
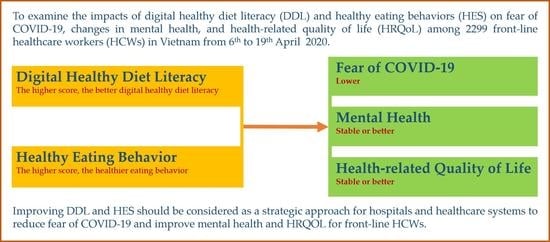
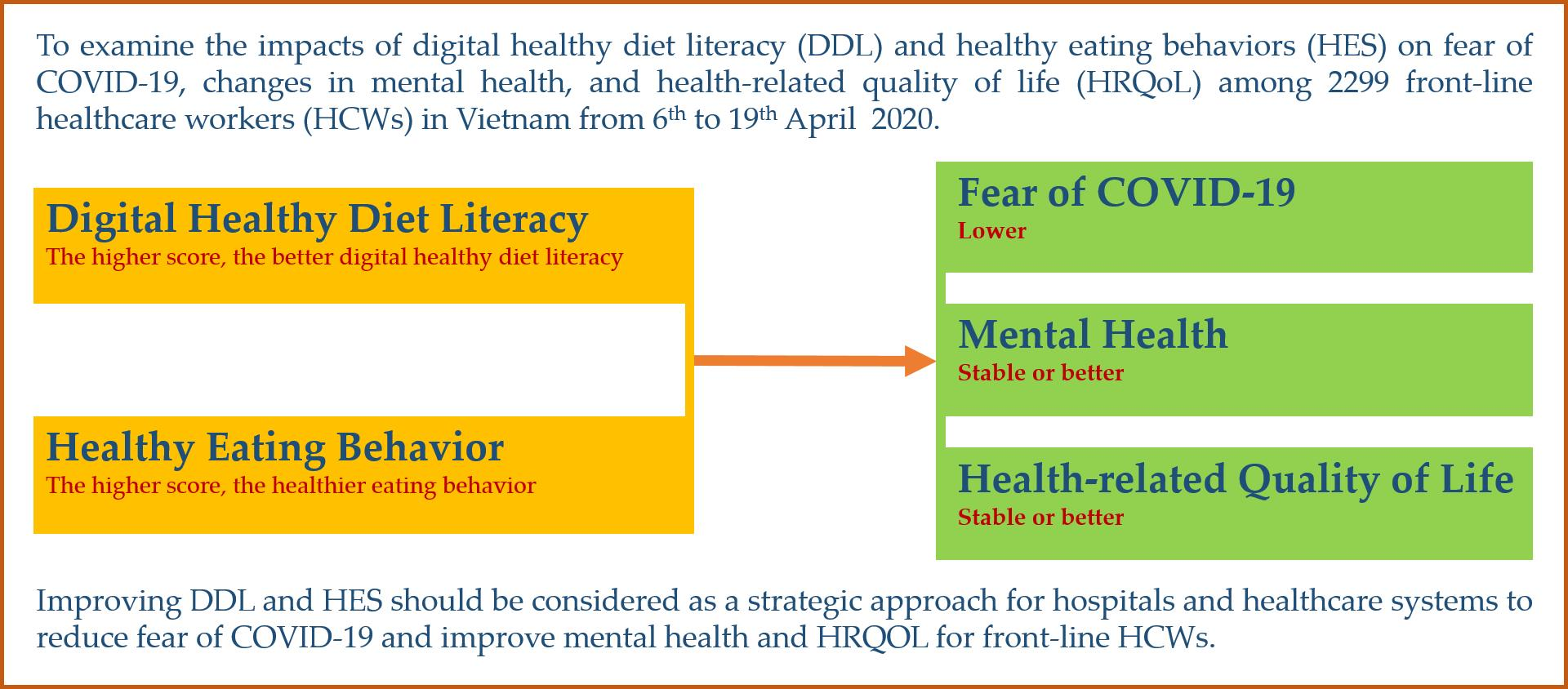
Impacts of Digital Healthy Diet Literacy and Healthy Eating Behavior on Fear of COVID-19, Changes in Mental Health, and Health-Related Quality of Life among Front-Line Health Care Workers


 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Participants’ Characteristics
2.2.2. Symptoms like COVID-19
2.2.3. Health Literacy and Digital Healthy Diet Literacy
2.2.4. eHealth Literacy Scale
2.2.5. Healthy Eating Behavior
2.2.6. Fear of COVID-19
2.2.7. Changes in Mental Health and Health-Related Quality of Life
2.3. Data Collection Procedure
2.4. Data Analysis
3. Results
3.1. Characteristics of Front-Line HCWs
3.2. Associated Factors of Fear of COVID-19
3.3. Associated Factors of Mental Health Changes
3.4. Associated Factors of HRQoL Changes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moitra, M.; Rahman, M.; Collins, P.Y.; Gohar, F.; Weaver, M.; Kinuthia, J.; Rössler, W.; Petersen, S.; Unutzer, J.; Saxena, S.; et al. Mental Health Consequences for Healthcare Workers during the COVID-19 Pandemic: A Scoping Review to Draw Lessons for LMICs. Front. Psychiatry 2021, 12, 602614. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.T.L.; Nguyen, T.B.L.; Pham, A.G.; Duong, K.N.C.; Gloria, M.A.J.; Vo, T.V.; Vo, B.V.; Phung, T.L. Psychological Stress Risk Factors, Concerns and Mental Health Support among Health Care Workers in Vietnam during the Coronavirus Disease 2019 (COVID-19) Outbreak. Front. Public Health 2021, 9, 628341. [Google Scholar] [CrossRef]
- Duffy, C.C.; Bass, G.A.; Fitzpatrick, G.; Doherty, E.M. What can We Learn from the Past? Pandemic Health Care Workers’ Fears, Concerns, and Needs: A Review. J. Patient Saf. 2020, in press. [Google Scholar] [CrossRef]
- Karlsson, U.; Fraenkel, C.J. Covid-19: Risks to healthcare workers and their families. BMJ 2020, 371, m3944. [Google Scholar] [CrossRef] [PubMed]
- Bagcchi, S. Stigma during the COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, 782. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Cag, Y.; Erdem, H.; Gormez, A.; Ankarali, H.; Hargreaves, S.; Ferreira-Coimbra, J.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Pelosi, P.; et al. Anxiety among front-line health-care workers supporting patients with COVID-19: A global survey. Gen. Hosp. Psychiatry 2021, 68, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Zaçe, D.; Hoxhaj, I.; Orfino, A.; Viteritti, A.M.; Janiri, L.; Di Pietro, M.L. Interventions to address mental health issues in healthcare workers during infectious disease outbreaks: A systematic review. J. Psychiatr. Res. 2021, 136, 319–333. [Google Scholar] [CrossRef]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 11, Cd013779. [Google Scholar]
