
The Rapid Implementation of Ad Hoc Tele-Critical Care Respiratory Therapy (eRT) Service in the Wake of the COVID-19 Surge

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Emergence of eRT Services
2.2. Workflow
2.3. Data Collection
2.4. Statistical Analysis
3. Results
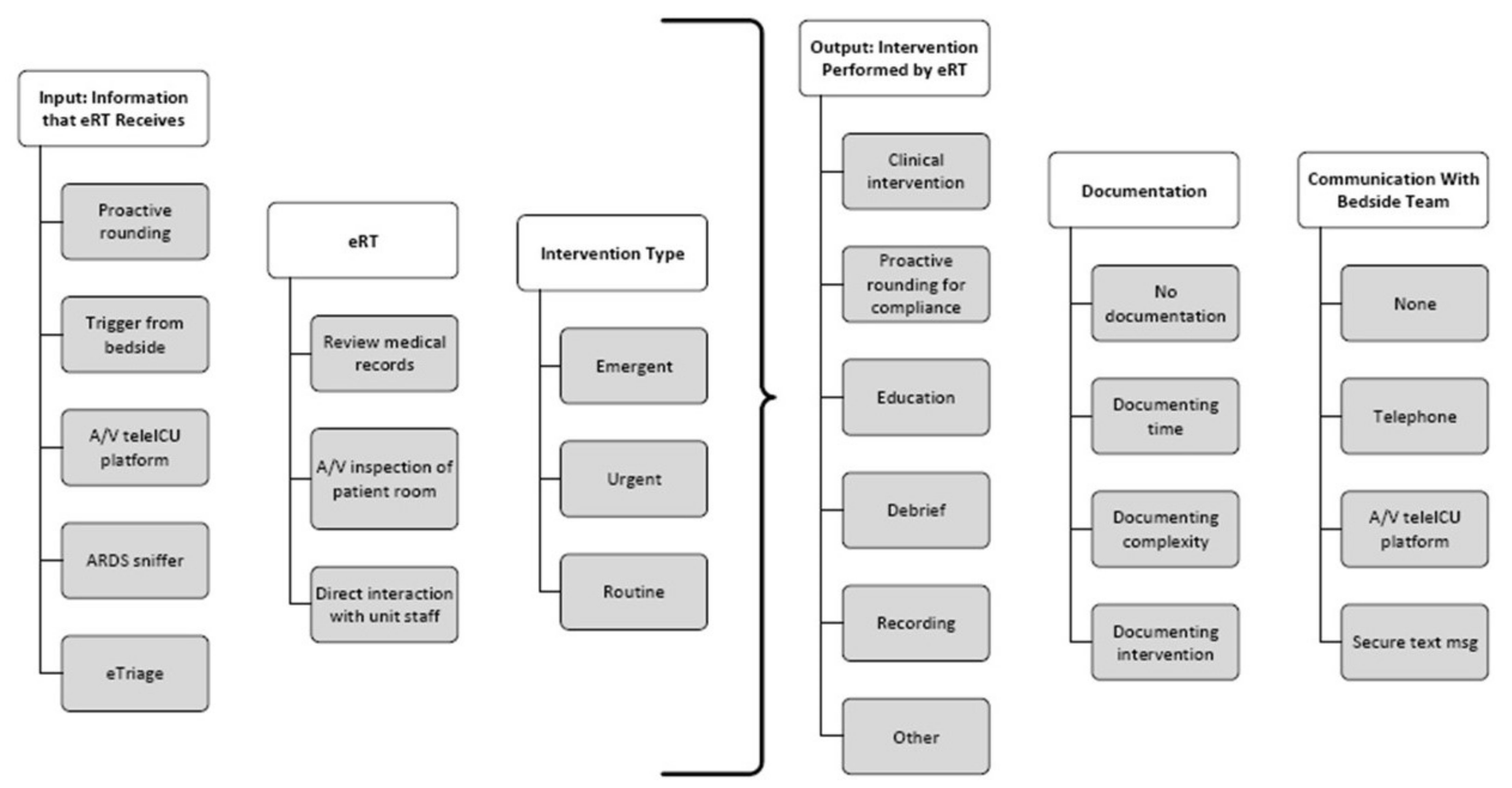
3.1. eRT Service Healthcare Delivery Model
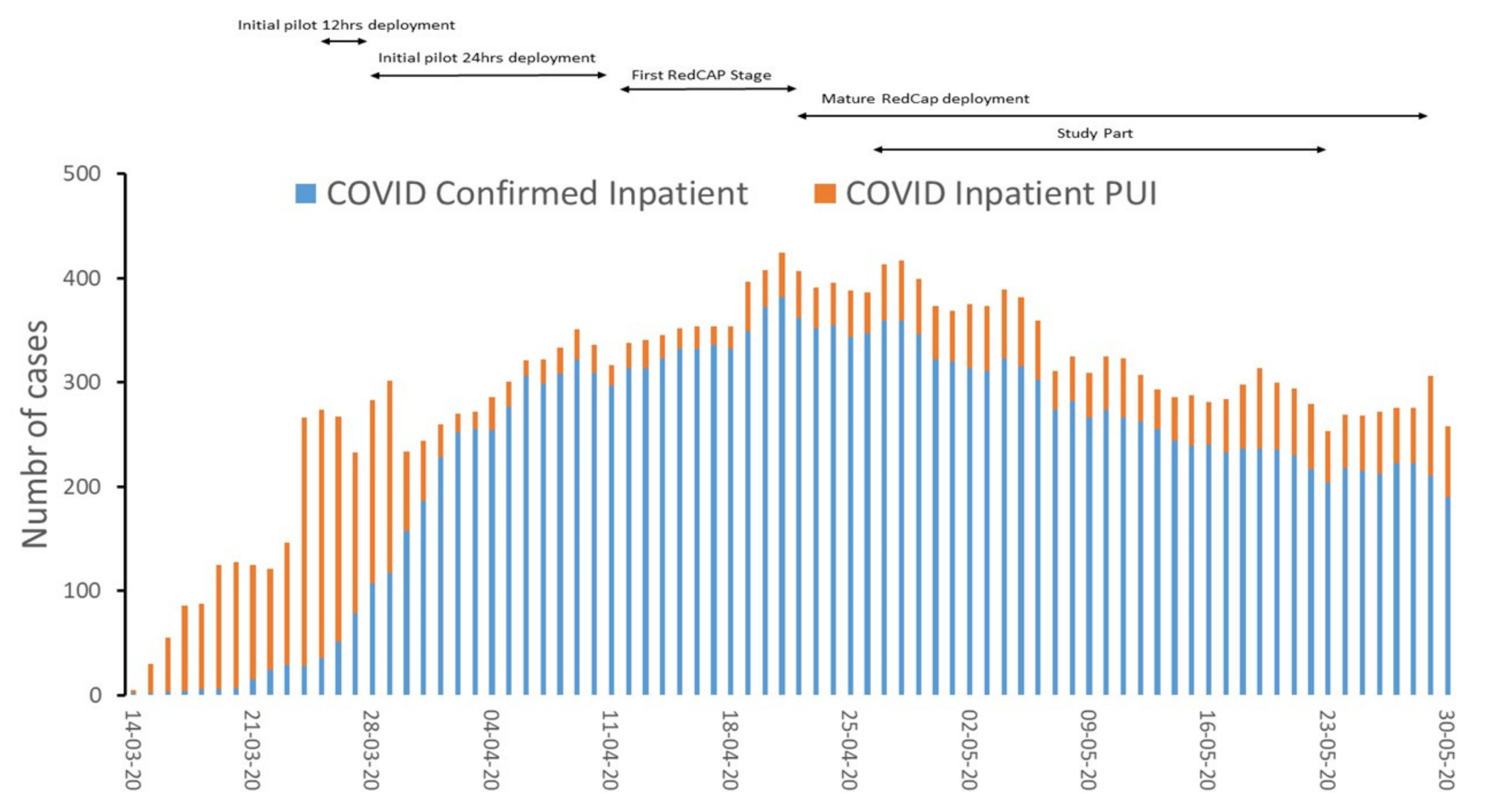
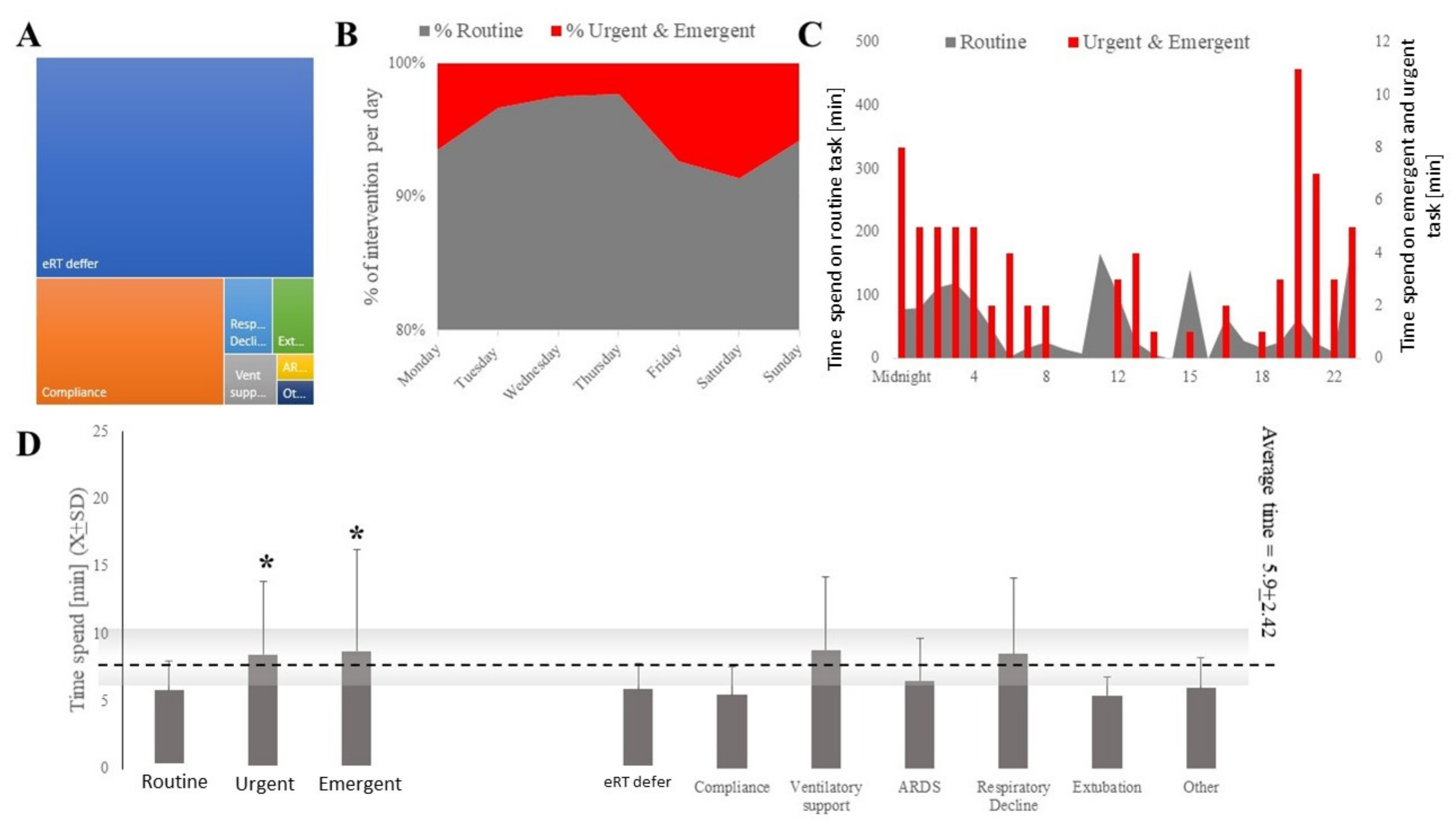
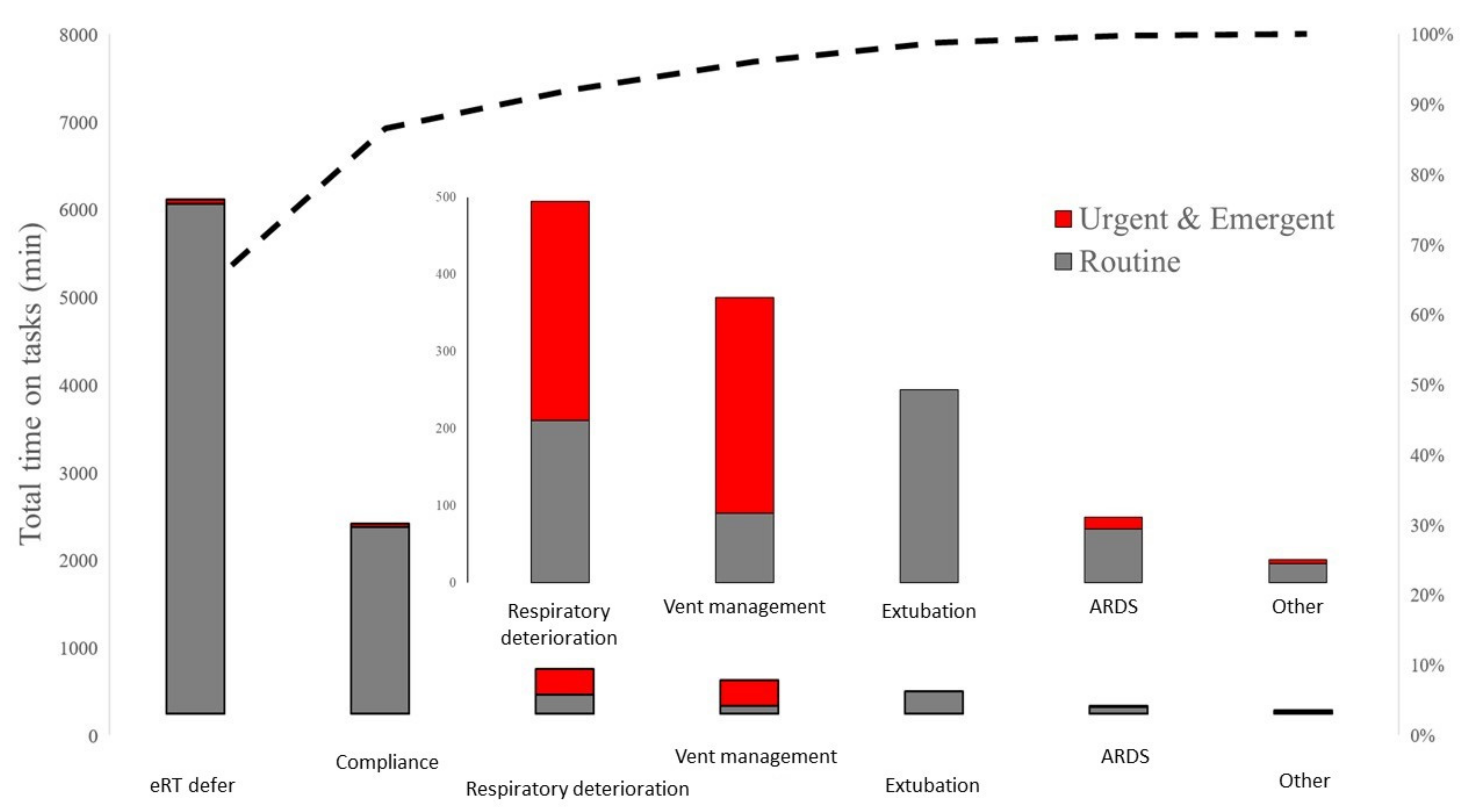
