
Effect of Community and Socio-Economic Factors on Cardiovascular, Cancer and Cardio-Oncology Patients with COVID-19

 ,
,
Abstract
:1. Introduction
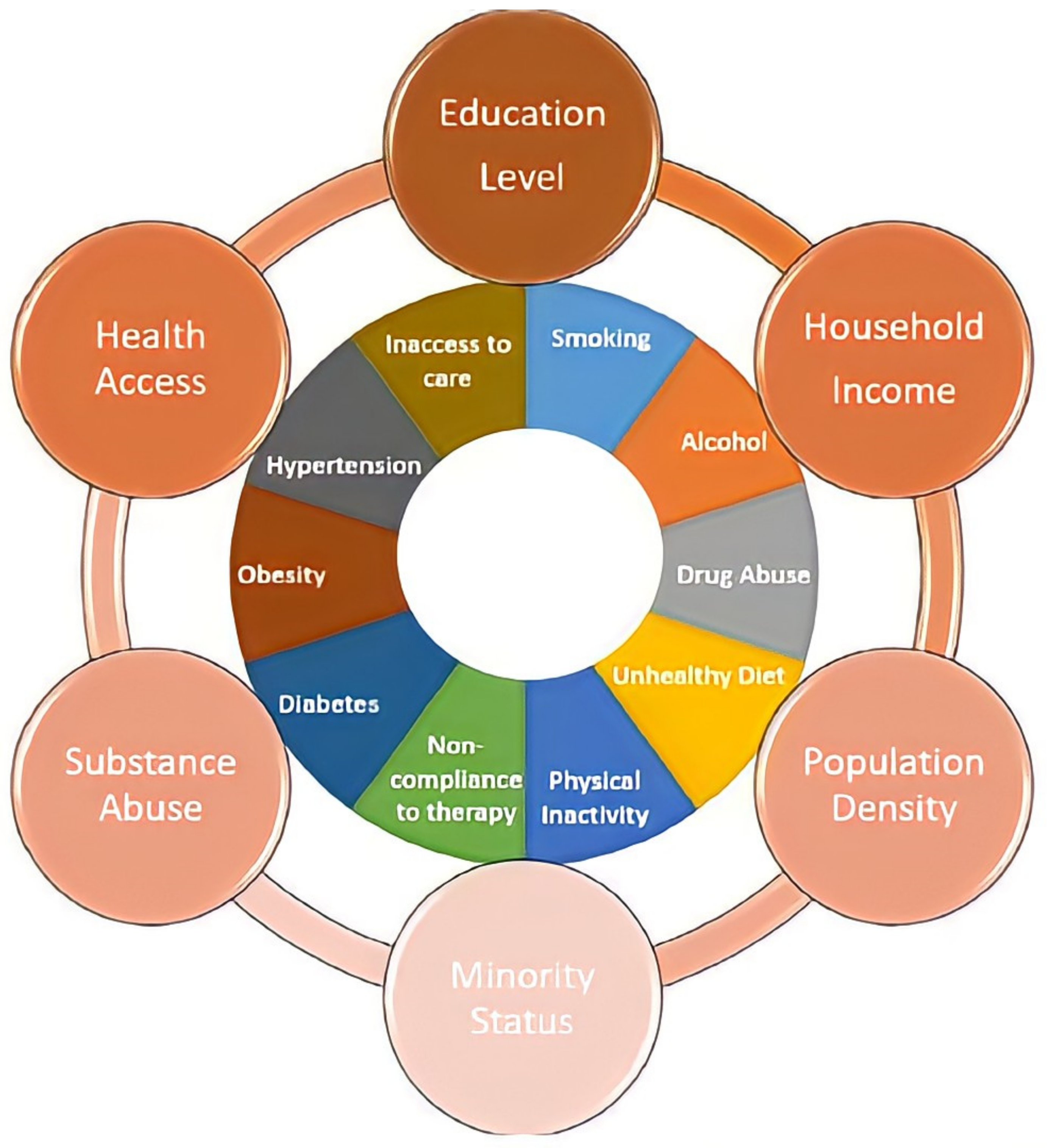
2. Community and Socio-Economic Factors Affecting Health Disparity
3. Socio-Economic and Community Factors Affecting COVID-19
4. Socio-Economic and Community Factors Affecting Cardiovascular Disease, Cancer, and Cardio-Oncology
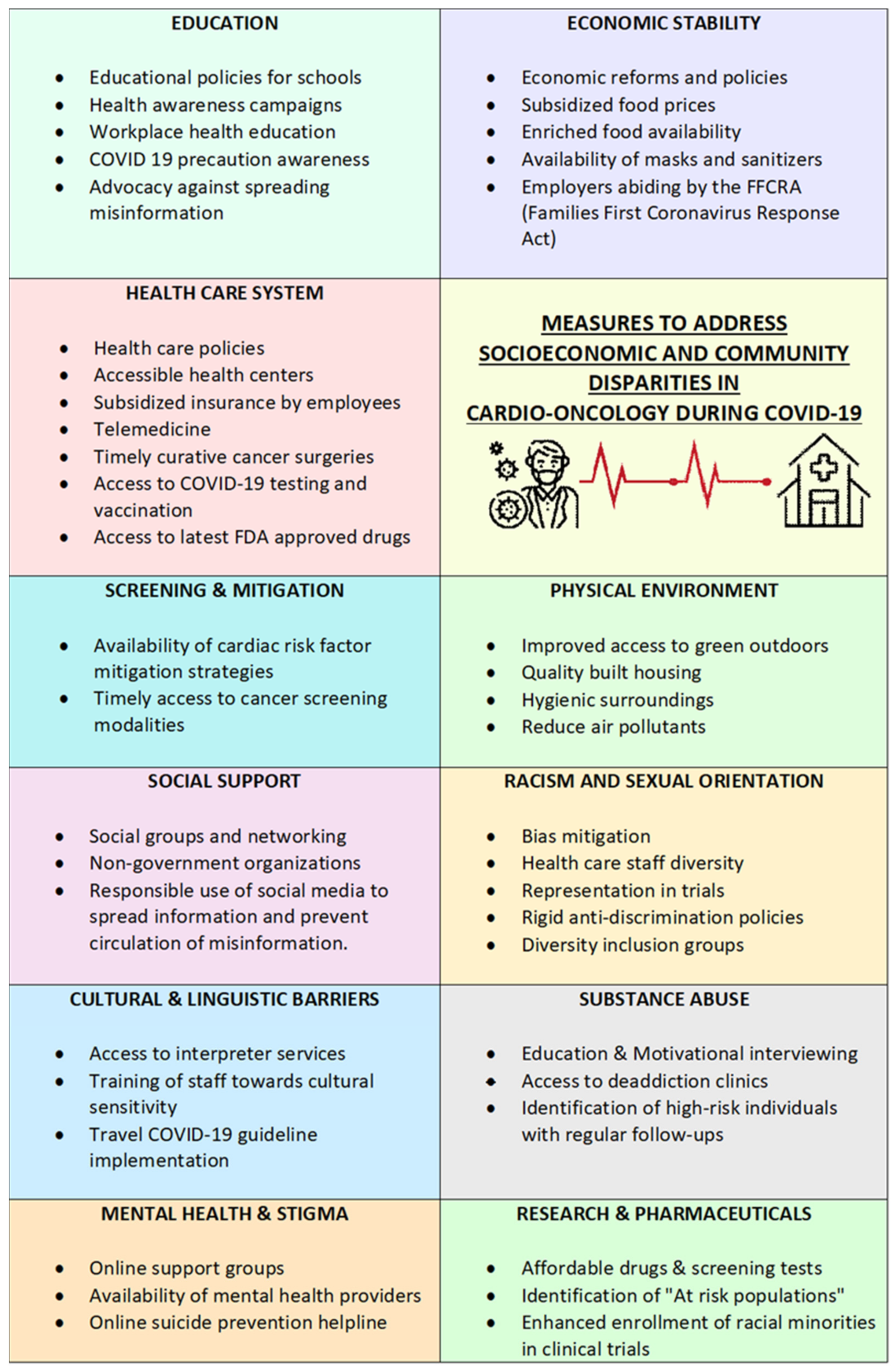
5. Measures to Address Socio-Economic and Community Disparities
Funding
Conflicts of Interest
References
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study. Lancet 2017, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Waddell, C.E. Population crowding and death rates due to heart disease. Ecol. Dis. 1983, 2, 271–275. [Google Scholar] [PubMed]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socio-economic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J. Socioeconomic inequalities in cardiovascular disease mortality. Int. Study. Eur. Heart J. 2000, 21, 1141–1151. [Google Scholar] [CrossRef]
- Roux, A.V.D.; Merkin, S.S.; Arnett, D.; Chambless, L.; Massing, M.; Nieto, F.J.; Sorlie, P.; Szklo, M.; Tyroler, H.A.; Watson, R.L. Neighborhood of Residence and Incidence of Coronary Heart Disease. N. Engl. J. Med. 2001, 345, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Lutsey, P.L.; Roux, A.V.D.; Jacobs, D.R.; Burke, G.L.; Harman, J.; Shea, S.; Folsom, A.R. Associations of Acculturation and Socioeconomic Status with Subclinical Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. Am. J. Public Health 2008, 98, 1963–1970. [Google Scholar] [CrossRef]
- Kelly, M.J.; Weitzen, S. The Association of Lifetime Education with the Prevalence of Myocardial Infarction: An Analysis of the 2006 Behavioral Risk Factor Surveillance System. J. Community Health 2010, 35, 76–80. [Google Scholar] [CrossRef]
- Kucharska-Newton, A.M.; Harald, K.; Rosamond, W.D.; Rose, K.M.; Rea, T.D.; Salomaa, V. Socioeconomic indicators and the risk of acute coronary heart disease events: Comparison of population-based data from the United States and Finland. Ann. Epidemiol. 2011, 21, 572–579. [Google Scholar] [CrossRef] [Green Version]
- Stirbu, I.; Looman, C.; Nijhof, G.J.; Reulings, P.G.; MacKenbach, J.P. Income inequalities in case death of ischaemic heart disease in the Netherlands: A national record-linked study. J. Epidemiol. Community Health 2012, 66, 1159–1166. [Google Scholar] [CrossRef]
- Joynt, K.E.; Orav, E.J.; Jha, A.K. Patient race, site of care, and 30-day readmission rates among elderly Americans. JAMA 2011, 305, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosamond, W.D.; Chambless, L.E.; Heiss, G.; Mosley, T.H.; Coresh, J.; Whitsel, E.A.; Wagenknecht, L.E.; Ni, H.; Folsom, A.R. Twenty-two–year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation 2012, 125, 1848–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frierson, G.M.; Howard, E.N.; DeFina, L.F.; Powell-Wiley, T.M.; Willis, B.L. Effect of race and socio-economic status on cardiovascular risk factor burden: The Cooper Center Longitudinal Study. Ethn. Dis. 2013, 23, 35. [Google Scholar]
- Yu, T.H.; Hou, Y.C.; Chung, K.P. Do low-income coronary artery bypass surgery patients have equal opportunity to access excellent quality of care and enjoy good outcome in Taiwan? Int. J. Equity Health 2014, 13, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meneton, P.; Kesse-Guyot, E.; Méjean, C.; Fezeu, L.; Galan, P.; Hercberg, S.; Ménard, J. Unemployment is associated with high cardiovascular event rate and increased all-cause mortality in middle-aged socially privileged individuals. Int. Arch. Occup. Environ. Health 2015, 88, 707–716. [Google Scholar] [CrossRef]
- Lewis, M.W.; Khodneva, Y.; Redmond, N.; Durant, R.W.; Judd, S.E.; Wilkinson, L.L.; Howard, V.J.; Safford, M.M. The impact of the combination of income and education on the incidence of coronary heart disease in the prospective Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort study. BMC Public Health 2015, 15, 1312. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.; Guo, X.L.; Lu, Z.L.; Zhang, J.Y.; Tang, J.L.; Chen, X.; Gao, C.C.; Xu, C.X.; Xu, A.Q. Ideal cardiovascular health status and its association with socio-economic factors in Chinese adults in Shandong, China. BMC Public Health 2016, 16, 942. [Google Scholar] [CrossRef] [Green Version]
