
Evaluation of Screening Tests in Bavarian Healthcare Facilities during the Second Wave of the SARS-CoV-2 Pandemic

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Bavarian Corona Testing Strategy
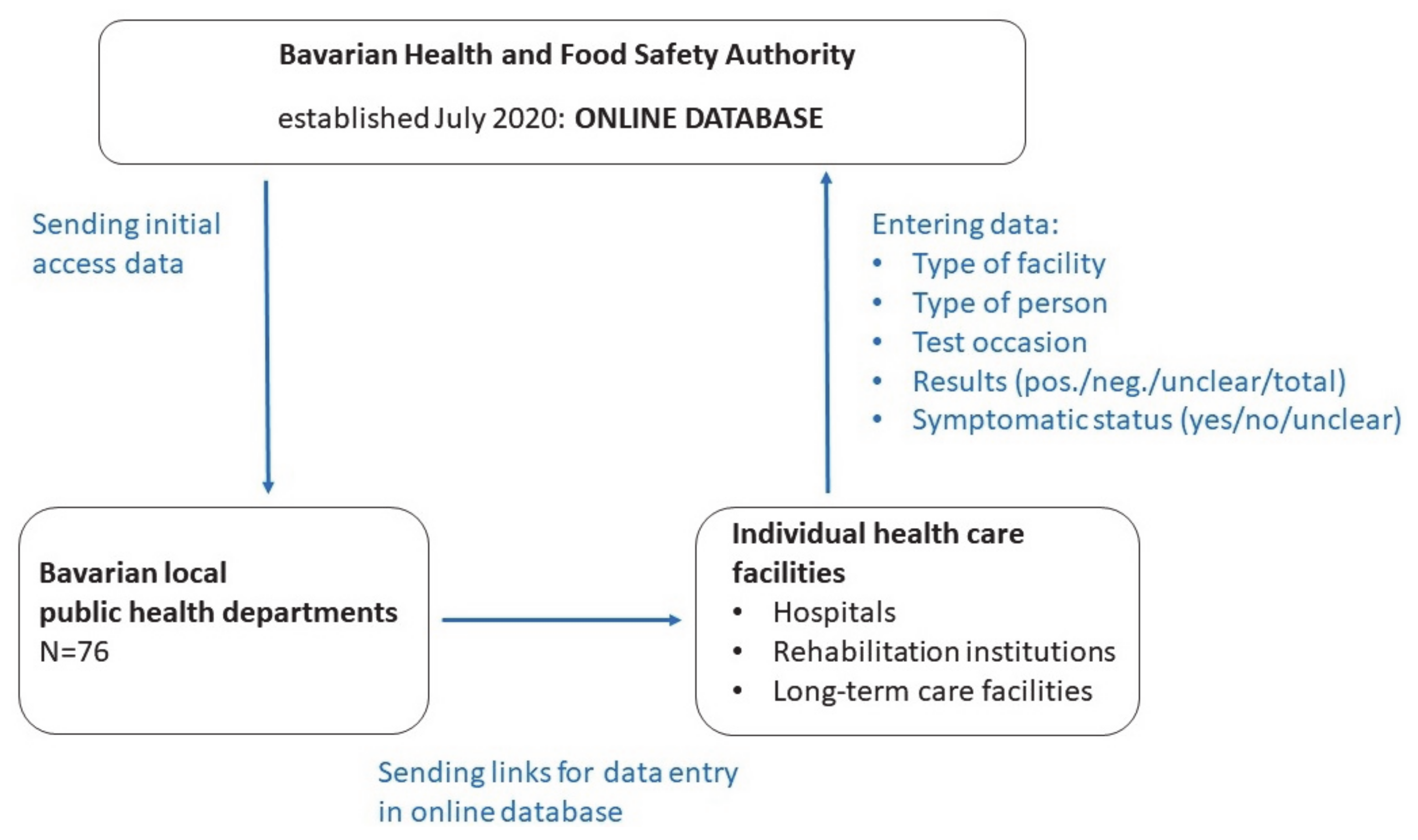
2.2. The Bavarian Online Database BayCoRei
2.3. Study Design of the Current Investigation
2.4. Statistical Methods
3. Results
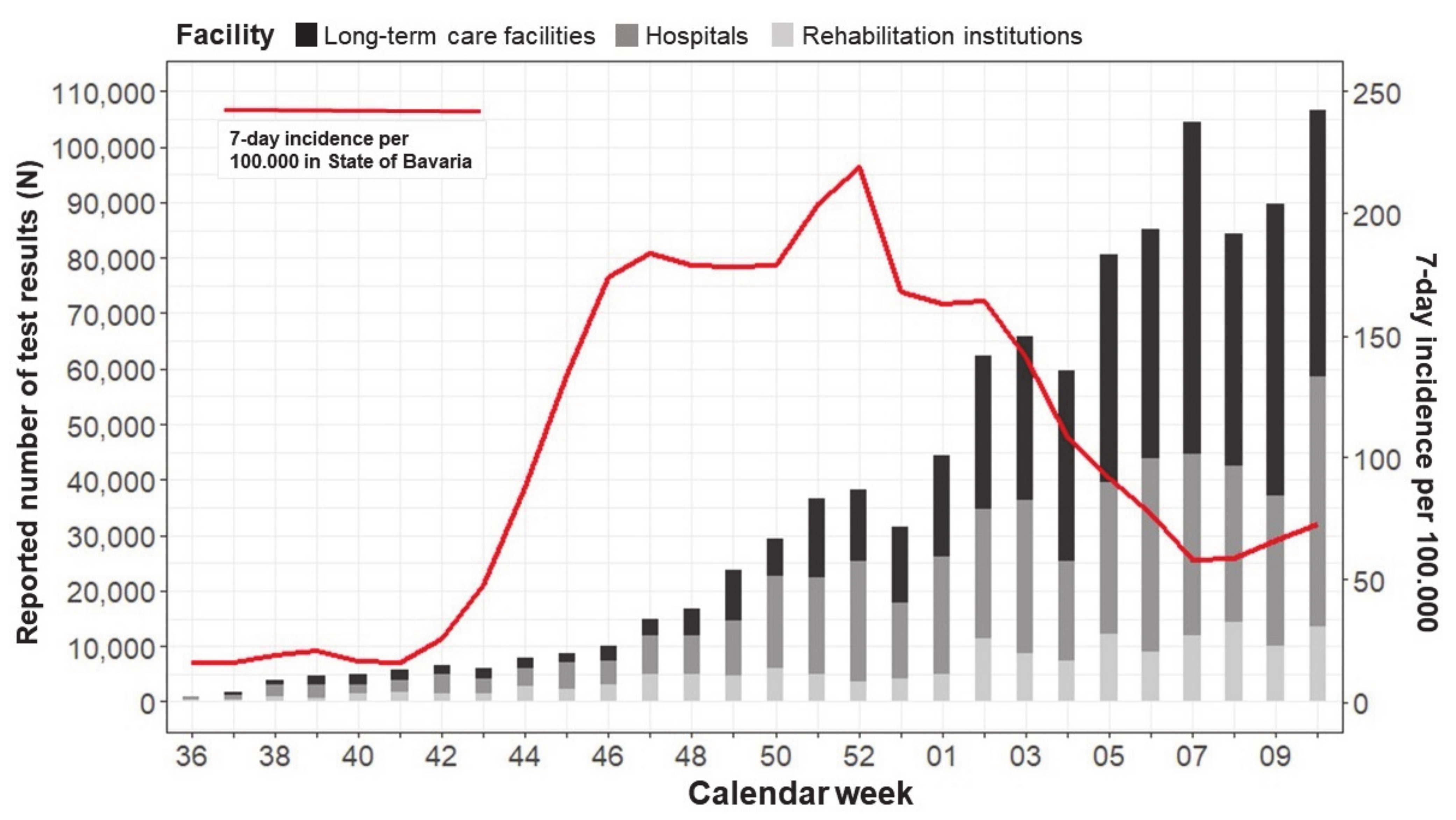
3.1. Reported Test Data in Comparison with Current Statistics
