
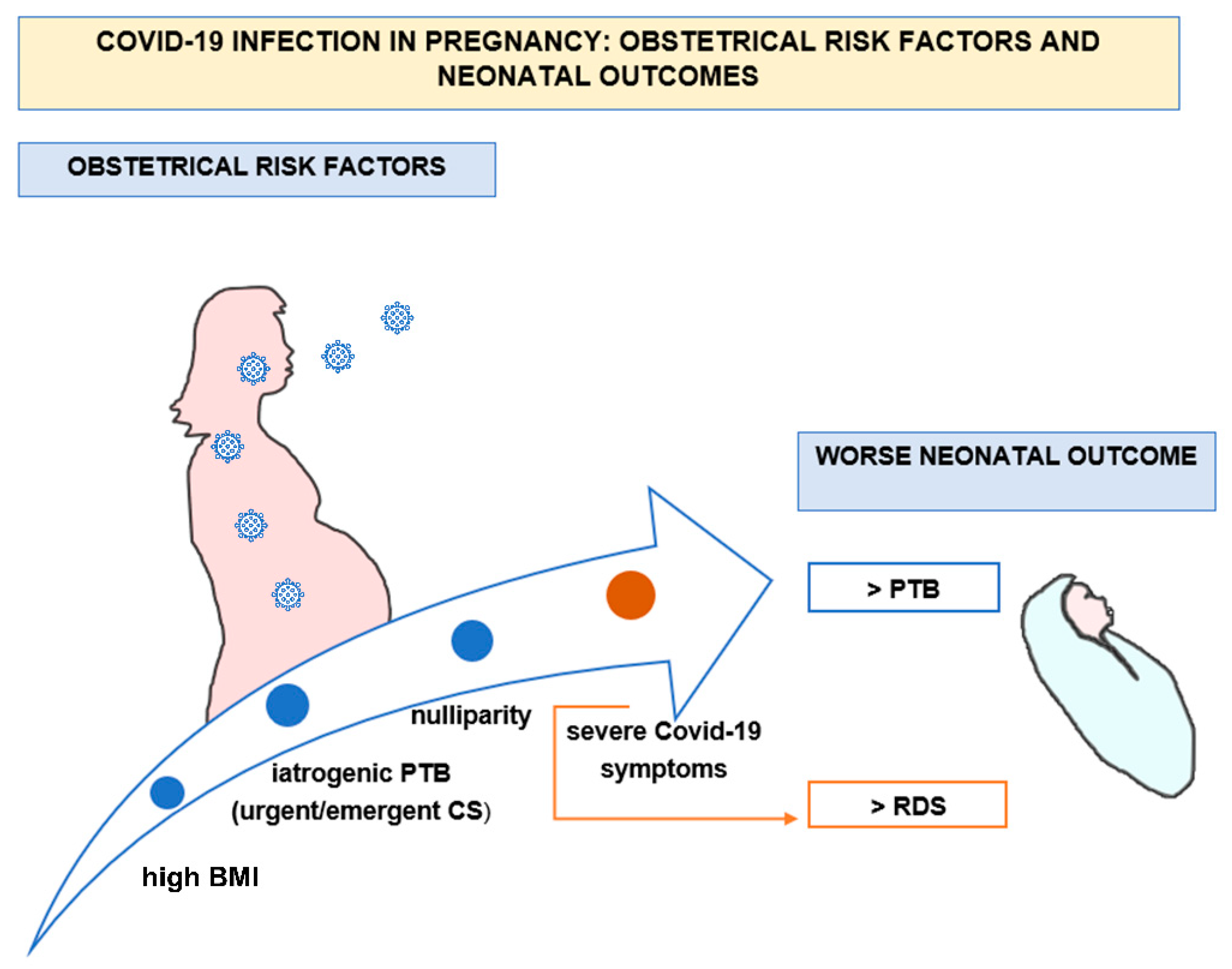
COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes—A Monocentric, Single-Cohort Study

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Results from Descriptive Statistics of the Population under Study (Mothers and Neonates)
- General characteristics of the population under study and main neonatal outcomes
- 2.
- COVID-19 symptoms among the population under study
- 3.
- Comorbidities of the population under study
- 4.
- Rates of different modes of delivery, preterm birth, and neonatal respiratory distress syndrome
3.2. Results from Correlations between Maternal or Obstetric Risk Factors and COVID-19 Disease Severity, Gestational Age at Birth, and Neonatal Respiratory Distress Syndrome
- The correlation between maternal/obstetric risk factors and COVID-19 disease severity
- 2.
- Maternal characteristics and neonatal birth age (full-term vs. preterm birth)
- 3.
- The correlation between the presence of neonatal respiratory distress syndrome (RDS) and the severity of maternal COVID-19 symptoms
- 4.
- Bad neonatal outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Volpe, N.; Schera, G.B.L.; Frusca, T. COVID-19 in pregnancy: Italian experience. Perinat. J. 2020, 28, 149–153. [Google Scholar] [CrossRef]
- Edlow, A.G.; Li, J.Z.; Collier, A.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2030455. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, E.H.; Moreno, W.; Zofkie, A.C.; MacDonald, L.; McIntire, D.D.; Collins, R.R.J.; Spong, C.Y. Pregnancy Outcomes Among Women with and without Severe Acute Respiratory Syndrome Coronavirus 2 Infection. JAMA Netw. Open 2020, 3, e2029256. [Google Scholar] [CrossRef] [PubMed]
- Di Guardo, F.; Di Grazia, F.M.; Di Gregorio, L.M.; Zambrotta, E.; Carrara, G.; Gulino, F.A.; Tuscano, A.; Palumbo, M. Poor maternal-neonatal outcomes in pregnant patients with confirmed SARS-Cov-2 infection: Analysis of 145 cases. Arch. Gynecol. Obstet. 2021, 303, 1483–1488. [Google Scholar] [CrossRef]
- Capozza, M.; Salvatore, S.; Baldassarre, M.E.; Inting, S.; Panza, R.; Fanelli, M.; Perniciaro, S.; Morlacchi, L.; Vimercati, A.; Agosti, M. Perinatal Transmission and Outcome of Neonates Born to SARS-CoV-2-Positive Mothers: The Experience of 2 Highly Endemic Italian Regions. Neonatology 2021, 118, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Angelidou, A.; Sullivan, K.; Melvin, P.R.; Shui, J.E.; Goldfarb, I.T.; Bartolome, R.; Chaudhary, N.; Vaidya, R.; Culic, I.; Singh, R.; et al. Association of Maternal Perinatal SARS-CoV-2 Infection with Neonatal Outcomes During the COVID-19 Pandemic in Massachusetts. JAMA Netw. Open 2021, 4, e217523. [Google Scholar] [CrossRef]
- Donati, S.; Corsi, E.; Maraschini, A.; