
Applications of Medical Digital Technologies for Noncommunicable Diseases for Follow-Up during the COVID-19 Pandemic
 ,
,  and
and
Abstract
:1. Introduction
1.1. Magnitude of the Problem
1.2. Aim of the Study
1.3. Research Questions
- -
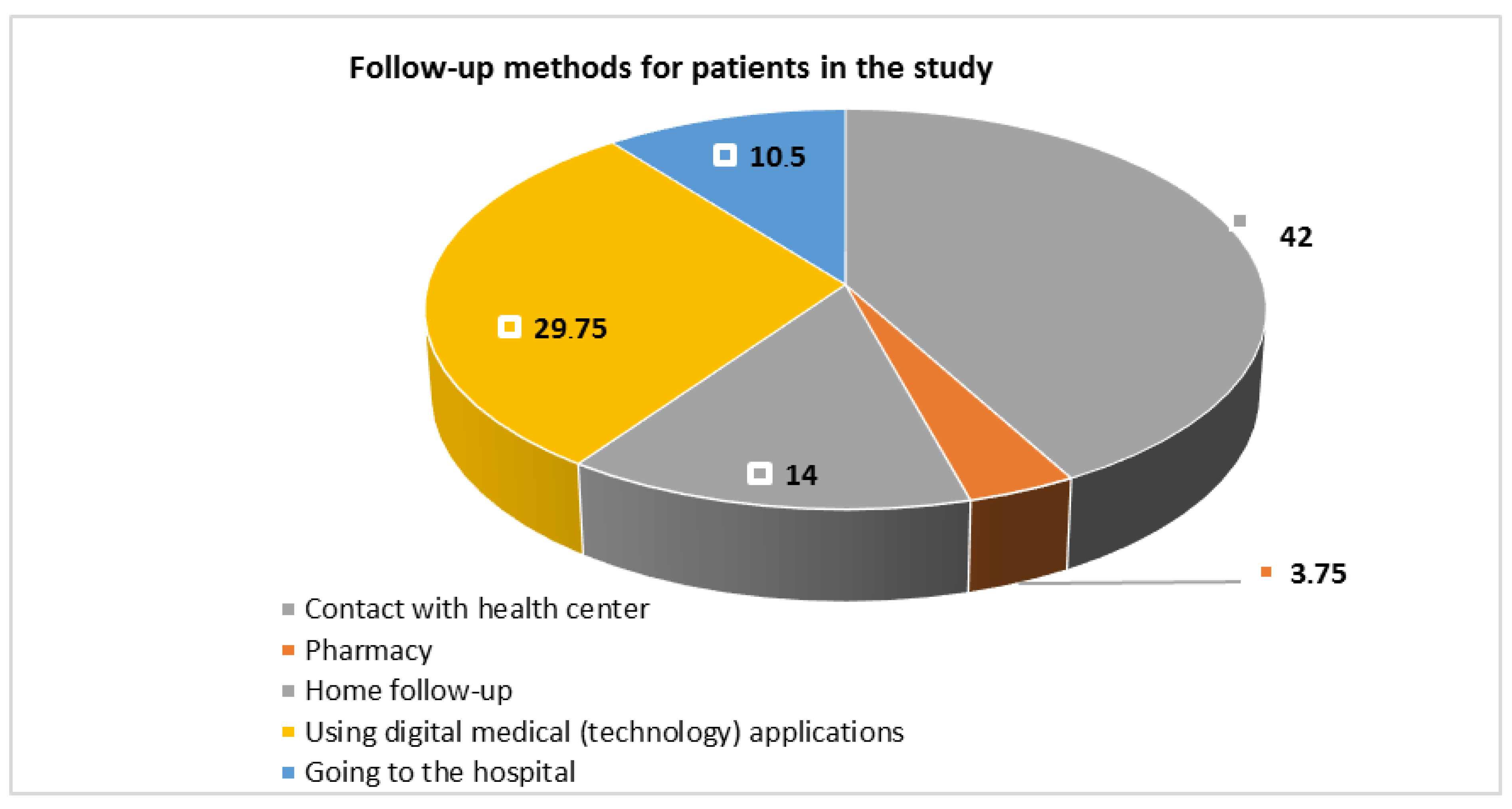
- What are the methods of follow-up for patients with NCDs during the COVID-19 pandemic?
- -
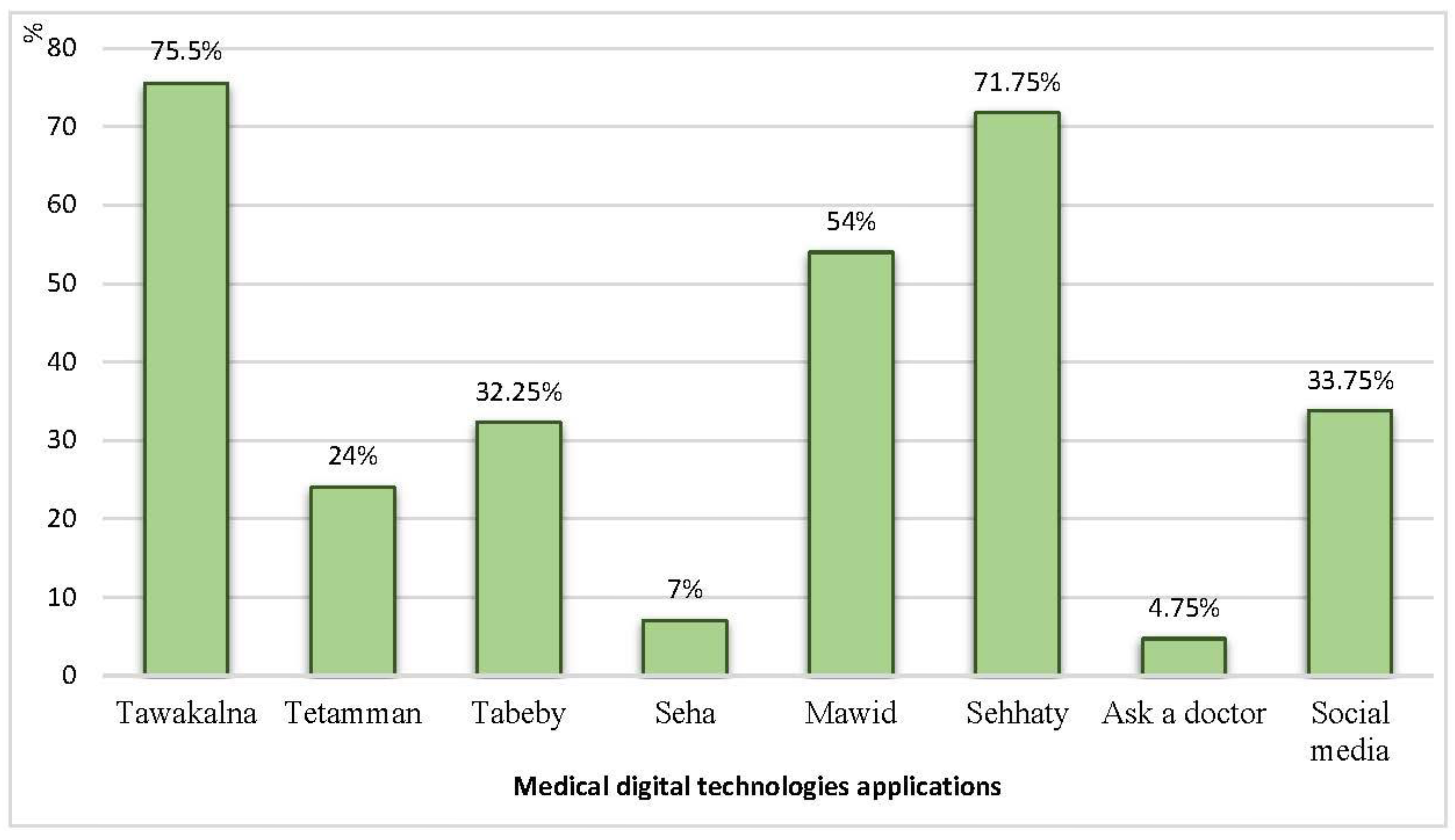
- What are the applications of medical digital technologies in the follow-up of patients with NCDs during the COVID-19 pandemic?
- -
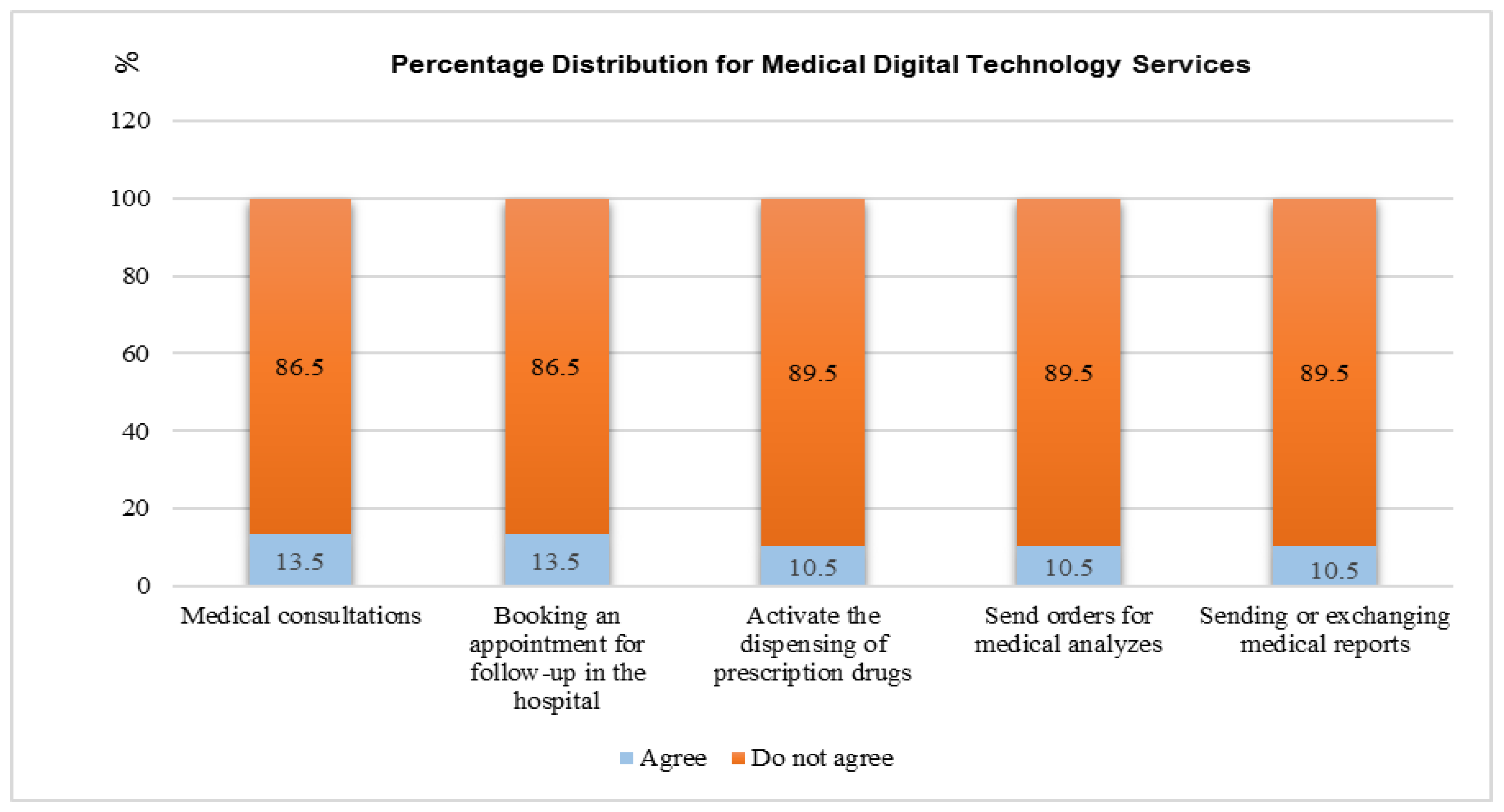
- What are the services of applications of medical digital technologies for follow-up of patients with NCDs during the COVID-19 pandemic?
