pendu and Ruvoën-Clouet, 2020).
Last, it has been suggested that natural anti-A and anti-B could neutralize the virus when transmission occurs in an ABO-incompatible manner and this may reduce virus transmissibility by at least 60% (Ellis, 2021). Natural anti-A and anti-B antibodies present in ABO-incompatible virus recipients could recognize and bind to A and/or B epitopes expressed on the viral envelope glycoproteins, prevent the interaction of the virus and ACE2 receptor, and consequently prevent entry into lung epithelial cells (Goel et al., 2021). This mechanism is supported by the finding that COVID-19 patients had significantly lower anti-A and anti-B antibody levels compared to controls (Deleers et al., 2021). Additionally, Boukhari et al. (2022) demonstrated only recently that ABO incompatibility between spouses strongly decreased the risk of SARS-CoV-2 transmission.
Although we and others have demonstrated lower SARS-CoV-2 susceptibility in children and adolescents compared to adults (Spielberger et al., 2021; Stich et al., 2021; Tönshoff et al., 2021), pediatric data on the impact of ABO blood group on SARS-CoV-2 infection susceptibility or COVID-19 severity are scarce (Bari et al., 2021). Moreover, the association between ABO/Rh blood group and SARS-CoV-2 infection within households has not been evaluated so far.
In this large multi-center family cohort study, we examined the prevalence of ABO/Rh blood groups in SARS-CoV-2 seropositive and seronegative children and adults. We evaluated the contribution of ABO/Rh blood group to SARS-CoV-2 susceptibility and symptomatic infection. Additionally, we investigated a role of ABO compatibility between infected and exposed individuals on the SARS-CoV-2 transmissibility.
Materials and Methods
Study Design and Cohort
This cohort study on ABO blood group forms part of a non-interventional, national multi-center SARS-CoV-2 seroprevalence study and includes 668 adults and children living in 164 households with at least one confirmed SARS-CoV-2 index case (Supplementary Methods). It was initiated by the University Children’s Hospitals in Freiburg, Heidelberg, Tübingen, and Ulm and approved by the independent ethics committee of each center. Blood samples and data for this sub-study were collected at the study sites in Tübingen and Ulm in July and August 2020 and at a second visit in February and March 2021. Informed written consent was obtained from all participants or their legal guardians prior to enrollment. All authors had access to primary clinical trial data. The study is registered at the German Clinical Trials Register (DRKS), study ID 00021521 (German Clinical Trials Register, 2020), and was conducted according to the Declaration of Helsinki and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Data and Sample Collection
Participants completed a questionnaire documenting number of household members, age, gender, date of infection, and COVID-19-related symptoms. Distribution of blood groups was compared to the reference population (Wagner et al., 1995).
Blood samples were drawn during study visits. SARS-CoV-2 serology was performed using two assays directed against the viral spike protein and one directed against the nucleocapsid protein. In general, results were interpreted as positive if at least the Euroimmun IgG and the Roche Elecsys pan Ig assay were positive. In samples with discordant results or equivocal results in the Euroimmun IgG, decision about seropositivity or seronegativity were made by considering the result of the ADVIA Centaur XPT SARS-CoV-2 IgG assay (Supplementary Methods). For blood group typing ABO (forward and reverse) and Rhesus D, blood groups were typed using the ERYTRA Automated System blood group analyzer (Grifols S.A., Barcelona, Spain). Column agglutination cards [DG Gel AB0/Rh (CR)] and reagent cells (Reverse-Cyte 0.8%) from Grifols were used.
Statistical Analysis
Chi-square tests were applied to test for difference in frequencies, and a generalized mixed model accounting for clustered data (cluster = family) was used to estimate fixed effects of the factors under consideration [blood group of index case (anti-A/no anti-A), symptomatic index case, yes/no, rhesus factor (positive/negative), age group of index (child/adult), age group of exposed family member (child/adult), blood group of exposed family member (anti-A/no anti-A), and rhesus factor of exposed family member (positive/negative)] on the risk of SARS-CoV-2 seropositivity and of age group, blood group, and rhesus factor on the occurrence of symptoms.
Results
General Characteristics of the Cohort
Blood group and SARS-CoV-2 antibodies were determined in 281 children and 355 adults. Mean age of children was 9 years (IQR 5;13), and that of adults was 43 years (IQR 38;50). Ten children and 98 adults were index cases. All other individuals were both exposed and infected (n = 244) or exposed and non-infected (n = 314). Eighty of 98 adult and 6 of 10 pediatric index cases showed symptoms including fever, cough, dysgeusia, and diarrhea (Table 1).
