Article Text

Abstract
During the first wave of the coronavirus pandemic, the UK government took the decision to centralise the procurement, allocation and distribution of mission-critical intensive care unit (ICU) medical equipment. Establishing new supply chains in the context of global shortages presented significant challenges. This report describes the development of an innovative platform developed rapidly and voluntarily by clinical engineers, to mobilise the UK’s shared medical equipment inventory, in order to match ICU capacity to dynamically evolving clinical demand. The ‘Coronavirus ICU Medical Equipment Distribution’ platform was developed to optimise ICU equipment allocation, distribution, collection, redeployment and traceability across the National Health Service. Although feedback on the platform has largely been very positive, the platform was built for a scenario that did not fully materialise in the UK and this affected the implementation approach. As such, it was not used to its full potential. Nonetheless, the platform and the insights derived and disseminated in its development have been extremely valuable. It provides a prototype for not only optimising system capacity in future pandemic scenarios but also a means for maximally exploiting the large amount of new equipment in the UK health system, as a result of the coronavirus pandemic. This early stage innovation has demonstrated that a system-wide pooled information resource can benefit the operations of individual organisations. It has also generated numerous lessons to be borne in mind in innovation projects.
- equipment and supplies
- COVID-19
- critical care
Data availability statement
Data may be obtained from a third party and are not publicly available
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Background
During the Coronavirus pandemic’s first wave, there was a need to rapidly expand the critical care capacity of the National Health Service (NHS). The UK government had taken the early decision to centralise the procurement, allocation and distribution of mission-critical intensive care unit (ICU) medical equipment to meet this challenge.1 This system-level approach had the potential advantage of leveraging economies of scale in procurement, instead of local market forces determining outcomes. However, rapidly establishing new supply chains in the context of global shortages presented significant challenges.
Clinical engineers are key specialists whose remit includes ‘developing, managing, assessing, installing and maintaining (health) technologies for their safe and cost-effective use’.2 National and regional networks of clinical engineers formed in the early phase of the UK’s pandemic response with the support of NHS England. These networks created communication channels between NHS clinical engineers and the central national teams, procuring and allocating ICU equipment—and they facilitated numerous initiatives.3 As clinical demand fluctuated across the UK, the network escalated the need for responsive and efficient allocation and redistribution of equipment. This would mean overcoming integration and communication challenges, to enable robust and effective ICU capacity where it was needed most.
Here we describe an innovative platform developed rapidly and voluntarily by clinical engineers, to mobilise the UK’s shared medical equipment inventory, in order to match ICU capacity to dynamically evolving clinical demand. It involved ICU equipment allocation, distribution, collection, redeployment and traceability across the NHS.
Objectives
The team hoped to address several challenges:
Provide early sight of incoming unfamiliar equipment models to clinical engineering teams.
Allow organisations to express preference for equipment models: under normal circumstances, and especially when clinical staff are newly trained and stressed, standardised inventory is safety critical4 5—these communications enable this.
Signal demand: allowing organisations to communicate their current and forecasted shortfall, on the basis of local arrangements.
Enable optimal allocation: incorporating the above into decision-support for allocators.
Assure efficiency and robustness: in equipment receipt and deployment6 ; cutting out costly delays by engaging the correct stakeholders in each organisation.
Enable transfers between organisations: enabling direct-‘swapping’ between organisations to achieve standardisation.
Improve traceability of centrally owned equipment assets
Methods
Early in the pandemic, the designers recognised the need for centralised equipment distribution teams to be able to offer equipment to healthcare providers and for healthcare providers to be able to accept or reject offers based on local need. The Coronavirus ICU Medical Equipment Distribution (CIMED) platform was conceived to address this.
The CIMED platform requirements (in the form of ‘user stories’7) were captured from key stakeholders including regional and national equipment distributors, NHS Trust Clinical Engineering leads and logistics providers. The final list of requirements was related to redistribution and return of equipment and the need for nationwide traceability.
Initially the designers envisaged a database with web interfaces for equipment distributors and for hospital-based equipment management staff. The distributors’ interface would allow them to offer equipment to hospitals, which they could then accept or reject using their own interface. Existing products were surveyed, but no suitable option was identified. A commercial web developer was approached with the concept; however, the offered development timeframe was prohibitive. The designers, therefore, opted to develop their own solution.
To minimise development time, the designers used a pre-existing web-based office suite (Google docs) as a development platform. This suite includes spreadsheet software (used for data storage and the user interface), an email client (used to send notifications to users and to the logistics provider) and a scripting platform (used to create workflows and relational database functionality).
In the absence of upfront resourcing, this was a voluntary effort with no guaranteed buy-in.
Results
What was delivered?