2. Subjects and Methods
2.1. Research Design
2.2. Setting
2.3. Subjects
2.4. Sampling Design
2.5. Sample Size
2.6. Tools for Data Collection
2.6.1. Fieldwork
2.6.2. Validity and Reliability
2.6.3. Pilot Study
2.6.4. Data Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Recommendation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). The World Health Report 2008: Primary Health Care: Now More TEMPthan Ever. 2020. Available online: https://apps.who.int/iris/handle/10665/43949 (accessed on 1 May 2020).
- Mandil, A.M.; Alfurayh, N.A.; Aljebreen, M.A.; Aldukhi, S.A. Physical activity and major non-communicable diseases among physicians in Central Saudi Arabia. Saudi Med. J. 2016, 37, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Status Report on Noncommunicable Diseases. 2010. Available online: https://www.who.int/nmh/publications/ncd_report_full_en.pdf (accessed on 23 April 2021).
- Larentis, A.V.; Barbosa, D.N.F.; da Silva, C.R.; Barbosa, J.L.V. Applied Computing to Education on Noncommunicable Chronic Diseases: A Systematic Mapping Study. Telemed. e-Health 2020, 26, 147–163. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Country Cooperation Strategy for WHO and Saudi Arabia 2012–2016. 2013. Available online: https://apps.who.int/iris/handle/10665/113227 (accessed on 25 August 2021).
- Memish, Z.A.; Jaber, S.; Mokdad, A.H.; AlMazroa, M.A.; Murray, C.J.; Al Rabeeah, A.A. Burden of disease, injuries, and risk factors in the Kingdom of Saudi Arabia, 1990–2010. Prev. Chronic Dis. 2014, 11, 140176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Noncommunicable Diseases. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 March 2021).
- Lunde, P.; Nilsson, B.B.; Bergland, A.; Kvaerner, K.J.; Bye, A. The Effectiveness of Smartphone Apps for Lifestyle Improvement in Noncommunicable Diseases: Systematic Review and Meta-Analyses. J. Med. Internet Res. 2018, 20, e162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pop, T.L.; Namazova-Baranova, L.; Mestrovic, J.; Nigri, L.; Vural, M.; Sacco, M.; Giardino, I.; Ferrara, P.; Pettoello-Mantovani, M. The Role of Healthy Lifestyle Promotion, Counseling, and Follow-up in Noncommunicable Diseases Prevention. J. Pediatr. 2020, 217, 221–223.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaga, O.M.; Vasilescu, L.; Chereches, R.M. Use and effectiveness of behavioural economics in interventions for lifestyle risk factors of non-communicable diseases: A systematic review with policy implications. Perspect. Public Health 2018, 138, 100–110. [Google Scholar] [CrossRef]
- Golechha, M. Healthcare agenda for the Indian government. Indian J. Med. Res. 2015, 141, 151–153. [Google Scholar] [CrossRef]
- WHO. COVID-19 Disrupting Services to Treat Non-Communicable Diseases, WHO Survey Finds. 2020. Available online: https://news.un.org/en/story/2020/06/1065172 (accessed on 15 March 2021).
- Kluge, H.H.P.; Wickramasinghe, K.; Rippin, H.L.; Mendes, R.; Peters, D.H.; Kontsevaya, A.; Breda, J. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet 2020, 395, 1678–1680. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; WHO, World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/311941/9789241550505-eng.pdf?ua=1 (accessed on 14 January 2021).
