
Prediction of SARS-CoV-2-Related Lung Inflammation Spreading by V:ERITAS (Vanvitelli Early Recognition of Inflamed Thoracic Areas Spreading)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Chart Review
2.2. Definition of Outcome and Group Definitions
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.; Sigurslid, H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clin-ical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Foieni, F.; Sala, G.; Mognarelli, J.G.; Suigo, G.; Zampini, D.; Pistoia, M.; Ciola, M.; Ciampani, T.; Ultori, C.; Ghiringhelli, P. Derivation and validation of the clinical prediction model for COVID-19. Intern. Emerg. Med. 2020, 15, 1409–1414. [Google Scholar] [CrossRef]
- Ageno, W.; Cogliati, C.; Perego, M.; Girelli, D.; Crisafulli, E.; Pizzolo, F.; Olivieri, O.; Cattaneo, M.; Benetti, A.; Corradini, E.; et al. Clinical risk scores for the early prediction of severe outcomes in patients hospitalized for COVID-19. Intern. Emerg. Med. 2021, 16, 989–996. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT imaging features of 2019 novel coronavirus (2019–nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosentini, R.; Groff, P.; Brambilla, A.M.; Todeschini, R.C.; Gangitano, G.; Ingrassia, S.; Marino, R.; Nori, F.; Pagnozzi, F.; Panero, F.; et al. SIMEU position paper on non-invasive respiratory support in COVID-19 pneumonia. Intern. Emerg. Med. 2022, 1–15. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or moderate COVID-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflamma-tory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef]
- Engberg, M.; Bonde, J.; Sigurdsson, S.T.; Møller, K.; Nayahangan, L.J.; Berntsen, M.; Eschen, C.T.; Haase, N.; Bache, S.; Konge, L.; et al. Training non-intensivist doctors to work with COVID-19 patients in inten-sive care units. Acta Anaesthesiol. Scand. 2021, 65, 664–673. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diag-nosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Vranas, K.C.; Golden, S.E.; Mathews, K.S.; Schutz, A.; Valley, T.S.; Duggal, A.; Seitz, K.P.; Chang, S.Y.; Nugent, S.; Slatore, C.G.; et al. The Influence of the COVID-19 Pandemic on ICU Organization, Care Processes, and Frontline Clinician Experiences. Chest 2021, 160, 1714–1728. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.; Li, P.; Chen, Y.; Fang, K.; Chen, B.; Wang, S.; Feng, X.; Wang, Z.; Xiong, M.; Zheng, R.; et al. A Risk Prediction Model for Evaluating the Disease Progression of COVID-19 Pneumonia. Front. Med. 2020, 7, 556886. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients With COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.; Du, H.; Li, J.; Wang, Y.; Wu, X.; Wang, C.; Zhang, Y.; Zhang, G.; Zhao, Y.; Kang, W.; et al. Early pre-diction and identification for severe patients during the pandemic of COVID-19: A severe COVID-19 risk model constructed by multivariate logistic regression analysis. J. Glob. Health 2020, 10, 020510. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Cobben, N.A.; Henderson, R.F.; Wouters, E.F.; van Dieijen-Visser, M. Usefulness of lactate dehy-drogenase and its isoenzymes as indicators of lung damage or inflammation. Eur. Respir. J. 1996, 9, 1736–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Respiratory Support Outcome | ||||
|---|---|---|---|---|
| No. | No Respiratory Support, NC, or HFNC | Need for CPAP, NIV, or OTI | p * | |
| Age (years) † | 0.7036 | |||
| mean 62 ± 4 | ||||
| range 26–89 | ||||
| ≤63 | 67 | 44 | 23 | |
| >63 | 56 | 34 | 22 | |
| Gender | 0.0012 ‡ | |||
| Male | 80 | 42 | 38 | |
| Female | 43 | 36 | 7 | |
| CTSS † | <0.0001 ‡ | |||
| mean 7.7 ± 4.4 | ||||
| range 0–17 | ||||
| ≤7 | 63 | 54 | 9 | |
| >7 | 60 | 24 | 36 | |
| P/F ratio † | <0.0001 ‡ | |||
| mean 260 ± 101 | ||||
| range 69–500 | ||||
| >268 | 61 | 57 | 4 | |
| <268 | 63 | 21 | 41 | |
| LDH (U/L) a | <0.0001 ‡ | |||
| mean 297 ± 114 | ||||
| range 125–243 | ||||
| ≤243 | 48 | 43 | 5 | |
| >243 | 75 | 35 | 40 | |
| NLR † | 0.0002 ‡ | |||
| mean 8.1 ± 6.8 | ||||
| range 1.0–47.8 | ||||
| ≤6.2 | 61 | 49 | 12 | |
| >6.2 | 62 | 29 | 33 | |
| LMR † | 0.0523 | |||
| mean 2.2 ± 1.2 | ||||
| range 0.6–7.0 | ||||
| >1.9 | 62 | 45 | 17 | |
| <1.9 | 61 | 33 | 28 | |
| CRP a | 0.0305 ‡ | |||
| mean 52 ± 54 | ||||
| range 0.09–252 | ||||
| ≤5 | 18 | 16 | 2 | |
| >5 | 105 | 62 | 43 | |
| Fibrinogen (mg/dL) a | 0.4444 | |||
| mean 590 ± 193 | ||||
| range 208–1000 | ||||
| ≤3.75 | 13 | 10 | 3 | |
| >3.75 | 110 | 68 | 42 | |
| D-dimer (ng/mL) a | 0.0445 ‡ | |||
| mean 418 ± 528 | ||||
| range 74–4662 | ||||
| ≤260 | 57 | 42 | 15 | |
| >260 | 66 | 36 | 30 | |
| AST (U/L) a | 0.0004 ‡ | |||
| mean 39 ± 42 | ||||
| range 9–356 | ||||
| ≤33 | 78 | 59 | 19 | |
| >33 | 45 | 19 | 26 | |
| ALT (U/L) a | 0.5175 | |||
| mean 46 ± 42 | ||||
| range 3–221 | ||||
| ≤49 | 85 | 56 | 29 | |
| >49 | 38 | 22 | 16 | |
| ALP (U/L) a | 0.7459 | |||
| mean 46 ± 42 | ||||
| range 3–221 | ||||
| ≤49 | 115 | 73 | 42 | |
| >49 | 8 | 5 | 3 | |
| Albumin (g/dL) a | 0.9261 | |||
| mean 3.8 ± 0.4 | ||||
| range 2.7–4.8 | ||||
| ≥3.5 | 103 | 66 | 37 | |
| <3.5 | 20 | 12 | 8 | |
| Variable | Coefficient | Standard Error | p |
|---|---|---|---|
| Age | 0.054682 | 0.024616 | 0.0263 |
| Gender | −1.37100 | 0.62439 | 0.0281 |
| CTSS | 0.14322 | 0.075131 | 0.0566 |
| LDH | 0.0059958 | 0.0034632 | 0.0834 |
| NLR | 0.057745 | 0.054739 | 0.2915 |
| LMR | −0.024549 | 0.24068 | 0.9188 |
| CRP | 0.0088529 | 0.0065703 | 0.1778 |
| Fibrinogen | 0.00084544 | 0.0016936 | 0.6176 |
| D-dimer | 0.00023585 | 0.00054009 | 0.6623 |
| AST | −0.010337 | 0.0096558 | 0.2844 |
| ALT | 0.0051031 | 0.0070821 | 0.4712 |
| ALP | 0.0027839 | 0.0038827 | 0.4734 |
| Albumin | 0.20774 | 0.70751 | 0.7691 |