3.2. Overview of Accumulated Screening Tests and Positive Rates
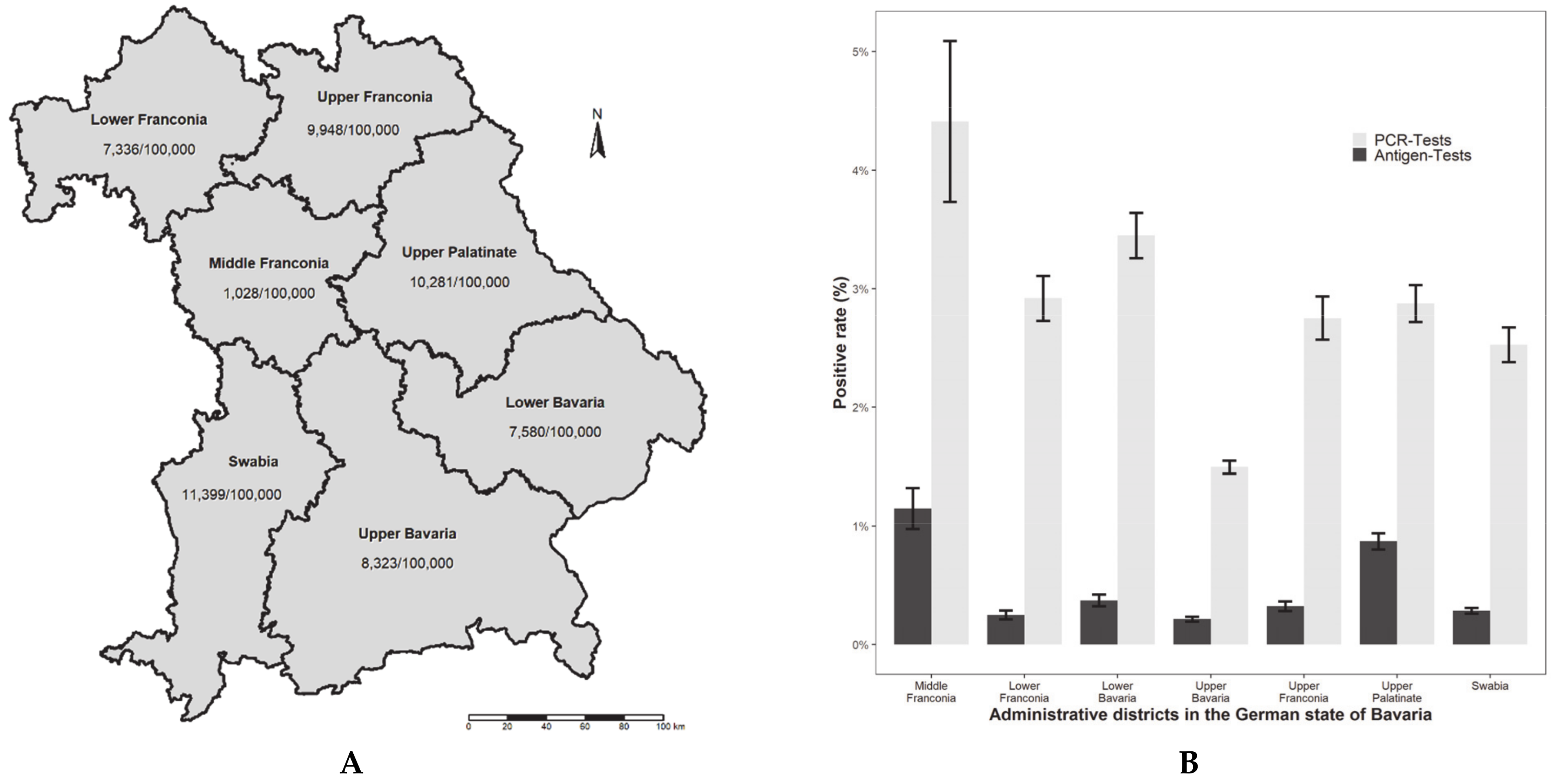
3.3. Comparison of Regional Differences in the State of Bavaria
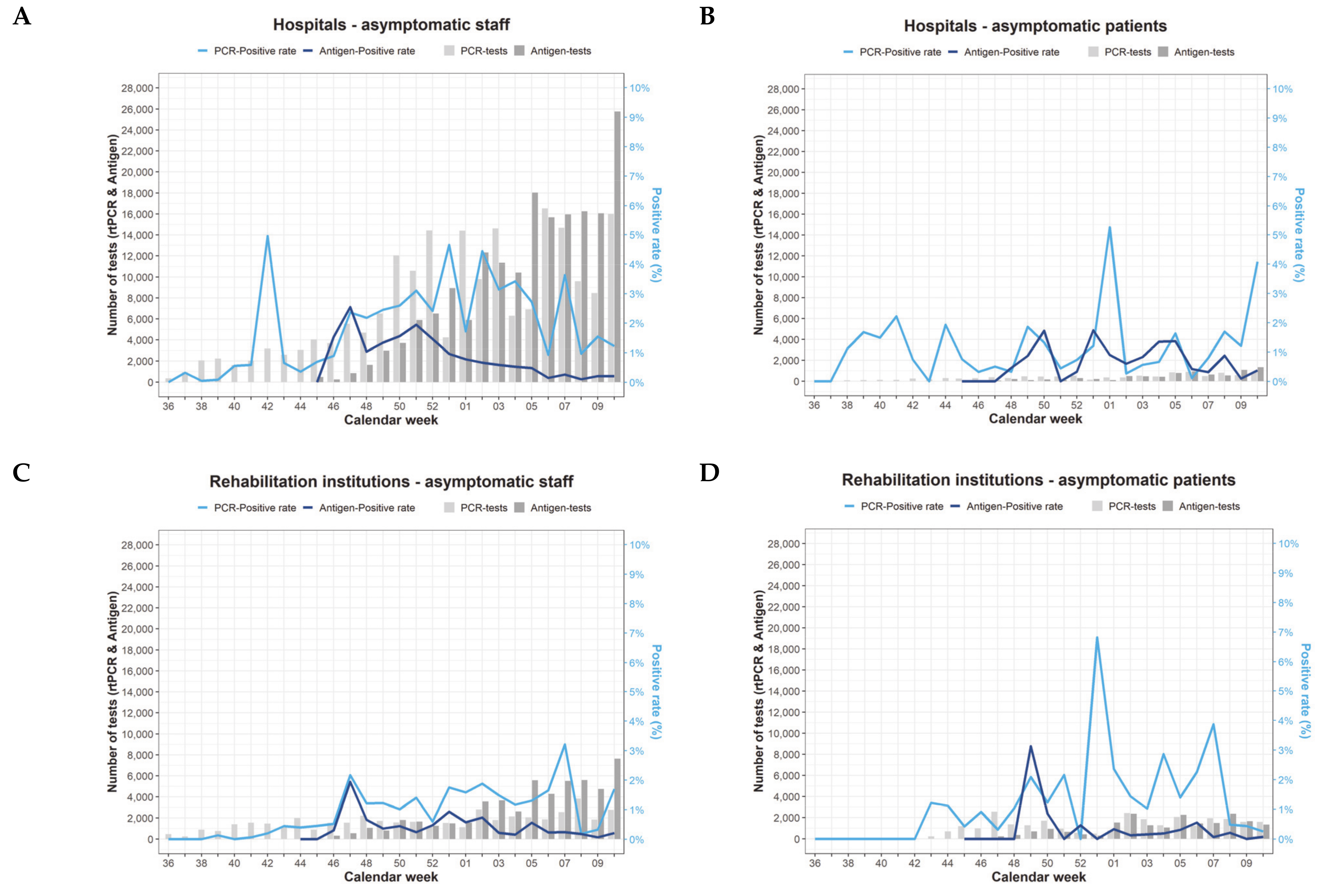
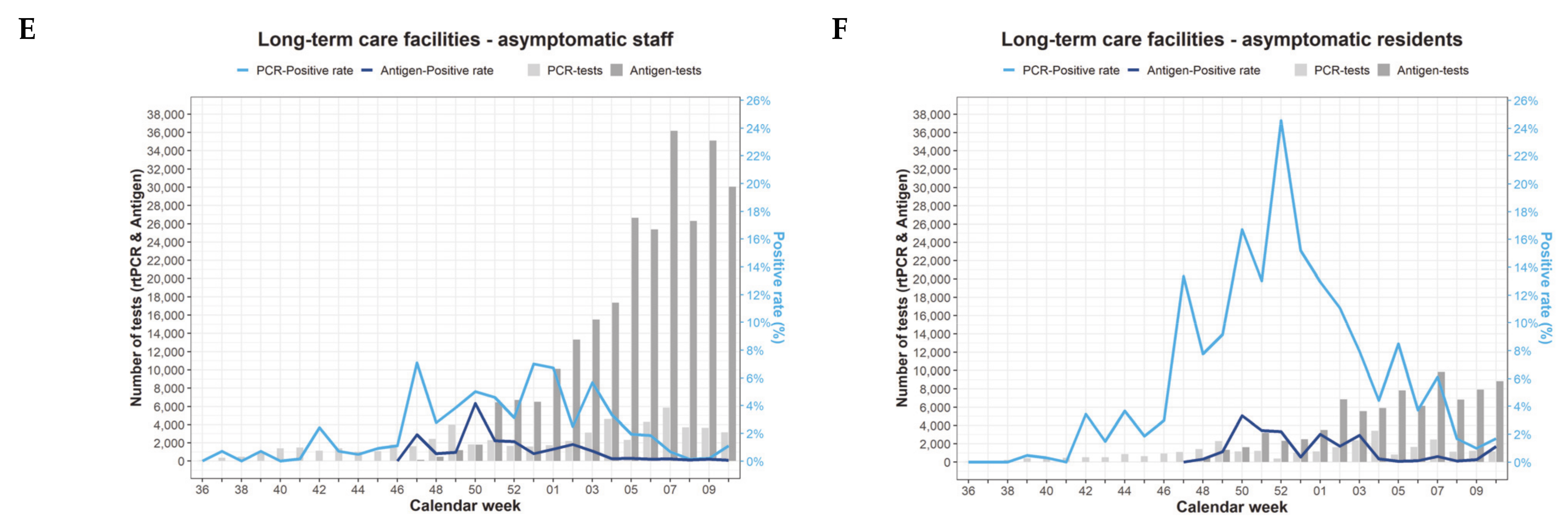
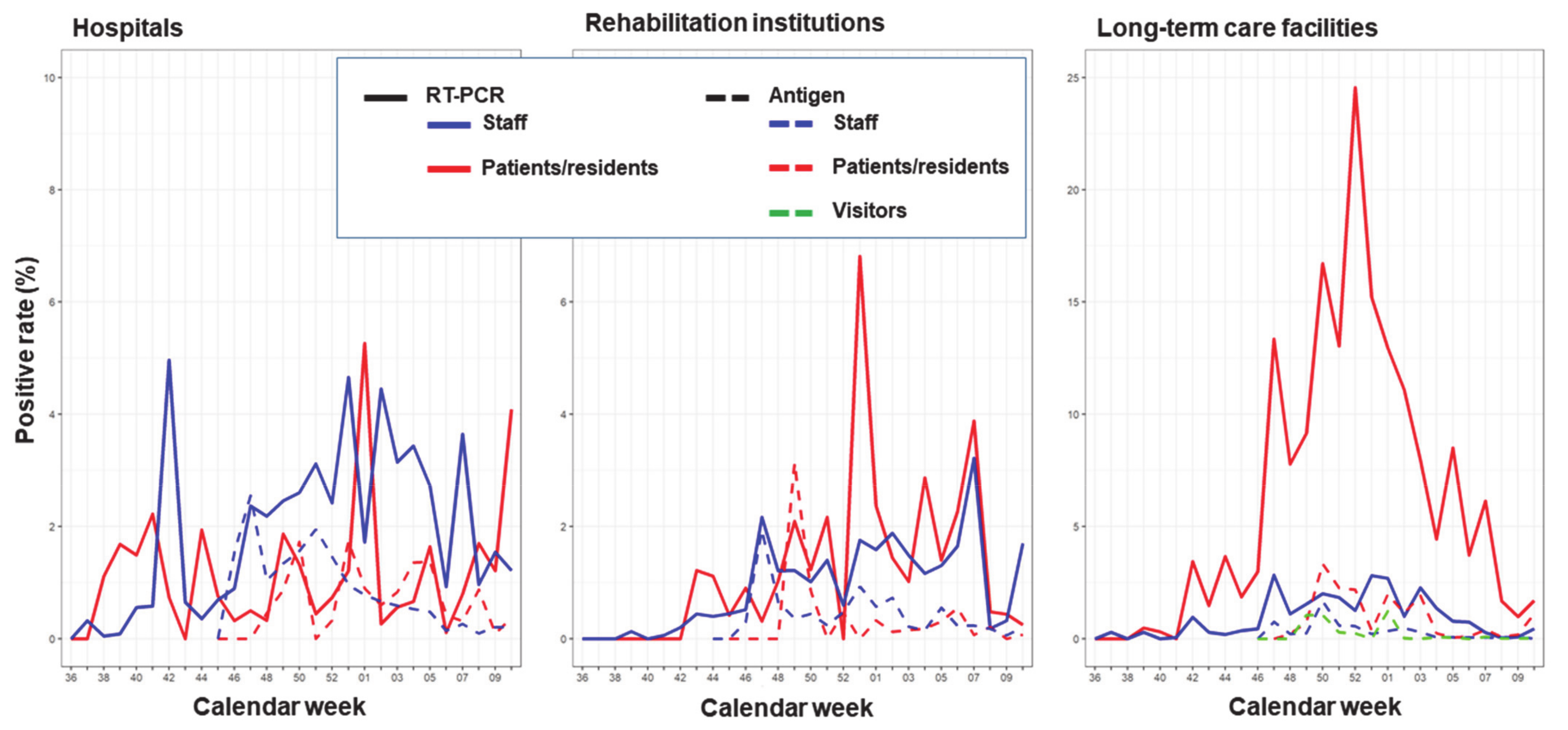
3.4. Temporal Variation of Screening Test Results and Positive Rates
4. Discussion
4.1. Summary of the Main Findings
4.2. Findings in Comparison to Previous Studies
4.3. Asymptomatic Testing as a Surveillance Instrument