- World Health Organization. Global Strategy on Digital Health 2020–2025; WHO: Geneva, Switzerland, 2010; Available online: https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf (accessed on 23 April 2021).
- Saleh, S.; Farah, A.; Dimassi, H.; El Arnaout, N.; Constantin, J.; Osman, M.; El Morr, C.; Alameddine, M. Using Mobile Health to Enhance Outcomes of Noncommunicable Diseases Care in Rural Settings and Refugee Camps: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e137. [Google Scholar] [CrossRef]
- Uppal, H.; Rai, S. Role of Rehabilitation during COVID-19 pandemic: An Indian Perspective. Disaster Med. Public Health Prep. 2020, 16, 409–412. [Google Scholar] [CrossRef]
- Boitsov, S.A.; Vylegzhanin, S.V. Prevention of noncommunicable diseases in a local therapist’s practice: Content, problems, solution ways, and prospects. Ter. Arkhiv 2015, 87, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Kelli, H.M.; Witbrodt, B.; Shah, A. The future of mobile health applications and devices in cardiovascular health. Eur. Med. J. Innov. 2017, 2017, 92. [Google Scholar]
- Domeyer, P.; Katsari, V.; Mariolis, A. Chronic non-communicable diseases: A sacrifice on the altar of COVID-19? Br. J. Gen. Pract. 2020, 70, 281. [Google Scholar] [CrossRef] [PubMed]
- Anthony Jnr, B. Implications of telehealth and digital care solutions during COVID-19 pandemic: A qualitative literature review. Inform. Health Soc. Care 2021, 46, 68–83. [Google Scholar] [CrossRef]
- Molina, E.; Sarmiento Torres, C.E.; Salazar-Cabrera, R.; Lopez, D.M.; Vargas-Canas, R. Intelligent Telehealth System To Support Epilepsy Diagnosis. J. Multidiscip. Healthc. 2020, 13, 433–445. [Google Scholar] [CrossRef]
- Abdel-Basset, M.; Chang, V.; Nabeeh, N.A. An intelligent framework using disruptive technologies for COVID-19 analysis. Technol. Forecast. Soc. Change 2021, 163, 120431. [Google Scholar] [CrossRef] [PubMed]
- Algabbani, A.; Alqahtani, A.; BinDhim, N. Prevalence and determinants of non-communicable diseases in Saudi Arabia. Food Drug Regul. Sci. J. 2019, 2, 1. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K. Socioeconomic determinants and inequalities in the prevalence of non-communicable diseases in Saudi Arabia. Int. J. Equity Health 2021, 20, 174. [Google Scholar] [CrossRef]
- Gosadi, I.M.; Daghriri, K.A.; Otayf, A.A.; Nemri, A.A.; Kaal, A.A.; Qussadi, A.M.; Maashi, M.M.; Arishy, A.M.; Mushafa, H.M.; Salim, A.M. Are patients affected by chronic non-communicable diseases aware of their own clinical and laboratory parameters? A cross-sectional study from the south of Saudi Arabia. Saudi J. Biol. Sci. 2021, 28, 2951–2955. [Google Scholar] [CrossRef]
- Rahamathulla, M.P. Frequency and Awareness of Risk Factors of Non-Communicable Diseases among University Students in Saudi Arabia. Pak. J. Med. Sci. 2020, 36, 740–745. [Google Scholar] [CrossRef] [Green Version]
- Geleta, T.A.; Deriba, B.S.; Beyane, R.S.; Mohammed, A.; Birhanu, T.; Jemal, K. COVID-19 Pandemic Preparedness and Response of Chronic Disease Patients in Public Health Facilities. Int. J. Gen. Med. 2020, 13, 1011–1023. [Google Scholar] [CrossRef] [PubMed]
