
Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy

 ,
,  , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Questionnaire
- Declare if they were favorable to vaccinations in general (yes/no);
- Report if they had been immunized against the influenza virus in the season 2019/20 (yes/no);
- Report if they had been immunized against the influenza virus in the season 2020/21 (yes/no);
- Refer if COVID-19 vaccines may cause health problems (yes/no);
- Report if they had received at least a single dose of a COVID-19 vaccine (yes/no);
- Refer, if not yet vaccinated, if they were willing to be vaccinated against COVID-19 (yes/no);
- Refer, if not yet vaccinated, if they were willing to be vaccinated against COVID-19 with any formulation (yes/no);
- Refer, if not willing to be vaccinated, the main motivation (I don’t trust vaccines/these vaccines are not effective/I’m allergic/I’ve had the disease/I’m not at risk/the available vaccines may cause severe health consequences);
- Refer if, in their opinion, the COVID-19 vaccination should be mandatory (yes/no);
- Refer if they were favorable to the adoption of the “green pass” (yes/no);
- Report their main source of information about COVID-19 vaccination (health care personnel, scientists/mass media/social media).
2.3. Statistical Analyses
3. Results
- -
- The percentage of individuals vaccinated/willing to be vaccinated changed from 96% to 87.9% (p value < 0.001);
- -
- The proportion of respondents who were favorable to vaccinations in general changed from 51.9% to 35.2% (p value < 0.001);
- -
- The percentage of those who thought that COVID-19 vaccines may cause health problems changed from 80.7% to 96.4% (p value < 0.001);
- -
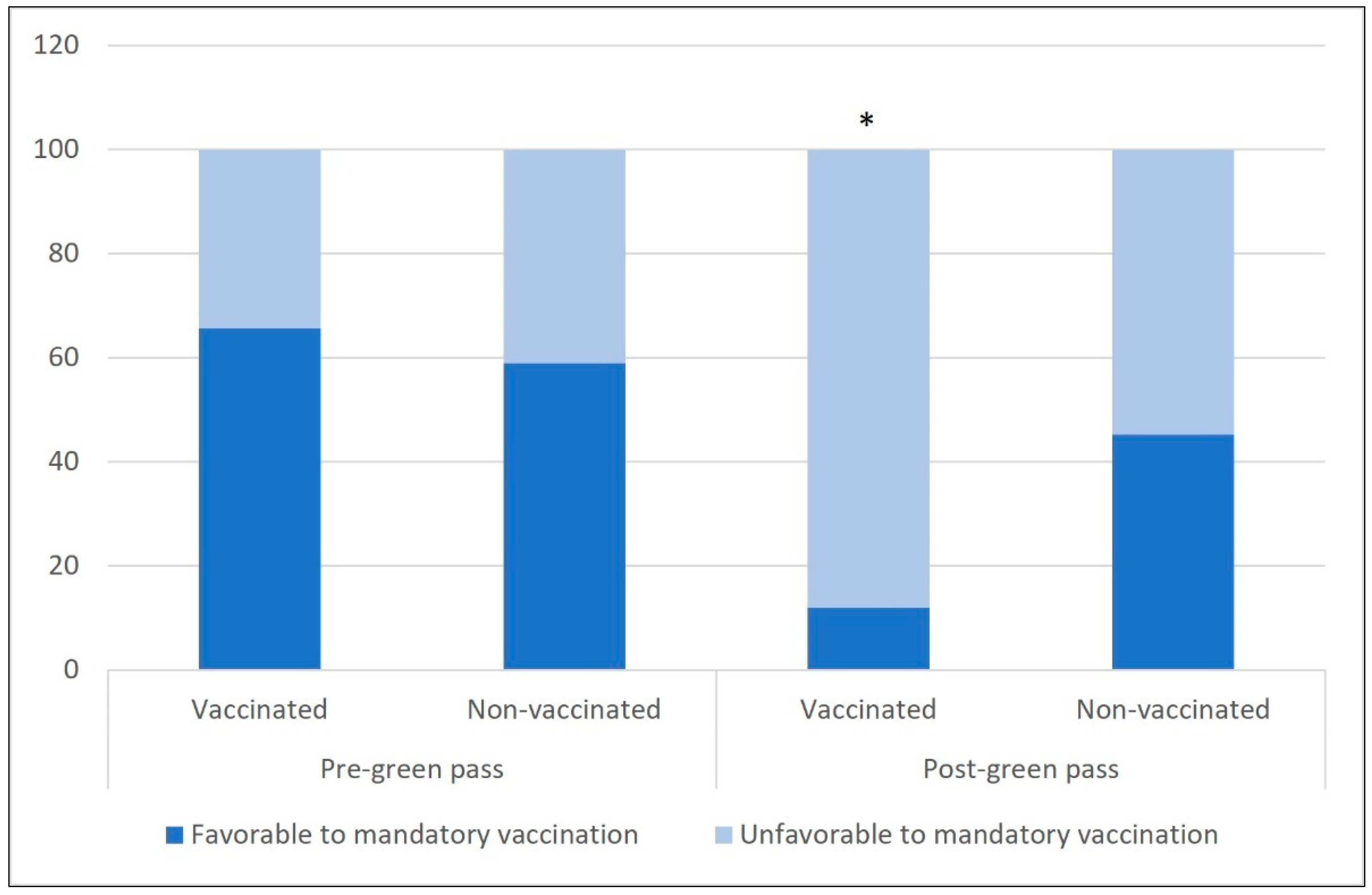