4.4. Comparison of RT-PCR and Antigen Positivity Rates among Asymptomatic Populations
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahase, E. Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization COVID-19 Dashboard. 2021. Available online: https://covid19.who.int/ (accessed on 29 June 2021).
- Black, J.R.M.; Bailey, C.; Przewrocka, A.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Park, S.; Oh, H.; Hong, D. Mass screening of healthcare personnel for SARS-CoV-2 in the Northern Emirates. J. Hosp. Infect. 2021, 108, 52–54. [Google Scholar] [CrossRef]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife 2020, 9, e58728. [Google Scholar] [CrossRef] [PubMed]
- Panagiotou, O.A.; Kosar, C.M.; White, E.M.; Bantis, L.E.; Yang, X.; Santostefano, C.M.; Feifer, R.A.; Blackman, C.; Rudolph, J.L.; Gravenstein, S.; et al. Risk Factors Associated with All-Cause 30-Day Mortality in Nursing Home Residents with COVID-19. JAMA Intern. Med. 2021, 181, 439. [Google Scholar] [CrossRef]
- Smith, D.R.M.; Duval, A.; Pouwels, K.B.; Guillemot, D.; Fernandes, J.; Huynh, B.-T.; Temime, L.; Opatowski, L. Optimizing COVID-19 surveillance in long-term care facilities: A modelling study. BMC Med. 2020, 18, 386. [Google Scholar] [CrossRef]
- World Health Organization. Preventing and Managing COVID-19 across Long-Term Care Services: Policy Brief. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Policy_Brief-Long-term_Care-2020.1 (accessed on 23 February 2021).