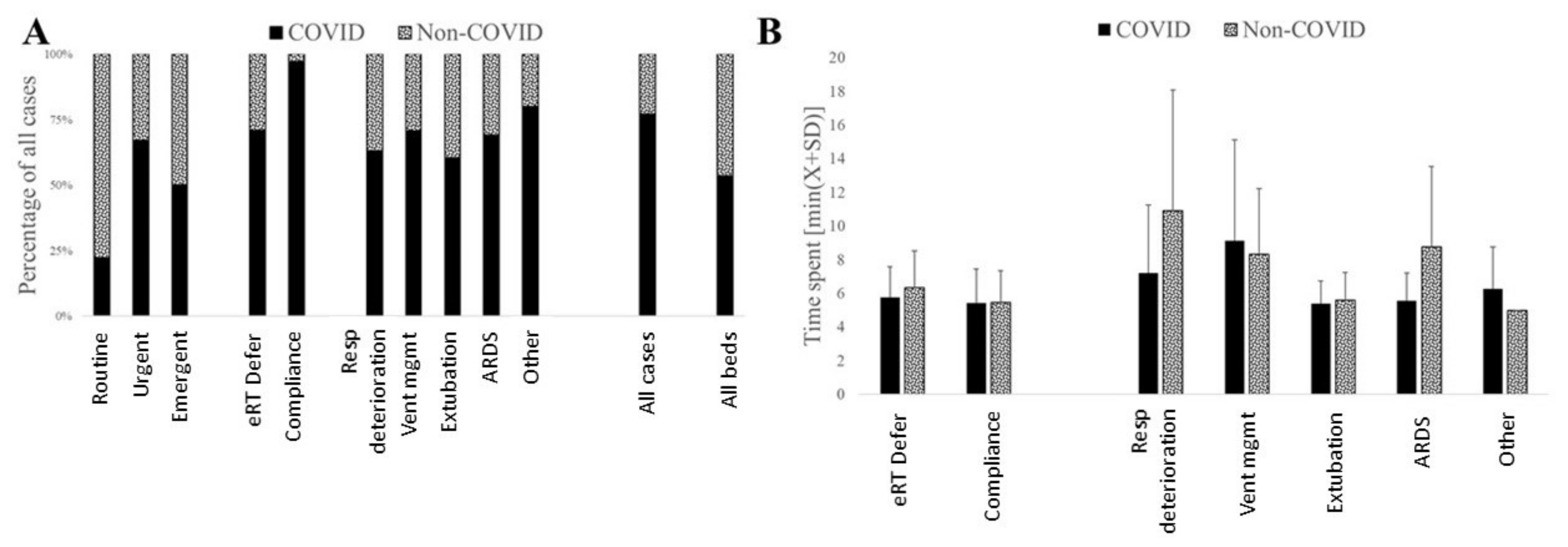
3.2. The Involvement of eRT Services with COVID-19 and Non-COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poston, J.T.; Patel, B.K.; Davis, A.M. Management of Critically Ill Adults With COVID-19. JAMA 2020, 323, 1839–1841. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.S.; Horton, D.B.; Roy, J.; Gennaro, M.L.; Brooks, A.; Tischfield, J.; Greenberg, P.; Andrews, T.; Jagpal, S.; Reilly, N.; et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic. BMC