
A Pilot Study of a Sensor Enhanced Activity Management System for Promoting Home Rehabilitation Exercise Performed during the COVID-19 Pandemic: Therapist Experience, Reimbursement, and Recommendations for Implementation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. System Description
2.3. Data Collection and Statistical Analysis
3. Results
3.1. Adherence
3.2. Survey Responses
3.3. End of Study Interviews
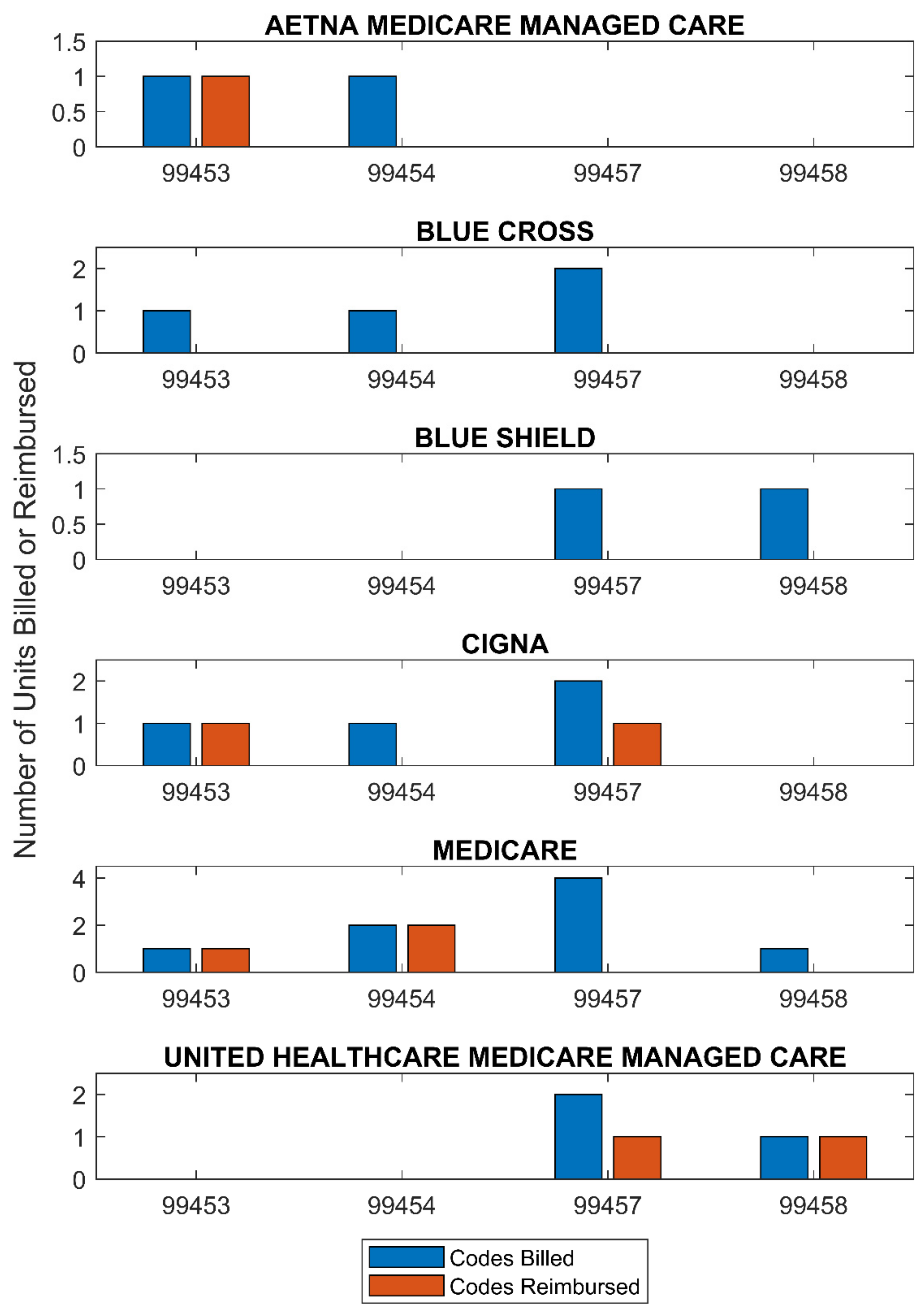
3.4. Billing and Reimbursement
4. Discussion
4.1. Adherence and Motivation
Therapist 1: “One thing I learned was that the use of the technology is highly motivating. Initially my patient was being non-compliant, and after the introduction of this technology they were doing their homework and going for walks.”