- Salcher-Konrad, M.; Jhass, A.; Naci, H.; Tan, M.; El-Tawil, Y.; Comas-Herrera, A. COVID-19 related mortality and spread of disease in long-term care: A living systematic review of emerging evidence. MedRxiv 2020. [CrossRef]
- Padula, W.V. Why Only Test Symptomatic Patients? Consider Random Screening for COVID-19. Appl. Health Econ. Health Policy 2020, 18, 333–334. [Google Scholar] [CrossRef] [Green Version]
- Burki, T. Mass testing for COVID-19. Lancet Microbe 2020, 1, e317. [Google Scholar] [CrossRef]
- Iacobucci, G. Covid-19: Mass population testing is rolled out in Liverpool. BMJ 2020, 371, m4268. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.K.; Scott, H.M.; DuBois, A.; Sturtz, N.; Lu, W.; Stoltey, J.; Masinde, G.; Cohen, S.; Sachdev, D.; Philip, S.; et al. Lessons From Mass-Testing for Coronavirus Disease 2019 in Long-Term Care Facilities for the Elderly in San Francisco. Clin. Infect. Dis. 2021, 72, 2018–2020. [Google Scholar] [CrossRef]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z.; et al. Asymptomatic and Presymptomatic SARS-CoV-2 Infections in Residents of a Long-Term Care Skilled Nursing Facility—King County, Washington, March 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böhmer, M.M.; Buchholz, U.; Corman, V.M.; Hoch, M.; Katz, K.; Marosevic, D.V.; Böhm, S.; Woudenberg, T.; Ackermann, N.; Konrad, R.; et al. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: A case series. Lancet Infect. Dis. 2020, 20, 920–928. [Google Scholar] [CrossRef]
- Wjst, M. Die frühe Phase der COVID-19-Pandemie in Bayern. DMW Dtsch. Med. Wochenschr. 2021, 146, e1–e9. [Google Scholar] [CrossRef]
- StMGP. Bayerische Teststrategie. 2020. Available online: https://www.stmgp.bayern.de/coronavirus/bayerische-teststrategie/ (accessed on 26 January 2021).
- Bayerische Staatskanzlei. Bericht aus der Kabinettssitzung Nr.114: 1. Bayerische Teststrategie zur Bewältigung der Corona-Pandemie/Testungen zum Schutz bei akutem Infektionsgeschehen/Testungen zur Sicherheit der Bewohner Bayerns/Testungen zur Prävention in infektionsgefährdeten Bereichen. 30 June 2020. Available online: https://www.bayern.de/wp-content/uploads/2020/08/200630-ministerrat.pdf (accessed on 26 January 2021).
- Mühle, U.; Kuhn, J.; Nennstiel, U. Protecting vulnerable populations from COVID-19: Why health governance and operations matter to implement interventions fast. Bavarian perspective. HealthManagement.org 2020, 20, 628–635. [Google Scholar]
- Bayerisches Staatsministerium für Gesundheit und Pflege. Vollzug des Infektionsschutzgesetzes (IfSG): Allgemeinverfügung Notfallplan Corona-Pandemie Regelungen für Pflegeeinrichtungen: Vom 24 February 2021, Az. G43f-G8300-2020/1628-16. 2021. Available online: https://www.verkuendung-bayern.de/baymbl/2021-148/ (accessed on 12 March 2021).
- Bayerisches Staatsministerium für Gesundheit und Pflege. Vollzug des Infektionsschutzgesetzes (IfSG): Allgemeinverfügung Notfallplan Corona-Pandemie Regelungen für stationäre Einrichtungen für Menschen mit Behinderung: Vom 24 February 2021, Az. G43f-G8300-2020/1628-17. 2021. Available online: https://www.verkuendung-bayern.de/files/baymbl/2021/147/baymbl-2021-147.pdf (accessed on 12 March 2021).
- Bayerische Staatskanzlei. Bericht aus der Kabinettssitzung Nr. 197. 06 December 2020. Available online: https://www.bayern.de/wp-content/uploads/2021/01/201206-ministerrat-1-1.pdf (accessed on 12 March 2021).
- Robert Koch Institute (RKI). Situation Report—14 October 2020: Nationale Teststrategie—Wer Wird in Deutschland auf das Vorliegen Einer SARS-CoV-2 Infektion Getestet? 2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Okt_2020/2020-10-14-en.html (accessed on 13 April 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bayerisches Landesamt für Gesundheit und Lebensmittelsicherheit. Übersicht der Fallzahlen von Coronavirusinfektionen in Bayern. Available online: https://www.lgl.bayern.de/gesundheit/infektionsschutz/infektionskrankheiten_a_z/coronavirus/karte_coronavirus/ (accessed on 16 March 2021).
- Bayerisches Landesamt für Statistik. Statistische Berichte: Krankenhausstatistik 2019: Grunddaten, Diagnosen und Kostennachweis. 2021. Available online: https://www.statistik.bayern.de/mam/produkte/veroffentlichungen/statistische_berichte/a4200c_201900.pdf (accessed on 23 April 2021).
- Bayerisches Landesamt für Statistik. Statistische Berichte: Einrichtungen und betreute Wohnformen für volljährige Menschen mit Behinderung in Bayern 2018. 2019. Available online: https://www.statistik.bayern.de/mam/produkte/veroffentlichungen/statistische_berichte/k8200c_201851.pdf (accessed on 23 April 2021).
- Bayerisches Landesamt für Statistik. Statistische Berichte: Pflegeeinrichtungen, Ambulante Sowie Stationäre und Pflegegeldempfänger in Bayern. 2020. Available online: https://www.statistik.bayern.de/mam/produkte/veroffentlichungen/statistische_berichte/k8300c_201951.pdf (accessed on 23 April 2021).
