
Practice of Awake Prone Positioning in Critically Ill COVID-19 Patients—Insights from the PRoAcT–COVID Study
 , ,
on behalf of the PRoAcT–COVID Collaborative Group
, ,
on behalf of the PRoAcT–COVID Collaborative Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Collected Data
2.4. Patient Classification
2.5. Endpoints
2.6. Power Calculation
2.7. Statistical Analyses
3. Results
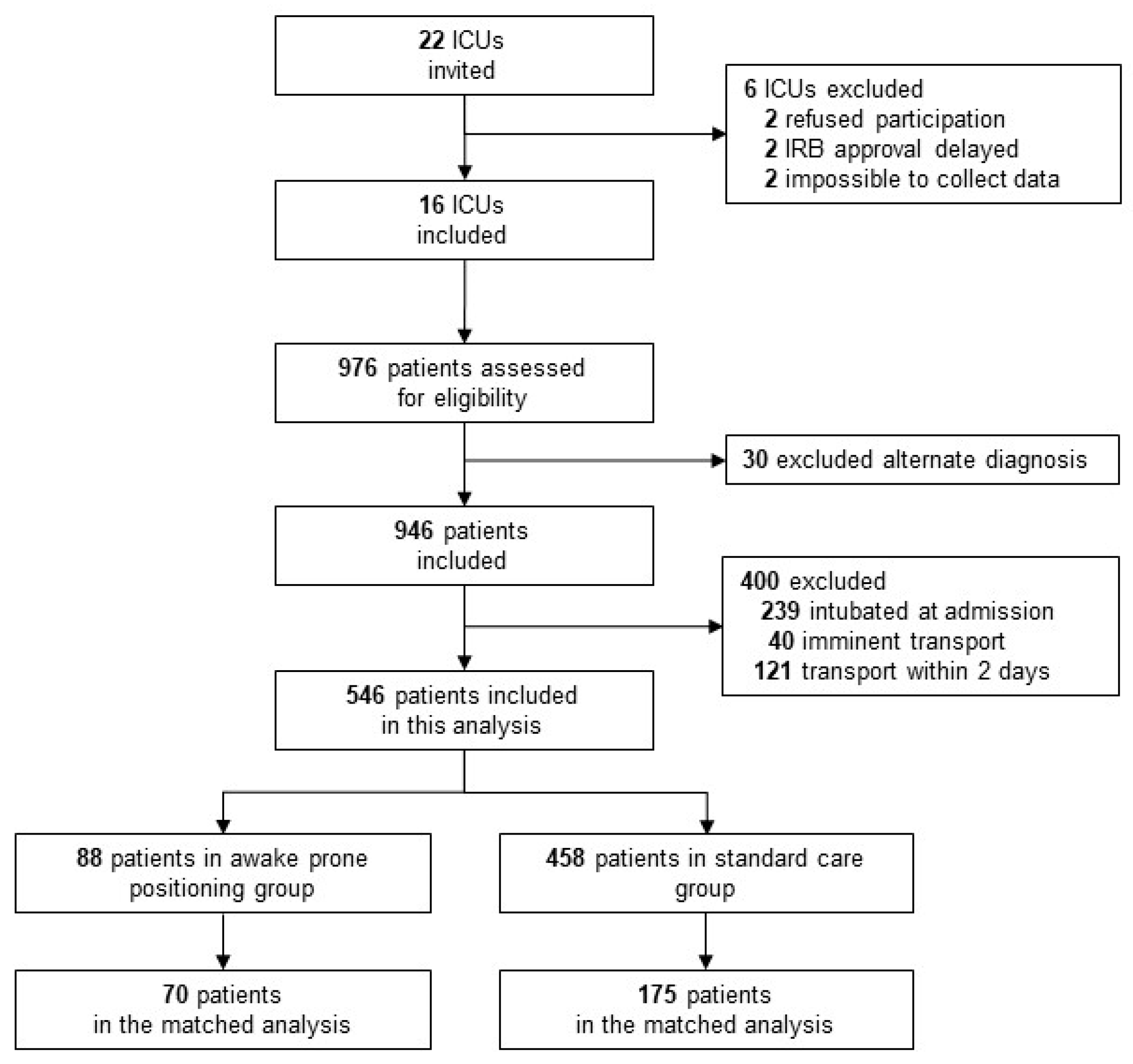
3.1. Patients Enrolled
3.2. Practice of Awake Prone Positioning
3.3. Epidemiology
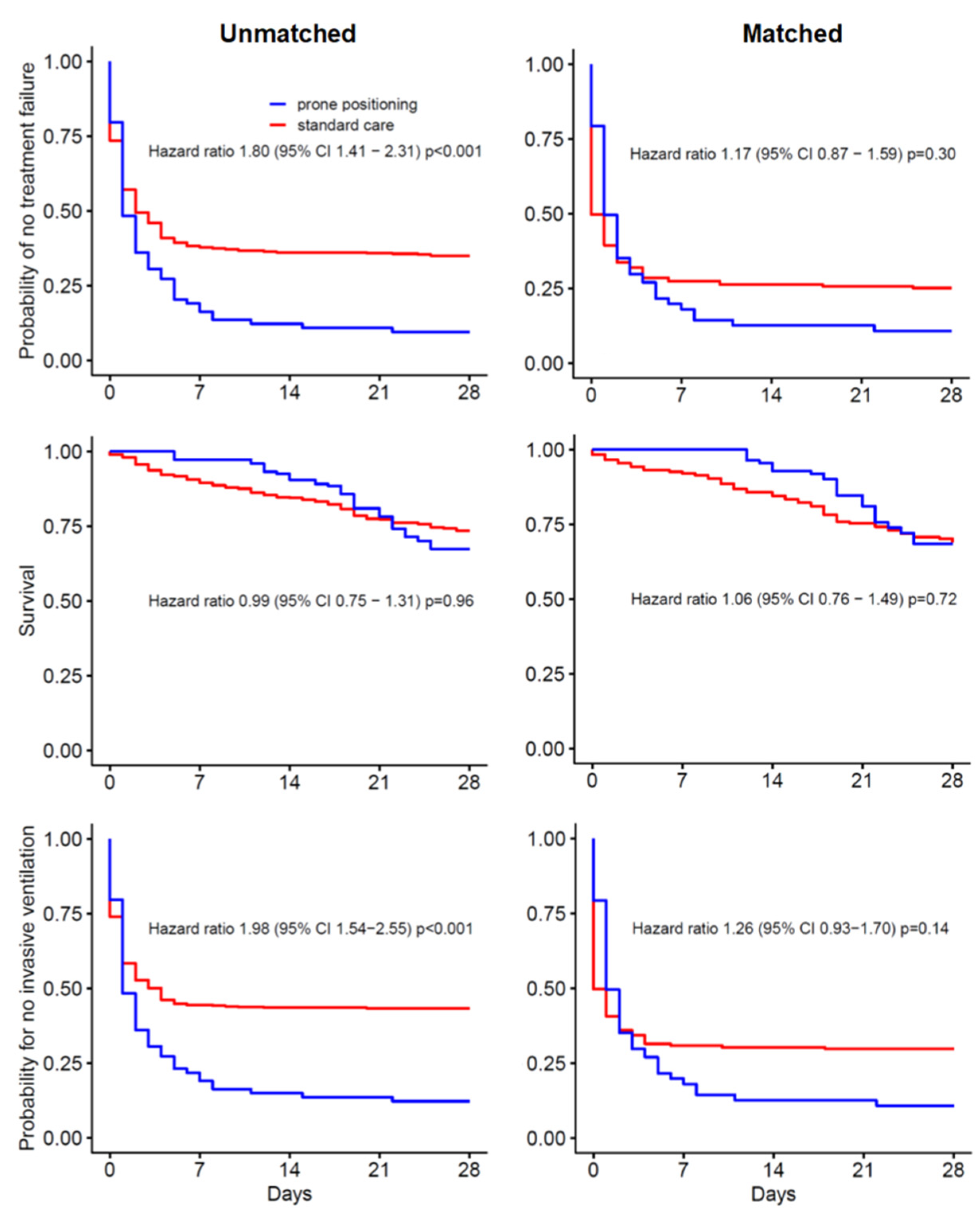
3.4. Treatment Failure
3.5. Other Outcomes
3.6. Propensity Matched Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- COVID-ICU Group on Behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Hadaya, J.; Benharash, P. Prone Positioning for Acute Respiratory Distress Syndrome (ARDS). JAMA 2020, 324, 1361. [Google Scholar] [CrossRef]
- Damarla, M.; Zaeh, S.; Niedermeyer, S.; Merck, S.; Niranjan-Azadi, A.; Broderick, B.; Punjabi, N. Prone Positioning of Nonintubated Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 604–606. [Google Scholar] [CrossRef]
- Esperatti, M.; Busico, M.; Fuentes, N.A.; Gallardo, A.; Osatnik, J.; Vitali, A.; Wasinger, E.G.; Olmos, M.; Quintana, J.; Saavedra, S.N.; et al. Impact of exposure time in awake prone positioning on clinical outcomes of patients with COVID-19-related acute respiratory failure treated with high-flow nasal oxygen: A multicenter cohort study. Crit. Care 2022, 26, 16. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Mellado-Artigas, R.; Gea, A.; Arruti, E.; Aldecoa, C.; Adalia, R.; Ramasco, F.; Monedero, P.; Maseda, E.; Tamayo, G.; et al. Awake prone positioning does not reduce the risk of intubation in COVID-19 treated with high-flow nasal oxygen therapy: A multicenter, adjusted cohort study. Crit. Care 2020, 24, 597. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, S.; Li, J.; Ibarra-Estrada, M.; Perez, Y.; Pavlov, I.; McNicholas, B.; Roca, O.; Mirza, S.; Vines, D.; Garcia-Salcido, R.; et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: A randomised, controlled, multinational, open-label meta-trial. Lancet Respir. Med. 2021, 9, 1387–1395. [Google Scholar] [CrossRef]
- Alhazzani, W.; Parhar, K.K.; Weatherald, J.; Al Duhailib, Z.; Alshahrani, M.; Al-Fares, A.; Buabbas, S.; Cherian, S.V.; Munshi, L.; Fan, E.; et al. Effect of Awake Prone Positioning on Endotracheal Intubation in Patients With COVID-19 and Acute Respiratory Failure: A Randomized Clinical Trial. JAMA 2022, 327, 2104–2113. [Google Scholar] [CrossRef]
- Nasa, P.; Azoulay, E.; Khanna, A.K.; Jain, R.; Gupta, S.; Javeri, Y.; Juneja, D.; Rangappa, P.; Sundararajan, K.; Alhazzani, W.; et al. Expert consensus statements for the management of COVID-19-related acute respiratory failure using a Delphi method. Crit. Care 2021, 25, 106. [Google Scholar] [CrossRef]
