
Antispike Immunoglobulin-G (IgG) Titer Response of SARS-CoV-2 mRNA-Vaccine (BNT162b2): A Monitoring Study on Healthcare Workers

 ,
,  ,
,  , ,
, ,  , , , , , , ,
, , , , , , ,  , , ,
, , ,  ,
,  , ,
, ,  ,
,  and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
- Elderly 65 years of age or older: people aged 65 and over should receive a booster injection. The risk of severe COVID-19 disease increases with age.
- Long-term care facility residents aged 18 and over: Long-term care facility residents live closely together in group settings.
- People with comorbidities between the ages of 18 and 64.
- People who work or live in high-risk environments between the ages of 18 and 64.
2. Materials and Methods
2.1. General Characteristics
- -
- dental area: dental physicians, chair assistants, hygienists, and nurses: a total of 90 were evaluated. (39.13% of 230 total)
- -
- radiological area: radiology physicians, technicians, and nurses: a total of 72 were evaluated (31.30% of a total of 230)
- -
- internal medicine area: a total of 34 were evaluated (14.78% of a total of 230);
- -
- Forensic Medicine area: a total of 34 (14.78% of 230 total) were evaluated.
- Group I: subjects between 20–30 years old;
- Group II: subjects between 30–40 years old;
- Group III: subjects between 40–50 years old;
- Group IV: subjects between 50–60 years old;
- Group V: subjects between 60–70 years old;
2.2. Statistical Analysis
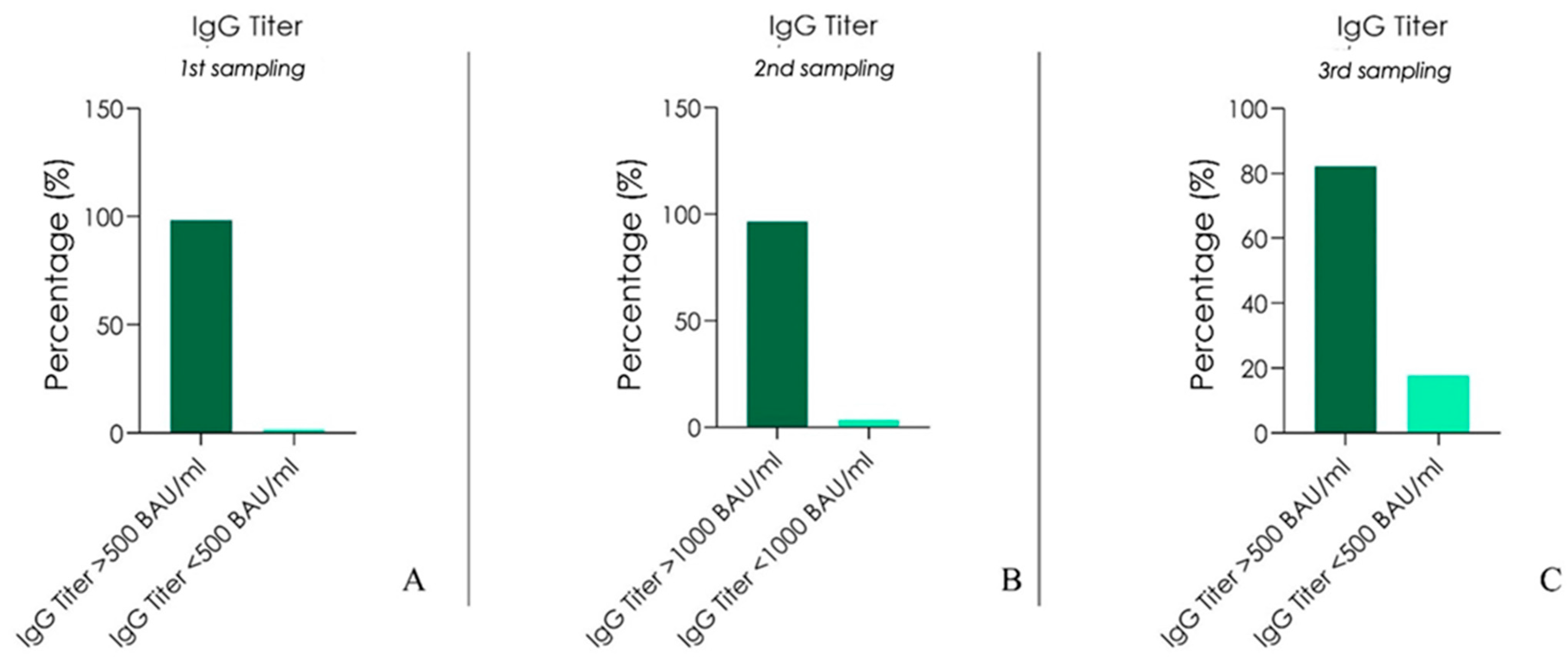
3. Results
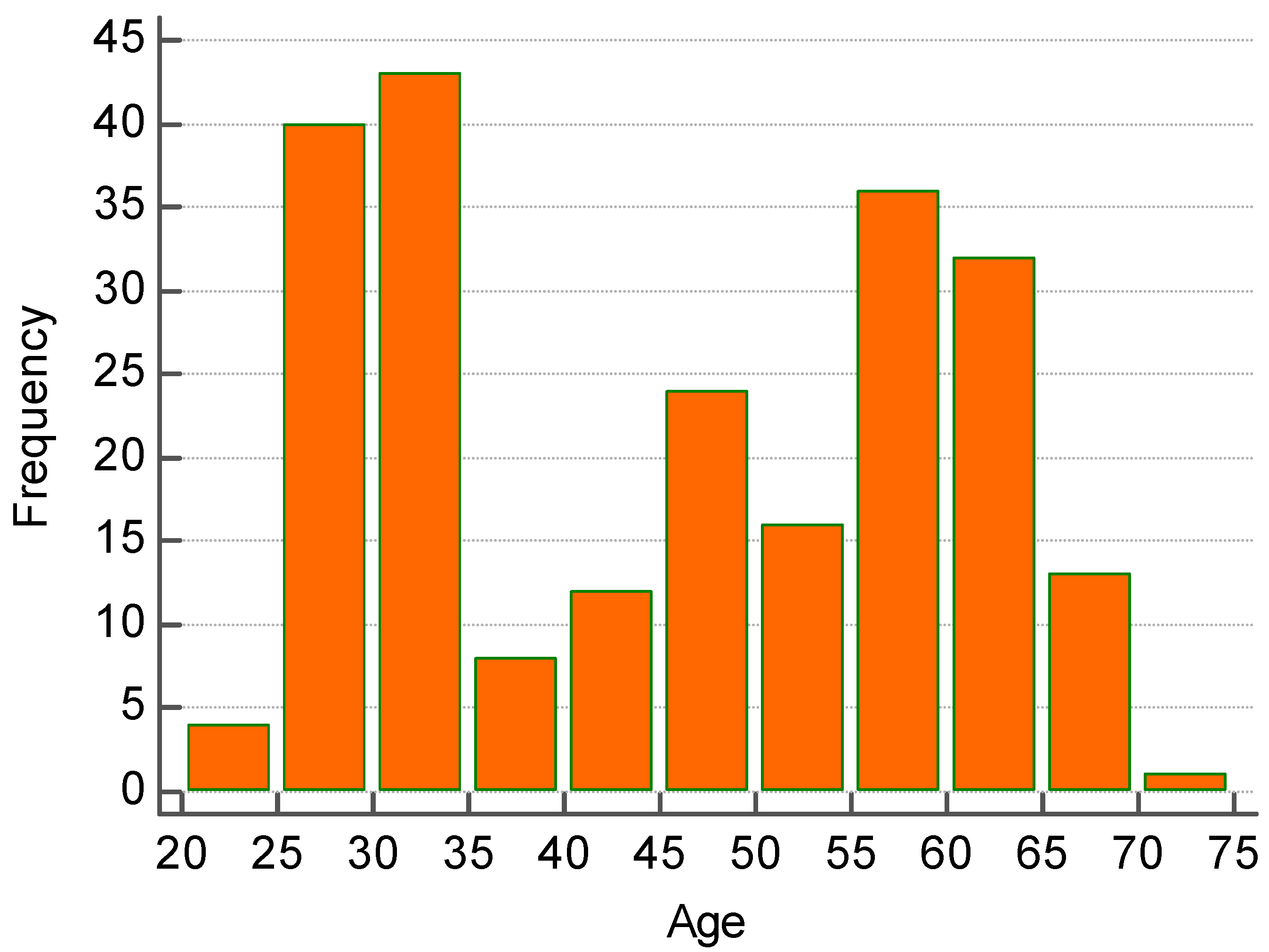
- Between the age of 20 and 30 years old there were 45 subjects (19.57% of 230 enrolled).