- The percentage of participants who thought that COVID-19 vaccination should be compulsory changed from 64.9% to 16.9% (p value < 0.001);
- -
- The percentage of those who were favorable to the green pass changed from 44.9 to 16.2% (p value < 0.001).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=Cj0KCQiA-OeBBhDiARIsADyBcE7PVve11fZgyLj_kI8swygsjyQf8sMt-rAkiRRBbPgHo0VpON9KyPMaAkgfEALw_wcB (accessed on 23 September 2021).
- Italian National Institute of Health. Caratteristiche dei Pazienti Deceduti Positivi All’infezione da SARS-CoV-2 in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-decessi-italia (accessed on 5 May 2021).
- Napoli, C.; Riccardo, F.; Declich, S.; Dente, M.G.; Pompa, M.G.; Rizzo, C.; Rota, M.C.; Bella, A.; National Working Group. An early warning system based on syndromic surveillance to detect potential health emergencies among migrants: Results of a two-year experience in Italy. Int. J. Environ. Res. Public Health 2014, 11, 8529–8541. [Google Scholar] [CrossRef] [Green Version]
- Napoli, C.; Dente, M.G.; Kärki, T.; Riccardo, F.; Rossi, P.; Declich, S.; Network for the Control of Cross-Border Health Threats in the Mediterranean Basin and Black Sea. Screening for Infectious Diseases among Newly Arrived Migrants: Experiences and Practices in Non-EU Countries of the Mediterranean Basin and Black Sea. Int. J. Environ. Res. Public Health 2015, 12, 15550–15558. [Google Scholar] [CrossRef] [Green Version]
- De Giglio, O.; Napoli, C.; Lovero, G.; Diella, G.; Rutigliano, S.; Caggiano, G.; Montagna, M.T. Antibiotic susceptibility of Legionella pneumophila strains isolated from hospital water systems in Southern Italy. Environ. Res. 2015, 142, 586–590. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Regional Office for Europe Coronavirus disease (COVID-19) Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 5 August 2021).