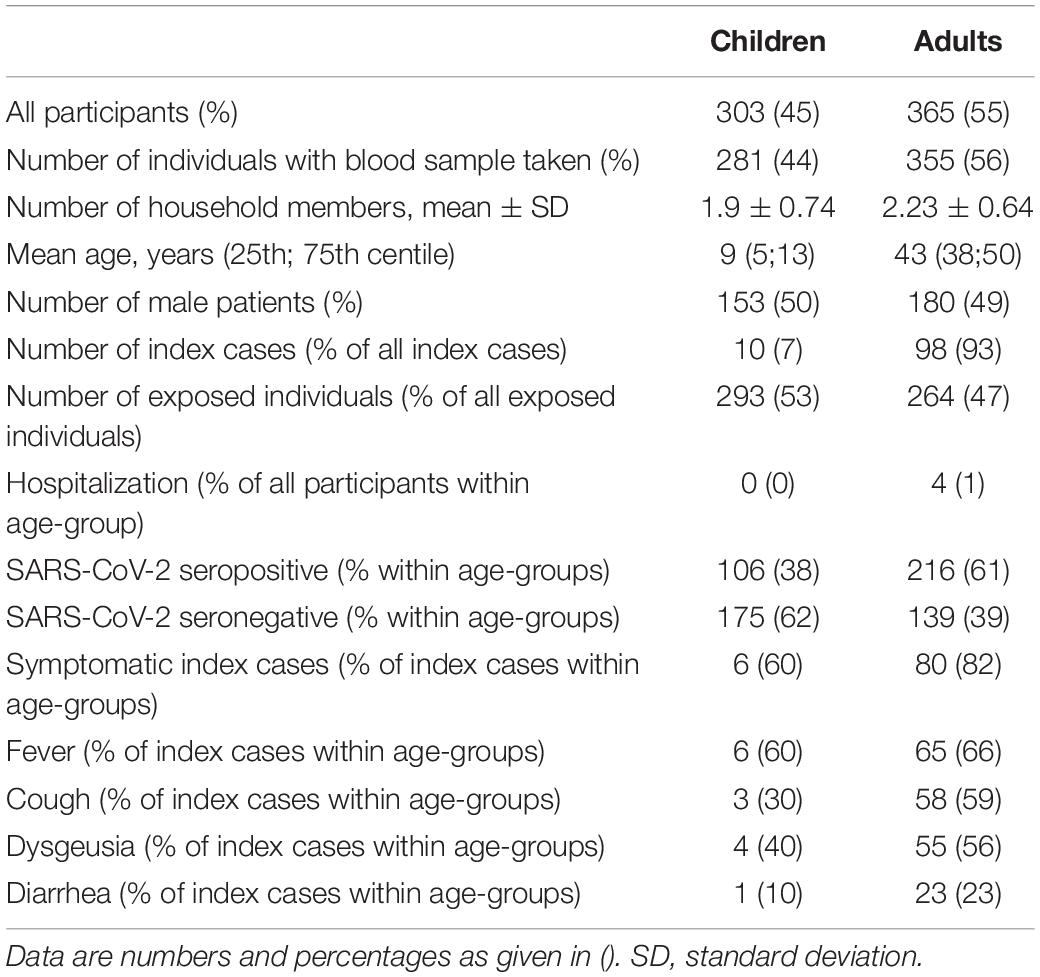
Table 1. Study cohort and patient characteristics.
Frequency of ABO/Rh Blood Group in SARS-CoV-2 Seropositive and Seronegative Individuals
In our cohort, 38% of children and 61% of adults were SARS-CoV-2 seropositive. The overall distribution of blood group frequency did not differ by serostatus. Frequency of blood group A was 45% among SARS-CoV-2 seronegative and 49% among SARS-CoV-2 seropositive individuals, whereas frequency of blood group O was 39 and 43%, respectively (Figure 1 and Table 2A). As shown in Table 2A the overrepresentation of blood group A along with an underrepresentation of blood group O was only seen in adults, not in children. In contrast, Rh-positive blood groups were present more frequently among seronegative individuals (p = 0.02), and the effect can be mainly attributed to the difference found in children (77% seropositive versus 88% seronegative; p = 0.01) (Table 2A).