- Greenberg, N.; Brooks, S.K.; Wessely, S.; Tracy, D.K. How might the NHS protect the mental health of health-care workers after the COVID-19 crisis? Lancet Psychiatry 2020, 7, 733–734. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apisarnthanarak, A.; Apisarnthanarak, P.; Siripraparat, C.; Saengaram, P.; Leeprechanon, N.; Weber, D.J. Impact of anxiety and fear for COVID-19 toward infection control practices among Thai healthcare workers. Infect. Control. Hosp. Epidemiol. 2020, 41, 1093–1094. [Google Scholar] [CrossRef]
- Diver, S.; Buccheri, N.; Ohri, C. The value of healthcare worker support strategies to enhance wellbeing and optimise patient care. Future Healthc. J. 2021, 8, e60–e66. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: The potential benefit of health literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Pham, K.M.; Do, B.N.; Kim, G.B.; Dam, H.T.B.; Le, V.-T.T.; Nguyen, T.T.P.; Nguyen, H.T.; Nguyen, T.T.; Le, T.T.; et al. Digital Healthy Diet Literacy and Self-Perceived Eating Behavior Change during COVID-19 Pandemic among Undergraduate Nursing and Medical Students: A Rapid Online Survey. Int. J. Environ. Res. Public Health 2020, 17, 7185. [Google Scholar] [CrossRef]
- Pham, K.M.; Pham, L.V.; Phan, D.T.; Tran, T.V.; Nguyen, H.C.; Nguyen, M.H.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Nguyen, P.B.; et al. Healthy Dietary Intake Behavior Potentially Modifies the Negative Effect of COVID-19 Lockdown on Depression: A Hospital and Health Center Survey. Front. Nutr. 2020, 7, 581043. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.H.; Pham, T.T.M.; Nguyen, K.T.; Nguyen, Y.H.; Tran, T.V.; Do, B.N.; Dao, H.K.; Nguyen, H.C.; Do, N.T.; Ha, T.H.; et al. Negative Impact of Fear of COVID-19 on Health-Related Quality of Life Was Modified by Health Literacy, eHealth Literacy, and Digital Healthy Diet Literacy: A Multi-Hospital Survey. Int. J. Environ. Res. Public Health 2021, 18, 4929. [Google Scholar] [CrossRef] [PubMed]
- Do, B.N.; Tran, T.V.; Phan, D.T.; Nguyen, H.C.; Nguyen, T.T.P.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Trinh, M.V.; Do, T.V.; et al. Health Literacy, eHealth Literacy, Adherence to Infection Prevention and Control Procedures, Lifestyle Changes, and Suspected COVID-19 Symptoms among Health Care Workers during Lockdown: Online Survey. J. Med. Internet Res. 2020, 22, e22894. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Editorial. Overview of Novel Coronavirus (2019-nCoV). Available online: https://bestpractice.bmj.com/topics/en-gb/3000165 (accessed on 2 October 2020).