A system of interconnected tables was created (see figure 1). These were used for capture, storage, transfer and reporting of data relevant to equipment allocation and distribution. Workflows were email driven.
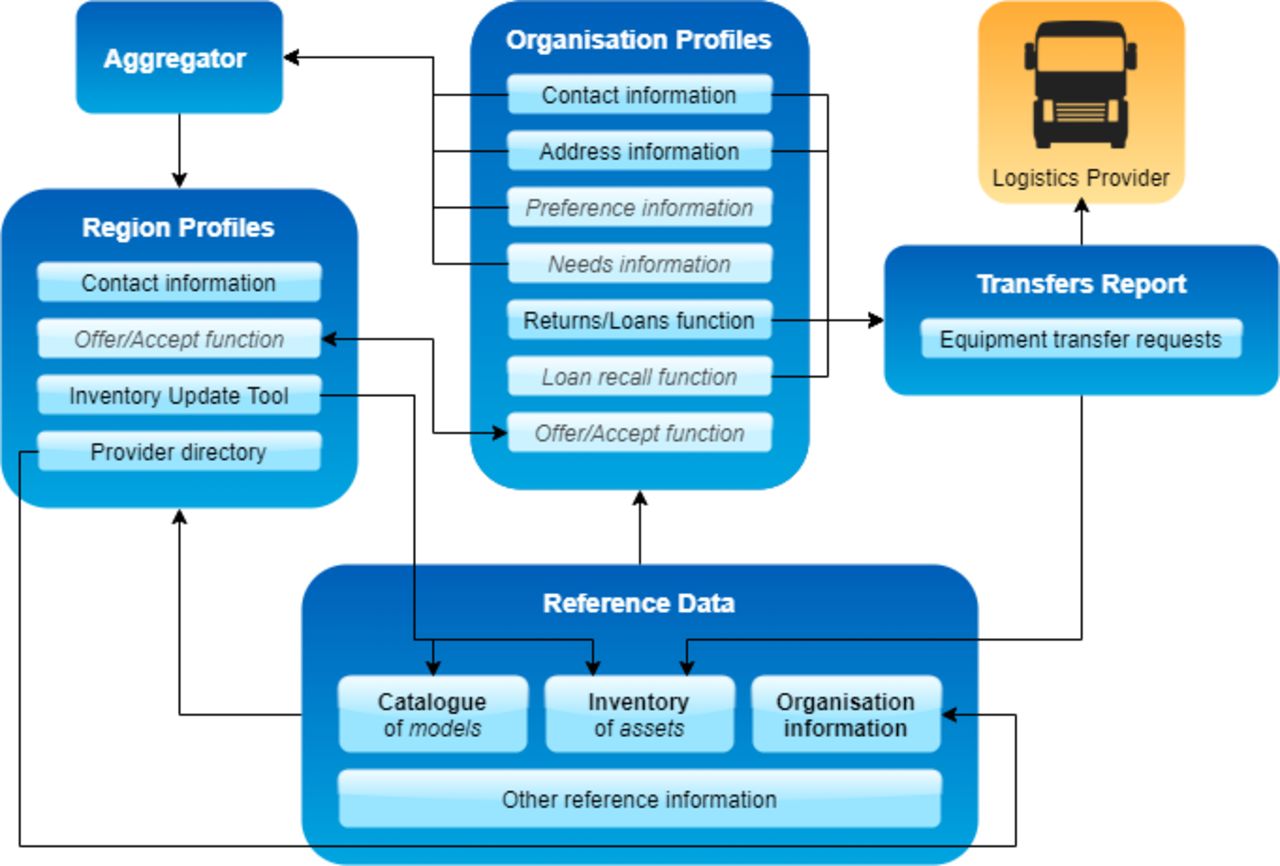
Schematic of the Coronavirus ICU Medical Equipment Distribution (CIMED) platform.
The system included a reference data set that held a complete inventory of all centrally procured equipment, including location information, together with contact and delivery details for every acute healthcare provider in the UK.
‘Region profiles’ were created to allow regional equipment allocators to view a complete list of the providers in their region, a list of all the equipment available for allocation. They would have the ability to allocate equipment efficiently (more so, using optimisation-driven decision support) and to offer equipment to individual providers with a few mouse clicks, instead of via time-consuming phone and email conversations.
‘Organisation profiles’ were created for all healthcare providers. Identifying the relevant contacts was a significant challenge. Users within these organisations could use their profile to enter contact and delivery details, together with information about local equipment needs and preferences. The profiles contained a list of equipment located with that provider, drawn from the reference data set. Users could arrange equipment return to central loan stock and accept or reject equipment offers from regional allocators with a few mouse clicks. The profile also gave users early sight of the models available for allocation with a complete list of all models available within the system.