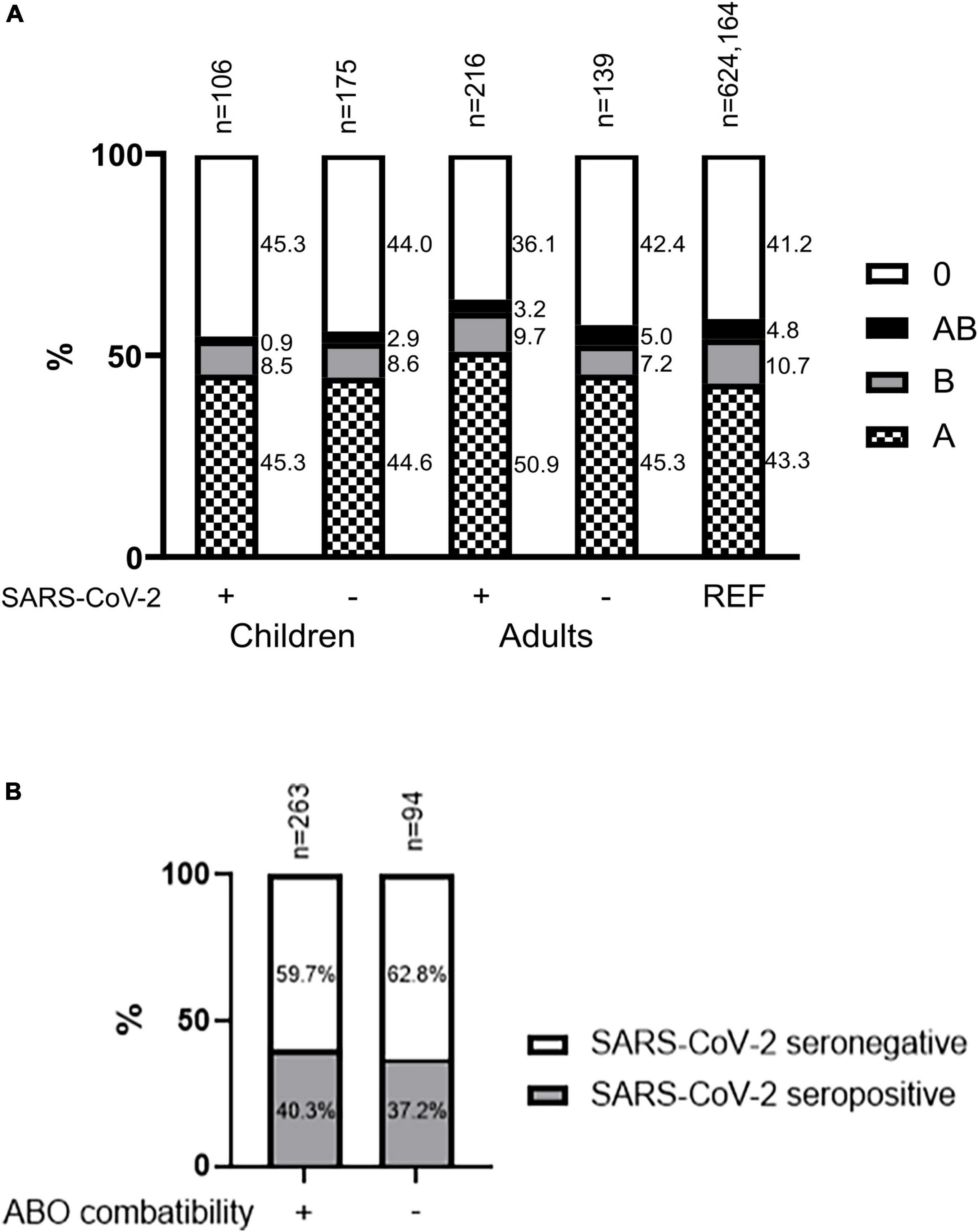
Figure 1. Overall observed blood group type distribution in children and adults (A) and frequency of SARS-CoV-2 transmission from index case to exposed individuals (n = 357) within the household cohort according to ABO blood group compatibility (B). (A) Blood group prevalence in child and adult household members and in a German reference population (20). Numbers next to the columns represent the proportion of the particular blood group within the subject group (in percent). Rh, rhesus factor. (B) The black bar indicates the proportion of SARS-CoV-2 seropositive individuals, and the white bar indicates the proportion of SARS-CoV-2 seronegative individuals.
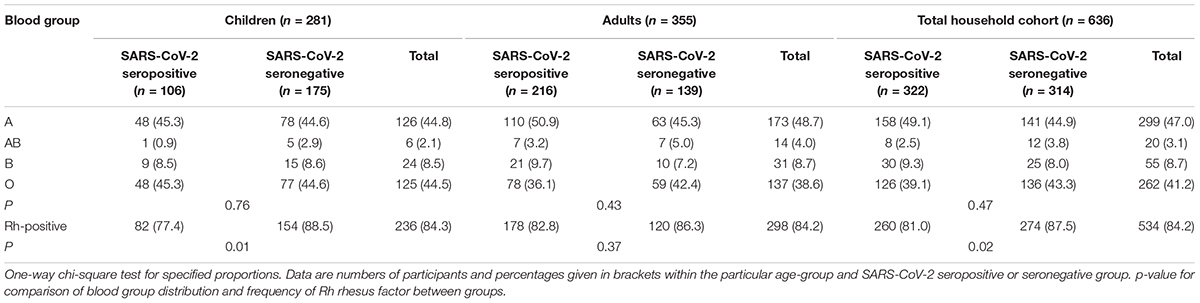
Table 2A. Blood type distribution within the cohort among SARS-CoV-2 seropositive and seronegative children and adults.
In comparison to the reference population, the distribution of blood groups among all SARS-CoV-2 seropositive individuals was different (marginally significant; p = 0.05) (Table 2B). The frequency of blood group A was 6.1% higher and the frequency of blood group O was 1.9% lower compared to the reference population. This effect was not seen when comparing the SARS-CoV-2 seronegative individuals to the reference population (p = 0.24). In comparison to the reference population, Rh-positive blood groups were present more frequently in seronegative individuals (+ 4.5%; p = 0.03). Although as well present in adults (+ 3.3; p = 0.3), this effect can also be mainly attributed to the difference found in children (+ 5.5%; p = 0.05) (Table 2B).