- Barber, S.; Hickson, D.A.; Wang, X.; Sims, M.; Nelson, C.; Diez-Roux, A.V. Neighborhood disadvantage, poor social conditions, and cardiovascular disease incidence among African American adults in the Jackson heart study. Am. J. Public Health 2016, 106, 2219–2226. [Google Scholar] [CrossRef]
- Yan, R.; Li, W.; Yin, L.; Wang, Y.; Bo, J.; PURE-China Investigators; Liu, L.; Liu, B.; Hu, B. Cardiovascular diseases and risk-factor burden in urban and rural communities in high-, middle-, and low-income regions of china: A large community-based epidemiological study. J. Am. Heart Assoc. 2017, 6, e004445. [Google Scholar] [CrossRef]
- Carnethon, M.R.; Pu, J.; Howard, G.; Albert, M.A.; Anderson, C.A.; Bertoni, A.G.; Mujahid, M.S.; Palaniappan, L.; Taylor, H.A., Jr.; Willis, M.; et al. Cardiovascular Health in African Americans: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e393–e423. [Google Scholar] [CrossRef]
- Breathett, K.; Liu, W.G.; Allen, L.A.; Daugherty, S.L.; Blair, I.V.; Jones, J.; Grunwald, G.K.; Moss, M.; Kiser, T.H.; Burnham, E.; et al. African Americans are less likely to receive care by a cardiologist during an intensive care unit admission for heart failure. JACC Heart Fail. 2018, 6, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Foraker, R.E.; Bush, C.; Greiner, M.A.; Sims, M.; Henderson, K.; Smith, S.; Bidulescu, A.; Shoben, A.B.; Hardy, N.C.; O’Brien, E. Distribution of cardiovascular health by individual-and neighborhood-level socio-economic status: Findings from the Jackson Heart Study. Glob. Heart 2019, 14, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.H.; Jung, M.H.; Kwon, C.H.; Lee, C.J.; Kim, D.H.; Kim, H.L.; Kim, W.; Kang, S.H.; Lee, J.H.; Kim, H.M.; et al. Disparities in Mortality and Cardiovascular Events by Income and Blood Pressure Levels Among Patients with Hypertension in South Korea. J. Am. Heart Assoc. 2021, 10, e018446. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.Q.; Buxton, J.A.; Scheuermeyer, F.X.; Palis, H.; Zhao, B.; Desai, R.; Janjua, N.Z.; Slaunwhite, A.K. Risk of cardiovascular diseases in relation to substance use disorders. Drug Alcohol Depend. 2021, 229, 109132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.B.; Chen, C.; Pan, X.F.; Guo, J.; Li, Y.; Franco, O.H.; Liu, G.; Pan, A. Associations of healthy lifestyle and socio-economic status with mortality and incident cardiovascular disease: Two prospective cohort studies. BMJ 2021, 373, n604. [Google Scholar] [CrossRef] [PubMed]
- Ohm, J.; Skoglund, P.H.; Häbel, H.; Sundström, J.; Hambraeus, K.; Jernberg, T.; Svensson, P. Association of socio-economic status with risk factor target achievements and use of secondary prevention after myocardial infarction. JAMA Netw. Open 2021, 4, e211129. [Google Scholar] [CrossRef] [PubMed]
- Terrier, C.; Chen, D.L.; Sutter, M. COVID-19 within families amplifies the prosociality gap between adolescents of high and low socio-economic status. Proc. Natl. Acad. Sci. USA 2021, 118, 46. [Google Scholar] [CrossRef]
- Evans, R.G. Thomas McKeown, meet Fidel Castro: Physicians, population health and the Cuban paradox. Healthc. Policy 2008, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.C.; Cubbin, C.; Ahn, D.; Winkleby, M.A. Effects of neighbourhood socio-economic status and convenience store concentration on individual level smoking. Tob. Control 2005, 14, 337. [Google Scholar]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary lifestyle: Overview of updated evidence of potential health risks. Korean J. Fam. Med. 2020, 41, 365. [Google Scholar] [CrossRef]
- Duchaine, C.S.; Aubé, K.; Gilbert-Ouimet, M.; Vézina, M.; Ndjaboué, R.; Massamba, V.; Talbot, D.; Lavigne-Robichaud, M.; Trudel, X.; Pena-Gralle, A.P.; et al. Psychosocial stressors at work and the risk of sickness absence due to a diagnosed mental disorder: A systematic review and meta-analysis. JAMA Psychiatry 2020, 77, 842–851. [Google Scholar] [CrossRef] [PubMed]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129 (Suppl. 2), 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steptoe, A.; Marmot, M. The role of psychobiological pathways in socio-economic inequalities in cardiovascular disease risk. Eur. Heart J. 2002, 23, 13–25. [Google Scholar] [CrossRef]