A ‘transfer report’, viewable by the national logistics provider, contained summary information about all equipment deliveries and collections arranged using CIMED. This information was sent by email every time a delivery or collection was requested by any user of the system. Barcode-scannable collection slips with equipment decontamination prompts and declarations were generated and emailed out.
How was it used?
CIMED was used by the national logistics provider. A relatively small number of healthcare providers used the system directly to return superfluous equipment and to reconcile central inventory records with their local inventory data. Others used a more manual process, which was partly defined by the CIMED team.
Discussion
Performance
CIMED worked and has been used; feedback has been very positive. The platform was robust and stable with users reporting no problems related to its core functionality. Users at some institutions had difficulty accessing the platform due to local firewall settings—however most engineers were able to resolve this. Two users commented that some elements of the system were slow to update and respond. The designers agree that these are important limitations.
These limitations could be overcome by changing the system architecture. This would require use of a custom web application and SQL database. This option had been rejected in the early stages due to the development time required. With hindsight, given the limitations of the office suite and the functionality required in the finished product, development of a custom web application may have been preferable. However, this could not have been foreseen with the information available at the beginning of the project.
CIMED relied on equipment location data gathered from central equipment distributors. This data had been recorded in different ways and to varying quality standards. The majority of queries from health organisations that adopted CIMED were concerning errors in this underlying data. Correction of these errors required direct user engagement, which was labour intensive although curating the inventory data were an unexpected benefit of the system.
Extent of system-wide adoption
Central distributors initially saw CIMED as a platform for coordinating return of medical equipment from healthcare providers to central loan stock. Contacts at over 100 healthcare organisations were given access to CIMED. Eighty-two transfers were issued via CIMED directly in the first wave. Many opted to use the manual equivalent, which used CIMED templates for email-based transfer requests to be handled by a dedicated central team.
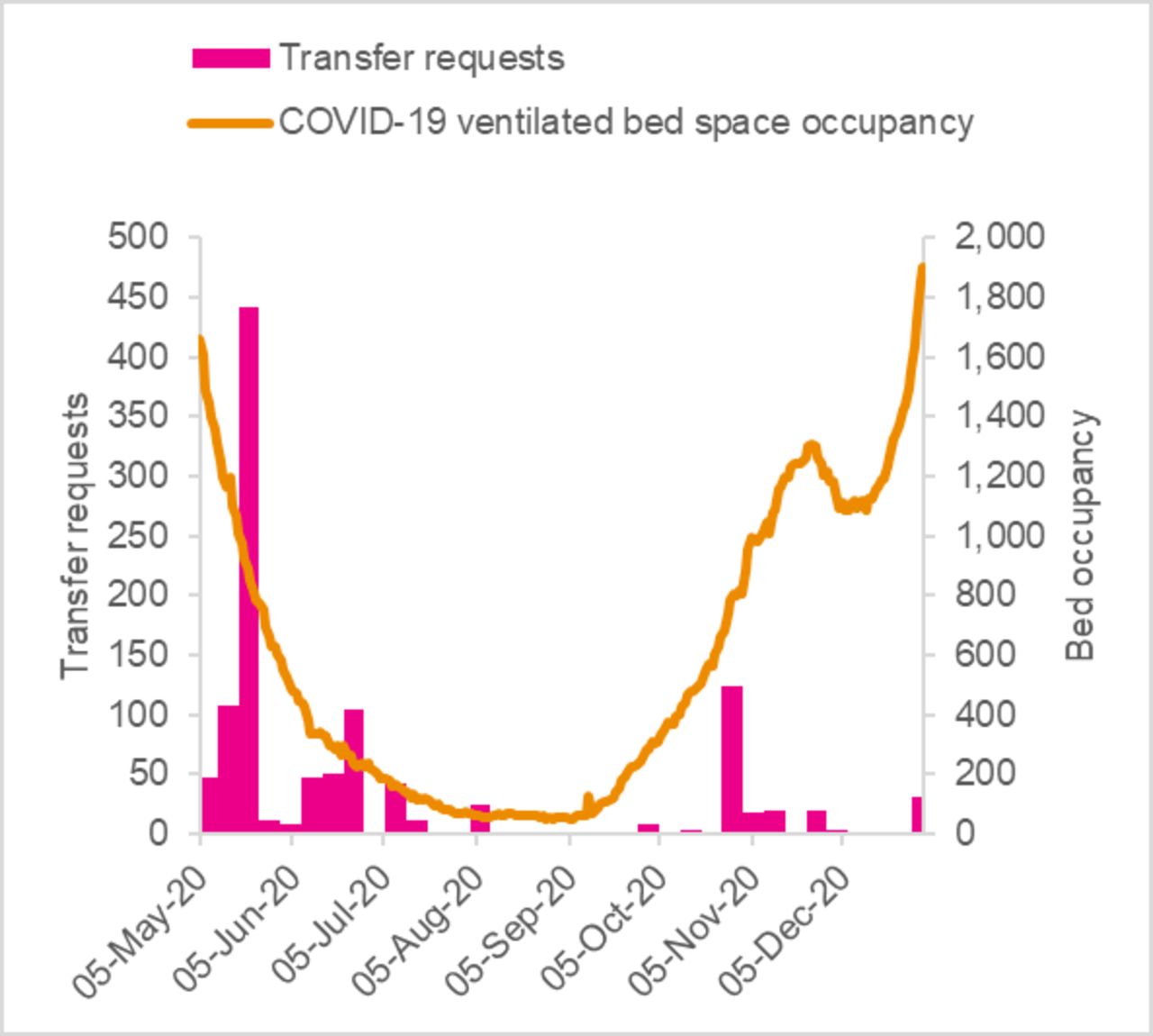
The user access mechanism was a significant limitation. Users were issued personal links, rather than using more familiar, navigate-to and login processes. In the period between the first and second waves, most organisations naturally continued to hold equipment. This was a natural response to uncertainty, while system-wide plans for scaling up ICU capacity were being clarified. Similar behaviour is observed in local ‘medical equipment library’ services.8 As a result, the traffic of medical equipment transfers as a whole, corresponded to increases in ICU activity as illustrated in figure 2. As each user engaged with the platform intermittently, retrieving/recalling their personal link proved harder than initiating the manual process for transfer requests.

{kind=link}
{kind=link}
Number of device transfers requested, by month, vs UK pandemic caseload.
Extent of adoption by central decision-makers