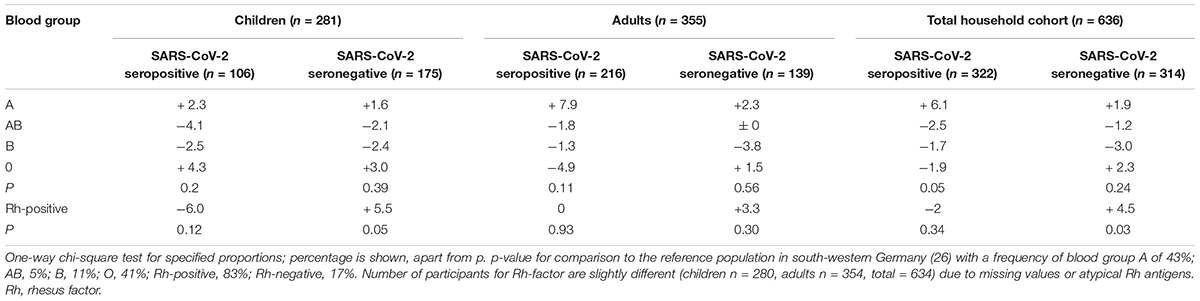
Table 2B. Differences in the frequency of each blood group among SARS-CoV-2 seropositive and seronegative individuals compared to the reference population.
SARS-CoV-2 Seropositivity of Exposed Individuals According to ABO Compatibility
In total, 263 exposed individuals had an ABO-compatible blood group compared to the index case and 94 had an incompatible blood group. A total of 106 ABO-compatible and 35 ABO-incompatible transmissions occurred and the frequency of transmission was similar in both groups (40.3 and 37.2%; Figure 1B).
Analysis of Risk Factors for SARS-CoV-2 Seropositivity and Symptomatic Disease
The cluster analysis did not reveal an increased odds ratio (OR) for SARS-CoV-2 seropositivity in individuals with blood group A or AB versus O or B, neither in children nor in adults. However, children with Rh-positive blood groups were twice as vulnerable to SARS-CoV-2 infection compared to those with Rh-negative blood groups [cluster-adjusted OR of 2.1 (95% CI 1.0–4.6)]. In the total cohort, compatibility of ABO blood group did not influence the risk for SARS-CoV-2 infection [cluster-adjusted OR of 1.2 (95% CI 0.6–2.3), Table 3].
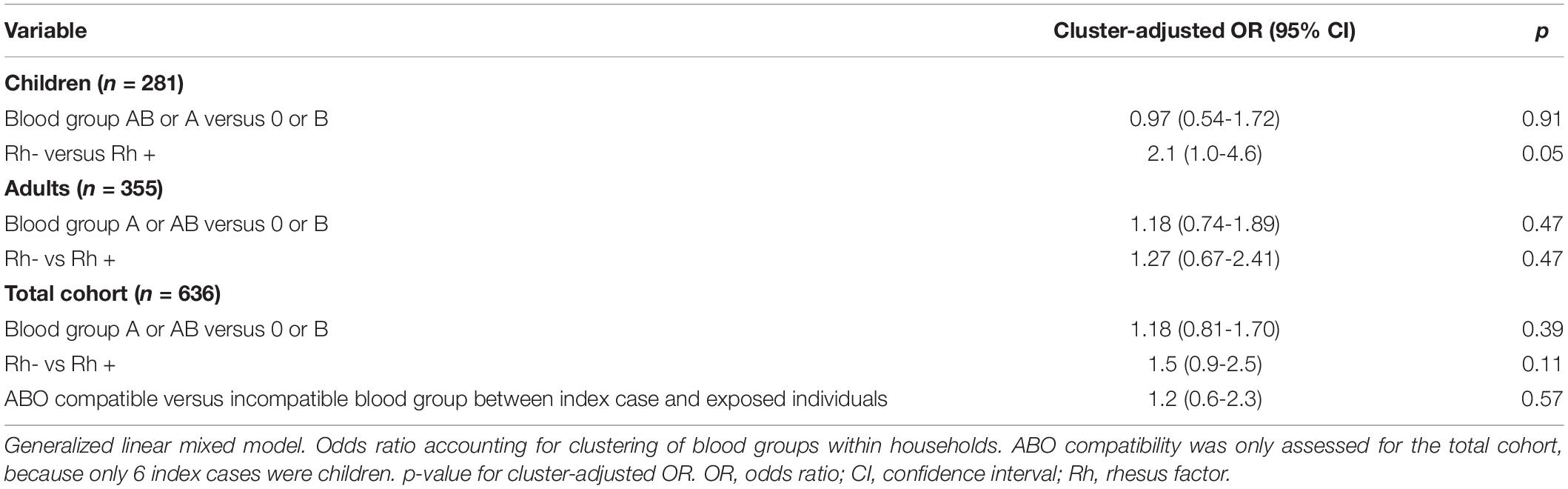
Table 3. Risk of household members having blood group AB or A versus 0 or B or being Rh-negative versus Rh-positive for SARS-CoV-2 seropositivity.