- Mitwalli, J.; Njaifan, N.; Harere, R.; Sharaf, N.; Owaidah, A.; Bamookrah, K. The Impact of COVID 19 Precautionary Measures on Management of Chronic Disease Patients Following in Primary Health Care Centers Jeddah, Saudi Arabia, 2020. Am. J. Health Med. Nurs. Pract. 2021, 6, 53–65. [Google Scholar] [CrossRef]
- Goncalves-Bradley, D.C.; AR, J.M.; Ricci-Cabello, I.; Villanueva, G.; Fonhus, M.S.; Glenton, C.; Lewin, S.; Henschke, N.; Buckley, B.S.; Mehl, G.L.; et al. Mobile technologies to support healthcare provider to healthcare provider communication and management of care. Cochrane Database Syst. Rev. 2020, 8, CD012927. [Google Scholar] [CrossRef] [PubMed]
- Miele, G.; Straccia, G.; Moccia, M.; Leocani, L.; Tedeschi, G.; Bonavita, S.; Lavorgna, L.; Digital Technologies, W. How to Ensure Patient Needs and Continuity of Care at the Time of COVID-19 Pandemic. Telemed. J. e-Health 2020, 26, 1533–1536. [Google Scholar] [CrossRef] [PubMed]
- Anglemyer, A.; Moore, T.H.; Parker, L.; Chambers, T.; Grady, A.; Chiu, K.; Parry, M.; Wilczynska, M.; Flemyng, E.; Bero, L. Digital contact tracing technologies in epidemics: A rapid review. Cochrane Database Syst. Rev. 2020, 8, CD013699. [Google Scholar] [CrossRef]
- Gummidi, B.; John, O.; Jha, V. Continuum of care for non-communicable diseases during COVID-19 pandemic in rural India: A mixed methods study. J. Fam. Med. Prim. Care 2020, 9, 6012–6017. [Google Scholar] [CrossRef]
- Alanzi, T.M.; Althumairi, A.; Aljaffary, A.; Alfayez, A.; Alsalman, D.; Alanezi, F.; Alhodaib, H.; AlShammari, M.M.; Al-Dossary, R.; Al-Rayes, S.; et al. Evaluation of the Mawid mobile healthcare application in delivering services during the COVID-19 pandemic in Saudi Arabia. Int. Health 2021, 14, 142–151. [Google Scholar] [CrossRef]
- Khan, A.; Alahmari, A.; Almuzaini, Y.; Alturki, N.; Aburas, A.; Alamri, F.A.; Albagami, M.; Alzaid, M.; Alharbi, T.; Alomar, R.; et al. The Role of Digital Technology in Responding to COVID-19 Pandemic: Saudi Arabia’s Experience. Risk Manag. Healthc. Policy 2021, 14, 3923–3934. [Google Scholar] [CrossRef]
- Alharbi, R.; Qadri, A.; Mahnashi, M.; Hakami, A.; Darraj, B.; Shnaimer, J.; Gosadi, I. Utilization of Health Applications Among Patients Diagnosed with Chronic Diseases in Jazan, Saudi Arabia During the COVID-19 Pandemic. Patient Prefer. Adherence 2021, 15, 2063–2070. [Google Scholar] [CrossRef]
- Ilowite, J.; Lisker, G.; Greenberg, H. Digital Health Technology and Telemedicine-Based Hospital and Home Programs in Pulmonary Medicine During the COVID-19 Pandemic. Am. J. Ther. 2021, 28, e217–e223. [Google Scholar] [CrossRef]
- Hoffman, J.D.; Shayegani, R.; Spoutz, P.M.; Hillman, A.D.; Smith, J.P.; Wells, D.L.; Popish, S.J.; Himstreet, J.E.; Manning, J.M.; Bounthavong, M.; et al. Virtual academic detailing (e-Detailing): A vital tool during the COVID-19 pandemic. J. Am. Pharm. Assoc. 2020, 60, e95–e99. [Google Scholar] [CrossRef] [PubMed]