Therapist 2: “It really helped keep my patients on task with their home exercise program. Because they knew that they were being monitored, I think that helps them to be more compliant with their home exercises.”
Therapist 3: “Very beneficial, even just having the puck there, believe it or not. I felt just having that there, even if it wasn’t necessarily capturing all of their repetitions, it was just something that reminded them ‘this is something that I’m doing.’ Versus just sitting there and you’re stretching your hand or your arm, here you’re given something that’s visual or tangible that helps keep you on track.”
Therapist 3: “Overall, it did help compliance and accountability. When they walked in, if they didn’t do their exercises that week, they already came in with the “I’m so sorry, this is the reason why I didn’t get it done.” For me, I felt like it was always in there, in the back of their mind. They knew I had a way of seeing that they did or did not complete their exercises.”
4.2. Reimbursement for Remote Patient Monitoring
Therapist 2: “Having the ability to bill the insurance for some remote patient monitoring really helped make my time more productive, from a billing perspective. When the pandemic first started, and the clinic was closed, I was making a lot of phone calls to patients and asking them questions and giving them advice, but I wasn’t able to bill for any of that. But with this system, that could be very useful.”
“This allows health care professionals who were previously ineligible to furnish and bill for Medicare telehealth services, including physical therapists, occupational therapists, speech language pathologists, and others, to receive payment for Medicare telehealth services” [29].
4.3. Limitations, Recommendations, and Future Directions
Therapist 3: “Overall, the biggest challenge is time. And it’s not the study or the program, it’s just time. Being able to incorporate something new and novel into your program takes a little bit more time and effort to be proficient with it. And with some of the constraints that we have, you’re always pressed. I think it’s just the nature of the beast of how healthcare is right now. Everything is just maximize time, maximize productivity, and then everything else kind of falls in wherever it can.”
Therapist 3: “There are definitely diagnoses that I feel it would work really well with, higher level patients that basically you give your home exercise program to, you’re able to monitor it, you check in with them a couple times a week, just to make sure that they’re doing it safely, that they’re doing them correctly, or if they have any questions. Some of the other patients, with more moderate to severe impairments, it’s definitely challenging because, one of the big things that we do as therapists is putting our hands on the patients to help facilitate movements or inhibit movements and you just can’t do that via telerehab.”
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- Bassett, S. The assessment of patient adherence to physiotherapy rehabilitation. N. Z. J. Physiother. 2003, 31, 60–66. [Google Scholar]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for enhancing adherence with physiotherapy: A systematic review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Holden, M.A.; Haywood, K.L.; Potia, T.A.; Gee, M.; McLean, S. Recommendations for exercise adherence measures in musculoskeletal settings: A systematic review and consensus meeting (protocol). Syst. Rev. 2014, 3, 1–6. [Google Scholar] [CrossRef]
- Nicolson, P.J.A.; Hinman, R.S.; Wrigley, T.V.; Stratford, P.W.; Bennell, K.L. Self-reported Home Exercise Adherence: A Validity and Reliability Study Using Concealed Accelerometers. J. Orthop. Sports Phys. Ther. 2018, 48, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Peek, K.; Carey, M.; Mackenzie, L.; Sanson-Fisher, R. Patient adherence to an exercise program for chronic low back pain measured by patient-report, physiotherapist-perception and observational data. Physiother. Theory Pract. 2019, 35, 1304–1313. [Google Scholar] [CrossRef]
- Mourad, S.; Eddine, H.K.; Karaki, H.; Hassan, K.H. Patient’s adherence to prescribed home exercises: Barriers and interventions. Genet. Mol. Res. 2018, 17, 12. [Google Scholar]