Although the risk for SARS-CoV-2 infection in exposed individuals was slightly increased for adults relative to children, the ABO/Rh blood group was not associated with increased risk of SARS-CoV-2 infection (Table 4A). Additionally, ABO/Rh blood groups were not specifically associated with symptomatic infections. The only variable associated with the occurrence of symptoms in SARS-CoV-2 infection was an age above 18 years [OR 5.48 (95% CI 1.81–16.57)] (Table 4B).
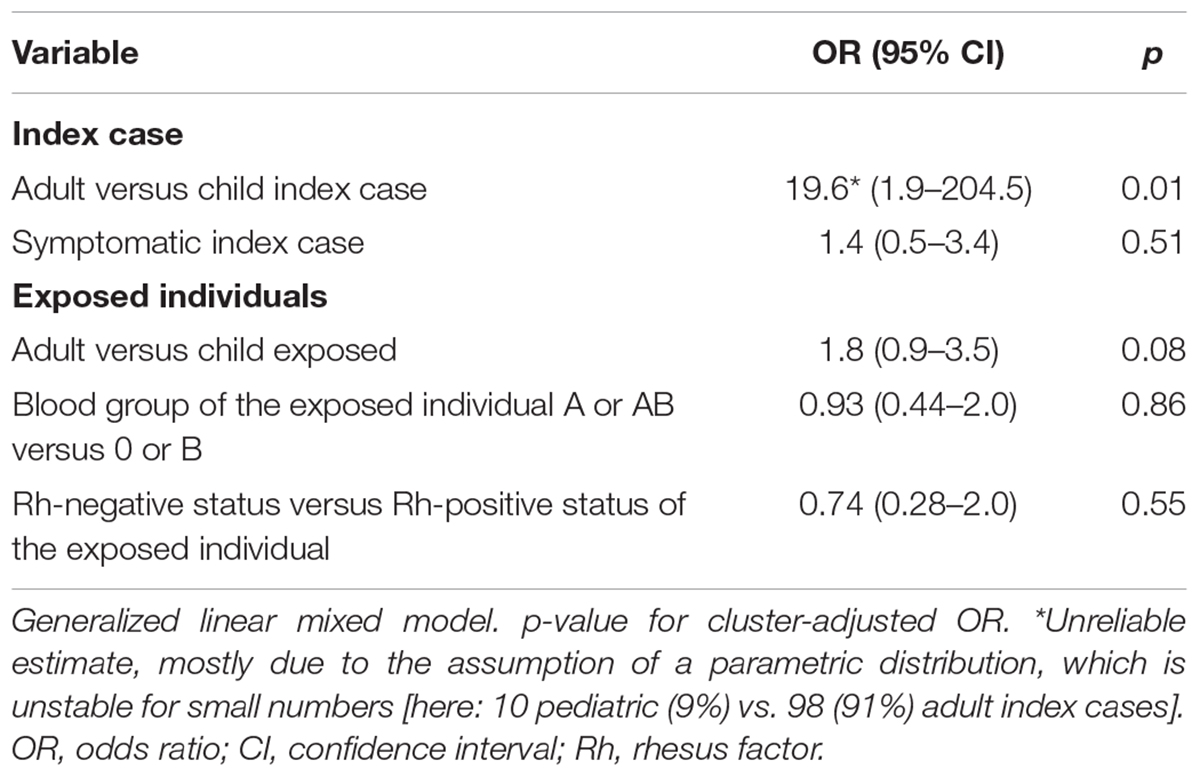
Table 4A. Risk factors for SARS-CoV-2 seropositivity and symptomatic infection. Generalized linear mixed model for risk of SARS-CoV-2 seropositivity of exposed household members.
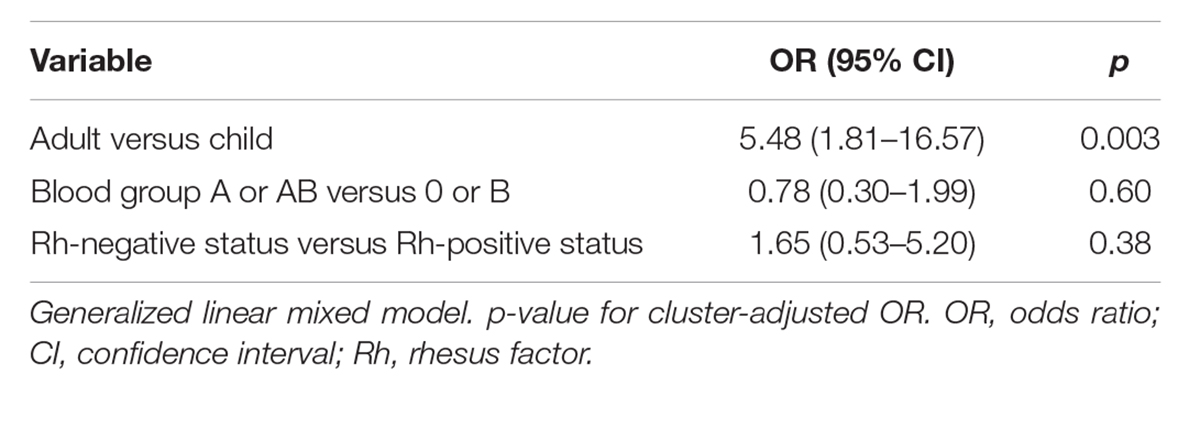
Table 4B. Generalized linear mixed model for risk of symptomatic SARS-CoV-2 infection.