- Campbell, F.A.; Ramey, C.T.; Pungello, E.; Sparling, J.; Miller-Johnson, S. Early childhood education: Young adult outcomes from the Abecedarian Project. Appl. Dev. Sci. 2002, 6, 42–57. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W.; et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530–15535. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.; Dranitsaris, G.; Mubashir, T.; Bartoszko, J.; Riazi, S. A country level analysis measuring the impact of government actions, country preparedness and socio-economic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine 2020, 25, 100464. [Google Scholar] [CrossRef]
- Garnier, R.; Benetka, J.R.; Kraemer, J.; Bansal, S. Socioeconomic disparities in social distancing during the COVID-19 pandemic in the United States. medRxiv 2020, 23, e24591. [Google Scholar] [CrossRef]
- Gu, T.; Mack, J.A.; Salvatore, M.; Sankar, S.P.; Valley, T.S.; Singh, K.; Nallamothu, B.K.; Kheterpal, S.; Lisabeth, L.; Fritsche, L.G. COVID-19 outcomes, risk factors and associations by race: A comprehensive analysis using electronic health records data in Michigan Medicine. medRxiv 2020, 118, e2110891118. [Google Scholar] [CrossRef]
- Guha, A.; Bonsu, J.; Dey, A.; Addison, D. Community and Socioeconomic Factors Associated with COVID-19 in the United States: Zip code level cross sectional analysis. medRxiv 2020. In press. [Google Scholar]
- Hawkins, R.B.; Charles, E.J.; Mehaffey, J.H. Socio-economic status and COVID-19–related cases and fatalities. Public Health 2020, 189, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Whittle, R.S.; Diaz-Artiles, A. An ecological study of socio-economic predictors in detection of COVID-19 cases across neighborhoods in New York City. BMC Med. 2020, 18, 271. [Google Scholar] [CrossRef] [PubMed]
- Bhuiya, T.; Klares Iii, R.; Conte, M.A.; Cervia, J.S. Predictors of misperceptions, risk perceptions, and personal risk perceptions about COVID-19 by country, education and income. J. Investig. Med. 2021, 69, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Cromer, S.J.; Lakhani, C.M.; Wexler, D.J.; Burnett-Bowie, S.A.M.; Udler, M.; Patel, C.J. Geospatial Analysis of Individual and Community-Level Socio-economic Factors Impacting SARS-CoV-2 Prevalence and Outcomes. medRxiv 2020. [Google Scholar] [CrossRef]
- Liao, T.F.; De Maio, F. Association of Social and Economic Inequality with Coronavirus Disease 2019 Incidence and Mortality Across US Counties. JAMA Netw. Open 2021, 4, e2034578. [Google Scholar] [CrossRef] [PubMed]
- Dueñas, M.; Campi, M.; Olmos, L.E. Changes in mobility and socio-economic conditions during the COVID-19 outbreak. Humanit. Soc. Sci. Commun. 2021, 8, 101. [Google Scholar] [CrossRef]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors with COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. [Google Scholar] [CrossRef]
- Khanijahani, A.; Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Naghibi, D. A systematic review of racial/ethnic and socio-economic disparities in COVID-19. Int. J. Equity Health 2021, 20, 248. [Google Scholar] [CrossRef]
- Mena, G.E.; Martinez, P.P.; Mahmud, A.S.; Marquet, P.A.; Buckee, C.O.; Santillana, M. Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile. Science 2021, 372, eabg5298. [Google Scholar] [CrossRef]
- Tan, A.X.; Hinman, J.A.; Abdel Magid, H.S.; Nelson, L.M.; Odden, M.C. Association Between Income Inequality and County-Level COVID-19 Cases and Deaths in the US. JAMA Netw. Open 2021, 4, e218799. [Google Scholar] [CrossRef] [PubMed]
- Lustig, N.; Martinez Pabon, V.; Federico, S.; Younger, D.D. The Impact of COVID-19 and Expanded Social Assistance on Inequality and Poverty in Argentina, Brazil, Colombia and Mexico, No 92, Commitment to Equity (CEQ) Working Paper Series, Tulane University, Department of Economics. 2021. Available online: https://EconPapers.repec.org/RePEc:tul:ceqwps:92 (accessed on 15 February 2022).