- Tran, T.V.; Nguyen, H.C.; Pham, L.V.; Nguyen, M.H.; Nguyen, H.C.; Ha, T.H.; Phan, D.T.; Dao, H.K.; Nguyen, P.B.; Trinh, M.V.; et al. Impacts and interactions of COVID-19 response involvement, health-related behaviours, health literacy on anxiety, depression and health-related quality of life among healthcare workers: A cross-sectional study. BMJ Open 2020, 10, e041394. [Google Scholar] [CrossRef]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Nurjanah, N.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Su, T.T.; et al. Development and validation of a new short-form health literacy instrument (HLS-SF12) for the general public in six Asian countries. Health Lit. Res. Pract. 2019, 3, e91–e102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duong, T.V.; Nguyen, T.T.P.; Pham, K.M.; Nguyen, K.T.; Giap, M.H.; Tran, T.D.X.; Nguyen, C.X.; Yang, S.-H.; Su, C.-T. Validation of the short-form health literacy questionnaire (HLS-SF12) and its determinants among people living in rural areas in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 3346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HLS-EU Consortium. Comparative Report of Health Literacy in Eight EU Member States. The European Health Literacy Project 2009–2012. Available online: https://www.healthliteracyeurope.net/hls-eu (accessed on 22 October 2012).
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Purvis, D.L.; Lentino, C.V.; Jackson, T.K.; Murphy, K.J.; Deuster, P.A. Nutrition as a component of the performance triad: How healthy eating behaviors contribute to soldier performance and military readiness. US Army Med. Dep. J. 2013, 66–78. Available online: https://europepmc.org/article/med/24146244 (accessed on 29 July 2021).
- Shams-White, M.M.; Chui, K.; Deuster, P.A.; McKeown, N.M.; Must, A. Investigating Items to Improve the Validity of the Five-Item Healthy Eating Score Compared with the 2015 Healthy Eating Index in a Military Population. Nutrients 2019, 11, 251. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9, in press. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.T.; Do, B.N.; Pham, K.M.; Kim, G.B.; Dam, H.T.B.; Nguyen, T.T.; Nguyen, T.T.P.; Nguyen, Y.H.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, G.; Greenland, S. Simulation study of confounder-selection strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amatori, S.; Donati Zeppa, S.; Preti, A.; Gervasi, M.; Gobbi, E.; Ferrini, F.; Rocchi, M.B.L.; Baldari, C.; Perroni, F.; Piccoli, G.; et al. Dietary Habits and Psychological States during COVID-19 Home Isolation in Italian College Students: The Role of Physical Exercise. Nutrients 2020, 12, 3660. [Google Scholar] [CrossRef]
- Głąbska, D.; Guzek, D.; Groele, B.; Gutkowska, K. Fruit and Vegetable Intake and Mental Health in Adults: A Systematic Review. Nutrients 2020, 12, 115. [Google Scholar] [CrossRef] [Green Version]
