
Impact of SARS-CoV-2 Alpha and Gamma Variants among Symptomatic Pregnant Women: A Two-Center Retrospective Cohort Study between France and Brazil


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
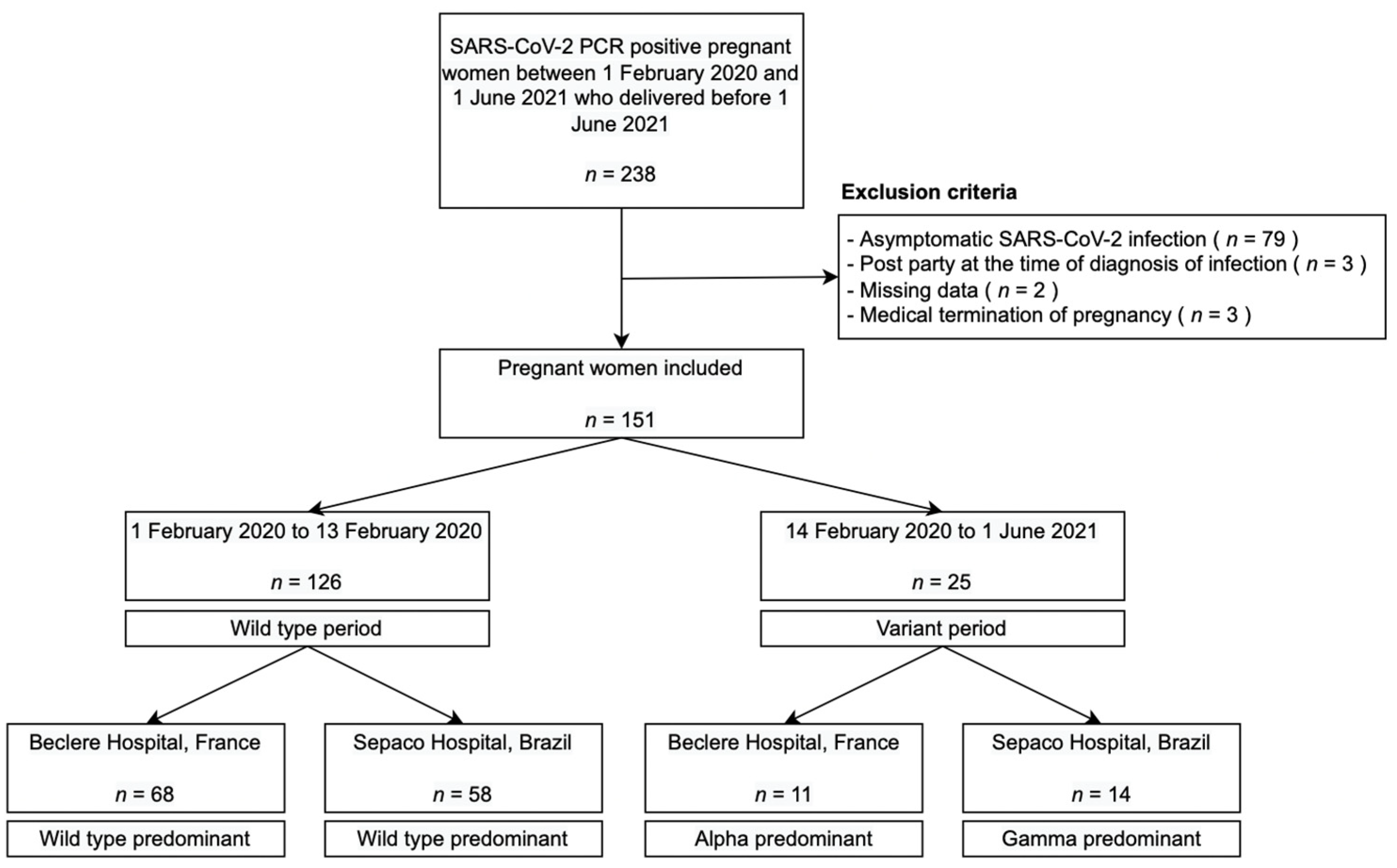
2.1. Study Design
2.2. Epidemiology of Variants in France and Brazil during the Study Period
2.3. Data
2.4. Outcomes
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Baseline Characteristics
3.2. Primary Outcome—Disease Severity
3.3. Secondary Outcomes—Obstetrical and Neonatal Outcomes
3.4. Subpopulation Analysis: Comparison of Each Variant in Each Center
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Thangaratinam, S. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, 3320. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 193, E540–E548. [Google Scholar] [CrossRef] [PubMed]
- Badr, D.A.; Picone, O.; Bevilacqua, E.; Carlin, A.; Meli, F.; Sibiude, J.; Mattern, J.; Fils, J.-F.; Mandelbrot, L.; Lanzone, A.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 and Pregnancy Outcomes According to Gestational Age at Time of Infection. Emerg. Infect. Dis. 2021, 27, 2535–2543. [Google Scholar] [CrossRef] [PubMed]
- Donati, S.; Corsi, E.; Maraschini, A.; Salvatore, M.A. ItOSS-COVID-19 working group. SARS-CoV-2 infection among hospitalized pregnant women and impact of different viral strains on COVID-19 severity in Italy: A national prospective population-based cohort study. BJOG 2021, 129, 221–231. [Google Scholar] [CrossRef]
- Engjom, H.; Aabakke, A.J.M.; Klungsøyr, K.; Svanvik, T.; Äyräs, O.; Jonasdottir, E.; Thurn, L.; Jones, E.; Pettersson, K.; Nyfløt, L.T.; et al. COVID-19 in pregnancy-characteristics and outcomes of pregnant women admitted to hospital because of SARS-CoV-2 infection in the Nordic countries. Acta Obstet. Gynecol. Scand. 2021, 100, 1611–1619. [Google Scholar] [CrossRef]
- Vousden, N.; Ramakrishnan, R.; Bunch, K.; Morris, E.; Simpson, N.A.B.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; et al. Severity of maternal infection and perinatal outcomes during periods of SARS-CoV-2 wildtype, alpha, and delta variant dominance in the UK: Prospective cohort study. BMJ Med. 2022. [Google Scholar] [CrossRef]
- DeSisto, C.L.; Wallace, B.; Simeone, R.M.; Polen, K.; Ko, J.Y.; Meaney-Delman, D.; Ellington, S.R. Risk for Stillbirth among Women with and without COVID-19 at Delivery Hospitalization—United States, March 2020–September 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1640–1645. [Google Scholar] [CrossRef]