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Ganatra, S.; Dani, S.S.; Redd, R.; Rieger-Christ, K.; Patel, R.; Parikh, R.; Asnani, A.; Bang, V.; Shreyder, K.; Brar, S.S.; et al. Outcomes of COVID-19 in patients with a history of cancer and comorbid cardiovascular disease. J. Natl. Compr. Cancer Netw. 2020, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Jee, J.; Foote, M.B.; Lumish, M.; Stonestrom, A.J.; Wills, B.; Narendra, V.; Avutu, V.; Murciano-Goroff, Y.R.; Chan, J.E.; Derkach, A.; et al. Chemotherapy and COVID-19 outcomes in patients with cancer. J. Clin. Oncol. 2020, 38, 3538–3546. [Google Scholar] [CrossRef]
- Bolton, K.L.; Koh, Y.; Foote, M.B.; Im, H.; Jee, J.; Sun, C.H.; Safonov, A.; Ptashkin, R.; Moon, J.H.; Lee, J.Y.; et al. Clonal hematopoiesis is associated with risk of severe Covid-19. Nat. Commun. 2021, 12, 5975. [Google Scholar] [CrossRef]
- Alom, S.; Chiu, C.M.; Jha, A.; Lai, S.H.; Yau, T.H.; Harky, A. The effects of COVID-19 on cancer care provision: A systematic review. Cancer Control 2021, 28, 1073274821997425. [Google Scholar] [CrossRef]
- Burki, T.K. Cancer guidelines during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 629–630. [Google Scholar] [CrossRef]
- Civantos, F.J.; Leibowitz, J.M.; Arnold, D.J.; Stubbs, V.C.; Gross, J.H.; Thomas, G.R.; Perez, C. Ethical Surgical Triage of Head and Neck Cancer Patients during the COVID-19 Pandemic. Head Neck 2020, 47, 1423–1447. [Google Scholar] [CrossRef]
- Chang, W.T.; Toh, H.S.; Liao, C.T.; Yu, W.L. Cardiac involvement of COVID-19: A comprehensive review. Am. J. Med. Sci. 2021, 361, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Pathan, N.; Hemingway, C.A.; Alizadeh, A.A.; Stephens, A.C.; Boldrick, J.C.; Oragui, E.E.; McCabe, C.; Welch, S.B.; Whitney, A.; O’Gara, P.; et al. Role of interleukin 6 in myocardial dysfunction of meningococcal septic shock. Lancet 2004, 363, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Klok, F.A.; Kruip, M.J.; Van der Meer, N.J.; Arbous, M.S.; Gommers, D.A.; Kant, K.M.; Kaptein, F.H.; van Paassen, J.; Stals, M.A.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Sperotto, F.; Friedman, K.G.; Son, M.B.; VanderPluym, C.J.; Newburger, J.W.; Dionne, A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: A comprehensive review and proposed clinical approach. Eur. J. Pediatrics 2021, 180, 307–322. [Google Scholar] [CrossRef] [PubMed]
- Bach, P.B.; Schrag, D.; Brawley, O.W.; Galaznik, A.; Yakren, S.; Begg, C.B. Survival of blacks and whites after a cancer diagnosis. J. Am. Med. Assoc. 2002, 287, 2106–2113. [Google Scholar] [CrossRef]
- Taylor, A.; Cheng, K.K. Social deprivation and breast cancer. J. Public Health Med. 2003, 25, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.B.F.; Hole, D.J.; Cooke, T.G. Breast cancer incidence trends in deprived and affluent Scottish women. Breast Cancer Res. Treat. 2006, 103, 233–238. [Google Scholar] [CrossRef]
- Mouw, T.; Koster, A.; Wright, M.; Blank, M.M.; Moore, S.C.; Hollenbeck, A.; Schatzkin, A. Education and Risk of Cancer in a Large Cohort of Men and Women in the United States. PLoS ONE 2008, 3, e3639. [Google Scholar] [CrossRef]
- Shack, L.; Jordan, C.; Thomson, C.S.; Mak, V.; Møller, H. Variation in incidence of breast, lung and cervical cancer and malignant melanoma of skin by socio-economic group in England. BMC Cancer 2008, 8, 271. [Google Scholar] [CrossRef] [Green Version]
- Sidorchuk, A.; Agardh, E.E.; Aremu, O.; Hallqvist, J.; Allebeck, P.; Moradi, T. Socioeconomic differences in lung cancer incidence: A systematic review and meta-analysis. Cancer Causes Control. 2009, 20, 459–471. [Google Scholar] [CrossRef]
- Aarts, M.J.; Lemmens, V.E.P.P.; Louwman, M.W.J.; Kunst, A.E.; Coebergh, J.W.W. Socio-economic status and changing inequalities in colorectal cancer? A review of the associations with risk, treatment and outcome. Eur. J. Cancer 2010, 46, 2681–2695. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Williams, S.D.; Siahpush, M.; Mulhollen, A. Socioeconomic, Rural-Urban, and Racial Inequalities in US Cancer Mortality: Part I—All Cancers and Lung Cancer and Part II—Colorectal, Prostate, Breast, and Cervical Cancers. J. Cancer Epidemiol. 2011, 2011, 107497. [Google Scholar] [CrossRef] [PubMed]
- Riaz, S.P.; Horton, M.; Kang, J.; Mak, V.; Lüchtenborg, M.; Møller, H. Lung Cancer Incidence and Survival in England: An Analysis by Socio-economic Deprivation and Urbanization. J. Thorac. Oncol. 2011, 6, 2005–2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung-Choi, K.; Khang, Y.H.; Cho, H.J. Socio-economic differentials in cause-specific mortality among 1.4 million South Korean public servants and their dependents. J. Epidemiol. Community Health 2011, 65, 632–638.14. [Google Scholar] [CrossRef]
- De Vries, E.; Arroyave, I.; Pardo, C.; Wiesner, C.; Murillo, R.; Forman, D.; Burdorf, A.; Avendano, M. Trends in inequalities in premature cancer mortality by educational level in Colombia, 1998–2007. J. Epidemiol. Community Health 2015, 69, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef]
- Teng, A.M.; Atkinson, J.; Disney, G.; Wilson, N.; Blakely, T. Changing socio-economic inequalities in cancer incidence and mortality: Cohort study with 54 million person-years follow-up 1981-2011. Int. J. Cancer 2017, 140, 1306–1316. [Google Scholar] [CrossRef]
- Hovanec, J.; Siemiatycki, J.; Conway, D.I.; Olsson, A.; Stucker, I.; Guida, F.; Jockel, K.; Pohlabeln, H.; Ahrens, W.; Bruske, I.; et al. Lung cancer and socio-economic status in a pooled analysis of case-control studies. PLoS ONE 2018, 13, e0192999. [Google Scholar] [CrossRef]
- Arık, A.; Dodd, E.; Streftaris, G. Cancer morbidity trends and regional differences in England—A Bayesian analysis. PLoS ONE 2020, 15, e0232844. [Google Scholar]
- Cheng, E.; Soulos, P.R.; Irwin, M.L.; Feliciano, E.M.C.; Presley, C.J.; Fuchs, C.S.; Meyerhardt, J.A.; Gross, C.P. Neighborhood and Individual Socioeconomic Disadvantage and Survival Among Patients with Nonmetastatic Common Cancers. JAMA Netw. Open 2021, 4, e2139593. [Google Scholar] [CrossRef]
- Unger, J.M.; Moseley, A.B.; Cheung, C.K.; Osarogiagbon, R.U.; Symington, B.; Ramsey, S.D.; Hershman, D.L. Persistent Disparity: Socioeconomic Deprivation and Cancer Outcomes in Patients Treated in Clinical Trials. J. Clin. Oncol. 2021, 39, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Soofi, M.; Karami-Matin, B.; Najafi, F.; Naghshbandi, P.; Soltani, S. Decomposing socio-economic disparity in the utilization of screening mammography: A cross-sectional analysis from the RaNCD cohort study. Health Care Women Int. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Dinh, K.; Lombardo, F.; Kark, J. Doxorubicin cardiotoxicity in African Americans. J. Natl. Med. Assoc. 2004, 96, 196–199. [Google Scholar] [PubMed]