- Between the age of 30 and 40 years old there were 52 subjects (22.61% of 230 enrolled)
- Between the age of 40 and 50 years old there were 34 subjects (14.78% of 230 enrolled).
- Between the age 50 and 60 years old there were 53 subjects (23.04% of 230 enrolled)
- Between the age of 60 and 70 years of age there were 46 subjects (20% of 230 enrolled).
3.1. Statistical Findings
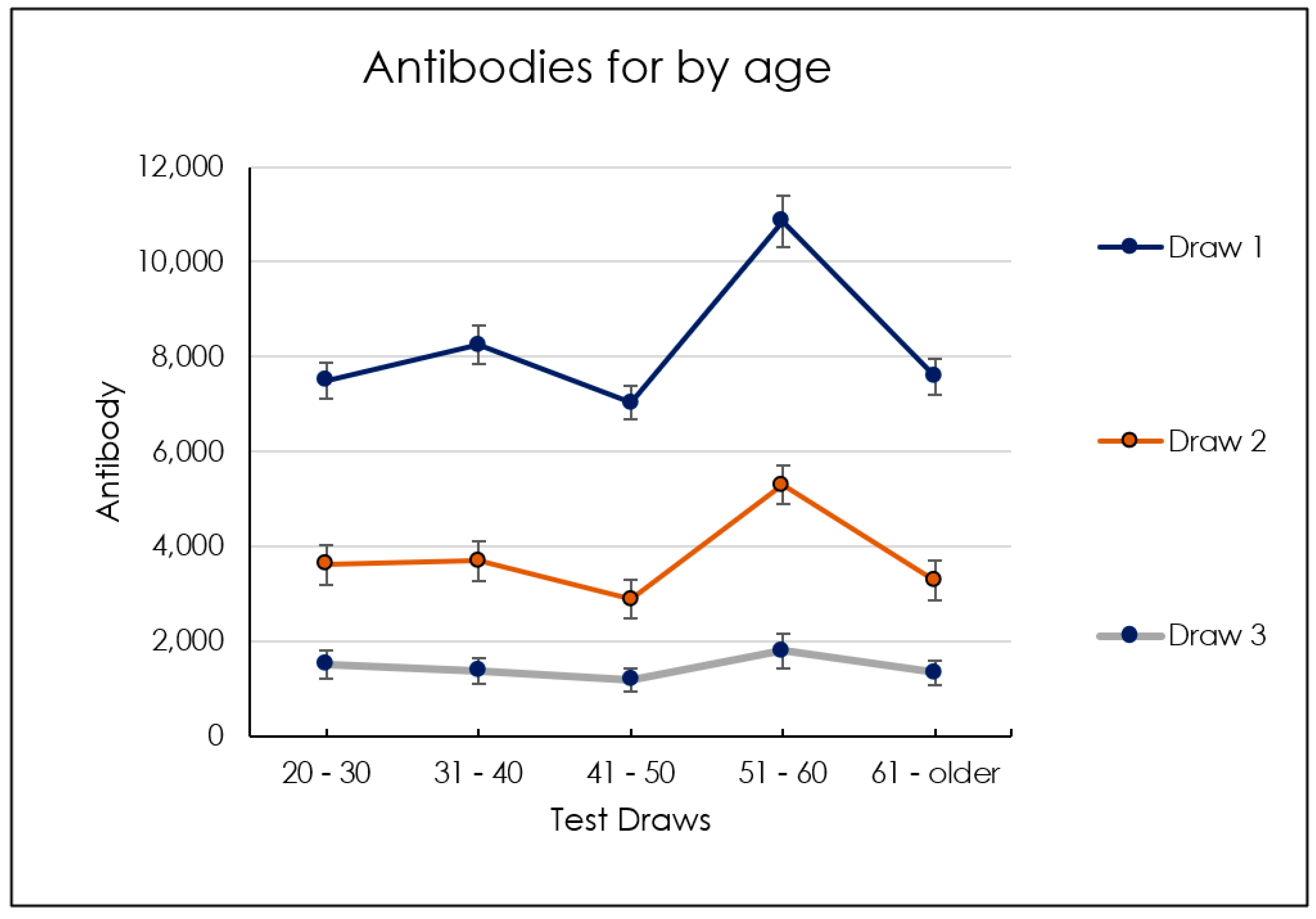
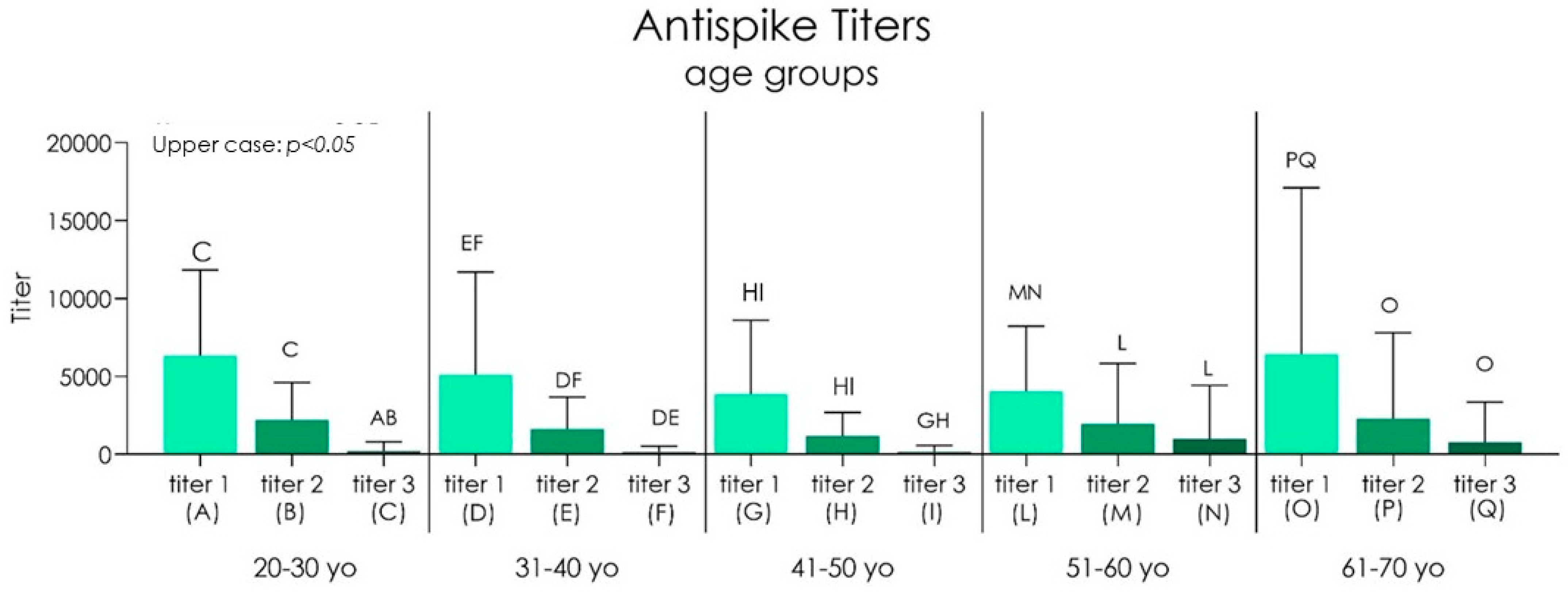
3.1.1. Age-Related Findings
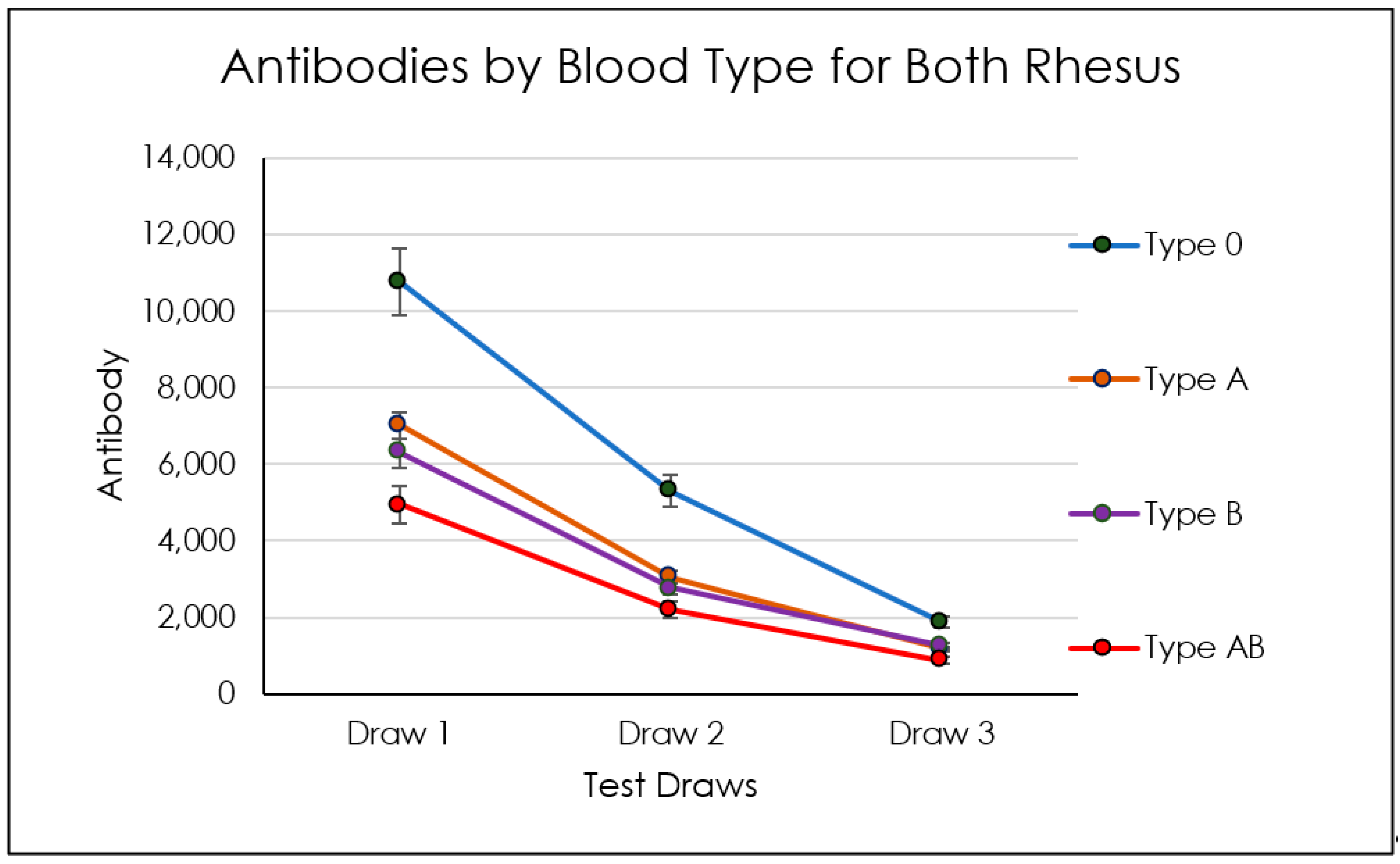
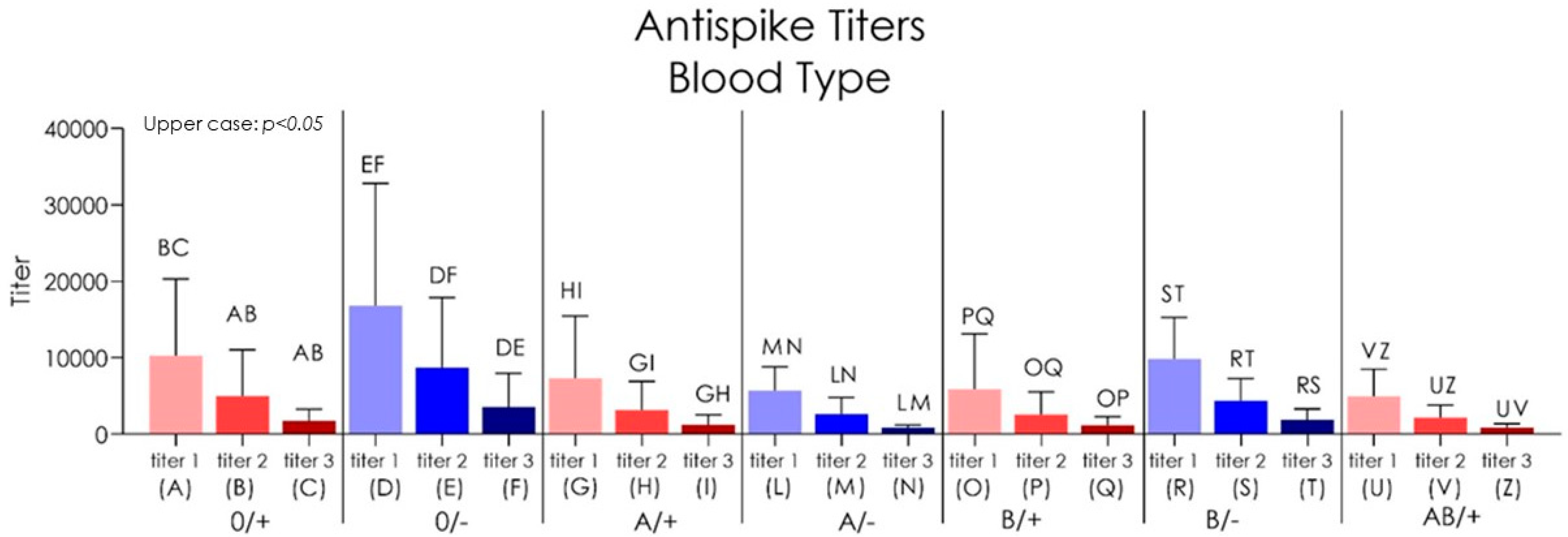
3.1.2. Blood-Type-Related Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE2 | angiotensin-converting enzyme-2 |
| ACE | angiotensin-converting enzyme |
| ACE1 | angiotensin-converting enzyme 1 |
| AIFA | Agenzia Italiana del Farmaco |
| Alfa | English variant B.1.1.7 |
| anti-RBD IgG | Immunogloublin G anti receptor-binding domain |
| Antispike | Test IgG Antispike |
| BAU | unità arbitrarie vincolanti |
| Beta variant | (former of South Africa) |
| BMI | Body mass index |
| CI | Interval of confidence |
| CLIAs | chemiluminescence immunoassay |
| CRP | C-reactive protein |
| Delta | Indian variant B.1.617.2 |
| ELISA | enzyme-linked immunosorbent assay |
| EMA | European Medicines Agency |
| ETA | variant B.1.525; Date of designation March 2021 |
| Gamma | Brasilian variant P.1 |
| hACE2 receptor | human angiotensin I-converting enzyme 2 receptor |
| IFN | Interferon |
| IgA | Immunoglobulins A |
| IgG | Immunoglobulins G |
| IgM | Immunoglobulins M |
| IOTA | variant B.1.526; earliest documented samples USA (November 2020), Date of designation March 2021 |
| IQR | Interquartile range |
| KAPPA | Indian variant B.1.617.1 |
| LAMBA | variant C.37; earliest documented samples Peru (August 2020), Date of designation June 2021 |
| LFIAs | lateral flow immunoassays. |
| MERS | Middle East Respiratory Syndrome |
| MMF | mycophenolate mofetil |
| MPA | mycophenolic acid |
| MPPDH | inosine-5’-monophosphate dehydrogenase |
| NAAT | nucleic acid amplification test |
| NGS | Next Generation Sequencing |
| bNAbs | Broadly neutralizing antibodies |
| N-IgG | Anti-N-IgG |
| PRD | Viral Prion-like domain |
| RBD | receptor-binding domain |
| RBDs | receptor-binding domains |
| RDB-IgG | receptor-binding domain neutralizing antibodies |
| RT-PCR | real-time PCR Polymerase chain reaction |
| S | the Spike glycoprotein |
| SARS-CoV-1 | Severe Acute Respiratory Syndrome Coronavirus 1 |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 (COVID-19) |
| SARSr-CoV Rp3 | salivar protein similar to fused 8a and 8b SARS-CoV Beta Coronavirus |
| S-IgG | Antispike IgG |
| thio-NAD | thionicotinamide-adenine dinucleotide |
| TNF | Tumor Necrosis Factor |
| VIPIT | prothrombotic immune thrombocytopenia |
| VOC | Variants of Concern |
| VOI | Variants of Interest |
| ZETA | variant P.2 |
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Buonanno, G.; Stabile, L.; Morawska, L. Estimation of Airborne Viral Emission: Quanta Emission Rate of SARS-CoV-2 for Infection Risk Assessment. Environ. Int. 2020, 141, 105794. [Google Scholar] [CrossRef] [PubMed]
- Meselson, M. Droplets and Aerosols in the Transmission of SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2063. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the COVID-19 Pandemic: A Narrative Insight. BioMed Res. Int. 2020, 2020, 8896812. [Google Scholar] [CrossRef] [PubMed]
- Isha, S.N.; Ahmad, A.; Kabir, R.; Apu, E.H. Dental Clinic Architecture Prevents COVID-19-like Infectious Diseases. HERD Health Environ. Res. Des. J. 2020, 13, 240–241. [Google Scholar] [CrossRef]
- Xie, X.; Li, Y.; Sun, H.; Liu, L. Exhaled Droplets Due to Talking and Coughing. J. R. Soc. Interface 2009, 6 (Suppl. 6), S703–S714. [Google Scholar] [CrossRef] [PubMed]
- Somsen, G.A.; van Rijn, C.; Kooij, S.; Bem, R.A.; Bonn, D. Small Droplet Aerosols in Poorly Ventilated Spaces and SARS-CoV-2 Transmission. Lancet Respir. Med. 2020, 8, 658–659. [Google Scholar] [CrossRef]
- Karahan, S.; Katkat, F. Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey. J. Nutr. Health Aging 2021, 25, 189–196. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Fontes-Garfias, C.R.; Swanson, K.A.; Cai, H.; Sarkar, R.; Chen, W.; Cutler, M.; et al. Neutralizing Activity of BNT162b2-Elicited Serum—Preliminary Report. N. Engl. J. Med. 2021, 384, 1466–1468. [Google Scholar] [CrossRef]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses during Infection by SARS-CoV-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Balzanelli, G.M.; Distratis, P.; Aityan, S.K.; Amatulli, F.; Catucci, O.; Cefalo, A.; Dipalma, G.; Inchingolo, F.; Lazzaro, R.; Nguyen, K.C.D.; et al. COVID-19 and COVID-like Patients: A Brief Analysis and Findings of Two Deceased Cases. Open Access Maced. J. Med. Sci. 2020, 8, 490–495. [Google Scholar] [CrossRef]
- Tetz, G.; Tetz, V. Prion-Like Domains in Spike Protein of SARS-CoV-2 Differ across Its Variants and Enable Changes in Affinity to ACE2. Microorganisms 2022, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations Among Adults Without Immunocompromising Conditions—United States, March–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.L.; Lutrick, K.; et al. Prevention and Attenuation of COVID-19 with the BNT162b2 and MRNA-1273 Vaccines. N. Engl. J. Med. 2021, 385, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Naioti, E.A.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; et al. Sustained Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Associated Hospitalizations Among Adults—United States, March–July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Nanduri, S.; Pilishvili, T.; Derado, G.; Soe, M.M.; Dollard, P.; Wu, H.; Li, Q.; Bagchi, S.; Dubendris, H.; Link-Gelles, R.; et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines in Preventing SARS-CoV-2 Infection Among Nursing Home Residents Before and During Widespread Circulation of the SARS-CoV-2 B.1.617.2 (Delta) Variant—National Healthcare Safety Network, 1 March–1 August 2021. MMWR Morb Mortal Wkly. Rep. 2021, 70, 1163–1166. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. The Impact of SARS-CoV-2 Vaccination on Alpha & Delta Variant Transmission. medRxiv 2021. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Janeway, C.A., Jr.; Travers, P.; Walport, M.; Shlomchik, M.J. Immunobiology: The Immune System in Health and Disease, 5th ed.; Garland Science: New York, NY, USA, 2001. [Google Scholar]
- William, P.E. Fundamental Immunology, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003. [Google Scholar]
- Humphrey, J.H.; White, R.G. Immunology for Students of Medicine, 3rd ed.; Humphrey, J.H.; White, R.G. Blackwell Scientific: Oxford, UK, 1970; pp. 65–100. [Google Scholar]
- Webster, A.D. Primary Immunodeficiency. Hum. Exp. Toxicol. 1995, 14, 99–100. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; Cefalo, A.; Catucci, O.; Aityan, S.K.; Dipalma, G.; Vimercati, L.; Inchingolo, A.D.; Maggiore, M.E.; et al. The Vitamin D, IL-6 and the EGFR Markers a Possible Way to Elucidate the Lung–Heart–Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion. Microorganisms 2021, 9, 1903. [Google Scholar] [CrossRef] [PubMed]
- Phan, D.Q.; Nguyen, L.D.N.; Pham, S.T.; Nguyen, T.; Pham, P.T.T.; Nguyen, S.T.H.; Pham, D.T.; Pham, H.T.; Tran, D.K.; Le, S.H.; et al. The Distribution of Dengue Virus Serotype in Quang Nam Province (Vietnam) during the Outbreak in 2018. Int. J. Environ. Res. Public Health 2022, 19, 1285. [Google Scholar] [CrossRef] [PubMed]
- Maglione, M.; Bevilacqua, L.; Dotto, F.; Costantinides, F.; Lorusso, F.; Scarano, A. Observational Study on the Preparation of the Implant Site with Piezosurgery vs. Drill: Comparison between the Two Methods in Terms of Postoperative Pain, Surgical Times, and Operational Advantages. BioMed Res. Int. 2019, 2019, 8483658. [Google Scholar] [CrossRef] [PubMed]
- Interim Statement on Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 6 November 2021).
- CDC. CDC COVID-19 Booster Shot. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 6 November 2021).
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during COVID-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [PubMed]
- Booster Shots and Third Doses for COVID-19 Vaccines: What You Need to Know. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/booster-shots-and-third-doses-for-covid19-vaccines-what-you-need-to-know (accessed on 6 November 2021).