- Bundesministerium für Gesundheit. Die nationale Teststrategie—Coronatests in Deutschland. 2020. Available online: https://www.bundesgesundheitsministerium.de/coronatest.html#c19143 (accessed on 1 March 2021).
- Bundesministerium für Gesundheit. Verordnung zum Anspruch auf Testung in Bezug auf einen Direkten Erregernachweis des Coronavirus SARS-CoV-2 (Coronavirus-Testverordnung—TestV). 2020. Available online: https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/C/Coronavirus/Verordnungen/Corona-Test-VO_BAnz_AT_141020.pdf (accessed on 20 May 2021).
- Oran, D.P.; Topol, E. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Bernadou, A.; Bouges, S.; Catroux, M.; Rigaux, J.C.; Laland, C.; Levêque, N.; Noury, U.; Larrieu, S.; Acef, S.; Habold, D.; et al. High impact of COVID-19 outbreak in a nursing home in the Nouvelle-Aquitaine region, France, March to April 2020. BMC Infect. Dis. 2021, 21, 198. [Google Scholar] [CrossRef]
- Heudorf, U.; Müller, M.; Schmehl, C.; Gasteyer, S.; Steul, K. COVID-19 in long-term care facilities in Frankfurt am Main, Germany: Incidence, case reports, and lessons learned. GMS Hyg. Infect. Control 2020, 15, Doc26. [Google Scholar] [CrossRef]
- Brown, C.S.; Clare, K.; Chand, M.; Andrews, J.; Auckland, C.; Beshir, S.; Choudhry, S.; Davies, K.; Freeman, J.; Gallini, A.; et al. Snapshot PCR surveillance for SARS-CoV-2 in hospital staff in England. J. Infect. 2020, 81, 427–434. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef] [PubMed]
- Oran, A.D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic. Ann. Intern. Med. 2021, 174, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, A.N.; Hemarajata, P.; Mehta, N.; Campbell, S.; Mitchell, S.; Palavecino, E.; Butler-Wu, S.; Miller, M.B. When Should Asymptomatic Persons Be Tested for COVID-19? J. Clin. Microbiol. 2020, 59. [Google Scholar] [CrossRef] [PubMed]
- StMGP. Neunte Bayerische Infektionsschutzmaßnahmenverordnung (9. BayIfSMV); 30 November 2020. Available online: https://www.verkuendung-bayern.de/files/baymbl/2020/683/baymbl-2020-683.pdf (accessed on 8 July 2021).
- StMGP. Zehnte Bayerische Infektionsschutzmaßnahmenverordnung (10. BayIfSMV); 8 December 2020. Available online: https://www.verkuendung-bayern.de/files/baymbl/2020/711/baymbl-2020-711.pdf (accessed on 8 July 2021).
- StMGP. Elfte Bayerische Infektionsschutzmaßnahmenverordnung (11. BayIfSMV); 15 December 2020. Available online: https://www.verkuendung-bayern.de/files/baymbl/2020/737/baymbl-2020-737.pdf (accessed on 8 July 2021).
- Mor, V.; Gutman, R.; Yang, X.; White, E.M.; McConeghy, K.W.; Feifer, R.A.; Blackman, C.R.; Kosar, C.M.; Bardenheier, B.H.; Gravenstein, S.A. Short-term impact of nursing home SARS-CoV -2 vaccinations on new infections, hospitalizations, and deaths. J. Am. Geriatr. Soc. 2021. [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Mac Aonghusa, P.; O’Shea, D.F. Correlation of national and healthcare workers COVID-19 infection data; implications for large-scale viral testing programs. PLoS ONE 2021, 16, e0250699. [Google Scholar] [CrossRef]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Tambe, M.; Mina, M.J.; Parker, R. Test sensitivity is secondary to frequency and turnaround time for COVID-19 screening. Sci. Adv. 2021, 7, eabd5393. [Google Scholar] [CrossRef]
- Paul-Ehrlich-Institut. Bundesinstitut für Impfstoffe und biomedizinische Arzneimittel. Mindestkriterien für SARS-CoV-2 Antigentests im Sinne von § 1 Abs. 1 Satz 1 TestVO: Antigenschnelltests. 2021. Available online: https://www.pei.de/SharedDocs/Downloads/DE/newsroom/dossiers/mindestkriterien-sars-cov-2-antigentests-01-12-2020.pdf?__blob=publicationFile&v=6 (accessed on 24 April 2021).
- Dinnes, J.; Deeks, J.J.; Adriano, A.; Berhane, S.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; Beese, S.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2020, 2020, CD013705. [Google Scholar] [CrossRef]
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection Using Rapid Immunoassays: Interim Guidance. 2020. Available online: https://apps.who.int/iris/handle/10665/334253 (accessed on 1 March 2021).