- Bamford, P.; Bentley, A.; Dean, J.; Whitmore, D.; Wilson-Baig, N. ICS Guidance for Prone Positioning of the Conscious COVID Patient 2020. Intensive Care Soc. 2020. Available online: https://emcrit.org/wp-content/uploads/2020/04/2020-04-12-Guidance-for-conscious-proning.pdf (accessed on 1 March 2022).
- Stilma, W.; Åkerman, E.; Artigas, A.; Bentley, A.; Bos, L.D.; Bosman, T.J.C.; de Bruin, H.; Brummaier, T.; Buiteman-Kruizinga, L.A.; Carcò, F.; et al. Awake Proning as an Adjunctive Therapy for Refractory Hypoxemia in Non-Intubated Patients with COVID-19 Acute Respiratory Failure: Guidance from an International Group of Healthcare Workers. Am. J. Trop. Med. Hyg. 2021, 104, 1676–1686. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, Y.; Li, Y.; Song, C.; Lin, F.; Pan, P. The Application of Awake-Prone Positioning Among Non-intubated Patients With COVID-19-Related ARDS: A Narrative Review. Front. Med. 2022, 9, 817689. [Google Scholar] [CrossRef] [PubMed]
- Valk, C.M.; Swart, P.; Boers, L.S.; Botta, M.; Bos, L.D.; de Abreu, M.G.; Hol, L.; Hollmann, M.W.; Horn, J.; Martin-Loeches, I.; et al. Practice of adjunctive treatments in critically ill COVID-19 patients-rational for the multicenter observational PRoAcT-COVID study in The Netherlands. Ann. Transl. Med. 2021, 9, 813. [Google Scholar] [CrossRef] [PubMed]
- PRoAcT COVID study—Awake Prone Positioning—Statistical Analysis. Available online: https://sites.google.com/view/proact-covid/awake-prone-positioning (accessed on 1 March 2022).