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Santacroce, L.; Marinelli, G.; Mancini, A.; Vimercati, L.; Maggiore, M.E.; D’Oria, M.T.; Hazballa, D.; et al. COVID-19 Infection in Children, Infants and Pregnant Subjects: An Overview of Recent Insights and Therapies. Microorganisms 2021, 9, 1964. [Google Scholar] [CrossRef]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Vito, D.D.; Saini, R.; Inchingolo, F. Probiotics Improve Urogenital Health in Women. Open Access Maced. J. Med. Sci. 2018, 6, 1845–1850. [Google Scholar] [CrossRef]
- Santacroce, L.; Inchingolo, F.; Topi, S.; Del Prete, R.; Di Cosola, M.; Charitos, I.A.; Montagnani, M. Potential Beneficial Role of Probiotics on the Outcome of COVID-19 Patients: An Evolving Perspective. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 295–301. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. BNT162b2 Vaccine Booster Dose Protection: A Nationwide Study from Israel. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Shapiro Ben David, S.; Shamir-Stein, N.; Baruch Gez, S.; Lerner, U.; Rahamim-Cohen, D.; Ekka Zohar, A. Reactogenicity of a Third BNT162b2 MRNA COVID-19 Vaccine among Immunocompromised Individuals and Seniors—A Nationwide Survey. Clin. Immunol. 2021, 232, 108860. [Google Scholar] [CrossRef]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Bozman, D.-F.; Hanafi, L.; Faucon, A.-L.; Housset, P. SARS-CoV-2 Antibody Response After a Third Dose of the BNT162b2 Vaccine in Patients Receiving Maintenance Hemodialysis or Peritoneal Dialysis. Am. J. Kidney Dis. 2021, 79, 185–192.e1. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Dipalma, G.; Vimercati, L.; Catucci, O.; Amatulli, F.; Cefalo, A.; Lazzaro, R.; Palazzo, D.; Aityan, S.K.; et al. Immunity Profiling of COVID-19 Infection, Dynamic Variations of Lymphocyte Subsets, a Comparative Analysis on Four Different Groups. Microorganisms 2021, 9, 2036. [Google Scholar] [CrossRef]
- Vomero, M.; Barbati, C.; Colasanti, T.; Celia, A.I.; Speziali, M.; Ucci, F.M.; Ciancarella, C.; Conti, F.; Alessandri, C. Autophagy Modulation in Lymphocytes From COVID-19 Patients: New Therapeutic Target in SARS-CoV-2 Infection. Front. Pharmacol. 2020, 11, 569849. [Google Scholar] [CrossRef] [PubMed]
- Bordea, I.R.; Xhajanka, E.; Candrea, S.; Bran, S.; Onișor, F.; Inchingolo, A.D.; Malcangi, G.; Pham, V.H.; Inchingolo, A.M.; Scarano, A.; et al. Coronavirus (SARS-CoV-2) Pandemic: Future Challenges for Dental Practitioners. Microorganisms 2020, 8, 1704. [Google Scholar] [CrossRef] [PubMed]
- Bellocchio, L.; Bordea, I.R.; Ballini, A.; Lorusso, F.; Hazballa, D.; Isacco, C.G.; Malcangi, G.; Inchingolo, A.D.; Dipalma, G.; Inchingolo, F.; et al. Environmental Issues and Neurological Manifestations Associated with COVID-19 Pandemic: New Aspects of the Disease? Int J. Environ. Res. Public Health 2020, 17, 8049. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.S.; Kim, W.; Kalaidina, E.; Goss, C.W.; Rauseo, A.M.; Schmitz, A.J.; Hansen, L.; Haile, A.; Klebert, M.K.; Pusic, I.; et al. SARS-CoV-2 Infection Induces Long-Lived Bone Marrow Plasma Cells in Humans. Nature 2021, 595, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Algaissi, A.; Alfaleh, M.A.; Hala, S.; Abujamel, T.S.; Alamri, S.S.; Almahboub, S.A.; Alluhaybi, K.A.; Hobani, H.I.; Alsulaiman, R.M.; AlHarbi, R.H.; et al. SARS-CoV-2 S1 and N-Based Serological Assays Reveal Rapid Seroconversion and Induction of Specific Antibody Response in COVID-19 Patients. Sci Rep. 2020, 10, 16561. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Aityan, S.K.; Amatulli, F.; Catucci, O.; Cefalo, A.; De Michele, A.; Dipalma, G.; Inchingolo, F.; Lazzaro, R.; et al. An Alternative “Trojan Horse” Hypothesis for COVID-19: Immune Deficiency of IL-10 and SARS-CoV-2 Biology. Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 1–5. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease Adjuvant Therapies and Supplements Breakthrough for the Infection Prevention. Microorganisms 2021, 9, 525. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Dipalma, G.; Inchingolo, A.M.; Malcangi, G.; Santacroce, L.; D’oria, M.T.; Isacco, C.G.; Bordea, I.R.; Candrea, S.; Scarano, A.; et al. The 15-Months Clinical Experience of SARS-CoV-2: A Literature Review of Therapies and Adjuvants. Antioxidants 2021, 10, 881. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Qorri, E.; Converti, I.; Lorusso, F.; Delvecchio, M.; Gnoni, A.; Scacco, S.; Scarano, A. Inflammatory Status and Glycemic Control Level of Patients with Type 2 Diabetes and Periodontitis: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3018. [Google Scholar] [CrossRef]
- Corsalini, M.; Di Venere, D.; Sportelli, P.; Magazzino, D.; Ripa, C.; Cantatore, F.; Cagnetta, G.; De Rinaldis, C.; Montemurro, N.; De Giacomo, A. Evaluation of prosthetic quality and masticatory efficiency in patients with total removable prosthesis study of 12 cases. ORAL Implantol. 2018, 11, 230–240. [Google Scholar]