- Bennell, K.L.; Marshall, C.J.; Dobson, F.; Kasza, J.; Lonsdale, C.; Hinman, R.S. Does a Web-Based Exercise Programming System Improve Home Exercise Adherence for People With Musculoskeletal Conditions? A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2019, 98, 850–858. [Google Scholar] [CrossRef]
- Lambert, T.E.; Harvey, L.A.; Avdalis, C.; Chen, L.W.; Jeyalingam, S.; Pratt, C.A.; Tatum, H.J.; Bowden, J.L.; Lucas, B.R. An app with remote support achieves better adherence to home exercise programs than paper handouts in people with musculoskeletal conditions: A randomised trial. J. Physiother. 2017, 63, 161–167. [Google Scholar] [CrossRef]
- Bäcker, H.C.; Wu, C.H.; Schulz, M.R.G.; Weber-Spickschen, T.S.; Perka, C.; Hardt, S. App-based rehabilitation program after total knee arthroplasty: A randomized controlled trial. Arch. Orthop. Trauma Surg. 2021, 141, 1575–1582. [Google Scholar] [CrossRef]
- Simpson, D.B.; Bird, M.-L.; English, C.; Gall, S.L.; Breslin, M.; Smith, S.; Schmidt, M.; Callisaya, M.L. Connecting patients and therapists remotely using technology is feasible and facilitates exercise adherence after stroke. Top. Stroke Rehabil. 2020, 27, 93–102. [Google Scholar] [CrossRef]
- NW, 1615 L. St; Washington, S. 800; Inquiries, D. 20036 U.-419-4300 | M.-857-8562 | F.-419-4372 | M. Smartphone Ownership Is Growing Rapidly Around the World, but Not Always Equally. Pew Research Center’s Global Attitudes Project, 5 February 2019. Available online: https://www.pewresearch.org/global/2019/02/05/smartphone-ownership-is-growing-rapidly-around-the-world-but-not-always-equally/ (accessed on 12 August 2021).
- Nussbaum, R.; Kelly, C.; Quinby, E.; Mac, A.; Parmanto, B.; Dicianno, B.E. Systematic Review of Mobile Health Applications in Rehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 115–127. [Google Scholar] [CrossRef]
- Meinhart, F.; Stütz, T.; Sareban, M.; Kulnik, S.T.; Niebauer, J. Mobile Technologies to Promote Physical Activity during Cardiac Rehabilitation: A Scoping Review. Sensors 2021, 21, 65. [Google Scholar] [CrossRef]
- Moral-Munoz, J.A.; Zhang, W.; Cobo, M.J.; Herrera-Viedma, E.; Kaber, D.B. Smartphone-based systems for physical rehabilitation applications: A systematic review. Assist. Technol. Off. J. RESNA 2019, 33, 223–236. [Google Scholar] [CrossRef]
- Zhou, X.; Du, M.; Zhou, L. Use of mobile applications in post-stroke rehabilitation: A systematic review. Top. Stroke Rehabil. 2018, 25, 489–499. [Google Scholar] [CrossRef]
- Guo, J.; Smith, T.; Messing, D.; Tang, Z.; Lawson, S.; Feng, J.H. ARMStrokes: A Mobile App for Everyday Stroke Rehabilitation. In Proceedings of the 17th International ACM SIGACCESS Conference on Computers & Accessibility, Lisbon, Portugal, 26–28 October 2015; Association for Computing Machinery: New York, NY, USA, 2015; pp. 429–430. [Google Scholar]
- Chen, C.-J.; Lin, Y.-T.; Lin, C.-C.; Chen, Y.-C.; Lee, Y.-J.; Wang, C.-Y. Rehabilitation System for Limbs using IMUs. In Proceedings of the 2020 21st International Symposium on Quality Electronic Design (ISQED), Santa Clara, CA, USA, 25–26 March 2020; pp. 285–291. [Google Scholar]
- Puhan, M.A.; Scharplatz, M.; Troosters, T.; Steurer, J. Respiratory rehabilitation after acute exacerbation of COPD may reduce risk for readmission and mortality—A systematic review. Respir. Res. 2005, 6, 54. [Google Scholar] [CrossRef] [Green Version]
- Robison, J.; Wiles, R.; Ellis-Hill, C.; McPherson, K.; Hyndman, D.; Ashburn, A. Resuming previously valued activities post-stroke: Who or what helps? Disabil. Rehabil. 2009, 31, 1555–1566. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 12, CD007146. [Google Scholar] [CrossRef]
- Nas, K.; Yazmalar, L.; Şah, V.; Aydın, A.; Öneş, K. Rehabilitation of spinal cord injuries. World J. Orthop. 2015, 6, 8–16. [Google Scholar] [CrossRef]
- Kleinitz, P.; Mills, J.-A.; Connolly, B.; Skelton, P.; Smith, G.; Clift, Z. Rehabilitation Considerations during the COVID-19 Outbreak; Pan American Health Organization: Washington, DC, USA, 2020; Available online: https://iris.paho.org/handle/10665.2/52035 (accessed on 27 January 2021).