- Tracking SARS-CoV-2 Variants n.d. Available online: https://www.who.int/emergencies/emergency-health-kits/trauma-emergency-surgery-kit-who-tesk-2019/tracking-SARS-CoV-2-variants (accessed on 25 September 2021).
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; Van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance 2021, 26, 2100509. [Google Scholar] [CrossRef]
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Karim, S.S.A.; Sridhar, D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Cevik, M.; Mishra, S. SARS-CoV-2 variants and considerations of inferring causality on disease severity. Lancet Infect. Dis. 2021, 21, 1472–1474. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.-M.; Cui, L.; Toh, M.P.H.; Ding, Y.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and Virological Features of SARS-CoV-2 Variants of Concern: A Retrospective Cohort Study Comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2021, ciab721. [Google Scholar] [CrossRef]
- Lapinsky, S.E.; Adhikari, N.K. COVID-19, variants of concern and pregnancy outcome. Obstet. Med 2021, 14, 65–66. [Google Scholar] [CrossRef]
- Kadiwar, S.; Smith, J.J.; Ledot, S.; Johnson, M.; Bianchi, P.; Singh, N.; Montanaro, C.; Gatzoulis, M.; Shah, N.; Ukor, F.-E. Were pregnant women more affected by COVID-19 in the second wave of the pandemic? Lancet 2021, 397, 1539–1540. [Google Scholar] [CrossRef]
- Adhikari, E.H.; SoRelle, J.A.; McIntire, D.D.; Spong, C.Y. Increasing severity of COVID-19 in pregnancy with Delta (B.1.617.2) variant surge. Am. J. Obstet. Gynecol. 2022, 226, 149–151. [Google Scholar] [CrossRef]
- Seasely, A.R.; Blanchard, C.T.; Arora, N.; Battarbee, A.N.; Casey, B.M.; Dionne-Odom, J.; Leal, S.M., Jr.; Moates, D.B.; Sinkey, R.G.; Szychowski, J.M.; et al. Maternal and Perinatal Outcomes Associated with the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Delta (B.1.617.2) Variant. Obstet. Gynecol. 2021, 138, 842–844. [Google Scholar] [CrossRef]
- Mahajan, N.N.; Pophalkar, M.; Patil, S.; Yewale, B.; Chaaithanya, I.K.; Mahale, S.D.; Gajbhiye, R.K. Pregnancy Outcomes and Maternal Complications During the Second Wave of Coronavirus Disease 2019 (COVID-19) in India. Obstet. Gynecol. 2021, 138, 660–662. [Google Scholar] [CrossRef]
- Bmm, G.; Rpv, F.; As, R. Maternal mortality associated with COVID-19 in Brazil in 2020 and 2021: Comparison with non-pregnant women and men. PLoS ONE 2021, 16, e0261492. [Google Scholar] [CrossRef]
- Enquêtes Flash: Évaluation de la Circulation Des Variants du SARS-CoV-2 en France n.d. Available online: https://www.santepubliquefrance.fr/etudes-et-enquetes/enquetes-flash-evaluation-de-la-circulation-des-variants-du-sars-cov-2-en-france (accessed on 10 October 2021).