- Grassi, F.R.; Grassi, R.; Rapone, B.; Alemanno, G.; Balena, A.; Kalemaj, Z.; Gianfranco, A. Dimensional Changes of Buccal Bone Plate in Immediate Implants Inserted through Open Flap, Open Flap and Bone Grafting and Flapless Techniques: A Cone-Beam Computed Tomography Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2019, 30, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Quaglia, E.; Moscufo, L.; Corsalini, M.; Coscia, D.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Rapone, B.; Carossa, M.; Carossa, S. Polyamide vs Silk Sutures in the Healing of Postextraction Sockets: A Split Mouth Study. Oral Implantol. 2018, 11, 115–120. [Google Scholar]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Cesarano, F.; Arazzi, M.; Liberato, L.D.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Periodontal Microbiological Status Influences the Occurrence of Cyclosporine-A and Tacrolimus-Induced Gingival Overgrowth. Antibiotics 2019, 8, 124. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Converti, I.; Santacroce, L.; Cesarano, F.; Vecchiet, F.; Cacchio, L.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Impact of Periodontal Inflammation on Nutrition and Inflammation Markers in Hemodialysis Patients. Antibiotics 2019, 8, 209. [Google Scholar] [CrossRef]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Corsalini, M.; Di Venere, D.; Carossa, M.; Ripa, M.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Di Santantonio, G.; Lenoci, G.; Barile, G. Comparative clinical study between zirconium-ceramic and metal-ceramic fixed rehabilitations. ORAL Implantol. 2018, 11, 150–160. [Google Scholar]
- Baum, A.; Fulton, B.O.; Wloga, E.; Copin, R.; Pascal, K.E.; Russo, V.; Giordano, S.; Lanza, K.; Negron, N.; Ni, M.; et al. Antibody Cocktail to SARS-CoV-2 Spike Protein Prevents Rapid Mutational Escape Seen with Individual Antibodies. Science 2020, 369, 1014–1018. [Google Scholar] [CrossRef]
- Schäfer, A.; Muecksch, F.; Lorenzi, J.C.C.; Leist, S.R.; Cipolla, M.; Bournazos, S.; Schmidt, F.; Maison, R.M.; Gazumyan, A.; Martinez, D.R.; et al. Antibody Potency, Effector Function and Combinations in Protection from SARS-CoV-2 Infection in Vivo. J. Exp. Med. 2021, 218, e20201993. [Google Scholar] [CrossRef]
- Charitos, I.A.; Del Prete, R.; Inchingolo, F.; Mosca, A.; Carretta, D.; Ballini, A.; Santacroce, L. What We Have Learned for the Future about COVID-19 and Healthcare Management of It? Acta Biomed. 2020, 91, e2020126. [Google Scholar] [PubMed]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Scacco, S.; Perillo, L.; Scarano, A.; Aityan, S.K.; Contaldo, M.; Cd Nguyen, K.; Santacroce, L.; Syed, J.; et al. A Comparative Study on Different Stemness Gene Expression between Dental Pulp Stem Cells vs. Dental Bud Stem Cells. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1626–1633. [Google Scholar] [CrossRef]
- Rapone, B.; Corsalini, M.; Converti, I.; Loverro, M.T.; Gnoni, A.; Trerotoli, P.; Ferrara, E. Does Periodontal Inflammation Affect Type 1 Diabetes in Childhood and Adolescence? A Meta-Analysis. Front. Endocrinol 2020, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 5467. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.G.; Distratis, P.; Catucci, O.; Cefalo, A.; Lazzaro, R.; Inchingolo, F.; Tomassone, D.; Aityan, S.K.; Ballini, A.; Nguyen, K.C.D.; et al. Mesenchymal Stem Cells: The Secret Children’s Weapons against the SARS-CoV-2 Lethal Infection. Appl. Sci. 2021, 11, 1696. [Google Scholar] [CrossRef]
- Bemark, M.; Hazanov, H.; Strömberg, A.; Komban, R.; Holmqvist, J.; Köster, S.; Mattsson, J.; Sikora, P.; Mehr, R.; Lycke, N.Y. Limited Clonal Relatedness between Gut IgA Plasma Cells and Memory B Cells after Oral Immunization. Nat. Commun. 2016, 7, 12698. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; Connors, T.J.; Zhu, Y.; Baldwin, M.R.; Lin, W.-H.; Wontakal, S.; Szabo, P.A.; Wells, S.B.; Dogra, P.; Gray, J.; et al. Distinct Antibody Responses to SARS-CoV-2 in Children and Adults across the COVID-19 Clinical Spectrum. Nat. Immunol. 2021, 22, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Facial Skin Temperature and Discomfort When Wearing Protective Face Masks: Thermal Infrared Imaging Evaluation and Hands Moving the Mask. Int. J. Environ. Res. Public Health 2020, 17, 4624. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Rapone, B.; Festa, F.; Tari, S.R.; Lorusso, F. Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery. Int. J. Environ. Res. Public Health 2021, 18, 2363. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, F.; Inchingolo, F.; Scarano, A. The Impact of The Novel COVID-19 on the Scientific Production Spread: A Five-Month Bibliometric Report of The Worldwide Research Community. Acta Med. Mediterr. 2020, 36, 3357–3360. [Google Scholar]
- Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; D’Ettorre, E.; Nico, A.; Inchingolo, F.; Dipalma, G.; Tomassone, D.; Serlenga, E.M.; Dalagni, G.; et al. New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient. J. Pers. Med. 2022, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.G.; Distratis, P.; Dipalma, G.; Vimercati, L.; Inchingolo, A.D.; Lazzaro, R.; Aityan, S.K.; Maggiore, M.E.; Mancini, A.; Laforgia, R.; et al. SARS-CoV-2 Virus Infection May Interfere CD34+ Hematopoietic Stem Cells and Megakaryocyte–Erythroid Progenitors Differentiation Contributing to Platelet Defection towards Insurgence of Thrombocytopenia and Thrombophilia. Microorganisms 2021, 9, 1632. [Google Scholar] [CrossRef] [PubMed]
- Stera, G.; Pierantoni, L.; Masetti, R.; Leardini, D.; Biagi, C.; Buonsenso, D.; Pession, A.; Lanari, M. Impact of SARS-CoV-2 Pandemic on Bronchiolitis Hospitalizations: The Experience of an Italian Tertiary Center. Children 2021, 8, 556. [Google Scholar] [CrossRef] [PubMed]
- Charitos, I.A.; Ballini, A.; Bottalico, L.; Cantore, S.; Passarelli, P.C.; Inchingolo, F.; D’Addona, A.; Santacroce, L. Special Features of SARS-CoV-2 in Daily Practice. World J. Clin. Cases 2020, 8, 3920–3933. [Google Scholar] [CrossRef]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.-H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally Enhanced Neutralizing Breadth against SARS-CoV-2 One Year after Infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 418–421; author reply 421–422. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Charrier, J.-B. Selecting a Relevant in Vitro Cell Model for Testing and Comparing the Effects of a Choukroun’s Platelet-Rich Fibrin (PRF) Membrane and a Platelet-Rich Plasma (PRP) Gel: Tricks and Traps. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2010, 110, 409–411. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Qorri, E.; Dipalma, G.; Mancini, A.; Corsalini, M.; Fabbro, M.D.; Scarano, A.; Tartaglia, G.M.; Inchingolo, F. The Impact of Periodontal Inflammation on Endothelial Function Assessed by Circulating Levels of Asymmetric Dimethylarginine: A Single-Blinded Randomized Clinical Trial. J. Clin. Med. 2022, 11, 4173. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Lorusso, F.; Noumbissi, S. Infrared Thermographic Evaluation of Temperature Modifications Induced during Implant Site Preparation with Steel vs. Zirconia Implant Drill. J. Clin. Med. 2020, 9, 148. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological Memory to SARS-CoV-2 Assessed for up to 8 Months after Infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Rana, R.; Ranjan, V.; Kumar, N. Association of ABO and Rh Blood Group in Susceptibility, Severity, and Mortality of Coronavirus Disease 2019: A Hospital-Based Study from Delhi, India. Front. Cell Infect. Microbiol. 2021, 11, 767771. [Google Scholar] [CrossRef]
- Janda, A.; Engel, C.; Remppis, J.; Enkel, S.; Peter, A.; Hörber, S.; Ganzenmueller, T.; Schober, S.; Weinstock, C.; Jacobsen, E.-M.; et al. Role of ABO Blood Group in SARS-CoV-2 Infection in Households. Front. Microbiol. 2022, 13, 857965. [Google Scholar] [CrossRef] [PubMed]
- Shachor-Meyouhas, Y.; Hussein, K.; Dabaja-Younis, H.; Szwarcwort-Cohen, M.; Almog, R.; Weissman, A.; Mekel, M.; Hyams, G.; Horowitz, N.A.; Gepstein, V.; et al. Immunogenicity Trends 1 and 3 Months after Second BNT162B2 Vaccination among Healthcare Workers in Israel. Clin. Microbiol Infect. 2021, 28, 450.e1–450.e4. [Google Scholar] [CrossRef]
- Israel, A.; Shenhar, Y.; Green, I.; Merzon, E.; Golan-Cohen, A.; Schäffer, A.A.; Ruppin, E.; Vinker, S.; Magen, E. Large-Scale Study of Antibody Titer Decay Following BNT162b2 MRNA Vaccine or SARS-CoV-2 Infection. medRxiv 2021, 10, 64. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Burnham, E.L.; Janssen, W.J.; Riches, D.W.H.; Moss, M.; Downey, G.P. The Fibroproliferative Response in Acute Respiratory Distress Syndrome: Mechanisms and Clinical Significance. Eur. Respir. J. 2014, 43, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Doykov, I.; Hällqvist, J.; Gilmour, K.C.; Grandjean, L.; Mills, K.; Heywood, W.E. ‘The Long Tail of COVID-19’—The Detection of a Prolonged Inflammatory Response after a SARS-CoV-2 Infection in Asymptomatic and Mildly Affected Patients. F1000Research 2020, 9, 1349. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, G.; De Michele, L.; De Ceglie, M.; Pierucci, P.; Mirabile, A.; Vita, M.; Palmieri, V.O.; Carpagnano, G.E.; Scardapane, A.; D’Agostino, C. Lung Ultrasonography for Long-Term Follow-up of COVID-19 Survivors Compared to Chest CT Scan. Respir. Med. 2021, 181, 106384. [Google Scholar] [CrossRef]
- Vimercati, L.; Maria, L.D.; Quarato, M.; Caputi, A.; Gesualdo, L.; Migliore, G.; Cavone, D.; Sponselli, S.; Pipoli, A.; Inchingolo, F.; et al. Association between Long COVID and Overweight/Obesity. J. Clin. Med. 2021, 10, 4143. [Google Scholar] [CrossRef] [PubMed]
- Nath, A. Long-Haul COVID. Neurology 2020, 95, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Silva Andrade, B.; Siqueira, S.; de Assis Soares, W.R.; de Souza Rangel, F.; Santos, N.O.; dos Santos Freitas, A.; Ribeiro da Silveira, P.; Tiwari, S.; Alzahrani, K.J.; Góes-Neto, A.; et al. Long-COVID and Post-COVID Health Complications: An Up-to-Date Review on Clinical Conditions and Their Possible Molecular Mechanisms. Viruses 2021, 13, 700. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and Its Microbiome at a Glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-Acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Belizário, J.E.; Faintuch, J. Microbiome and Gut Dysbiosis. Exp. Suppl. 2018, 109, 459–476. [Google Scholar] [CrossRef] [PubMed]