- Van Dam, R.M.; Li, T.; Spiegelman, D.; Franco, O.H.; Hu, F.B. Combined impact of lifestyle factors on mortality: Prospective cohort study in US women. BMJ 2008, 337, a1440. [Google Scholar]
- Braithwaite, D.; Tammemagi, C.M.; Moore, D.H.; Ozanne, E.M.; Hiatt, R.A.; Belkora, J.; West, D.W.; Satariano, W.A.; Liebman, M.; Esserman, L. Hypertension is an independent predictor of survival disparity between African-American and white breast cancer patients. Int. J. Cancer 2009, 124, 1213–1219. [Google Scholar] [CrossRef]
- Rugo, H.S.; Brufsky, A.M.; Yood, M.U.; Tripathy, D.; Kaufman, P.A.; Mayer, M.; Yoo, B.; Abidoye, O.O.; Yardley, D.A. Racial disparities in treatment patterns and clinical outcomes in patients with HER2-positive metastatic breast cancer. Breast Cancer Res. Treat. 2013, 141, 461–470. [Google Scholar] [CrossRef] [Green Version]
- Baron, K.B.; Brown, J.R.; Heiss, B.L.; Marshall, J.; Tait, N.; Tkaczuk, K.H.; Gottlieb, S.S. Trastuzumab-Induced Cardiomyopathy: Incidence and Associated Risk Factors in an Inner-City Population. J. Card. Fail. 2014, 20, 555–559. [Google Scholar] [CrossRef]
- Berkman, A.; Cole, B.F.; Ades, P.A.; Dickey, S.; Higgins, S.T.; Trentham-Dietz, A.; Sprague, B.L.; Lakoski, S.G.; Ades, P.A. Racial differences in breast cancer, cardiovascular disease, and all-cause mortality among women with ductal carcinoma in situ of the breast. Breast Cancer Res. Treat. 2014, 148, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Woodward, M.; Peters, S.A.; Batty, G.D.; Ueshima, H.; Woo, J.; Giles, G.G.; Barzi, F.; Ho, S.C.; Huxley, R.R.; Arima, H.; et al. Socio-economic status in relation to cardiovascular disease and cause-specific mortality: A comparison of Asian and Australasian populations in a pooled analysis. BMJ Open 2015, 5, e006408. [Google Scholar] [CrossRef] [Green Version]
- Solanki, P.A.; Ko, N.Y.; Qato, D.M.; Calip, G.S. Risk of cancer-specific, cardiovascular, and all-cause mortality among Asian and Pacific Islander breast cancer survivors in the United States, 1991–2011. SpringerPlus 2016, 5, 82. [Google Scholar] [CrossRef] [Green Version]
- Caplin, D.A.; Smith, K.R.; Ness, K.K.; Hanson, H.A.; Smith, S.; Nathan, P.C.; Hudson, M.M.; Leisenring, W.; Robison, L.L.; Oeffinger, K.C. Effect of Population Socioeconomic and Health System Factors on Medical Care of Childhood Cancer Survivors: A Report from the Childhood Cancer Survivor Study. J. Adolesc. Young Adult Oncol. 2017, 6, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Litvak, A.; Batukbhai, B.; Russell, S.D.; Tsai, H.-L.; Rosner, G.L.; Jeter, S.C.; Armstrong, D.; Emens, L.A.; Fetting, J.; Wolff, A.C.; et al. Racial disparities in the rate of cardiotoxicity of HER2-targeted therapies among women with early breast cancer. Cancer 2018, 124, 1904–1911. [Google Scholar] [CrossRef] [PubMed]
- Troeschel, A.N.; Liu, Y.; Collin, L.J.; Bradshaw, P.T.; Ward, K.C.; Gogineni, K.; McCullough, E.L. Race differences in cardiovascular disease and breast cancer mortality among US women diagnosed with invasive breast cancer. Int. J. Epidemiol. 2019, 48, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Collin, L.J.; Troeschel, A.N.; Liu, Y.; Gogineni, K.; Borger, K.; Ward, K.C.; McCullough, L.E. A balancing act: Racial disparities in cardiovascular disease mortality among women diagnosed with breast cancer. Ann. Cancer Epidemiol. 2020, 4, 4. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipila, P.N.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M.; et al. Association between socio-economic status and the development of mental and physical health conditions in adulthood: A multi-cohort study. Lancet Public Health 2020, 5, e140–e149. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.B.; Dalsania, R.K.; Hamad, E.A. Healthcare disparities in cardio oncology: Patients receive same level of surveillance regardless of race at a safety net hospital. Cardio Oncol. 2021, 7, 3. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Giuliani, M.; Papadakos, T.; Papadakos, J. Propelling a new Era of patient education into practice—cancer care post–COVID-19. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 404–406. [Google Scholar] [CrossRef]
- Charles, C.Z.; Roscigno, V.J.; Torres, K.C. Racial inequality and college attendance: The mediating role of parental investments. Soc. Sci. Res. 2007, 36, 329–352. [Google Scholar] [CrossRef]
- Isaacs, J.B.; Sawhill, I.V.; Haskins, R. Getting Ahead or Losing Ground: Economic Mobility in America; Brookings Institution: Washington, DC, USA, 2008. [Google Scholar]
- Naylor-Wardle, J.; Rowland, B.; Kunadian, V. Socioeconomic status and cardiovascular health in the COVID-19 pandemic. Heart 2021, 107, 358–365. [Google Scholar] [CrossRef]
- Ludbrook, A. Fiscal measures to promote healthier choices: An economic perspective on price-based interventions. Public Health 2019, 169, 180–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeller, P.; Joumard, I.; Koske, I. Reducing income inequality while boosting economic growth: Can it be done? Evidence from OECD countries. Singap. Econ. Rev. 2014, 59, 1450001. [Google Scholar] [CrossRef] [Green Version]
- Prasad, P.; Branch, M.; Asemota, D.; Elsayed, R.; Addison, D.; Brown, S. Cardio-Oncology Preventive Care: Racial and Ethnic Disparities. Curr. Cardiovasc. Risk Rep. 2020, 14, 18. [Google Scholar] [CrossRef]
- Lopez, L.; Hart, L.H.; Katz, M.H. Racial and ethnic health disparities related to COVID-19. JAMA 2021, 325, 719–720. [Google Scholar] [CrossRef] [PubMed]
- Sadler, D.; DeCara, J.M.; Herrmann, J.; Arnold, A.; Ghosh, A.K.; Abdel-Qadir, H.; Yang, E.H.; SZmit, S.; Akhter, N.; Leja, M.; et al. The COVID-19 Pandemic Impact on Cardio-Oncology: Results From the COVID-19 International Collaborative Network Survey. Cardio Oncol. 2020, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease 2019 (COVID-19). US Food and Drug Administration. 2022. Available online: https://www.fda.gov/emergency-preparedness-and-response/counterterrorism-and-emerging-threats/coronavirus-disease-2019-covid-19 (accessed on 15 February 2022).



{kind=link}
{kind=link}
| Authors (Year) | SE Factor | Findings |
|---|---|---|
| [37] | Income | Lockdown data from Italy showed that lockdown was more effective in municipalities with higher fiscal capacity. |
| [38] | Income | Data from the 50 countries leading in COVID-19 cases showed reduced income dispersion correlated with reduced mortality. |
| [39] | Income and Population density | Mobility data from the United States showed that social distancing is less effective in counties with higher poverty levels and higher amounts of essential workers. |