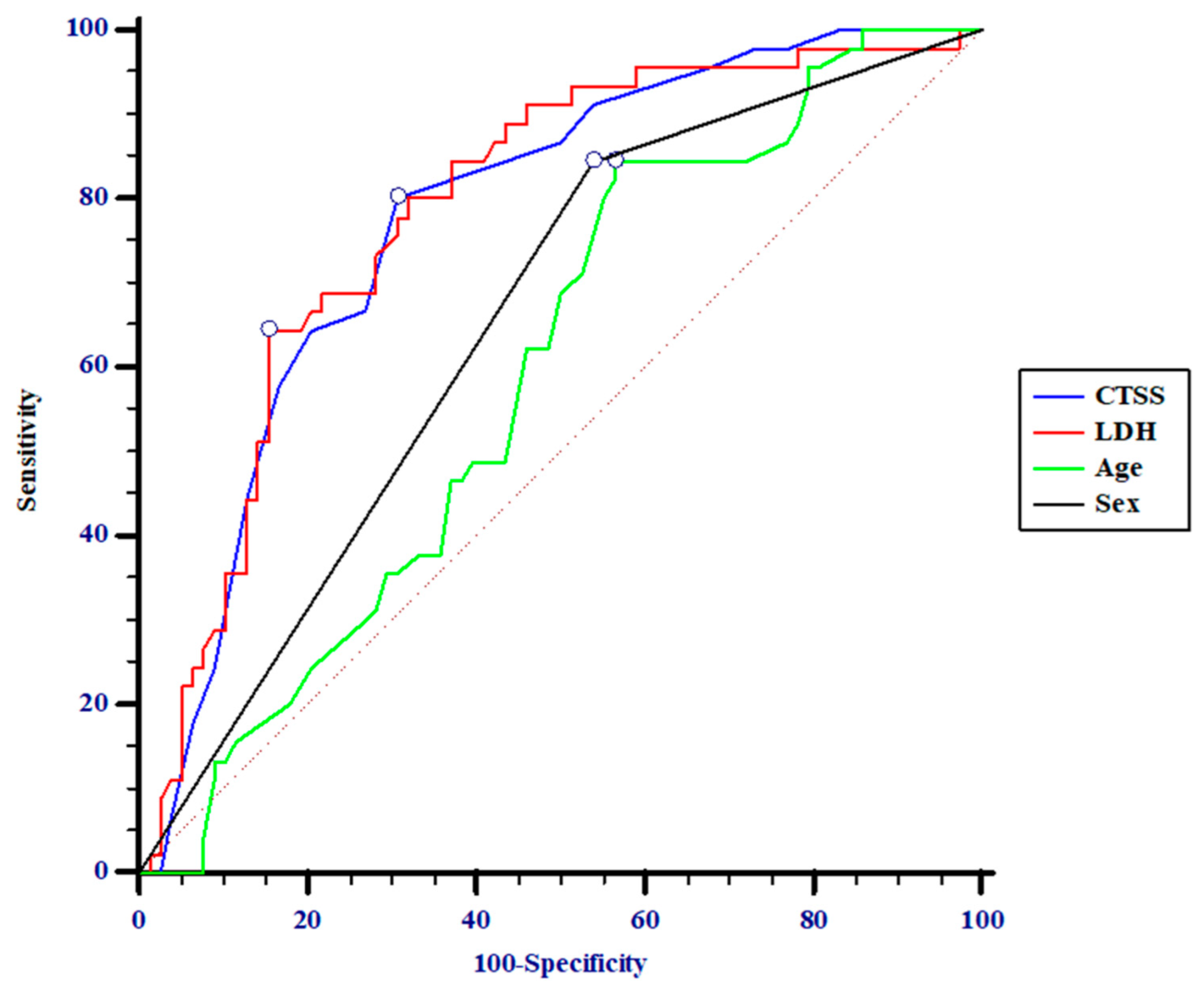
| Variable | AUC | p | Sensitivity % | Specificity % | +PV % | −PV % |
|---|---|---|---|---|---|---|
| Age > 56 years | 0.59 (0.5–0.7) | 0.0678 | 84 (70–93) | 44 (32–55) | 46 (35–58) | 83 (68–93) |
| Male gender | 0.65 (0.6–0.7) | 0.0021 | 84 (70–93) | 46 (35–58) | 47 (36–59) | 84 (69–93) |
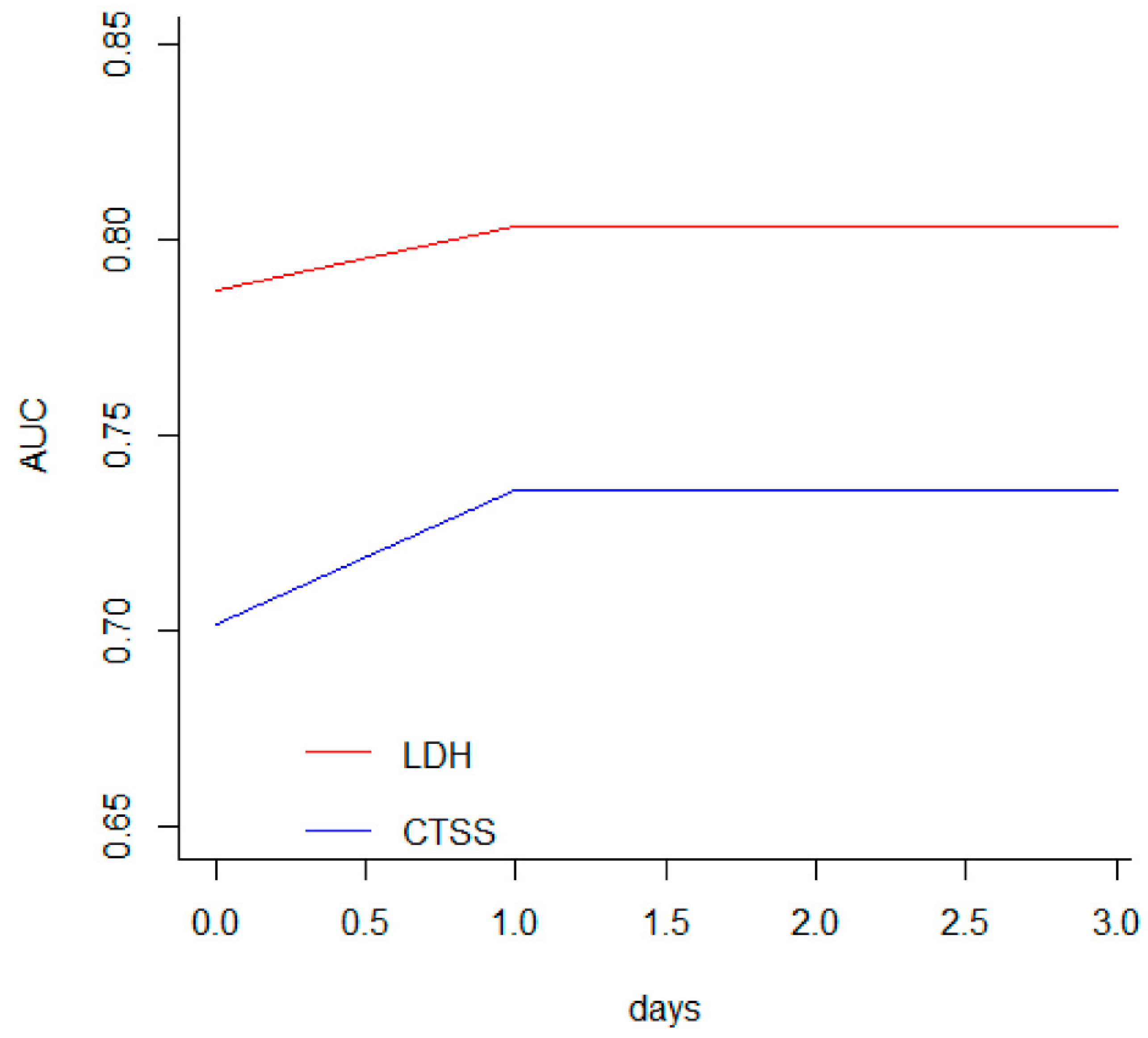
| CTSS > 7 | 0.78 (0.7–0.8) | <0.0001 | 80 (65–90) | 69 (58–79) | 60 (46–72) | 86 (75–93) |
| LDH > 328 U/L | 0.78 (0.7–0.8) | <0.0001 | 64 (49–78) | 84 (75–92) | 71 (54–84) | 81 (70–88) |
| LDH ≤ 328 U/L 82 Patients | LDH > 328 U/L 41 Patients | |
|---|---|---|
| CTSS ≤ 7 63 patients | 55 (5) | 8 (4) |
| CTSS > 7 60 patients | 27 (11) | 33 (25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, C.; Cozzolino, D.; Cuomo, G.; Abitabile, M.; Carusone, C.; Cinone, F.; Nappo, F.; Nevola, R.; Sellitto, A.; Auricchio, A.; et al. Prediction of SARS-CoV-2-Related Lung Inflammation Spreading by V:ERITAS (Vanvitelli Early Recognition of Inflamed Thoracic Areas Spreading). J. Clin. Med. 2022, 11, 2434. https://doi.org/10.3390/jcm11092434
Romano C, Cozzolino D, Cuomo G, Abitabile M, Carusone C, Cinone F, Nappo F, Nevola R, Sellitto A, Auricchio A, et al. Prediction of SARS-CoV-2-Related Lung Inflammation Spreading by V:ERITAS (Vanvitelli Early Recognition of Inflamed Thoracic Areas Spreading). Journal of Clinical Medicine. 2022; 11(9):2434. https://doi.org/10.3390/jcm11092434
Chicago/Turabian StyleRomano, Ciro, Domenico Cozzolino, Giovanna Cuomo, Marianna Abitabile, Caterina Carusone, Francesca Cinone, Francesco Nappo, Riccardo Nevola, Ausilia Sellitto, Annamaria Auricchio, and et al. 2022. "Prediction of SARS-CoV-2-Related Lung Inflammation Spreading by V:ERITAS (Vanvitelli Early Recognition of Inflamed Thoracic Areas Spreading)" Journal of Clinical Medicine 11, no. 9: 2434. https://doi.org/10.3390/jcm11092434