- García-Montero, C.; Fraile-Martínez, O.; Bravo, C.; Torres-Carranza, D.; Sanchez-Trujillo, L.; Gómez-Lahoz, A.M.; Guijarro, L.G.; García-Honduvilla, N.; Asúnsolo, A.; Bujan, J.; et al. An updated review of SARS-CoV-2 vaccines and the importance of effective vaccination programs in pandemic times. Vaccines 2021, 9, 433. [Google Scholar] [CrossRef] [PubMed]
- Pai, S.M.; Othman, A.A.; Rusch, L.; Masters, J.C.; Greene, D.; Rogge, M.; Gries, J.M.; Clementi, W.; Kumar, P.; Younis, I.; et al. Public Policy Committee of the American College of Clinical Pharmacology. Science and evidence-based review and approval of COVID-19 vaccines: A statement of support for the US FDA. J. Clin. Pharmacol. 2021, 61, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. Vaccinazione Anti-SARS-COV-2/COVID-19 Piano Strategico. Available online: https://www.trovanorme.salute.gov.it/norme/renderPdf.spring?seriegu=SG&datagu=24/03/2021&redaz=21A01802&artp=1&art=1&subart=1&subart1=10&vers=1&prog=001 (accessed on 7 August 2021).
- Italian Ministry of Health. Decreto 2/2/21 “Adozione del Piano Strategico Nazionale dei Vaccini per la Prevenzione Delle Infezioni da SARS-COV-2”. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2021&codLeg=78657&parte=1%20&serie=null (accessed on 7 August 2021).
- Italian Premiership. Piano Vaccinale Anti-COVID. Available online: https://www.governo.it/sites/governo.it/files/210313_Piano_Vaccinale_marzo_2021_1.pdf (accessed on 7 August 2021).
- Italian Premiership. Report Vaccini Anti-COVID 19. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 7 August 2021).
- Italian Premiership. COVID 19 Situazione Italia. Available online: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 7 August 2021).
- Italian Council of Ministers. EU Digital COVID Certificate. Available online: https://www.dgc.gov.it/web/ (accessed on 7 August 2021).
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Agenzia Italiana del Farmaco. Comunicato n. 637 del 15/03/21. AIFA: Sospensione Precauzionale del Vaccino AstraZeneca. Available online: https://www.aifa.gov.it/documents/20142/1289678/Comunicato_AIFA_637.pdf (accessed on 7 August 2021).
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef]
- Italian Council of Ministers. Decreto-Legge n.105 Misure Urgenti per Fronteggiare L’emergenza Epidemiologica da COVID-19 e per L’esercizio in Sicurezza di Attività Sociali ed Economiche. 23 Luglio 2021. Available online: https://www.gazzettaufficiale.it/eli/id/2021/07/23/21G00117/sg (accessed on 7 August 2021).
- Porat, T.; Burnell, R.; Calvo, R.A.; Ford, E.; Paudyal, P.; Baxter, W.L.; Parush, A. “Vaccine Passports” May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19. Vaccines 2021, 9, 902. [Google Scholar] [CrossRef]
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.A.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef]
- Charron, J.; Gautier, A.; Jestin, C. Influence of information sources on vaccine hesitancy and practices. Med. Mal. Infect. 2020, 50, 727–733. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Mazzini, D.; Pecorelli, S. Italian adults’ likelihood of getting a COVID-19 vaccine: A second online survey. Vaccines 2021, 9, 268. [Google Scholar] [CrossRef]
- Gallè, F.; Veshi, A.; Sabella, E.A.; Çitozi, M.; da Molin, G.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C.; Napoli, C. Awareness and Behaviors Regarding COVID-19 among Albanian Undergraduates. Behav. Sci. 2021, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef] [PubMed]
- Italian Institute of Statistics. Demografia in Cifre. Available online: http://demo.istat.it/index.php (accessed on 30 May 2021).