- Kądziołka, I.; Świstek, R.; Borowska, K.; Tyszecki, P.; Serednicki, W. Validation of APACHE II and SAPS II scales at the intensive care unit along with assessment of SOFA scale at the admission as an isolated risk of death predictor. Anaesthesiol. Intensiv. Ther. 2019, 51, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Lu, B. Propensity Score Matching with Time-Dependent Covariates. Biometrics 2005, 61, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.P.; Subramaniam, A.; Chua, C.; Ling, R.R.; Anstey, C.; Ramanathan, K.; Slutsky, A.S.; Shekar, K. Respiratory system mechanics, gas exchange, and outcomes in mechanically ventilated patients with COVID-19-related acute respiratory distress syndrome: A systematic review and meta-analysis. Lancet Respir. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Luo, J.; Pavlov, I.; Perez, Y.; Tan, W.; Roca, O.; Tavernier, E.; Kharat, A.; McNicholas, B.; Ibarra-Estrada, M.; et al. Awake prone positioning for non-intubated patients with COVID-19-related acute hypoxaemic respiratory failure: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 573–583. [Google Scholar] [CrossRef]
- Perez-Nieto, O.R.; Escarraman-Martinez, D.; Guerrero-Gutierrez, M.A.; Zamarron-Lopez, E.I.; Mancilla-Galindo, J.; Kammar-García, A.; Martinez-Camacho, M.A.; Deloya-Tomás, E.; Sanchez-Díaz, J.S.; Macías-García, L.A.; et al. Awake prone positioning and oxygen therapy in patients with COVID-19: The APRONOX study. Eur. Respir. J. 2021, 59, 2100265. [Google Scholar] [CrossRef] [PubMed]
- Fazzini, B.; Page, A.; Pearse, R.; Puthucheary, Z. Prone positioning for non-intubated spontaneously breathing patients with acute hypoxaemic respiratory failure: A systematic review and meta-analysis. Br. J. Anaesth. 2021, 128, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Qian, E.T.; Gatto, C.L.; Amusina, O.; Dear, M.L.; Hiser, W.; Buie, R.; Kripalani, S.; Harrell, F.E.; Freundlich, R.E.; Gao, Y.; et al. Assessment of Awake Prone Positioning in Hospitalized Adults With COVID-19: A Nonrandomized Controlled Trial. JAMA Intern. Med. 2022, 182, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Nieto, O.R.; Gutierrez, M.A.G.; Deloya-Tomas, E.; Ñamendys-Silva, S.A. Prone positioning combined with high-flow nasal cannula in severe noninfectious ARDS. Crit. Care 2020, 24, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The REMAP-CAP Investigators; The ACTIV-4a Investigators; The ATTACC Investigators. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef] [PubMed]
- The ATTACC, ACTIV-4a; REMAP-CAP Investigators. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Morales-Quinteros, L.; Schultz, M.J.; Serpa-Neto, A.; Antonelli, M.; Grieco, D.L.; Roca, O.; Juffermans, N.P.; de Haro, C.; de Mendoza, D.; Blanch, L.; et al. Awake prone positioning in nonintubated spontaneous breathing ICU patients with acute hypoxemic respiratory failure (PRONELIFE)-protocol for a randomized clinical trial. Trials 2022, 23, 30. [Google Scholar] [CrossRef] [PubMed]
- Botta, M.; Tsonas, A.M.; Pillay, J.; Boers, L.S.; Algera, A.G.; Bos, L.D.; Dongelmans, D.A.; Hollmann, M.W.; Horn, J.; Vlaar, A.P.; et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): A national, multicentre, observational cohort study. Lancet Respir. Med. 2021, 9, 139–148. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall N = 546 | Prone Positioning N = 88 | Standard Care N = 458 | p | |
|---|---|---|---|---|
| Age, years (median, IQR) | 67 (59–73) | 66 (60–73) | 67 (59–73) | 0.946 |
| Male gender, N (%) | 402 (73.6) | 60 (68.2) | 342 (74.7) | 0.257 |
| BMI, kg/m2 (median, IQR) | 28.0 (25.3–31.8) | 28.8 (25.7–31.9) | 27.9 (25.2–31.8) | 0.543 |
| SAPS II score (median, IQR) | 43 (33–53) | 47 (37–53) | 43 (32–53) | 0.056 |