- Hayer, J.; Kasapic, D.; Zemmrich, C. Real-world clinical performance of commercial SARS-CoV-2 rapid antigen tests in suspected COVID-19: A systematic meta-analysis of available data as per 20 November 2020. Int. J. Infect. Dis. 2020. [CrossRef]
- Corman, V.M.; Haage, V.C.; Bleicker, T.; Schmidt, M.L.; Mühlemann, B.; Zuchowski, M.; Jo, W.K.; Tscheak, P.; Möncke-Buchner, E.; A Müller, M.; et al. Comparison of seven commercial SARS-CoV-2 rapid point-of-care antigen tests: A single-centre laboratory evaluation study. Lancet Microbe 2021, 2, e311–e319. [Google Scholar] [CrossRef]
- Frnda, J.; Durica, M. On Pilot Massive COVID-19 Testing by Antigen Tests in Europe. Case Study: Slovakia. Infect. Dis. Rep. 2021, 13, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Malloy, G.S.P.; Puglisi, L.; Brandeau, M.L.; Harvey, T.D.; A Wang, E. Effectiveness of interventions to reduce COVID-19 transmission in a large urban jail: A model-based analysis. BMJ Open 2021, 11, e042898. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Kahwati, L.; Jahn, B.; Giger, K.; Dobrescu, A.I.; Hill, C.; Klerings, I.; Meixner, J.; Persad, E.; Teufer, B.; et al. Universal screening for SARS-CoV-2 infection: A rapid review. Cochrane Database Syst. Rev. 2020, 2020, CD013718. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: Mass testing in Slovakia may have helped cut infections. BMJ 2020, 371, m4761. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RT-PCR-Tests # N (%) | Positive n | Positive (%) (95%CI) | Antigen Tests ** N (%) | Positive n | Positive (%) (95%CI) | |
|---|---|---|---|---|---|---|
| OVERALL (100%) * | 382,240 (37%) | 8380 | 2.2% (2.1–2.2) | 655,906 (63%) | 2327 | 0.4% (0.3–0.4) |
| Hospitals | 213,170 (100%) | 4673 | 2.2% (2.1–2.3) | 196,723 (100%) | 1013 | 0.5% (0.5–0.5) |
| Staff | 201,826 (95%) | 4,511 | 2.2% (2.2–2.3) | 180,350 (92%) | 942 | 0.5% (0.5–0.6) |
| Patients | 10,940 (5%) | 147 | 1.3% (1.1–1.6) | 8,288 (4%) | 52 | 0.6% (0.5–0.8) |
| Visitors | 404 (0.2%) | 15 | 3.7% (2.3–6.1) | 8,085 (4%) | 19 | 0.2% (0.2–0.4) |
| Rehabilitation institutions | 76,244 (100%) | 923 | 1.2% (1.1–1.3) | 77,166 (100%) | 256 | 0.3% (0.3–0.4) |
| Staff | 46,779 (61%) | 508 | 1.1% (1.0–1.2) | 53,981 (70%) | 184 | 0.3% (0.3–0.4) |
| Patients | 29,029 (38%) | 412 | 1.4% (1.3–1.6) | 20,724 (27%) | 66 | 0.3% (0.3–0.4) |
| Visitors | 436 (0.6%) | 3 | 0.7% (0.2–2.1) | 2,461 (3%) | 6 | 0.2% (0.1–0.5) |
| Long-term care facilities | 92,826 (100%) | 2784 | 3.0% (2.9–3.1) | 382,017 (100%) | 1058 | 0.3% (0.3–0.3) |
| Staff | 61,450 (66%) | 602 | 1.0% (0.9–1.1) | 259,534 (68%) | 377 | 0.1% (0.1–0.2) |
| Residents | 30,758 (33%) | 2181 | 7.1% (6.8–7.4) | 80,808 (21%) | 636 | 0.8% (0.7–0.9) |
| Visitors | 618 (0.7%) | 1 | 0.2% (0.02–1.1) | 41,675 (11%) | 45 | 0.1% (0.08–0.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tischer, C.; Stupp, C.; Janson, P.; Willeke, K.; Hung, C.-W.; Flöter, J.; Kirchner, A.; Zink, K.; Eder, L.; Hackl, C.; et al. Evaluation of Screening Tests in Bavarian Healthcare Facilities during the Second Wave of the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7371. https://doi.org/10.3390/ijerph18147371
Tischer C, Stupp C, Janson P, Willeke K, Hung C-W, Flöter J, Kirchner A, Zink K, Eder L, Hackl C, et al. Evaluation of Screening Tests in Bavarian Healthcare Facilities during the Second Wave of the SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(14):7371. https://doi.org/10.3390/ijerph18147371
Chicago/Turabian StyleTischer, Christina, Carolin Stupp, Patrick Janson, Kristina Willeke, Chu-Wei Hung, Jessica Flöter, Anna Kirchner, Katharina Zink, Lisa Eder, Christina Hackl, and et al. 2021. "Evaluation of Screening Tests in Bavarian Healthcare Facilities during the Second Wave of the SARS-CoV-2 Pandemic" International Journal of Environmental Research and Public Health 18, no. 14: 7371. https://doi.org/10.3390/ijerph18147371