- Hornef, M. Pathogens, Commensal Symbionts, and Pathobionts: Discovery and Functional Effects on the Host. ILAR J. 2015, 56, 159–162. [Google Scholar] [CrossRef]
- Sun, J.; Xiao, J.; Sun, R.; Tang, X.; Liang, C.; Lin, H.; Zeng, L.; Hu, J.; Yuan, R.; Zhou, P.; et al. Prolonged Persistence of SARS-CoV-2 RNA in Body Fluids. Emerg. Infect. Dis. 2020, 26, 1834–1838. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Blood Types | |||
|---|---|---|---|
| Titer 1 | Titer 2 | Titer 3 | |
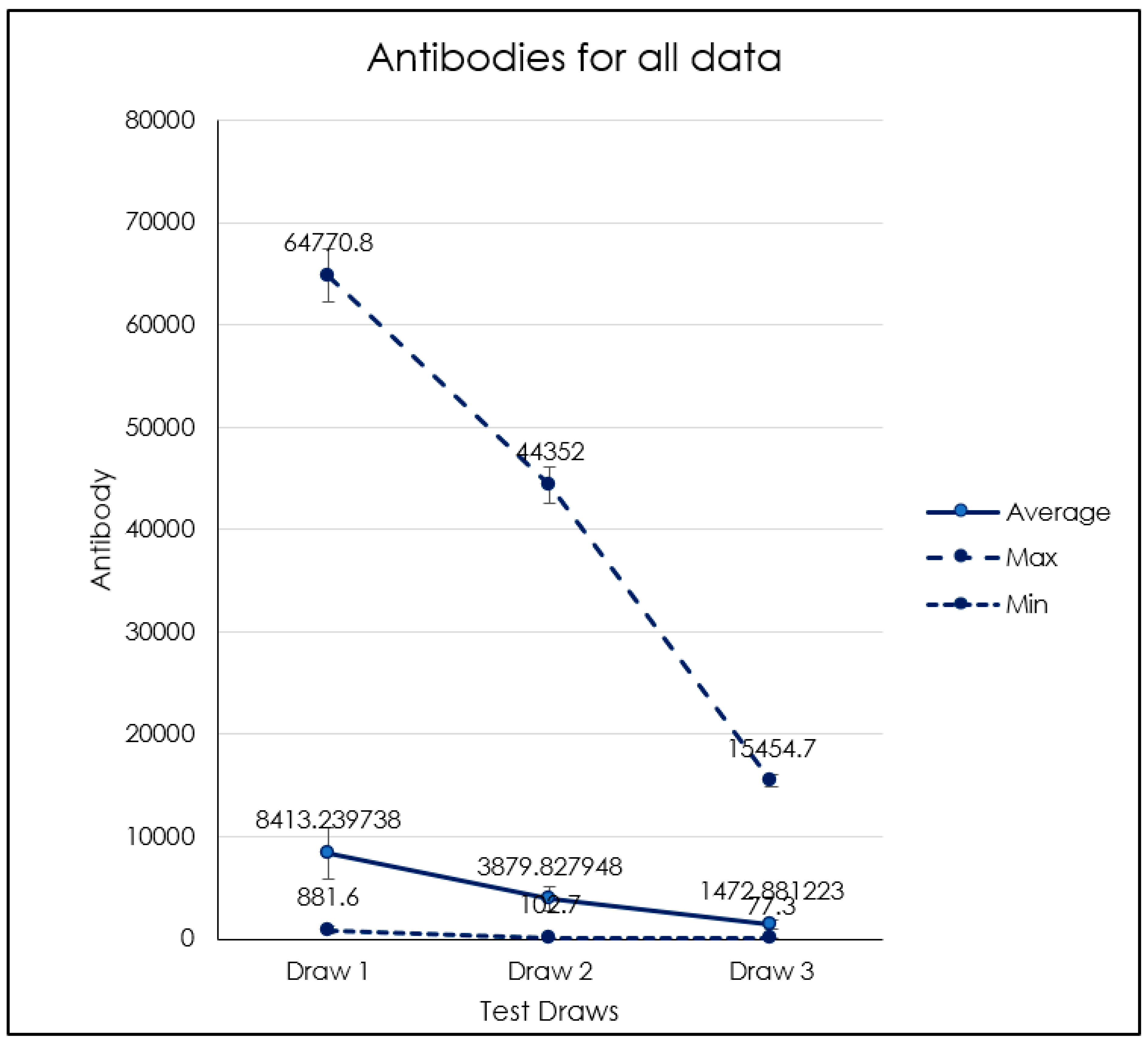
| Average | 8.413 | 3.880 | 1.473 |
| St.Dev | 9.510 | 5.156 | 1.818 |
| Max | 64.771 | 44.352 | 15.455 |
| Min | 882 | 103 | 77 |
| Range: | 63.889 | 44.249 | 15.377 |
| # Patients | 229 | ||
| Titer 1,2 | Titer 2,3 | Titer 1–3 | |
| Correlation | 0.97 | 0.80 | 0.81 |
| Ages Related Blood Types | |||
|---|---|---|---|
| Titer 1 | Titer 2 | Titer 3 | |
| Average | 8.413 | 3.880 | 1.473 |
| St.Dev | 9.510 | 5.156 | 1.818 |
| Max | 64.771 | 44.352 | 15.455 |
| Min | 882 | 103 | 77 |
| Range: | 63.889 | 44.249 | 15.377 |
| # Patients | 229 | ||
| Titer 1,2 | Titer 2,3 | Titer 1–3 | |
| Correlation | 0.97 | 0.80 | 0.81 |
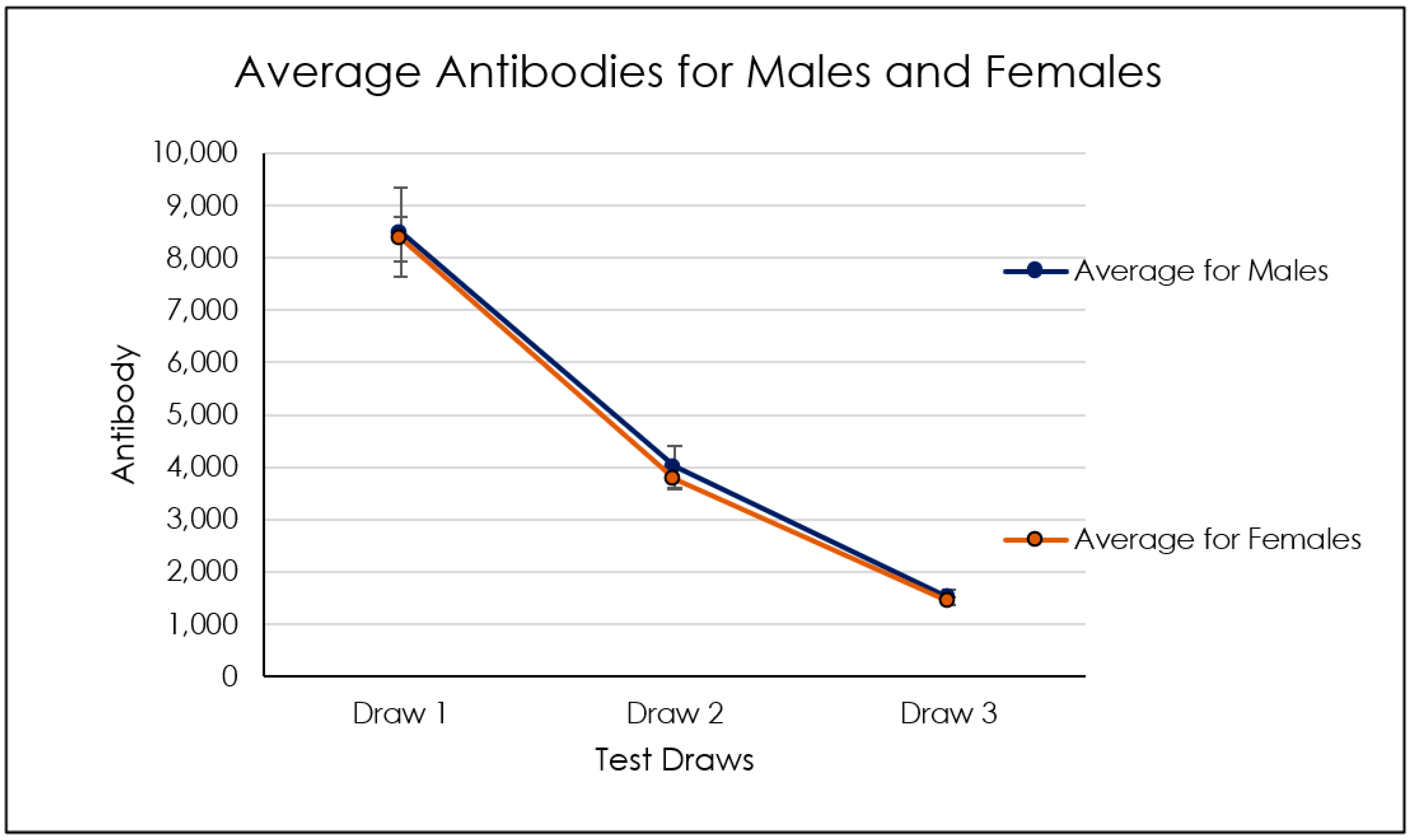
| Genders Referred Blood Types | |||
|---|---|---|---|
| Titer 1 | Titer 2 | Titer 3 | |
| Average | 8.413 | 3.880 | 1.473 |
| St.Dev | 9.510 | 5.156 | 1.818 |
| Max | 64.771 | 44.352 | 15.455 |
| Min | 882 | 103 | 77 |
| Range: | 63.889 | 44.249 | 15.377 |
| # Patients | 229 | ||
| Titer 1,2 | Titer 2,3 | Titer 1–3 | |
| Correlation | 0.97 | 0.80 | 0.81 |
| Group I 20–30 yo | Group II 31–40 yo | Group III 41–50 yo | Group IV 51–60 yo | Group V 61–70 yo | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| titer 1 | titer 2 | titer 3 | titer 1 | titer 2 | titer 3 | titer 1 | titer 2 | titer 3 | titer 1 | titer 2 | titer 3 | titer 1 | titer 2 | titer 3 | |
| Mean | 6342 | 2207 | 207.6 | 5118 | 1628 | 151.3 | 3871 | 1172 | 169.0 | 4046 | 1963 | 1010 | 6438 | 2289 | 780.6 |
| SD | 5506 | 2397 | 599.8 | 6593 | 2041 | 377.0 | 4737 | 1522 | 414.3 | 4174 | 3872 | 3413 | 10673 | 5513 | 2578 |
| Lower 95% CI | 4668 | 1479 | 25.29 | 3264 | 1054 | 45.30 | 2243 | 657.3 | 28.83 | 2896 | 895.2 | 69.02 | 3269 | 670.2 | 23.75 |
| Upper 95% CI | 8016 | 2936 | 390.0 | 6972 | 2202 | 257.4 | 5498 | 1687 | 309.2 | 5197 | 3030 | 1951 | 9608 | 3907 | 1537 |
| 0/+ | 0/− | |||||
|---|---|---|---|---|---|---|
| Titer 1 | Titer 2 | Titer 3 | Titer 1 | Titer 2 | Titer 3 | |
| Mean | 10,289 | 5025 | 1739 | 16,810 | 8710 | 3561 |
| SD | 10,013 | 6024 | 1548 | 15,992 | 9160 | 4414 |
| Lower 95% CI of mean | 8001 | 3648 | 1385 | 27.84 | 903 | −1071 |
| Upper 95% CI | 12,577 | 6401 | 2093 | 33,593 | 18,322 | 8192 |
| A/+ | A/− | |||||
| Titer 1 | Titer 1 | Titer 1 | Titer 1 | Titer 2 | Titer 3 | |
| Mean | 7327 | 5717 | 5717 | 5717 | 8710 | 3561 |
| SD | 8160 | 3095 | 3095 | 3095 | 9160 | 4414 |
| Lower 95% CI of mean | 5008 | 3638 | 3638 | 3638 | 903 | −1071 |
| Upper 95% CI | 9646 | 7797 | 7797 | 7797 | 18,322 | 8192 |
| B/+ | B/− | |||||
| Titer 1 | Titer 2 | Titer 1 | Titer 2 | Titer 1 | Titer 2 | |
| Mean | 5867 | 2574 | 5867 | 2574 | 5867 | 2574 |
| SD | 7293 | 2965 | 7293 | 2965 | 7293 | 2965 |
| Lower 95% CI of mean | 2856 | 1350 | 2856 | 1350 | 2856 | 1350 |
| Upper 95% CI | 8877 | 3798 | 8877 | 3798 | 8877 | 3798 |
| AB/+ | ||||||
| Titer 1 | Titer 1 | Titer 1 | ||||
| Mean | 4945 | 4945 | 4945 | |||
| SD | 3577 | 3577 | 3577 | |||
| Lower 95% CI of mean | 2672 | 2672 | 2672 | |||
| Upper 95% CI | 7218 | 7218 | 7218 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.D.; Malcangi, G.; Ceci, S.; Patano, A.; Corriero, A.; Azzollini, D.; Marinelli, G.; Coloccia, G.; Piras, F.; Barile, G.; et al. Antispike Immunoglobulin-G (IgG) Titer Response of SARS-CoV-2 mRNA-Vaccine (BNT162b2): A Monitoring Study on Healthcare Workers. Biomedicines 2022, 10, 2402. https://doi.org/10.3390/biomedicines10102402
Inchingolo AD, Malcangi G, Ceci S, Patano A, Corriero A, Azzollini D, Marinelli G, Coloccia G, Piras F, Barile G, et al. Antispike Immunoglobulin-G (IgG) Titer Response of SARS-CoV-2 mRNA-Vaccine (BNT162b2): A Monitoring Study on Healthcare Workers. Biomedicines. 2022; 10(10):2402. https://doi.org/10.3390/biomedicines10102402
Chicago/Turabian StyleInchingolo, Alessio Danilo, Giuseppina Malcangi, Sabino Ceci, Assunta Patano, Alberto Corriero, Daniela Azzollini, Grazia Marinelli, Giovanni Coloccia, Fabio Piras, Giuseppe Barile, and et al. 2022. "Antispike Immunoglobulin-G (IgG) Titer Response of SARS-CoV-2 mRNA-Vaccine (BNT162b2): A Monitoring Study on Healthcare Workers" Biomedicines 10, no. 10: 2402. https://doi.org/10.3390/biomedicines10102402