| Do-not-intubate order, N (%) | 31 (5.7) | 2 (2.3) | 29 (6.3) | 0.209 |
| Comorbidities | ||||
| Arterial hypertension, N (%) | 219 (40.1) | 39 (44.3) | 180 (39.3) | 0.447 |
| Cardiovascular disease, N (%) | 135 (24.7) | 14 (15.9) | 121 (26.4) | 0.050 |
| Heart failure, N (%) | 30 (5.5) | 2 (2.3) | 28 (6.1) | 0.233 |
| COPD or asthma, N (%) | 97 (17.8) | 16 (18.2) | 81 (17.7) | 1.000 |
| Diabetes mellitus, N (%) | 178 (32.6) | 24 (27.3) | 154 (33.6) | 0.298 |
| Chronic kidney disease, N (%) | 50 (9.2) | 7 (8.0) | 43 (9.4) | 0.822 |
| Malignancy, N (%) | 39 (7.1) | 6 (6.8) | 33 (7.2) | 1.000 |
| Neuromuscular disease, N (%) | 13 (2.4) | 2 (2.3) | 11 (2.4) | 1.000 |
| Obstructive sleep apnea, N (%) | 39 (7.1) | 6 (6.8) | 33 (7.2) | 1.000 |
| Days in hospital before ICU admission, (median, IQR) | 1.0 (0.0–4.0) | 2.0 9 (0.0–3.0) | 1.0 (0.0–4.0) | 0.085 |
| Prone Positioning N = 88 | |
|---|---|
| HFNO, N (%) | 70 (79.5) |
| FiO2, % (median, IQR) | 82 (65–95) |
| Air flow, L/min (median, IQR) | 60 (50–60) |
| CPAP, N (%) | 8 (9.1) |
| FiO2, % (median, IQR) | 67.5 (63.8–93.3) |
| Non-Rebreather or Venturi Mask, N (%) | 5 (5.7) |
| Oxygen, L (median, IQR) | 15.0 (15.0–15.0) |
| NIV, N (%) | 4 (4.5) |
| PEEP, cmH2O (median, IQR) | 8.0 (7.3–9.3) |
| FiO2, % (median, IQR) | 72.5 (57.5–86.3) |
| SpO2, % (median, IQR) | 91.3 (89.0–94.0) |
| PaO2, mmHg (median, IQR) | 72.0 (60.0–84.5) |
| Overall N = 478 | Prone Positioning N = 88 | Standard Care * N = 390 | p-Value | |
|---|---|---|---|---|
| Oxygen support ** | ||||
| Not known | 3 (0.6) | 0 (0.0) | 3 (0.8) | |
| Nasal sprong, N (%) | 24 (5.0) | 1 (1.1) | 23 (5.9) | |
| Oxygen, L (median, IQR) | 4 (3–5) | 5 (5–5) | 4 (3–5) | 0.376 |
| Non-Rebreather or Venturi Mask, N (%) | 60 (12.6) | 9 (10.2) | 51 (13.1) | |
| Oxygen, L (median, IQR) | 15 (12–15) | 15 (15–15) | 15 (12–15) | 0.038 |
| High Flow Nasal Oxygen (HFNO), N (%) | 372 (77.8) | 73 (83.0) | 299 (76.7) | |
| FiO2, % (median, IQR) | 80 (60–90) | 80 (60–94) | 75 (60–90) | 0.161 |
| Flow, Liters oxygen/min (median, IQR) | 50 (50–60) | 50 (50–60) | 50 (50–60) | 0.057 |
| Non-invasive ventilation (NIV), N (%) | 13 (2.7) | 2 (2.3) | 11 (2.8) | |
| PEEP, cmH2O (median, IQR) | 6 (5–8) | 9 (7–11) | 6 (5–8) | 0.688 |
| FiO2, % (median, IQR) | 50 (40–60) | 55 (52.5–57.5) | 50 (40–65) | 0.481 |
| Missing data, N (%) | 6 (0.01) | 3 (3.4) | 3 (0.7) | |
| Respiratory values *** | ||||
| SpO2, % (median, IQR) | 93 (90–95) | 91 (89–94) | 93 (90–96) | <0.001 |
| PaO2, mmHg (median, IQR) | 76 (25–87) | 73 (61–83) | 77 (19–88) | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stilma, W.; Valk, C.M.A.; van Meenen, D.M.P.; Morales, L.; Remmelzwaal, D.; Myatra, S.N.; Artigas, A.; Neto, A.S.; Paulus, F.; Schultz, M.J., on behalf of the PRoAcT–COVID Collaborative Group. Practice of Awake Prone Positioning in Critically Ill COVID-19 Patients—Insights from the PRoAcT–COVID Study. J. Clin. Med. 2022, 11, 6988. https://doi.org/10.3390/jcm11236988
Stilma W, Valk CMA, van Meenen DMP, Morales L, Remmelzwaal D, Myatra SN, Artigas A, Neto AS, Paulus F, Schultz MJ on behalf of the PRoAcT–COVID Collaborative Group. Practice of Awake Prone Positioning in Critically Ill COVID-19 Patients—Insights from the PRoAcT–COVID Study. Journal of Clinical Medicine. 2022; 11(23):6988. https://doi.org/10.3390/jcm11236988
Chicago/Turabian StyleStilma, Willemke, Christel M. A. Valk, David M. P. van Meenen, Luis Morales, Daantje Remmelzwaal, Sheila N. Myatra, Antonio Artigas, Ary Serpa Neto, Frederique Paulus, and Marcus J. Schultz on behalf of the PRoAcT–COVID Collaborative Group. 2022. "Practice of Awake Prone Positioning in Critically Ill COVID-19 Patients—Insights from the PRoAcT–COVID Study" Journal of Clinical Medicine 11, no. 23: 6988. https://doi.org/10.3390/jcm11236988