- Aderonmu, J.A. Emerging challenges in meeting physiotherapy needs during COVID-19 through telerehabilitation. Bull. Fac. Phys. Ther. 2020, 25, 1–4. [Google Scholar] [CrossRef]
- Tahan, H.M. Essential Case Management Practices Amidst the Novel Coronavirus Disease 2019 (COVID-19) Crisis: Part 1: Tele-Case Management, Surge Capacity, Discharge Planning, and Transitions of Care. Prof. Case Manag. 2020, 25, 248–266. [Google Scholar] [CrossRef]
- Jones, M.; Collier, G.; Reinkensmeyer, D.J.; DeRuyter, F.; Dzivak, J.; Zondervan, D.; Morris, J. Big Data Analytics and Sensor-Enhanced Activity Management to Improve Effectiveness and Efficiency of Outpatient Medical Rehabilitation. Int. J. Environ. Res. Public. Health 2020, 17, 748. [Google Scholar] [CrossRef] [Green Version]
- mRehab RERC. Available online: https://www.mrehabrerc.org (accessed on 28 January 2021).
- Morris, J.; Thompson, N.; Wallace, T.; Jones, M.; DeRuyter, F. Survey of Rehabilitation Clinicians in the United States: Barriers and Critical Use-Cases for mRehab Adoption. In Computers Helping People with Special Needs; Miesenberger, K., Manduchi, R., Covarrubias Rodriguez, M., Peňáz, P., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020; Volume 12377, pp. 250–258. ISBN 978-3-030-58804-5. [Google Scholar]
- US Centers for Medicare & Medicaid Services. COVID-19 Emergency Declaration Blanket Waivers for Health Care Providers. (Updated) 4 August 2021. Available online: https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf) (accessed on 16 December 2020).
- Medicare Remote Patient Monitoring Reimbursement FAQs: Everything You Need to Know About Chronic Care Remote Physiologic Monitoring Codes | Blogs | Health Care Law Today | Foley & Lardner LLP. Available online: https://www.foley.com/en/insights/publications/2018/11/medicareremote-patient-monitoring-reimbursement-fa (accessed on 18 April 2021).
- Federal Register Volume 83, Issue 226 (23 November 2018). Available online: https://www.govinfo.gov/content/pkg/FR-2018-11-23/pdf/2018-24170.pdf (accessed on 18 April 2021).
- Medicare Remote Patient Monitoring: CMS Finalizes New Code and General Supervision | Foley & Lardner LLP. Available online: https://www.foley.com/en/insights/publications/2019/11/cms-finalizes-new-rpm-code-general-supervision (accessed on 10 February 2021).
- Donohue, D. A Primary Care Answer to a Pandemic: Keeping a Population of Patients Safe at Home through Chronic Care Management and Remote Patient Monitoring. Am. J. Lifestyle Med. 2020, 14, 595–601. [Google Scholar] [CrossRef]
- Pt App | United States | Pt Pal. Available online: https://www.ptpal.com (accessed on 28 January 2021).
- FitMi Stroke Therapy for Clinic Use. Flint Rehab. Available online: https://www.flintrehab.com/product/fitmi-clinic/ (accessed on 28 January 2021).
- Intrinsic Motivation Inventory (IMI)—Selfdeterminationtheory.org. Available online: https://selfdeterminationtheory.org/intrinsic-motivation-inventory/ (accessed on 24 March 2021).
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: A confirmatory factor analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef]
- US Department of Health and Human Services Centers for Medicare & Medicaid Services. Federal Register Volume 85, Issue 248 (28 December 2020). Office of the Federal Register, National Archives and Records Administration, 28 December 2020. (85 FR 84472-85377). Available online: https://www.govinfo.gov/content/pkg/FR-2020-12-28/pdf/2020-26815.pdf (accessed on 18 April 2021).
- Outpatient Rehabilitation Therapy Services: Complying with Documentation Requirements; Centers for Medicare & Medicaid Services: Baltimore, MD, USA, 2019. Available online: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/OutptRehabTherapy-Booklet-MLN905365.pdf (accessed on 18 April 2021).