While CIMED became a tool for mobilising national ICU equipment capacity via a returns process, features that would facilitate the (re)allocation of equipment and interorganisational transfers were not adopted. This platform was developed voluntarily by one particular service rather than being centrally commissioned. Hence, the team simultaneously built and promoted the solution. In an unfamiliar, highly sensitive environment, with sporadic demand levels, reluctance from would-be adopters was understandable. Although feedback was positive, the required promotion alongside supporting local pandemic commitments exceeded our capacity as volunteers.
Conclusions
Impact
CIMED had limited direct impact, as it was built for a scenario that did not fully materialise in the UK. Its development, however, drove engagement between operational teams and decision-makers, informing various other logistic processes in the pandemic.
Key lessons
The CIMED platform shows that a system-wide pooled information resource can benefit the operations of individual organisations. Philanthropic efforts can rapidly develop innovative solutions, but rapid adoption is complex and should not be underestimated when planning. Clinical engineers and other professional groups can play an important role.
Managing expectations
At the outset, the risk of nonadoption was fully understood by the development team. Partial adoption and limited use, while disappointing crucially represented part of the nation’s pandemic readiness. It was important to reflect on and appreciate this, to motivate an already-stretched workforce.
Further work
CIMED can yet be useful, and the redistribution process it supports is vital for the resettling of services in-between periods of high intensive care demand. Similarly the system remains available for the scenario of scarce devices and mismatch of supply and demand for ICU medical equipment. In a period of low activity, the London regional Clinical Engineering Network identified that CIMED could allow different providers to exchange heterogeneous medical equipment inventories in a mutually supported movement towards standardisation.
The ambition to build regional partnerships to support healthcare delivery is at the forefront of the NHS long-term plan. The learning from this model of pan-organisational medical equipment asset management could inform the emerging integrated care systems structure within the NHS. Equipment services on a larger population footprint could improve economies of scale for purchasing, training and maintenance. It could also achieve better capture of data around inequalities in provision and safety and improve standardisation of equipment assets to best serve regional communities and organisations. The team is open to discussions on partnerships for reimplementing CIMED using a different architecture, for future pandemics or general use. More broadly, these experiences will inform subsequent efforts to explore, understand and improve technology adoption processes, for the benefit of patients and the public.9
Data availability statement
Data may be obtained from a third party and are not publicly available
Acknowledgments
The authors would like to thank Ruth Thomsen—Regional Scientific Director, NHSE&I Medical Directorate. She and her team supported and informed the development of this platform. They were instrumental in gathering and engaging its users across the UK. The authors would also like to thank Professor Steve Keevil, Head of the Medical Physics Department, Guy’s & St Thomas’ NHS Foundation Trust, who recognised the need to support the wider system during the pandemic.
Footnotes
Contributors EAA initiated the development. DS and EAA jointly developed the platform with support from NP and CS-A, and with DS leading on the implementation. CS-A facilitated the dissemination of the platform. All authors contributed to the final version of this paper. EAA is primarily responsible for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.