Discussion
This study found blood group A to be moderately overrepresented and blood group O to be moderately underrepresented in SARS-CoV-2 seropositive as compared to seronegative individuals and the reference population (Golinelli et al., 2020; Zietz et al., 2020; Ray et al., 2021). We observed this effect in adults, as previously reported by others (Pendu et al., 2021), but not in children. When considering the clustering of data in families, we found no evidence for blood groups A or AB as a substantial risk factor for SARS-CoV-2 infection in children or adults. This contrast to other studies might be explained by geographical, genetic, and methodological differences (Barnkob et al., 2020; Anderson et al., 2021). Here, we found a significantly lower frequency of Rh-positive blood groups among SARS-CoV-2 seropositive children and being Rh-negative doubled the risk for SARS-CoV-2 seropositivity. This contradicts previous reports in which Rh positivity constituted a risk factor for SARS-CoV-2 infection or severe COVID-19 (Latz et al., 2020; Zietz et al., 2020; Ray et al., 2021). Only one study from Sudan mentions a possible protective effect of presence of Rh-factor (Taha et al., 2020). A different ABO/Rh prevalence in the ethnically different Sudanese population prevents a comparison with our study. We can only hypothesize that the potential differences between adults and children may reflect a different underlying mechanism of ABO blood groups on SARS-CoV-2 infection.
Additionally, we investigated whether ABO incompatibility could potentially influence the risk for SARS-CoV-2 infection within the families. The frequency of transmission between index cases and exposed individuals was equally distributed between the ABO-compatible and ABO-incompatible group, and the risk for SARS-CoV-2 infection was not increased in ABO-compatible individuals in our cohort. This finding could be at least partially influenced by the natural phenomenon of a higher frequency of compatible blood groups within family cohorts due to inheritance of blood type, which makes ABO-compatible SARS-CoV-2 infections more likely. Therefore, to prove or reject the hypothesis of an effect of ABO compatibility on the risk of SARS-CoV-2 infection, transmission events need to be investigated in a cohort of unrelated individuals with known blood groups.
Since households represent the most important location for SARS-CoV-2 transmission, our data inform on the most common clinical scenario. In our cohort, the only parameters that positively correlated with the risk of intrafamilial transmission was the age of the exposed individual and the presence of symptoms in the index case, as described previously (Stich et al., 2021). Here, we confirm age group as a contributing factor, whereas ABO/Rh blood groups are not relevant for the risk of developing symptoms (Davies et al., 2020).
The strength of this multi-center study is its relatively large number of participants, and a separate analysis of infected and exposed children. Blood group determination within a household cohort of exposed SARS-CoV-2 seropositive and seronegative individuals allows controlling for genetic background and environmental influences. Nevertheless, the selection of participants and data collection may have been biased by voluntary participation and self-reporting of symptoms. Furthermore, we did not record data on ethnicity, and despite a relatively ethnic homogeneity in Southern Germany, this may have impacted the analysis. Finally, the findings apply to the SARS-CoV-2 variants circulating in Germany in spring 2020, and their validity in case of later virus variants (e.g., Delta and Omicron) is unclear.
In summary, we found that blood group A was moderately overrepresented in SARS-CoV-2-infected individuals, and the Rh-negative blood group was overrepresented in SARS-CoV-2-infected children. ABO compatibility did not increase the risk for SARS-CoV-2 infection. Individual ABO/Rh blood groups and ABO compatibility were not independent risk factors for SARS-CoV-2 acquisition, neither in children nor in adults.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committees of the University Hospitals Tübingen, Ulm, Freiburg and Heidelberg. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
AJ, HR, AF, and CE conceived the study and designed the experiments. AJ, HR, RE, AF, PH, BT, MS, and K-MD procured the funding. AP, SH, TS, AD, H-JG, and TG performed and interpreted the serological assays. SE and CW performed the blood grouping experiments. HR, AJ, AF, CE, DF, MZ, E-MJ, SFNB, and JR collected the samples or organized the collection. AJ, HR, AF, CE, and K-MD curated the data. CE, AJ, and HR performed the data analysis and generated the tables. AJ and HR wrote the first draft of the manuscript. SS, JR, TG, BT, MS, DF, SNFB, ADMH, and CE revised the first draft of the manuscript critically for important intellectual content. All authors approved the final version of the manuscript and confirm that they had full access to all the data in the study and accept responsibility for the decision to submit for publication.