- Hoang, T.D.; Colebunders, R.; Fodjo, J.N.S.; Nguyen, N.P.T.; Tran, T.D.; Vo, T.V. Well-Being of Healthcare Workers and the General Public during the COVID-19 Pandemic in Vietnam: An Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4737. [Google Scholar] [CrossRef]
- Editorial. Health and care workers are owed a better future. Lancet 2021, 397, 347. [Google Scholar] [CrossRef]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from Covid-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- Cawcutt, K.A.; Starlin, R.; Rupp, M.E. Fighting fear in healthcare workers during the COVID-19 pandemic. Infect. Control. Hosp. Epidemiol. 2020, 41, 1192–1193. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xu, Y.; Cai, L.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; et al. Gender differences in mental health problems of healthcare workers during the coronavirus disease 2019 outbreak. J. Psychiatr. Res. 2021, 137, 393–400. [Google Scholar] [CrossRef]
- Collantoni, E.; Saieva, A.M.; Meregalli, V.; Girotto, C.; Carretta, G.; Boemo, D.G.; Bordignon, G.; Capizzi, A.; Contessa, C.; Nesoti, M.V.; et al. Psychological Distress, Fear of COVID-19, and Resilient Coping Abilities among Healthcare Workers in a Tertiary First-Line Hospital during the Coronavirus Pandemic. J. Clin. Med. 2021, 10, 1465. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Coronavirus Disease (COVID-19) Outbreak in Vietnam. Available online: https://ncov.moh.gov.vn/ (accessed on 5 April 2020).

{kind=link}
| Variables | Total (n = 2299) | FCoV-19S | Worse MH * (n = 149) | Stable or Better MH * (n = 2150) | Worse HRQoL ** (n = 441) | Stable or Better HRQoL ** (n = 1858) | |||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | Mean ± SD | p | n (%) | n (%) | p | n (%) | n (%) | p | |
| Age, year | 0.444 | 0.160 | 0.004 | ||||||
| 21–40 | 1842 (80.1) | 18.7 ± 5.2 | 126 (84.6) | 1716 (79.8) | 375 (85.0) | 1467 (79.0) | |||
| 41–60 | 457 (19.9) | 18.9 ± 5.3 | 23 (15.4) | 434 (20.2) | 66 (15.0) | 391 (21.0) | |||
| Gender | <0.001 | 0.324 | 0.003 | ||||||
| Women | 1535 (66.8) | 19.1 ± 5.1 | 94 (63.1) | 1441 (67.0) | 268 (60.8) | 1267 (68.2) | |||
| Men | 764 (33.2) | 18 ± 5.6 | 55 (36.9) | 709 (33.0) | 173 (39.2) | 591 (31.8) | |||
| Marital status | 0.001 | 0.077 | 0.705 | ||||||
| Never married | 542 (23.6) | 18.1 ± 5.3 | 44 (29.5) | 498 (23.2) | 107 (24.3) | 435 (23.4) | |||
| Ever married | 1757 (76.4) | 19 ± 5.2 | 105 (70.5) | 1652 (76.8) | 334 (75.7) | 1423 (76.6) | |||
| Ability to pay for medication | 0.004 | 0.033 | <0.001 | ||||||
| Very or fairly difficult | 1210 (52.6) | 19.1 ± 5.5 | 91 (61.1) | 1119 (52.0) | 269 (61.0) | 941 (50.6) | |||
| Very or fairly easy | 1089 (47.4) | 18.4 ± 5 | 58 (38.9) | 1031 (48.0) | 172 (39.0) | 917 (49.4) | |||
| Social status | 0.084 | 0.044 | 0.001 | ||||||
| Low | 307 (13.4) | 19.3 ± 5.9 | 28 (18.8) | 279 (13.0) | 80 (18.1) | 227 (12.2) | |||