Infect. Dis. 2020, 20, 853. [Google Scholar] [CrossRef]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus Disease 2019 (COVID-2019) Infection Among Health Care Workers and Implications for Prevention Measures in a Tertiary Hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef] [PubMed]
- Benge, C.D.; Barwise, J.A. Aerosolization of COVID-19 and Contamination Risks During Respiratory Treatments. Fed. Pract. 2020, 37, 160–163. [Google Scholar]
- Petsonk, E.L.; Harber, P. Respiratory protection for health care workers: A 2020 COVID-19 perspective. Am. J. Ind. Med. 2020, 63, 655–658. [Google Scholar] [CrossRef]
- Li, R.; Rivers, C.; Tan, Q.; Murray, M.B.; Toner, E.; Lipsitch, M. Estimated Demand for US Hospital Inpatient and Intensive Care Unit Beds for Patients with COVID-19 Based on Comparisons With Wuhan and Guangzhou, China. JAMA Netw. Open 2020, 3, e208297. [Google Scholar] [CrossRef]
- Armaghan, R.; Geesey, B.; Juby, J.; Amador-Castaneda, J.; Bollinger, A.; Roberts, K.J.; Newberry, R.; Harshberger, M.; Radabaugh, N.; Pierce, M.; et al. Practice of Respiratory Therapists in Pennsylvania: A Statewide Survey. Respir. Care 2020, 65, 972–976. [Google Scholar] [CrossRef]
- Registered Respiratory Therapist (RRT). 2020. Available online: https://www.nbrc.org/examinations/rrt/ (accessed on 1 June 2020).