- de Lucena, D.S.; Stoller, O.; Rowe, J.B.; Chan, V.; Reinkensmeyer, D.J. Wearable sensing for rehabilitation after stroke: Bimanual jerk asymmetry encodes unique information about the variability of upper extremity recovery. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; IEEE: London, UK, 2017; pp. 1603–1608. [Google Scholar] [CrossRef]
- Okita, S.; Schwerz de Lucena, D.; Chan, V.; Reinkensmeyer, D. Measuring Movement Quality of the Stroke-Impaired Upper Extremity with a Wearable Sensor: Toward a Smoothness Metric for Home Rehabilitation Exercise Programs. In Proceedings of the 43rd International Engineering in Medicine and Biology Conference (EMBC), Online, 1–5 November 2021. [Google Scholar]
- Anderson, R.K.; Collier, G.; Kahn, N.; Dzivak, J. Getting from Start to Finish: Examination of Patient Status, Therapy Prescription, Therapy Participation, with Pain and Difficulty on Patient Likelihood of Finishing at Home Therapy Exercises. In Proceedings of the Poster Presented at: Rehabilitation Research 2020: Envisioning a Functional Future, National Institutes of Health, Online, 15–16 October 2020. [Google Scholar]
- Cowan, K.E.; McKean, A.J.; Gentry, M.T.; Hilty, D.M. Barriers to Use of Telepsychiatry: Clinicians as Gatekeepers. Mayo Clin. Proc. 2019, 94, 2510–2523. [Google Scholar] [CrossRef] [Green Version]
- Celian, C.; Swanson, V.; Shah, M.; Newman, C.; Fowler-King, B.; Gallik, S.; Reilly, K.; Reinkensmeyer, D.J.; Patton, J.; Rafferty, M.R. A day in the life: A qualitative study of clinical decision-making and uptake of neurorehabilitation technology. J. Neuroeng. Rehabil. 2021, 18, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Code | Description |
|---|---|
| 99453 | Initial set up and patient education |
| 99454 | Supply of devices and collection, transmission, and summary of services each 30 days |
| 99457 | First 20 min of remote physiologic monitoring by clinical staff, physician, or qualified healthcare provider in a calendar month |
| 99458 | For additional 20 min of remote physiologic monitoring by clinical staff, physician, or qualified healthcare provider in the same calendar month as 99457 |
| Therapist | Self-Rating after Initial Training | Time Spent Training after Session I (h) | Time Spent Training after Session II (h) |
|---|---|---|---|
| Therapist 1 | 3 | 6 | 1 |
| Therapist 2 | 3 | 1 | 1.5 |
| Therapist 3 | 4 | 0 | 0.25 |
| Patient ID | Payer Source | Care Setting | Care Domain (PT/OT) |
|---|---|---|---|
| SEAM 01 | Aetna MC PPO | Outpatient | PT |
| SEAM 03 | Medicare | Outpatient | OT |
| SEAM 04 | Cigna PPO | Outpatient | OT |
| SEAM 05 | Blue Cross | Outpatient | PT |
| SEAM 06 | Blue Cross HMO | Inpatient | PT |
| SEAM 07 | Blue Cross Blue Shield PPO | Outpatient | PT |
| SEAM 08 | Blue Shield PPO | Outpatient | OT |
| SEAM 09 | Healthy HMO | Outpatient | OT |
| SEAM 10 | Blue Cross PPO | Outpatient | PT |
| Study ID | Average Activities per Day | Average Sets per Activity | Average Reps per Set | Total Number of Days | Total Number of Activities |
|---|---|---|---|---|---|
| SEAM 01 | 40 | 1 | 9 | 49 | 1973 |
| SEAM 03 | 4 | 1 | 10 | 150 | 639 |
| SEAM 04 | 14 | 1 | 10 | 16 | 218 |
| SEAM 05 | 20 | 1 | 8 | 71 | 1437 |
| SEAM 07 | 12 | 1 | 9 | 46 | 549 |
| SEAM 08 | 11 | 1 | 10 | 135 | 1515 |
| SEAM 09 | 12 | 1 | 12 | 116 | 1419 |
| SEAM 10 | 11 | 1 | 7 | 74 | 823 |
| Study ID | Percent Active Days | Percent of Exercises Completed | Percent of Attempted Exercises with Puck Data |
|---|---|---|---|
| SEAM 01 | 24% | 6% | 35% |
| SEAM 03 | 24% | 16% | 0% |
| SEAM 04 | 6% | 5% | 0% |
| SEAM 05 | 54% | 37% | 76% |
| SEAM 07 | 35% | 13% | 36% |
| SEAM 08 | 52% | 36% | 16% |
| SEAM 09 | 34% | 11% | 0% |
| SEAM 10 | 92% | 78% | 0% |
| Patient | Therapist | Questions and Answers |
|---|---|---|
| Patient Question: What Did You Like Most about the System? | ||
| SEAM 01 | Therapist 1 | “It took me along progressively and I was able to watch the videos we recorded which helped.” Unfortunately, the patient accidentally deleted the videos. |
| SEAM 05 | Therapist 2 | “It kept me on task” |
| SEAM 07 | Therapist 2 | “I liked having the exercises organized by day and having the videos” |
| SEAM 04 | Therapist 3 | |
| Patient Question: What did you like least about the system? | ||
| SEAM 01 | Therapist 1 | “It was hard and uncomfortable to put the puck on my arm.” |
| SEAM 05 | Therapist 2 | “The puck was a hassle, large and bulky and did not always capture the repetitions and hard to understand “ |
| SEAM 07 | Therapist 2 | “The puck did not provide specific feedback so it didn’t seem beneficial” |
| SEAM 04 | Therapist 3 | |
| Therapist Question: What did you find most useful about the SEAM system for treating this patient? | ||
| SEAM 01 | Therapist 1 | “The ability to record videos” |
| SEAM 05 | Therapist 2 | “Patient was motivated to use the system because they knew I was monitoring their completion of their exercises” |
| SEAM 07 | Therapist 2 | “Pt Pal” |
| SEAM 04 | Therapist 3 | “Being able to monitor compliance” |
| Therapist Question: What was the most difficult or frustrating part of using the SEAM system with this patient? | ||
| SEAM 01 | Therapist 1 | “The multiple steps to use the system each time I saw the patient.” |
| SEAM 05 | Therapist 2 | “The puck was not useful for most of the exercises.” |
| SEAM 07 | Therapist 2 | “The puck was not very useful and the patient decided not to do Zoom after the 3rd visit and switched to in clinic visits for the remainder of the therapy” |
| SEAM 04 | Therapist 3 | “Time constraints for reviewing progress” |
| Themes | Code: Descriptions or Examples | Number of Mentions by Therapist (T#) | ||||
|---|---|---|---|---|---|---|
| T1 | T2 | T3 | ||||
| Positive | Value to Patients | adherence: compliance, adherence, accountability | 0 | 2 | 4 | |
| patient satisfaction: patients find the system interesting and engaging | 3 | 2 | 2 | |||
| game mode: gamification aspects, mentions of engagement relative to gamified exercises | 0 | 1 | 1 | |||
| patient motivation: motivation, excitement, having a physical device was motivating, motivation as a result of being monitored | 4 | 1 | 1 | |||
| feedback to patients: system provides feedback to patients | 1 | 0 | 0 | |||
| Facilitating Care | facilitate telerehab: communication with patients, remote monitoring | 1 | 2 | 0 | ||
| billing: making non-productive time productive, difficulties related to billing | 1 | 3 | 0 | |||
| order sets: convenience of creating order sets for prescribing | 0 | 1 | 0 | |||
| adding exercises: ability to create custom exercises | 0 | 1 | 0 | |||
| useful features: automatic Bluetooth connection, activity tracking, “copy to all exercises” | 4 | 0 | 0 | |||
| monitoring: ability to monitor patient activity even when they are not in the clinic | 1 | 1 | 3 | |||
| future and potential uses: to bridge gaps between evaluation and treatments | 1 | 0 | 0 | |||
| feedback from patients: feedback allows modification of programs or preventing injury | 0 | 0 | 2 | |||
| Negative | Implementation Issues | Patient Selection | patient attributes: consistency in following instructions, diagnosis, cognition, fear of technology, preference for paper instructions, state their phone or data plan could not support the intervention | 3 | 2 | 4 |
| patient unable to operate alone | 4 | 0 | 0 | |||
| lack of caregiver support: patients have no one to assist them with the system in the home setting | 2 | 0 | 0 | |||
| System Suitability | puck suitability for diagnoses: device does not capture data relevant to balance and stability exercises, patients have difficulty grasping puck | 0 | 4 | 0 | ||
| game mode: exercises that therapists wanted were not available, suitability for diagnosis | 2 | 1 | 0 | |||