- Martins, A.F.; Zavascki, A.P.; Wink, P.L.; Volpato, F.C.Z.; Monteiro, F.L.; Rosset, C.; de Paris, F.; Ramos, Á.K.; Barth, A.L. Detection of SARS-CoV-2 lineage P.1 in patients from a region with exponentially increasing hospitalisation rate, February 2021, Rio Grande do Sul, Southern Brazil. Euro Surveill 2021, 26, 2100276. [Google Scholar] [CrossRef] [PubMed]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, A.R. Nextstrain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Clinical Management: Living Guidance n.d. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-1 (accessed on 26 September 2021).
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 106: Intrapartum fetal heart rate monitoring: Nomenclature, interpretation, and general management principles. Obstet. Gynecol. 2009, 114, 192–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjoberg, D.D.; Whiting, K.; Curry, M.; Lavery, J.A.; Larmarange, J. Reproducible Summary Tables with the gtsummary Package. R J. 2021, 13, 570–580. [Google Scholar] [CrossRef]
- Géodes-Santé Publique France-Indicateurs: Cartes, Données et Graphiques n.d. Available online: https://geodes.santepubliquefrance.fr/#c=indicator&view=map2 (accessed on 27 April 2022).
- Brazil: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data n.d. Available online: https://covid19.who.int (accessed on 27 April 2022).


{kind=link}
| Characteristic | Overall 1 February 2020–1 June 2021 | Wild-Type Period 1 February 2020–13 February 2021 | Variant Period 14 February 2021–1 June 2021 | p-Value |
|---|---|---|---|---|
| Total, n (%) | n = 151/151 (100%) | n = 126/151 (83.4%) | n = 25/151 (16.6%) | |
| Patients distribution by hospital, n (%) | 0.4 | |||
| Sepaco Hospital, Brazil | 72/151 (48%) | 58/126 (46%) | 14/25 (56%) | |
| Béclère Hospital, France | 79/151 (52%) | 68/126 (54%) | 11/25 (44%) | |
| Mean age, years mean (IQR) | 31.0 (28.0, 35.0) | 31.0 (28.0, 34.0) | 33.0 (30.0, 36.0) | 0.069 |
| Ethnic group, n (%) | 0.5 | |||
| White | 85/151 (56%) | 70/126 (56%) | 15/25 (60%) | |
| Black | 27/151 (18%) | 24/126 (19%) | 3/25 (12%) | |
| Maghrebian | 18/151 (12%) | 13/126 (10%) | 5/25 (20%) | |
| Hispanic | 20/151 (13%) | 18/126 (14%) | 2/25 (8.0%) | |
| Asian | 1/151 (0.7%) | 1/126 (0.8%) | 0/25 (0%) | |
| Pre-pregnancy BMI, kg/m2 mean, (IQR) | 26.2 (23.3, 30.3) | 26.0 (23.0, 29.9) | 29.0 (26.0, 35.0) | 0.011 |
| Parity, n (%) | 0.4 | |||
| Nulliparous | 73/151 (48.3%) | 59/126 (46.9%) | 14/25 (56.0%) | |
| Multiparous | 78/151 (51.7%) | 67/126 (53.1%) | 11/25 (44.0%) | |
| Current smoking, n (%) | 16/151 (11%) | 13/126 (10%) | 3/25 (12%) | 0.7 |
| Pre-existing medical conditions, n (%) | 38/151 (25%) | 29/126 (23%) | 9/25 (36%) | 0.2 |
| Chronic hypertension | 14/151 (9.3%) | 13/126 (10%) | 1/25 (4.0%) | 0.5 |
| Diabetes mellitus | 1/151 (0.7%) | 0/126 (0%) | 1/25 (4.0%) | 0.2 |
| Pulmonary disease (including asthma) | 11/151 (7.3%) | 8/126 (6.3%) | 3/25 (12%) | 0.4 |
| Other | 12/151 (7.9%) | 8/126 (6.3%) | 4/25 (16%) | |