- Higny, J.; Feye, F.; Foret, F. COVID-19 pandemic: Overview of protective-ventilation strategy in ARDS patients. Acta Clin. Belg. 2020, 76, 509–511. [Google Scholar] [CrossRef]
- Kapoor, I.; Prabhakar, H.; Mahajan, C. Transference of COVID-19 patient in hospitals—A crucial phase. J. Clin. Anesth. 2020, 65, 109931. [Google Scholar] [CrossRef]
- Srinivasan, S.R. Editorial: Tele-ICU in the Age of COVID-19: Built for This Challenge. J. Nutr. Health Aging 2020, 24, 536–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef] [PubMed]
- Lilly, C.M.; Greenberg, B. The Evolution of Tele-ICU to Tele-Critical Care. Crit. Care Med. 2020, 48, 610–611. [Google Scholar] [CrossRef] [Green Version]
- Khunlertkit, A.; Carayon, P. Contributions of tele-intensive care unit (Tele-ICU) technology to quality of care and patient safety. J. Crit. Care 2013, 28, e311–e312. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Gudowski, S.W.; Roberts, K.J.; Scott, M.J.; Laudanski, K. Establishing a Telemedicine Respiratory Therapy Service (eRT) in the COVID-19 Pandemic. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.M.; Thongprayoon, C.; Kashyap, R.; Chute, C.G.; Gajic, O.; Pickering, B.W.; Herasevich, V. Developing the surveillance algorithm for detection of failure to recognize and treat severe sepsis. Mayo Clin. Proc. 2015, 90, 166–175. [Google Scholar] [CrossRef]
- Giannini, H.M.; Ginestra, J.C.; Chivers, C.; Draugelis, M.; Hanish, A.; Schweickert, W.D.; Fuchs, B.D.; Meadows, L.; Lynch, M.; Donnelly, P.J.; et al. A Machine Learning Algorithm to Predict Severe Sepsis and Septic Shock: Development, Implementation, and Impact on Clinical Practice. Crit. Care Med. 2019, 47, 1485–1492. [Google Scholar] [CrossRef]
- Anderson, B.J.; Do, D.; Chivers, C.; Choi, K.; Gitelman, Y.; Mehta, S.J.; Panchandam, V.; Gudowski, S.; Pierce, M.; Cereda, M.; et al. Clinical Impact of an Electronic Dashboard and Alert System for Sedation Minimization and Ventilator Liberation: A Before-After Study. Crit. Care Explor. 2019, 1, e0057. [Google Scholar] [CrossRef]
- Marra, A.; Ely, E.W.; Pandharipande, P.P.; Patel, M.B. The ABCDEF Bundle in Critical Care. Crit. Care Clin. 2017, 33, 225–243. [Google Scholar] [CrossRef] [Green Version]
- Barnes-Daly, M.A.; Pun, B.T.; Harmon, L.A.; Byrum, D.G.; Kumar, V.K.; Devlin, J.W.; Stollings, J.L.; Puntillo, K.A.; Engel, H.J.; Posa, P.J.; et al. Improving Health Care for Critically Ill Patients Using an Evidence-Based Collaborative Approach to ABCDEF Bundle Dissemination and Implementation. Worldviews Evid. Based Nurs. 2018, 15, 206–216. [Google Scholar] [CrossRef]
- Boehm, L.M.; Vasilevskis, E.E.; Mion, L.C. Interprofessional perspectives on ABCDE bundle implementation: A focus group study. Dimens. Crit. Care Nurs. 2016, 35, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, T.A.; Gale, D.D.; Kacmarek, R.M.; Kageler, W.V. Competencies needed by fraduate respiratory therapists in 2015 and beyond. Respir. Care 2010, 55, 601–616. [Google Scholar]