Funding
This work was supported by the State Ministry of Baden-Württemberg of Science, Research and the Arts Baden-Württemberg within the framework of the special funding line for COVID-19 research. The funding agencies of the study, the Ministry of Science of the State of Baden-Württemberg, had no role in study design, data collection, data analysis, interpretation of data, writing of the report, and the decision to submit the manuscript for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Mareike Walenta and Ann Kathrin Horlacher (Tübingen University) and Carmen Blum, Sevil Essig, Ulrike Formentini, Gudrun Kirsch, Alexandra Niedermeyer, and Boram Song (Ulm University) for assistance with sample processing and patient material storage. We also thank Andrea Evers-Bischoff, Andrea Bevot, and the CPCS at the University Hospital Tübingen and Sandra Steinmann, Yvonne Müller, and Vanessa Missel at University Hospital Ulm for organizational support in conducting the study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmicb.2022.857965/full#supplementary-material
References
Anderson, J. L., May, H. T., Knight, S., Bair, T. L., Muhlestein, J. B., Knowlton, K. U., et al. (2021). Association of sociodemographic factors and blood group type with risk of COVID-19 in a US population. JAMA Netw. Open. 4:e217429. doi: 10.1001/jamanetworkopen.2021.7429
Bari, A., Ch, A., Hareem, S., Bano, I., Rashid, J., and Sadiq, M. (2021). Association of blood groups with the severity and outcome of COVID-19 infection in children. J. Coll. Physicians Surg. Pak. 30, S57–S59.
Barnkob, M. B., Pottegård, A., Støvring, H., Haunstrup, T. M., Homburg, K., Larsen, R., et al. (2020). Reduced prevalence of SARS-CoV-2 infection in ABO blood group O. Blood Adv. 4, 4990–4993. doi: 10.1182/bloodadvances.2020002657
Boudin, L., and Dutasta, F. (2020). Relationship between ABO blood groups and coronavirus disease 2019: study design matters. Clin. Infect. Dis. 72:e918. doi: 10.1093/cid/ciaa1473
Boukhari, R., Breiman, A., Jazat, J., Ruvoën-Clouet, N., Martinez, S., Damais-Cepitelli, A., et al. (2022). ABO blood group incompatibility protects against SARS-CoV-2 transmission. Front. Microbiol. 12:799519. doi: 10.3389/fmicb.2021.799519
Cooling, L. (2015). Blood groups in infection and host susceptibility. Clin. Microbiol. Rev. 28, 801–870.
Davies, N. G., Klepac, P., Liu, Y., Prem, K., Jit, M., Pearson, C. A. B., et al. (2020). Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 26, 1205–1211. doi: 10.1038/s41591-020-0962-9
Deleers, M., Breiman, A., Daubie, V., Maggetto, C., Barreau, I., Besse, T., et al. (2021). Covid-19 and blood groups: ABO antibody levels may also matter. Int. J. Infect. Dis. 104, 242–249. doi: 10.1016/j.ijid.2020.12.025
Dzik, S., Eliason, K., Morris, E. B., Kaufman, R. M., and North, C. M. (2020). COVID-19 and ABO blood groups. Transfusion 60, 1883–1884.
Ellinghaus, D., Degenhardt, F., Bujanda, L., Buti, M., Albillos, A., Invernizzi, P., et al. (2020). Genomewide association study of severe Covid-19 with respiratory failure. N. Engl. J. Med. 383, 1522–1534. doi: 10.1056/NEJMoa2020283
Ellis, P. J. I. (2021). Modelling suggests ABO histo-incompatibility may substantially reduce SARS-CoV-2 transmission. Epidemics 35:100446. doi: 10.1016/j.epidem.2021.100446
German Clinical Trials Register (2020). Available online at from: https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00021521 (accessed February 12, 2021).
Goel, R., Bloch, E. M., Pirenne, F., Al-Riyami, A. Z., Crowe, E., Dau, L., et al. (2021). ABO blood group and COVID-19: a review on behalf of the ISBT COVID-19 working group. Vox Sang. 116, 849–861. doi: 10.1111/vox.13076
Golinelli, D., Boetto, E., Maietti, E., and Fantini, M. P. (2020). The association between ABO blood group and SARS-CoV-2 infection: a meta-analysis. PLoS One 15:e0239508. doi: 10.1371/journal.pone.0239508
Guillon, P., Clément, M., Sébille, V., Rivain, J. G., Chou, C. F., Ruvoën-Clouet, N., et al. (2008). Inhibition of the interaction between the SARS-CoV spike protein and its cellular receptor by anti-histo-blood group antibodies. Glycobiology 18, 1085–1093. doi: 10.1093/glycob/cwn093
Latz, C. A., DeCarlo, C., Boitano, L., Png, C. Y. M., Patell, R., Conrad, M. F., et al. (2020). Blood type and outcomes in patients with COVID-19. Ann. Hematol. 99, 2113–2118.
Le Pendu, J., and Ruvoën-Clouet, N. (2020). Fondness for sugars of enteric viruses confronts them with human glycans genetic diversity. Hum. Genet. 139, 903–910. doi: 10.1007/s00439-019-02090-w
Li, J., Wang, X., Chen, J., Cai, Y., Deng, A., and Yang, M. (2020). Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 190, 24–27.