- Gallè, F.; Sabella, E.A.; Da Molin, G.; Parisi, E.A.; Liguori, G.; Montagna, M.T.; De Giglio, O.; Tondini, L.; Orsi, G.B.; Napoli, C. Physical Activity in Older Adults: An Investigation in a Metropolitan Area of Southern Italy. Int. J. Environ. Res. Public Health 2020, 17, 1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallè, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B.; et al. Understanding knowledge and behaviors related to the COVID-19 epidemic in Italian undergraduate students: The EPICO Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary behaviors and physical activity of Italian undergraduate students during lockdown at the time of the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw–Hill: New York, NY, USA, 1978; p. 144. [Google Scholar]
- Kline, P. The Handbook of Psychological Testing, 2nd ed.; Routledge: London, UK, 1999; p. 627. [Google Scholar]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Ed. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Italian Institute of Statistics. Censimento Popolazione e Abitazioni. Available online: http://dati.istat.it/Index.aspx?QueryId=18550 (accessed on 30 May 2021).
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 vaccine acceptance: Results from a survey on vaccine hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Fadda, M.; Suggs, L.S.; Albanese, E. Willingness to vaccinate against Covid-19: A qualitative study involving older adults from Southern Switzerland. Vaccine 2021, 8, 100108. [Google Scholar] [CrossRef]
- Nikolovski, J.; Koldijk, M.; Weverling, G.J.; Spertus, J.; Turakhia, M.; Saxon, L.; Gibson, M.; Whang, J.; Sarich, T.; Zambon, R.; et al. Factors indicating intention to vaccinate with a COVID-19 vaccine among older U.S. adults. PLoS ONE 2021, 16, e0251963. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.J.; Strych, U.; Dor, A. Correlates and disparities of COVID-19 vaccine hesitancy. SSRN 2020. [Google Scholar] [CrossRef]
- Malani, P.N.; Solway, E.; Kullgren, J.T. Older Adults’ Perspectives on a COVID-19 Vaccine. Available online: 10.1001/jamahealthforum.2020.0961 (accessed on 12 August 2021).
- Domnich, A.; Cambiaggi, M.; Vasco, A.; Maraniello, L.; Ansaldi, F.; Baldo, V.; Bonanni, P.; Calabrò, G.E.; Costantino, C.; de Waure, C.; et al. Attitudes and beliefs on influenza vaccination during the COVID-19 pandemic: Results from a representative Italian survey. Vaccines 2020, 8, 711. [Google Scholar] [CrossRef]
- Graeber, D.; Schmidt-Petri, C.; Schröder, C. Attitudes on voluntary and mandatory vaccination against COVID-19: Evidence from Germany. PLoS ONE 2021, 16, e0248372. [Google Scholar] [CrossRef]
- Cave, E. Voluntary vaccination: The pandemic effect. Legal Stud. 2017, 37, 279–304. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Item | n (%) |
|---|---|
| Vaccinated against COVID-19 | |
| Yes | 901 (86.6) |
| No | 140 (13.4) |
| If not vaccinated, willing to be vaccinated against COVID-19 | |
| Yes | 64 (45.7) |
| No | 76 (54.3) |
| If not vaccinated, willing to be vaccinated against COVID-19 with any | |
| formulation | |
| Yes | 0 (0) |
| No | 140 (100) |
| If neither vaccinated nor willing to be, main motivation for refusal: | |
| I don’t trust vaccines | 3 (3.9) |
| The available vaccines are not effective | 48 (63.2) |
| I’m allergic | 0 (0) |
| I’ve had the disease | 15 (19.7) |
| I’m not at risk | 1 (1.3) |