- Darwish, T.; Korouri, S.; Pasini, M.; Cortez, M.V.; IsHak, W.W. Integration of Advanced Health Technology Within the Healthcare System to Fight the Global Pandemic: Current Challenges and Future Opportunities. Innov. Clin. Neurosci. 2021, 18, 31–34. [Google Scholar] [PubMed]
- Ammenwerth, E.; Duftschmid, G.; Al-Hamdan, Z.; Bawadi, H.; Cheung, N.T.; Cho, K.H.; Goldfarb, G.; Gulkesen, K.H.; Harel, N.; Kimura, M.; et al. International Comparison of Six Basic eHealth Indicators Across 14 Countries: An eHealth Benchmarking Study. Methods Inf. Med. 2020, 59, e46–e63. [Google Scholar] [CrossRef] [PubMed]
- Yin, A.L.; Gheissari, P.; Lin, I.W.; Sobolev, M.; Pollak, J.P.; Cole, C.; Estrin, D. Role of Technology in Self-Assessment and Feedback Among Hospitalist Physicians: Semistructured Interviews and Thematic Analysis. J. Med. Internet Res. 2020, 22, e23299. [Google Scholar] [CrossRef]
- Lapao, L.V.; Peyroteo, M.; Maia, M.; Seixas, J.; Gregorio, J.; Mira da Silva, M.; Heleno, B.; Correia, J.C. Implementation of Digital Monitoring Services During the COVID-19 Pandemic for Patients With Chronic Diseases: Design Science Approach. J. Med. Internet Res. 2021, 23, e24181. [Google Scholar] [CrossRef]
- Saudi Ministry of Health (MOH). e-Health Application Launched. 2017. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/News/Pages/News-2017-12-14-007.aspx (accessed on 16 July 2021).
- Seixas, A.A.; Olaye, I.M.; Wall, S.P.; Dunn, P. Optimizing Healthcare Through Digital Health and Wellness Solutions to Meet the Needs of Patients With Chronic Disease During the COVID-19 Era. Front. Public Health 2021, 9, 667654. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | N = 400 | % | |
|---|---|---|---|
| Age | 18 ≥ 25 years | 43 | 10.8 |
| 25 ≥ 35 years | 50 | 12.5 | |
| 35 ≥ 45 years | 48 | 12 | |
| 45 ≥ 55 years | 100 | 25 | |
| 55 ≥ 65 years | 136 | 34 | |
| 65 ≥ 75 years | 17 | 4.2 | |
| 75 ≥ 85 years | 6 | 1.5 | |
| Mean ± SD | 47.32 ± 14.362 | ||
| Min−max | 18–85 | ||
| Gender | Male | 149 | 37.2 |
| Female | 251 | 62.8 | |
| Marital status | Single | 54 | 13.5 |
| Married | 283 | 70.7 | |
| Divorced | 19 | 4.8 | |
| Widow | 44 | 11 | |
| Occupation | Worker | 9 | 2.2 |
| Housewife | 126 | 31.5 | |
| Student | 32 | 8 | |
| Office clerk | 110 | 27.5 | |
| Retired | 44 | 11 | |
| Not working | 79 | 19.8 | |
| Educational attainment | Illiterate | 100 | 25 |
| Literate | 94 | 23.6 | |
| Secondary level | 85 | 21.2 | |
| Highly qualified | 121 | 30.2 | |
| Financial status | Not enough to meet basic and medical needs | 115 | 28.8 |
| Enough to meet basic and medical needs | 285 | 71.2 | |
| Residence (type of town) | Village | 64 | 16 |
| City | 336 | 84 | |
| Items. | N = 400 | % | |
|---|---|---|---|
| * Patient diagnosed with: | |||
| 230 | 57.5 | |
| 277 | 69.2 | |
| 37 | 9.25 | |
| 35 | 8.75 | |
| 2 | 0.5 | |
| 1 | 0.25 | |
| Duration of disease |
| 32 | 8 |
| 100 | 25 | |
| 138 | 34.5 | |
| 130 | 32.5 | |
| Regular medication |
| 326 | 81.5 |
| 74 | 18.5 | |
| Family history for noncommunicable disease |
| 264 | 66 |
| 136 | 34 | |
| Smoking |
| 97 | 24.2 |
| 303 | 75.8 | |