| [40] | Population density | A retrospective cohort study in Michigan found that increased population density was associated with testing positive for COVID-19. |
| [41] | Population density | A zip code-level study from 5 major metropolitan areas showed that persons per household increased the proportion of positive COVID-19 cases by 1.83%. |
| [42] | Education | As of May 2020, in the US, the SE determinants of health with the strongest association to COVID-19 incidence and mortality per 100,000 persons was the percentage of adults without a high school degree. |
| [43] | Population density and Income | Data from New York at the start of the pandemic showed: -An increase of 10,000 people per km2 was associated with a 2.4% increase in COVID-19 positivity rate. -A USD 10,000 median household income decrease was associated with a 1.6% increase in the COVID-19 positivity rate. |
| [44] | Income and Education | Surveys across the USA, Canada, and the UK showed that: -Individuals with lower income and lower educational attainment were more likely to have misperceptions about COVID-19. -A lower-income level was correlated with a greater perception of personal risk from COVID-19 across all three countries. |
| [45] | Population density and Education | A retrospective analysis at Massachusetts General Hospital found that increased population density and lower education were associated with a higher likelihood of infection. |
| [46] | Income | A cross-sectional analysis of the first 200 days of the COVID-19 pandemic in the US found that a 1% increase in a county’s income inequality was associated with an adjusted relative risk of 1.020 for COVID-19 incidence and 1.030 for COVID-19 mortality. |
| [47] | Income | Lockdown data from Columbia showed areas with higher poverty had a lesser decline in mobility than areas with higher SE status. |
| [48] | Income, Employment, Education, and Race | A cross-sectional study in the US found various social factors, including SE status comprising unemployment rate, per capita income, and racial/ ethnic minority status, was associated with COVID-19 incidence and mortality. |
| [49] | Income, Education, Population density, Race and Minorities | 19 out of 28 studies in a systematic review showed that: -Individuals with low SE status, including poverty, lower education, and household overcrowding, were at higher risk of infection, death, and confirmed diagnosis of COVID-19. -Racial and ethnic minorities are at increased risk of infection, having positive test results, and hospital admission from COVID-19. |
| [50] | Income, Education, and Population density | A retrospective analysis mapping COVID-19 incidence and mortality in Chile found: -Areas with lower income, education, and health factors were less compliant with stay-at-home orders. -An overall strong association between low SE status and COVID-19 mortality. -Lower education and household crowding were associated with an increased likelihood of hospitalization. |
| [51] | Education and Population density | Lower level of education and number of people living in a household were positively associated with an increased likelihood of hospitalization due to COVID-19 infection. |
| Authors (Year) | SE Factor | Findings |
|---|---|---|
| [3] | Population density | Population morphology characteristics, especially an increase in the number of persons per housing unit, are positively associated with mortality due to CVD. |
| [4] | Education | SE status measures were closely associated with CVD risk factors (cigarette smoking, systolic and diastolic blood pressure, and total and high-density lipoprotein cholesterol) and with lower levels of education. |
| [5] | Occupation and Education | -In all countries, mortality from CVD is higher among persons with a lower occupational class or lower educational level. -Inequalities in CVD mortality are associated with disparities in certain risk factors, especially cigarette smoking and excessive alcohol consumption. |
| [6] | Neighborhood, Income, Education, Race, and Occupation | -Residents of disadvantaged neighborhoods had a higher risk of coronary heart disease than residents of advantaged neighborhoods, even after controlling for personal income, education, and occupation. -Hazard ratios for coronary heart disease among low-income persons living in the most disadvantaged neighborhoods, compared with high-income persons in the most advantaged neighborhoods, were 3.1 among Whites and 2.5 among Blacks, which remained unchanged after adjusting for established risk factors for coronary heart disease. |
| [7] | Race, Education, and Income | In Multi-Ethnic Study of Atherosclerosis with 6716 participants: -The US to foreign-born prevalence ratio for the carotid plaque was 1.20 in Whites, 1.91 in Chinese, 1.62 in Blacks, and 1.23 in Hispanics. -Greater carotid plaque prevalence was present in Whites, Blacks, and Hispanics with a greater number of generations with US residence. -Greater carotid plaque burden is present in Whites with less education and among Blacks with lower incomes. |
| [8] | Education | A higher risk of acute myocardial infarction was present in individuals with a lower educational level. |
| [9] | Income | Even after adjusting for smoking and alcohol consumption, an increased risk of nonfatal myocardial infarction and sudden cardiac death was found in the low-income cohorts. |
| [10] | Income | In a study of >15,000 patients in the Netherlands admitted for acute myocardial infarction or coronary heart disease, individuals in the lower quintiles of income had significantly higher 28-day and 1-year CVD-related mortality rates. |
| [11] | Race | Lack of access to quality care along with Black race compared to White race was associated with increased heart failure and post-acute myocardial ischemia hospital readmission rates in the United States. |
| [12] | Race | The trend of CVD between 1997 and 2008 in 4 communities in the US: -Average annual rate of incident myocardial infarction decreased non-uniformly across races (4.3% among White men vs. 1.5% among Black men) -Age-adjusted 28-day case fatality after hospitalized acute myocardial infarction declined non-uniformly across races (3.0%/y among White women vs. 2.6%/y among Black women) |
| [13] | Race | -African Americans had a higher prevalence of evaluated cardiovascular risk factors than Caucasians after controlling for obesity, tobacco use, and physical fitness. -Caucasians had a greater likelihood of no risk factors, while African Americans were more likely to have all three risk factors. |