| Multiple pregnancies, n (%) | 8/151 (5.3%) | 7/126 (5.6%) | 1/25 (4.0%) | >0.9 |
| COVID-19 infection-related information | ||||
| Gestational age at the time of positive RT-PCR, weeks mean (IQR) | 32 (26, 35) | 31 (26, 35) | 34 (32, 36) | 0.12 |
| Hospital admissions for COVID-19-related illness, n (%) | 57/151 (38%) | 43/126 (34%) | 14/25 (56%) | 0.039 |
| Characteristic | Wild-Type Period | Variant Period | Univariate Analysis | Multivariate Analysis 1 | ||||
|---|---|---|---|---|---|---|---|---|
| 126/151 (83.4%) | 25/151 (16.6%) | OR | 95%CI | p-Value | aOR 1 | 95%CI | p-Value | |
| Primary Outcome | ||||||||
| Severe-to-critical infection according to WHO | 22/126 (17%) | 13/25 (52%) | 5.12 | 2.07, 12.9 | <0.001 | 7.07 | 2.50, 21.6 | <0.001 |
| Secondary Outcomes | ||||||||
| Admission to ICU | 13/126 (10%) | 8/25 (32%) | 4.09 | 1.44, 11.3 | 0.007 | 3.75 | 1.22, 11.2 | 0.018 |
| Oxygen support | 21/126 (17%) | 12/25 (48%) | 4.62 | 1.84, 11.6 | 0.001 | 5.47 | 2.00, 15.7 | 0.001 |
| Pneumonia | 22/126 (17%) | 11/25 (44%) | 3.71 | 1.47, 9.30 | 0.005 | 3.94 | 1.43, 11.1 | 0.008 |
| ARDS | 7/126 (5.6%) | 5/25 (20%) | 4.25 | 1.16, 14.7 | 0.022 | 3.83 | 0.95, 14.6 | 0.050 |
| Mechanical ventilation | 6/126 (4.8%) | 5/25 (20%) | 5.00 | 1.33, 18.2 | 0.014 | 4.72 | 1.12, 19.6 | 0.030 |
| ECMO | 0/126 (0%) | 0/25 (0%) | - | - | - | - | - | - |
| Maternal death | 0/126 (0%) | 1/25 (4.0%) | - | - | - | - | - | - |
| Disease severity | 0.001 | |||||||
| Non-severe | 103/126 (82%) | 12/25 (48%) | ||||||
| Severe | 16/126 (13%) | 8/25 (32%) | ||||||
| Critical | 7/126 (5.6%) | 5/25 (20%) | ||||||
| Hospital admission for COVID-19-related illness | 43/126 (34%) | 14/25 (56%) | 0.039 | |||||
| Characteristic | Wild-Type Period | Variant Period | Univariate Analysis | Multivariate Analysis 1 | ||||
|---|---|---|---|---|---|---|---|---|
| 1 February 2020–13 February 2021 | 14 February 2021–1 June 2021 | OR | 95%CI | p | aOR 1 | 95%CI | p | |
| Composite adverse obstetric outcome | 51/126 (40%) | 15/25 (60%) | 2.21 | 0.93, 5.44 | 0.077 | 1.86 | 0.73, 4.86 | 0.2 |
| Secondary Obstetrical Outcomes | ||||||||
| Pre-eclampsia; eclampsia; HELLP | 11/126 (8.7%) | 2/25 (8.0%) | 0.91 | 0.13, 3.68 | 0.91 | 0.11 | 0.01, 0.84 | 0.056 |
| Gestational age at delivery, weeks mean (IQR) | 39.0 (37.3, 40.0) | 37.1 (34.1, 39.0) | - | - | 0.045 | - | - | - |
| <32 weeks | 11/126 (8.7%) | 1/25 (4.0%) | 0.44 | 0.02, 2.40 | 0.44 | 0.35 | 0.02, 2.34 | 0.4 |
| <37 weeks | 25/126 (20%) | 11/25 (44%) | 3.17 | 1.27, 7.85 | 0.012 | 3.87 | 1.44, 10.6 | 0.007 |
| Spontaneous delivery <37 weeks | 7/126 (5.6%) | 2/25 (8.0%) | 1.48 | 0.21, 6.59 | 0.64 | 2.45 | 0.21, 23.7 | 0.4 |
| Unscheduled cesarean | 42/126 (33%) | 10/25 (40%) | 1.33 | 0.54, 3.19 | 0.52 | 1.10 | 0.42, 2.77 | 0.8 |
| Suspected fetal distress | 24/126 (19.0%) | 6/25 (24.0%) | 0.88 | 0.29, 2.38 | 0.80 | 0.45 | 0.12, 1.41 | 0.2 |
| Postpartum hemorrhage | 20/126 (16%) | 0/25 (0%) | - | - | - | - | - | - |
| Stillbirth | 3/126 (2.4%) | 1/25 (4.0%) | ||||||