| Middle or high | 1992 (86.6) | 18.7 ± 5.1 | 121 (81.2) | 1871 (87.0) | 361 (81.9) | 1631 (87.8) | |||
| Type of health care personnel | <0.001 | 0.267 | 0.804 | ||||||
| Others | 756 (32.9) | 19.3 ± 5.4 | 47 (31.5) | 709 (33.0) | 144 (32.7) | 612 (32.9) | |||
| Nurse | 945 (41.1) | 19.2 ± 5.1 | 55 (36.9) | 890 (41.4) | 177 (40.1) | 768 (41.3) | |||
| Doctor | 598 (26.0) | 17.4 ± 5.1 | 47 (31.5) | 551 (25.6) | 120 (27.2) | 478 (25.7) | |||
| Epidemic containment experience | 0.188 | 0.001 | 0.004 | ||||||
| No | 1292 (56.2) | 18.9 ± 5.2 | 103 (69.1) | 1189 (55.3) | 275 (62.4) | 1017 (54.7) | |||
| Yes | 1007 (43.8) | 18.6 ± 5.3 | 46 (30.9) | 961 (44.7) | 166 (37.6) | 841 (45.3) | |||
| BMI, kg/m2 | 0.074 | 0.634 | 0.094 | ||||||
| <25.0 kg/m2 | 2024 (88.0) | 18.8 ± 5.3 | 133 (89.3) | 1891 (88.0) | 378 (85.7) | 1646 (88.6) | |||
| ≥3 25.0 kg/m2 | 275 (12.0) | 18.2 ± 5.2 | 16 (10.7) | 259 (12.0) | 63 (14.3) | 212 (11.4) | |||
| Comorbidity | 0.435 | 0.024 | 0.250 | ||||||
| None | 2164 (94.1) | 18.7 ± 5.3 | 134 (89.9) | 2030 (94.4) | 410 (93.0) | 1754 (94.4) | |||
| One or more | 135 (5.9) | 19.1 ± 4.8 | 15 (10.1) | 120 (5.6) | 31 (7.0) | 104 (5.6) | |||
| S-COVID-19-S *** | 0.044 | <0.001 | <0.001 | ||||||
| No | 1961 (85.3) | 18.7 ± 5.3 | 100 (67.1) | 1861 (86.6) | 338 (76.6) | 1623 (87.4) | |||
| Yes | 338 (14.7) | 19.3 ± 5.1 | 49 (32.9) | 289 (13.4) | 103 (23.4) | 235 (12.6) | |||
| FCoV-19S, Mean ± SD | 18.8 ± 5.3 | 23.0 ± 4.7 | 18.5 ± 5.2 | <0.001 | 20.4 ± 5.0 | 18.4 ± 5.2 | <0.001 | ||
| HL, Mean ± SD | 36.1 ± 7.1 | 33.7 ± 6.4 | 36.3 ± 7.1 | <0.001 | 34.8 ± 6.9 | 36.4 ± 7.1 | <0.001 | ||
| eHEALS, Mean ± SD | 33.1 ± 4.8 | 32.5 ± 4.8 | 33.1 ± 4.8 | 0.172 | 32.7 ± 5.4 | 33.2 ± 4.7 | 0.059 | ||
| DDL, Mean ± SD | 35.8 ± 8.2 | 33.6 ± 7.5 | 35.9 ± 8.2 | 0.001 | 34.4 ± 8.1 | 36.1 ± 8.2 | <0.001 | ||
| HES, Mean ± SD | 14.6 ± 4.8 | 13.7 ± 4.6 | 14.7 ± 4.8 | 0.013 | 13.8 ± 4.7 | 14.8 ± 4.8 | <0.001 |
| Variables | FCoV-19S | |||
|---|---|---|---|---|
| Bivariate | Multivariate | |||
| B (95% CI) | p | B (95% CI) | p | |
| Age, year | ||||
| 21–40 | Reference | Reference | ||
| 41–60 | 0.21 (−0.33, 0.75) | 0.444 | 0.30 (−0.26, 0.85) | 0.297 |
| Gender | ||||
| Women | Reference | Reference | ||
| Men | −1.10 (−1.56, −0.65) | <0.001 | −0.72 (−1.20, −0.24) | 0.003 |
| Marital status | ||||
| Never married | Reference | Reference | ||
| Ever married | 0.87 (0.37, 1.38) | 0.001 | 0.88 (0.36, 1.39) | 0.001 |
| Ability to pay for medication | ||||
| Very or fairly difficult | Reference | Reference | ||
| Very or fairly easy | −0.63 (−1.06, −0.20) | 0.004 | −0.28 (−0.72, 0.15) | 0.199 |
| Social status | ||||
| Low | Reference | Reference | ||
| Middle or high | −0.56 (−1.19, 0.07) | 0.084 | −0.19 (−0.83, 0.45) | 0.554 |
| Type of health care personnel | ||||
| Others | Reference | Reference | ||
| Nurse | −0.08 (−0.57, 0.42) | 0.765 | −0.11 (−0.62, 0.39) | 0.659 |