- Lilly, C.M.; Thomas, E.J. Tele-ICU: Experience to date. J. Intensive Care Med. 2010, 25, 16–22. [Google Scholar] [CrossRef]
- Fuhrman, S.A.; Lilly, C.M. ICU Telemedicine Solutions. Clin. Chest Med. 2015, 36, 401–407. [Google Scholar] [CrossRef]
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P.A. What Other Countries Can Learn From Italy During the COVID-19 Pandemic. JAMA 2020, 180, 927–928. [Google Scholar] [CrossRef] [Green Version]
- Pastores, S.M.; Kvetan, V.; Coopersmith, C.M.; Farmer, J.C.; Sessler, C.; Christman, J.W.; D’Agostino, R.; Diaz-Gomez, J.; Gregg, S.R.; Khan, R.A.; et al. Workforce, Workload, and Burnout Among Intensivists and Advanced Practice Providers: A Narrative Review. Crit. Care Med. 2019, 47, 550–557. [Google Scholar] [CrossRef]
- Kain, T.; Fowler, R. Preparing intensive care for the next pandemic influenza. Crit. Care 2019, 23, 337. [Google Scholar] [CrossRef] [Green Version]
- Kallet, R.H.; Zhuo, H.; Yip, V.; Gomez, A.; Lipnick, M.S. Spontaneous Breathing Trials and Conservative Sedation Practices Reduce Mechanical Ventilation Duration in Subjects With ARDS. Respir. Care 2018, 63, 1–10. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Total Count | % of Total | % Cumulative |
|---|---|---|---|
| Proactive rounding | 1024 | 59.67 | 59.67 |
| Site-trigger | 405 | 23.6 | 83.9 |
| eTriage | 84 | 4.89 | 88.81 |
| Sniffer/Dashboard Tool (ARDS, sepsis, etc.) | 11 | 0.6% | 88.81 |
| Push Button | 3 | 0.17% | 88.81 |
| Virtual consult | 1 | 0.1 | 89.04 |
| Other (place a note in Clinical Comment) | 1 | 0.1 | 89.10 |
| Missing | 187 | 10.89 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierce, M.; Gudowski, S.W.; Roberts, K.J.; Jackominic, A.; Zumstein, K.K.; Shuttleworth, A.; Ho, J.; Susser, P.; Parikh, A.; Chandler, J.M.; et al. The Rapid Implementation of Ad Hoc Tele-Critical Care Respiratory Therapy (eRT) Service in the Wake of the COVID-19 Surge. J. Clin. Med. 2022, 11, 718. https://doi.org/10.3390/jcm11030718
Pierce M, Gudowski SW, Roberts KJ, Jackominic A, Zumstein KK, Shuttleworth A, Ho J, Susser P, Parikh A, Chandler JM, et al. The Rapid Implementation of Ad Hoc Tele-Critical Care Respiratory Therapy (eRT) Service in the Wake of the COVID-19 Surge. Journal of Clinical Medicine. 2022; 11(3):718. https://doi.org/10.3390/jcm11030718
Chicago/Turabian StylePierce, Margarete, Steven W. Gudowski, Karsten J. Roberts, Anthony Jackominic, Karen K. Zumstein, Amanda Shuttleworth, Joshua Ho, Phillip Susser, Alomi Parikh, John M. Chandler, and et al. 2022. "The Rapid Implementation of Ad Hoc Tele-Critical Care Respiratory Therapy (eRT) Service in the Wake of the COVID-19 Surge" Journal of Clinical Medicine 11, no. 3: 718. https://doi.org/10.3390/jcm11030718