| The available vaccines may cause severe health consequences | 9 (11.8) |
| Item | Participants n = 1041 | Vaccinated/Willing to Be Vaccinated n (%) | p Value | |
|---|---|---|---|---|
| Yes | No | |||
| Gender | 0.024 | |||
| males | 434 (41.7) | 393 (90.6) | 41 (9.4) | |
| females | 607 (58.3) | 572 (94.2) | 35 (5.8) | |
| Age | <0.001 | |||
| ≤76 years | 553 (53.1) | 487 (88.1) | 66 (11.9) | |
| ≥77 years | 488 (46.9) | 47 8 (98) | 10 (2) | |
| Educational level | <0.001 | |||
| Elementary | 28 (2.7) | 26 (92.9) | 2 (7.1) | |
| Middle | 310 (29.8) | 277 (89.4) | 33 (10.6) | |
| High school | 515 (49.5) | 496 (96.3) | 19 (3.7) | |
| Degree | 188 (18.1) | 166 (88.3) | 22 (11.7) | |
| Item | Respondents n (%) | Vaccinated/Willing to Be Vaccinated n (%) | p Value | |
|---|---|---|---|---|
| Yes | No | |||
| Favorable to vaccination in general | <0.001 | |||
| Yes | 470 (45.1) | 460 (97.9) | 10 (2.1) | |
| No | 571 (54.9) | 505 (88.4) | 66 (11.6) | |
| Vaccinated against influenza (season 2019/20) | 0.004 | |||
| Yes | 269 (25.8) | 260 (96.7) | 9 (3.3) | |
| No | 772 (74.2) | 705 (91.3) | 67 (8.7) | |
| Vaccinated against influenza (season 2020/21) | <0.001 | |||
| Yes | 768 (73.8) | 726 (94.5) | 42 (5.5) | |
| No | 273 (26.2) | 239 (87.5) | 34 (12.5) | |
| Might the COVID-19 vaccines cause health problems? | 0.015 | |||
| Yes | 906 (87) | 833 (91.9) | 73 (8.1) | |
| No | 135 (13) | 132 (97.8) | 3 (2.2) | |
| Might all the COVID-19 vaccines have the same side effects? | 0.001 | |||
| Yes | 188 (18.1) | 185 (98.4) | 3 (1.6) | |
| No | 853 (81.9) | 780 (91.4) | 73 (8.6) | |
| Should COVID-19 vaccination become mandatory? | 0.388 | |||
| Yes | 474 (45.5) | 443 (93.5) | 31 (6.5) | |
| No | 567 (54.5) | 522 (92.1) | 45 (7.9) | |
| Favorable to the adoption of the “green pass” | 0.4 | |||
| Yes | 347 (33.3) | 325 (93.7) | 22 (6.3) | |
| No | 694 (66.7) | 640 (92.2) | 54 (7.8) | |
| Main sources of information about COVID-19 | 0.009 | |||
| vaccination | ||||
| Healthcare personnel, scientists | 636 (61.1) | 577 (90.7) | 59 (9.3) | |
| Mass media (i.e., television, magazines) | 402 (38.6) | 385 (95.8) | 17 (4.2) | |
| Social media (i.e., Facebook, Twitter, Instagram, WhatsApp) | 3 (0.3) | 3 (100) | 0 (0) | |
| Independent Variable | Vaccine Acceptance |
|---|---|
| OR (CI 95%) | |
| Educational level | |
| Elementary/middle | Reference |
| High school/degree | 1.875 (1.113–3.161) * |
| Source of information | |
| Health care personnel, scientists | Reference |
| Mass media/social media | 2.415 (1.358–4.296) ** |
| Date of fulfilling the questionnaire | |
| Before the mandatory adoption of green pass | Reference |
| After the mandatory adoption of green pass | 0.218 (0.129–0.369) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines 2021, 9, 1222. https://doi.org/10.3390/vaccines9111222
Gallè F, Sabella EA, Roma P, Da Molin G, Diella G, Montagna MT, Ferracuti S, Liguori G, Orsi GB, Napoli C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines. 2021; 9(11):1222. https://doi.org/10.3390/vaccines9111222
Chicago/Turabian StyleGallè, Francesca, Elita Anna Sabella, Paolo Roma, Giovanna Da Molin, Giusy Diella, Maria Teresa Montagna, Stefano Ferracuti, Giorgio Liguori, Giovanni Battista Orsi, and Christian Napoli. 2021. "Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy" Vaccines 9, no. 11: 1222. https://doi.org/10.3390/vaccines9111222