| Doctor | −1.89 (−2.44, −1.33) | <0.001 | −1.63 (−2.20, −1.06) | <0.001 |
| Epidemic containment experience | ||||
| No | Reference | Reference | ||
| Yes | −0.29 (−0.72, 0.14) | 0.188 | −0.31 (−0.75, 0.12) | 0.158 |
| BMI, kg/m2 | ||||
| <25.0 kg/m2 | Reference | Reference | ||
| ≥25.0 kg/m2 | −0.60 (−1.27, 0.06) | 0.074 | −0.31 (−0.98, 0.36) | 0.360 |
| Comorbidity | ||||
| None | Reference | Reference | ||
| One or more | 0.36 (−0.55, 1.28) | 0.435 | 0.22 (−0.69, 1.14) | 0.631 |
| S-COVID−19-S * | ||||
| No | Reference | Reference | ||
| Yes | 0.62 (0.02, 1.23) | 0.044 | 0.51 (−0.09, 1.11) | 0.098 |
| HL, One-point increment | −0.08 (−0.11, −0.05) | <0.001 | ||
| eHEALS, One-point increment | −0.03 (−0.08, 0.01) | 0.125 | ||
| DDL, One-point increment | −0.06 (−0.08, −0.03) | <0.001 | −0.04 (−0.07, −0.02) | 0.001 |
| HES, One-point increment | −0.11 (−0.16, −0.07) | <0.001 | −0.10 (−0.15, −0.06) | <0.001 |
| Variables | Mental Health Changes * | |||
|---|---|---|---|---|
| Bivariate | Multivariate | |||
| OR (95% CI) | p | OR (95% CI) | p | |
| Age, year | ||||
| 21–40 | Reference | Reference | ||
| 41–60 | 1.39 (0.88, 2.19) | 0.162 | 1.28 (0.79, 2.10) | 0.318 |
| Gender | ||||
| Women | Reference | Reference | ||
| Men | 0.84 (0.60, 1.19) | 0.324 | 0.91 (0.63, 1.33) | 0.640 |
| Marital status | ||||
| Never married | Reference | Reference | ||
| Ever married | 1.39 (0.96, 2.00) | 0.078 | 1.18 (0.80, 1.74) | 0.397 |
| Ability to pay for medication | ||||
| Very or fairly difficult | Reference | Reference | ||
| Very or fairly easy | 1.45 (1.03, 2.03) | 0.034 | 1.36 (0.95, 1.94) | 0.094 |
| Social status | ||||
| Low | Reference | Reference | ||
| Middle or high | 1.55 (1.01, 2.39) | 0.045 | 1.33 (0.84, 2.11) | 0.225 |
| Type of health care personnel | ||||
| Others | Reference | Reference | ||
| Nurse | 1.07 (0.72, 1.60) | 0.732 | 1.04 (0.68, 1.58) | 0.872 |
| Doctor | 0.78 (0.51, 1.18) | 0.239 | 0.69 (0.44, 1.08) | 0.102 |
| Epidemic containment experience | ||||
| No | Reference | Reference | ||
| Yes | 1.81 (1.27, 2.59) | 0.001 | 1.62 (1.11, 2.35) | 0.012 |
| BMI, kg/m2 | ||||
| <25.0 kg/m2 | Reference | Reference | ||
| ≥25.0 kg/m2 | 1.14 (0.67, 1.94) | 0.634 | 1.21 (0.69, 2.12) | 0.508 |
| Comorbidity | ||||
| None | Reference | Reference | ||
| One or more | 0.53 (0.30, 0.93) | 0.027 | 0.65 (0.35, 1.18) | 0.154 |
| S-COVID-19-S ** | ||||
| No | Reference | Reference | ||
| Yes | 0.32 (0.22, 0.46) | <0.001 | 0.36 (0.25, 0.53) | <0.001 |
| HL, One-point increment | 1.06 (1.03, 1.09) | <0.001 | ||
| eHEALS, One-point increment | 1.02 (0.99, 1.06) | 0.172 | ||
| DDL, One-point increment | 1.04 (1.01, 1.06) | 0.001 | 1.02 (1.00, 1.05) | 0.029 |
| HES, One-point increment | 1.04 (1.01, 1.08) | 0.013 | 1.04 (1.00, 1.07) | 0.043 |
| Variables | HRQoL Changes * | |||
|---|---|---|---|---|
| Bivariate | Multivariate | |||
| OR (95% CI) | p | OR (95% CI) | p | |
| Age, year | ||||