Ng, O. T., Marimuthu, K., Koh, V., Pang, J., Linn, K. Z., Sun, J., et al. (2021). SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: a retrospective cohort study. Lancet Infect. Dis. 21, 333–343. doi: 10.1016/S1473-3099(20)30833-1
Pendu, J. L., Breiman, A., Rocher, J., Dion, M., and Ruvoën-Clouet, N. A. B. O. (2021). Blood types and COVID-19: spurious, anecdotal, or truly important relationships? A reasoned review of available data. Viruses 13:160. doi: 10.3390/v13020160
Ray, J. G., Schull, M. J., Vermeulen, M. J., and Park, A. L. (2021). Association between ABO and Rh blood groups and SARS-CoV-2 infection or severe COVID-19 illness : a population-based cohort study. Ann. Intern. Med. 174, 308–315. doi: 10.7326/M20-4511
Spielberger, B. D., Goerne, T., Geweniger, A., Henneke, P., and Elling, R. (2021). Intra-household and close-contact SARS-CoV-2 transmission among children – a systematic review. Front. Pediatr. 9:613292. doi: 10.3389/fped.2021.613292
Stich, M., Elling, R., Renk, H., Janda, A., Garbade, S. F., Müller, B., et al. (2021). Transmission of severe acute respiratory syndrome coronavirus 2 in households with children, southwest Germany, May-August 2020. Emerg. Infect. Dis. 27, 3009–3019. doi: 10.3201/eid2712.210978
Taha, S. A. H., Osman, M. E. M., Abdoelkarim, E. A. A., Holie, M. A. I., Elbasheir, M. M., Abuzeid, N. M. K., et al. (2020). Individuals with a Rh-positive but not Rh-negative blood group are more vulnerable to SARS-CoV-2 infection: demographics and trend study on COVID-19 cases in Sudan. New Microbes New Infect. 38:100763. doi: 10.1016/j.nmni.2020.100763
Tönshoff, B., Müller, B., Elling, R., Renk, H., Meissner, P., Hengel, H., et al. (2021). Prevalence of SARS-CoV-2 infection in children and their parents in southwest Germany. JAMA Pediatr. 175, 586–593. doi: 10.1001/jamapediatrics.2021.0001
Wagner, F. F., Kasulke, D., Kerowgan, M., and Flegel, W. A. (1995). Frequencies of the blood groups ABO, Rhesus, D category VI, Kell, and of clinically relevant high-frequency antigens in south-western Germany. Infusionsther. Transfusionsmed. 22, 285–290. doi: 10.1159/000223144
Williamson, E. J., Walker, A. J., Bhaskaran, K., Bacon, S., Bates, C., Morton, C. E., et al. (2020). Factors associated with COVID-19-related death using OpenSAFELY. Nature 584, 430–436. doi: 10.1038/s41586-020-2521-4
Wu, B. B., Gu, D. Z., Yu, J. N., Yang, J., and Shen, W. Q. (2020). Association between ABO blood groups and COVID-19 infection, severity and demise: a systematic review and meta-analysis. Infect. Genet. Evol. 84:104485. doi: 10.1016/j.meegid.2020.104485
Wu, S.-C., Arthur, C. M., Wang, J., Verkerke, H., Josephson, C. D., Kalman, D., et al. (2021). The SARS-CoV-2 receptor-binding domain preferentially recognizes blood group A. Blood Adv. 5, 1305–1309. doi: 10.1182/bloodadvances.2020003259
Zhang, L., Huang, B., Xia, H., Fan, H., Zhu, M., Zhu, L., et al. (2020). Retrospective analysis of clinical features in 134 coronavirus disease 2019 cases. Epidemiol. Infect. 148:e199. doi: 10.1017/S0950268820002010
Keywords: SARS-CoV-2, ABO blood group, children, COVID-19, household transmission
Citation: Janda A, Engel C, Remppis J, Enkel S, Peter A, Hörber S, Ganzenmueller T, Schober S, Weinstock C, Jacobsen E-M, Fabricius D, Zernickel M, Stamminger T, Dietz A, Groß H-J, Bode SFN, Haddad ADM, Elling R, Stich M, Tönshoff B, Henneke P, Debatin K-M, Franz AR and Renk H (2022) Role of ABO Blood Group in SARS-CoV-2 Infection in Households. Front. Microbiol. 13:857965. doi: 10.3389/fmicb.2022.857965
Received: 19 January 2022; Accepted: 28 February 2022;
Published: 06 May 2022.
Edited by:
Fabrizio Chiodo, National Research Council (CNR), ItalyReviewed by:
Marcin Czerwiński, Hirszfeld Institute of Immunology and Experimental Therapy (PAN), PolandJacques Le Pendu, Institut National de la Santé et de la Recherche Médicale (INSERM), France
Cornelis Hendrik Hokke, Leiden University Medical Center, Netherlands
Copyright © 2022 Janda, Engel, Remppis, Enkel, Peter, Hörber, Ganzenmueller, Schober, Weinstock, Jacobsen, Fabricius, Zernickel, Stamminger, Dietz, Groß, Bode, Haddad, Elling, Stich, Tönshoff, Henneke, Debatin, Franz and Renk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanna Renk, Hanna.Renk@med.uni-tuebingen.de