| Training/ Education | survey: patients did not complete or selected answers straight down the middle, therapists were not trained how to optimally assign surveys | 1 | 1 | 2 | ||
| billing: confusion, missed billing opportunities, improper sequence, no preauthorization | 0 | 1 | 1 | |||
| exercise library: dissatisfaction with uniformity, not finding desired exercises, organization not what was expected, experience with other HEP software | 2 | 1 | 0 | |||
| portal interface: difficulties navigating and using interface | 2 | 0 | 1 | |||
| Potential System Improvements | reasons for non-complete: the reasons for non-complete did not line up with patients’ reasons | 0 | 1 | 0 | ||
| number of steps: patient forgot app access code, Bluetooth workflow | 5 | 0 | 0 | |||
| Technical Issues | app/software: software instability, number of steps required | 1 | 2 | 0 | ||
| pucks not recording/performing as expected: reported counts are different than expected, difficulties connecting to Bluetooth | 2 | 1 | 3 | |||
| Bluetooth problems: problems regarding making the Bluetooth connection | 6 | 0 | 1 | |||
| facility internet | 1 | 0 | 0 | |||
| patient frustration: patient frustration due to system not operating properly or as the patient believes it should | 0 | 2 | 2 | |||
| Payer | Code | Reason |
|---|---|---|
| Aetna Medicare Managed Care | 99457 | Non-Covered |
| 99458 | Non-Covered | |
| Medicare | 99457 | Non-Covered |
| 99458 | Non-Covered | |
| Cigna | 99454 | No Reason Given (one count of 99457 was reimbursed and one was not) |
| Blue Cross | 99453 | Contract for PT maxes at USD 317 per day |
| 99454 | Contract for PT maxes at USD 317 per day | |
| 99457 | Contract for PT maxes at USD 317 per day | |
| Blue Shield | 99457 | Non-Covered |
| 99458 | Non-Covered | |
| United Healthcare Medicare Managed Care | 99457 | Non-Covered (one count of 99457 was reimbursed and one was not) |
| Therapist | Domain | % | General Patient Diagnoses | Reasons Patients Might Not Be Eligible |
|---|---|---|---|---|
| 1 | PT | 22% | Movement disorders, neurologic conditions | Age, technological fluency, lack of smart phone, cognitive deficits from diagnosis |
| 2 | PT | 75% | Lymphedema | Technological fluency, lack of smart phone, diagnosis related barriers |
| 3 | OT | 100% | Neurologic conditions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swanson, V.A.; Chan, V.; Cruz-Coble, B.; Alcantara, C.M.; Scott, D.; Jones, M.; Zondervan, D.K.; Khan, N.; Ichimura, J.; Reinkensmeyer, D.J. A Pilot Study of a Sensor Enhanced Activity Management System for Promoting Home Rehabilitation Exercise Performed during the COVID-19 Pandemic: Therapist Experience, Reimbursement, and Recommendations for Implementation. Int. J. Environ. Res. Public Health 2021, 18, 10186. https://doi.org/10.3390/ijerph181910186
Swanson VA, Chan V, Cruz-Coble B, Alcantara CM, Scott D, Jones M, Zondervan DK, Khan N, Ichimura J, Reinkensmeyer DJ. A Pilot Study of a Sensor Enhanced Activity Management System for Promoting Home Rehabilitation Exercise Performed during the COVID-19 Pandemic: Therapist Experience, Reimbursement, and Recommendations for Implementation. International Journal of Environmental Research and Public Health. 2021; 18(19):10186. https://doi.org/10.3390/ijerph181910186
Chicago/Turabian StyleSwanson, Veronica A., Vicky Chan, Betsaida Cruz-Coble, Celeste M. Alcantara, Douglas Scott, Mike Jones, Daniel K. Zondervan, Naveen Khan, Jan Ichimura, and David J. Reinkensmeyer. 2021. "A Pilot Study of a Sensor Enhanced Activity Management System for Promoting Home Rehabilitation Exercise Performed during the COVID-19 Pandemic: Therapist Experience, Reimbursement, and Recommendations for Implementation" International Journal of Environmental Research and Public Health 18, no. 19: 10186. https://doi.org/10.3390/ijerph181910186