| [14] | Income | -5.65% of the low-income patients received excellent quality of cardiac care compared to 11.48% of patients not in the low-income group. -The mortality rate of low-income patients (12.10%) was higher than patients not in the low-income group (5.25%). -Patterns of quality of care partially mediated the relationship between patient income level and coronary artery bypass grafting mortality. |
| [15] | Employment | Unemployment is associated with a high cardiovascular event rate and increased all-cause mortality in middle-aged socially privileged individuals. |
| [16] | Income and Education | Low income remains associated with a higher risk of coronary heart disease for younger individuals, regardless of education. |
| [17] | Education and Income | In a study with 15,350 adults, higher education and income level were associated with a higher proportion of meeting five or more ideal cardiovascular health metrics. |
| [18] | Race and Neighborhood | Among African American women, each standard deviation increase in neighborhood disadvantage was associated with a 25% increased risk of CVD after covariate adjustment (hazard ratio = 1.25). |
| [19] | Income | CVD prevalence (stroke, ischemic heart disease, and other CVD that led to hospitalization) was lower in high- and middle-income areas than in low-income areas (7.46%, 7.42%, and 8.36%, respectively). |
| [20] | Race | The higher prevalence of traditional CVD risk factors (e.g., hypertension, diabetes mellitus, obesity, and atherosclerosis) was associated with the relatively earlier onset of CVDs among African Americans. |
| [21] | Race | -Caucasians had higher odds of care by a cardiologist than African Americans (adjusted odds ratio: 1.42). |
| [22] | Income and Neighborhood | -An average increase in cardiovascular health score of 0.31 points is associated with each 1-category increase in individual income. -Each 1-category increase in neighborhood SE score was associated with a 0.19-point increase in cardiovascular health score. |
| [23] | Income | Low income was associated with high cardiovascular mortality (HR 1.31) and cardiovascular events (HR 1.07) in patients with hypertension. |
| [24] | Substance use disorder | People with substance use disorder are more likely to have prevalent CVD and develop incident CVD than people without substance abuse. |
| [25] | Income, Occupation, Education, and Health insurance | In two nationwide cohort studies in US and UK adults, low SE status had higher risks of mortality and CVD, and overall lifestyle only explained 3.0% to 12.3% of the excess risks. |
| [26] | Income and Education | Higher SE status was associated with the better achievement of most risk factor targets, participation in programs aimed at lifestyle change, and evidence-based drug therapies after myocardial ischemia. |
| Authors (Year) | SE Factor | Findings |
|---|---|---|
| [66] | Race | -Compared with Whites, Blacks had an overall excess risk of death (HR 1.16). -After correction for deaths due to other causes, the cancer-specific hazard ratio was 1.07. -Of the 14 cancers studied, Blacks were at a significantly higher risk of cancer-specific death related to cancer of the breast, uterus, or bladder. |
| [67] | Income | Affluent women were less likely to present with invasive ductal tumors (70.8% vs. 85.9%), tumors of higher grade (36% vs. 44.7%), and estrogen receptor-negative tumors (22.4% vs. 33.3%). |
| [68] | Employment, car, and home ownership and Population density | -Townsend index incorporating four variables, including unemployment, non-car ownership, non-home ownership, and household overcrowding, was used to calculate deprivation level. -Breast cancer is rising in women of lower SE status in Scotland, and the deprived–affluent gap remains. -Trends in late age at first pregnancy, the prevalence of obesity, and screening uptake do not fully explain the observed trends. |
| [69] | Education | A higher risk of malignant disease, particularly smoking-related cancers, was found among the lowest educational attainment. Only some of the educational attainment could be related to smoking. |
| [70] | Income | Index of Multiple Deprivation 2004 is a tool composed of different variables of SE status. In this study, the postcode of residence-related income domain alone of the Index of Multiple Deprivation 2004 was used to calculate the level of deprivation. The cancer incidence was highest for the most deprived patients, especially for lung and cervical cancer. |
| [71] | Education, Employment, and Income | Overall, increased risk of lung cancer incidence in people with low education (61%), low occupational SE status (48%), and low income (37%). |
| [72] | Education, Employment, Poverty, and Income | -Low SE status groups exhibited a higher incidence of colorectal cancer than high SE status groups in the US and Canada. -Patients with a low SE status received (neo)adjuvant therapy less often, had worse survival rates, and generally exhibited the highest mortality rates up to 1.6 risk ratio for colon cancer and up to 3.1 risk ratio for rectal cancer. |
| [73] | Factor-based deprivation index | -Factor-based deprivation index that consisted of 11 census-based social indicators, which may be broadly represented by educational opportunities, labor force skills, economic and housing conditions in a given area, was used to measure deprivation. -More disadvantaged groups and rural areas residents had higher cancer mortality compared to those residing in more affluent and urban areas, especially for lung, colorectal, prostate, and cervical cancers. -SE inequalities were present in both Whites and Blacks. -Blacks experienced higher mortality from each cancer than Whites within each deprivation group. |
| [74] | Urban-rural area and Income | -The incidence of lung cancer was higher in urban deprived areas than in affluent rural areas in England. -Adjusting for SE deprivation, little difference was seen between the incidence and survival of lung cancer in urban and rural areas. |
| [75] | Income | Graded inverse associations between income and mortality were found for most, but not all, specific causes of death. The major contributors to income differentials in total mortality included lung and liver cancer in both men and women |
| [76] | Education | -Large educational inequalities were observed in cancer mortality, mainly for cancer of the cervix, stomach, and lung. -Mortality from cervical cancer declined more rapidly in groups with lower educational attainment. |
| [77] | Race, Neighborhood, and Ethnicity | Mortality was higher among Blacks than Whites. Cancer patient survival was significantly lower in more deprived neighborhoods and among most ethnic minority groups. |
| [78] | Income | Lung cancer was the most significant driver of cancer inequality trends, followed by colorectal cancer in men and breast cancer in women. |