| 21–40 | Reference | Reference | ||
| 41–60 | 1.51 (1.14, 2.01) | 0.004 | 1.53 (1.13, 2.07) | 0.006 |
| Gender | ||||
| Women | Reference | Reference | ||
| Men | 0.72 (0.58, 0.90) | 0.003 | 0.76 (0.60, 0.97) | 0.024 |
| Marital status | ||||
| Never married | Reference | Reference | ||
| Ever married | 1.05 (0.82, 1.34) | 0.705 | 0.88 (0.68, 1.14) | 0.347 |
| Ability to pay for medication | ||||
| Very or fairly difficult | Reference | Reference | ||
| Very or fairly easy | 1.52 (1.23, 1.88) | <0.001 | 1.43 (1.14, 1.78) | 0.002 |
| Social status | ||||
| Low | Reference | Reference | ||
| Middle or high | 1.59 (1.20, 2.11) | 0.001 | 1.37 (1.02, 1.84) | 0.037 |
| Type of health care personnel | ||||
| Others | Reference | Reference | ||
| Nurse | 1.02 (0.80, 1.30) | 0.868 | 0.95 (0.73, 1.23) | 0.708 |
| Doctor | 0.94 (0.72, 1.23) | 0.638 | 0.84 (0.63, 1.12) | 0.225 |
| Epidemic containment experience | ||||
| No | Reference | Reference | ||
| Yes | 1.37 (1.11, 1.70) | 0.004 | 1.29 (1.03, 1.61) | 0.026 |
| BMI, kg/m2 | ||||
| <25.0 kg/m2 | Reference | Reference | ||
| ≥25.0 kg/m2 | 0.77 (0.57, 1.05) | 0.095 | 0.83 (0.60, 1.15) | 0.264 |
| Comorbidity | ||||
| None | Reference | Reference | ||
| One or more | 0.78 (0.52, 1.19) | 0.251 | 0.90 (0.58, 1.39) | 0.636 |
| S-COVID-19-S ** | ||||
| No | Reference | Reference | ||
| Yes | 0.48 (0.37, 0.62) | <0.001 | 0.53 (0.40, 0.69) | <0.001 |
| HL, One-point increment | 1.03 (1.02, 1.05) | <0.001 | ||
| eHEALS, One-point increment | 1.02 (1.00, 1.04) | 0.060 | ||
| DDL, One-point increment | 1.03 (1.01, 1.04) | <0.001 | 1.02 (1.01, 1.03) | 0.006 |
| HES, One-point increment | 1.04 (1.02, 1.07) | <0.001 | 1.04 (1.02, 1.06) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vu, D.N.; Phan, D.T.; Nguyen, H.C.; Le, L.T.H.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Trinh, M.V.; Do, T.V.; Nguyen, H.Q.; et al. Impacts of Digital Healthy Diet Literacy and Healthy Eating Behavior on Fear of COVID-19, Changes in Mental Health, and Health-Related Quality of Life among Front-Line Health Care Workers. Nutrients 2021, 13, 2656. https://doi.org/10.3390/nu13082656
Vu DN, Phan DT, Nguyen HC, Le LTH, Nguyen HC, Ha TH, Dao HK, Trinh MV, Do TV, Nguyen HQ, et al. Impacts of Digital Healthy Diet Literacy and Healthy Eating Behavior on Fear of COVID-19, Changes in Mental Health, and Health-Related Quality of Life among Front-Line Health Care Workers. Nutrients. 2021; 13(8):2656. https://doi.org/10.3390/nu13082656
Chicago/Turabian StyleVu, Dinh N., Dung T. Phan, Hoang C. Nguyen, Lan T. H. Le, Huu C. Nguyen, Tung H. Ha, Hung K. Dao, Manh V. Trinh, Thinh V. Do, Hung Q. Nguyen, and et al. 2021. "Impacts of Digital Healthy Diet Literacy and Healthy Eating Behavior on Fear of COVID-19, Changes in Mental Health, and Health-Related Quality of Life among Front-Line Health Care Workers" Nutrients 13, no. 8: 2656. https://doi.org/10.3390/nu13082656