| Previous accidents |
| 74 | 18.5 |
| 326 | 81.5 | |
| Allergic conditions |
| 127 | 31.8 |
| 273 | 68.2 | |
| Sufficient time to sleep |
| 254 | 63.5 |
| 146 | 36.5 | |
| Passive smoking |
| 182 | 45.5 |
| 218 | 54.5 | |
| Items | N = 400 | % |
|---|---|---|
| Frequency of follow-up: | ||
| 31 | 7.8 |
| 20 | 5 |
| 210 | 52.4 |
| 139 | 34.8 |
| Pattern of follow-up: | ||
| 96 | 24 |
| 200 | 50 |
| 104 | 26 |
| Progress of health status during follow-up: | ||
| 145 | 36.2 |
| 131 | 32.8 |
| 57 | 14.2 |
| 67 | 16.8 |
| * Desire to visit member of the health team during follow-up: | ||
| 368 | 92 |
| 102 | 25.5 |
| 29 | 7.2 |
| 93 | 23.2 |
| Going to follow-up with a relative: | ||
| 181 | 45.2 |
| 219 | 54.8 |
| Specified treatment during follow-up: | ||
| 318 | 79.5 |
| 82 | 20.5 |
| Symptoms and signs known to the patient requiring a visit to the hospital: | ||
| 308 | 77 |
| 92 | 23 |
| Instructions/education given during follow-up: | ||
| 301 | 75.2 |
| 99 | 24.8 |
| Any change in medication during follow-up: | ||
| 230 | 57.5 |
| 170 | 42.5 |
| Items | N = 400 | % | |
|---|---|---|---|
| Do you know the health applications of the Ministry of Health? | Yes | 239 | 59.8 |
| No | 161 | 40.2 | |
| Do these applications use social distancing during the COVID-19 pandemic? | Yes | 172 | 43 |
| No | 228 | 57 | |
| Do you use telemedicine consultations? | Yes | 119 | 29.8 |
| No | 281 | 70.2 | |
| Does the use of medical digital technology applications prevent you from visiting the hospital? | Yes | 80 | 20 |
| No | 320 | 80 | |
| Do digital medical technology applications provide you with all the medical information you need? | Yes | 78 | 19.5 |
| No | 322 | 80.5 | |
| Is there an effective interaction with the medical team through the application? | Yes | 73 | 18.2 |
| No | 327 | 81.8 | |
| Does it send you notifications of health instructions through the application used? | Yes | 67 | 16.8 |
| No | 333 | 83.2 | |
| Are medical digital technology applications available at any time and place? | Yes | 66 | 16.5 |
| No | 334 | 83.5 | |
| Can you send medical reports through medical digital technology to the doctor in the hospital? | Yes | 58 | 14.5 |
| No | 342 | 85.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, E.S.E.; Al-Shenqiti, A.M.; Ramadan, R.M.E.-S. Applications of Medical Digital Technologies for Noncommunicable Diseases for Follow-Up during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 12682. https://doi.org/10.3390/ijerph191912682
Hussein ESE, Al-Shenqiti AM, Ramadan RME-S. Applications of Medical Digital Technologies for Noncommunicable Diseases for Follow-Up during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(19):12682. https://doi.org/10.3390/ijerph191912682
Chicago/Turabian StyleHussein, Eman Sobhy Elsaid, Abdullah Mohammed Al-Shenqiti, and Reda Mohamed El-Sayed Ramadan. 2022. "Applications of Medical Digital Technologies for Noncommunicable Diseases for Follow-Up during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 19: 12682. https://doi.org/10.3390/ijerph191912682