| [79] | Occupation type | SE status remained a significant risk factor for lung cancer after adjustment for smoking behavior. |
| [80] | Income | The absolute difference between the cancer rates in the highest- and lowest-incidence region, per 100,000 people, has widened from 39 to 86 for females and from 94 to 116 for males. |
| [81] | Area Deprivation Index | -In this study, neighborhood SE status was measured using the area deprivation index, a validated, comprehensive tool to measure SE status. Individual SES was evaluated by Medicare–Medicaid dual eligibility, a reliable indicator for patient-level low income. -Deprivation in the neighborhood was associated with worse survival among patients with non-metastatic cancers, even after accounting for individual SE factors. |
| [82] | Area Deprivation Index | -Zip codes linked Area Deprivation Index composed of 17 diverse indicators of SE status was used to evaluate the level of deprivation in the study. -Compared to the most affluent participants, participants from the highest SE deprivation area had worse overall progression-free and cancer-specific survival. |
| [83] | Income and Neighborhood | SE status, level of literacy, and area of residence were the main contributors to the observed inequality in screening mammography among Iranian women of Kurdish descent. |
| Authors (Year) | SE Factor | Findings |
|---|---|---|
| [84] | Race | Higher incidence of doxorubicin-related cardiotoxicity for breast cancer patients among Blacks compared to non-Black patients (7/100 compared to 10/399). |
| [85] | Income and Education | In a large cohort, the relative risk of five compared with zero lifestyle risk factors prevalent in low SE status areas was: -4.31 for all-cause mortality. -3.36 (95% CI 2.45 to 4.34) for cancer mortality. -8.17 (95% CI 4.96 to 13.47) for cardiovascular mortality. |
| [86] | Race | -Hypertension was an independent predictor of the survival disparity between Black and White survivors of invasive breast cancer. -In a follow-up of 9 years, African Americans had a higher overall crude mortality of 39.7% than Whites of 33.3%. |
| [87] | Race | A higher incidence of cardiac events was noted among Black patients with diabetes, hypertension, or CVD who were treated with trastuzumab compared to White patients with the same conditions: 3/15 (20%) vs. 4/48 (8.3%), respectively. |
| [88] | Race | African American patients with breast cancer had a higher risk of developing decreased left ventricle ejection fraction while on trastuzumab therapy compared to other races. |
| [89] | Race | There is a higher risk of cardiovascular death in Black breast cancer survivors than White breast cancer survivors with ductal carcinoma in situ at ages 40–49, 50–59, and 60–69 with a hazard ratio of 14.99, 6.43, and 2.26, respectively. There was no significant difference in hazard of cardiovascular death between Black and White patients 70 years and older. |
| [90] | Education | -Analyzing >2 million person-years of follow-up in 24 studies, 11,065 deaths (3655 from CVD and 4313 from cancer) and 1809 CVD nonfatal events were recorded. -Hazard ratios for primary relative to tertiary education were 1.81 for all-cause mortality, 2.47 for CVD mortality, 1.66 for cancer mortality, and 2.09 for all CVD. |
| [91] | Ethnicity | The mortality rates for cancers varied by national origin. Filipino, Asian Indian and Pakistani, and Pacific Islander groups had a risk of cardiovascular mortality similar to White women. Hawaiian women had a higher risk of cardiovascular mortality (hazard ratio, 1.43; 95% confidence interval, 1.17–1.75) compared with White women. US-born Asian and Pacific Islander breast cancer survivors had a higher risk of cardiovascular mortality (hazard ratio 1.29; 95% confidence interval, 1.08–1.54) compared with immigrant survivors of breast cancer. |
| [92] | Geography, Income, and Health care access | -The number of Childhood Cancer Survivor Study centers within the geographic area was associated with greater odds of receiving risk-based survivor-focused medical care. -Higher-income areas had higher echocardiogram screening among survivors at risk of cardiomyopathy (for every USD 10,000 increase in average income, there was a 12% increase in odds of echocardiogram screening). -A significant positive association was identified between the number of physicians and surgeons in the county of residence and the likelihood of an echocardiogram being recommended for residents. |
| [93] | Race | -The 1-year cardiotoxicity incidence was 12% overall, 24% in Black women, and 7% in White women. -Black patients had a higher likelihood of not completing therapy than White patients. |
| [94] | Race | Black survivors of breast cancer had an increased 20-year cumulative mortality rate from CVD, with a more pronounced effect in younger patients. |
| [95] | Race | Treatment with hormone therapy or chemotherapy was suggested to contribute to the CVD mortality disparities between Black and White survivors of breast cancer, although the results in this study did not reach statistical significance. |
| [96] | Education, Employment, and Population density | In 109,246 Finnish adults, a cascade of inter-related health issues with a hazard ratio>5 was identified: ischemic heart disease, cerebral infarction, lung cancer, and other diseases in lower SE status patients. |
| [97] | Income | Referral patterns of patients with hypertension and breast cancer receiving cardio-toxic chemotherapy agents to cardio-oncology or cardiology clinics were higher for residents of higher-income quartile ZIP codes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batra, A.; Swaby, J.; Raval, P.; Zhu, H.; Weintraub, N.L.; Terris, M.; Karim, N.A.; Keruakous, A.; Gutterman, D.; Beyer, K.; et al. Effect of Community and Socio-Economic Factors on Cardiovascular, Cancer and Cardio-Oncology Patients with COVID-19. COVID 2022, 2, 350-368. https://doi.org/10.3390/covid2030024
Batra A, Swaby J, Raval P, Zhu H, Weintraub NL, Terris M, Karim NA, Keruakous A, Gutterman D, Beyer K, et al. Effect of Community and Socio-Economic Factors on Cardiovascular, Cancer and Cardio-Oncology Patients with COVID-19. COVID. 2022; 2(3):350-368. https://doi.org/10.3390/covid2030024
Chicago/Turabian StyleBatra, Akshee, Justin Swaby, Priyanka Raval, Haidong Zhu, Neal Lee Weintraub, Martha Terris, Nagla Abdel Karim, Amany Keruakous, David Gutterman, Kirsten Beyer, and et al. 2022. "Effect of Community and Socio-Economic Factors on Cardiovascular, Cancer and Cardio-Oncology Patients with COVID-19" COVID 2, no. 3: 350-368. https://doi.org/10.3390/covid2030024