| <24 weeks | 1/126 (0.8%) | 1/25 (4.0%) | 5.21 | 0.20, 135 | 0.25 | 6.04 | 0.15, 690 | 0.3 |
| >24 weeks | 2/126 (1.6%) | 0/25 (0%) | - | - | - | - | - | - |
| Deep venous thromboembolism/pulmonary embolism | 0/126 (0%) | 0/25 (0%) | - | - | - | - | - | - |
| Maternal death | 0/126 (0%) | 1/25 (4.0%) | - | - | - | - | - | - |
| Characteristic | Wild-Type Period | Variant Period | Univariate Analysis | Multivariate Analysis 1 | ||||
|---|---|---|---|---|---|---|---|---|
| 1 February 2020–13 February 2021 | 14 February 2021–1 June 2021 | OR | 95%CI | p | aOR 1 | 95%CI | p | |
| Composite adverse neonatal outcome | 42/131 (32%) | 10/24 (42%) | 1.51 | 0.61, 3.67 | 0.36 | 1.42 | 0.55, 3.58 | 0.5 |
| Secondary Neonatal Outcomes | ||||||||
| Weight, g (IQR) | 3060 (2612, 3402) | 2945 (2285, 3332) | - | - | 0.3 | - | - | 0.6 |
| Z-score | −0.52 (−1.23, 0.23) | −0.43 (−1.22, 0.25) | - | - | 0.9 | - | - | 0.8 |
| SGA (Z-score < −1.28) | 28/128 (21.9%) | 6/23 (26.1%) | 0.89 | 0.20, 2.93 | 0.86 | 0.93 | 0.20, 3.29 | >0.9 |
| Admission to NICU | 11/128 (8.6%) | 8/23 (35%) | 5.67 | 1.93, 16.4 | 0.001 | 4.94 | 1.37, 18.4 | 0.014 |
| 5′ Apgar score < 7 | 9/128 (7.0%) | 0/23 (0%) | - | - | 0.4 | - | - | - |
| Arterial umbilical cord pH, mean (IQR) | 7.24 (7.18, 7.28) | 7.24 (7.21, 7.29) | - | - | 0.6 | - | - | 0.7 |
| Neonatal respiratory distress | 10/128 (7.8%) | 6/23 (26%) | 4.16 | 1.28, 12.8 | 0.014 | 3.34 | 0.88, 12.2 | 0.068 |
| Grade 3/4 intraventricular hemorrhage | 3/128 (2.3%) | 1/23 (4.3%) | 1.89 | 0.09, 15.6 | 0.59 | 1.10 | 0.05, 10.3 | >0.9 |
| Neonatal death | 4/128 (3.1%) | 0 (0%) | - | - | - | - | - | - |
| Congenital malformation | 2/128 (1.5%) | 0/23 (0%) | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosnino, E.; Bernardes, L.S.; Mattern, J.; Hipólito Micheletti, B.; Aparecida de Castro Maldonado, A.; Vauloup-Fellous, C.; Doucet-Populaire, F.; De Luca, D.; Benachi, A.; Vivanti, A.J. Impact of SARS-CoV-2 Alpha and Gamma Variants among Symptomatic Pregnant Women: A Two-Center Retrospective Cohort Study between France and Brazil. J. Clin. Med. 2022, 11, 2663. https://doi.org/10.3390/jcm11092663
Mosnino E, Bernardes LS, Mattern J, Hipólito Micheletti B, Aparecida de Castro Maldonado A, Vauloup-Fellous C, Doucet-Populaire F, De Luca D, Benachi A, Vivanti AJ. Impact of SARS-CoV-2 Alpha and Gamma Variants among Symptomatic Pregnant Women: A Two-Center Retrospective Cohort Study between France and Brazil. Journal of Clinical Medicine. 2022; 11(9):2663. https://doi.org/10.3390/jcm11092663
Chicago/Turabian StyleMosnino, Elie, Lisandra S. Bernardes, Jeremie Mattern, Bruna Hipólito Micheletti, Amarilis Aparecida de Castro Maldonado, Christelle Vauloup-Fellous, Florence Doucet-Populaire, Daniele De Luca, Alexandra Benachi, and Alexandre J. Vivanti. 2022. "Impact of SARS-CoV-2 Alpha and Gamma Variants among Symptomatic Pregnant Women: A Two-Center Retrospective Cohort Study between France and Brazil" Journal of Clinical Medicine 11, no. 9: 2663. https://doi.org/10.3390/jcm11092663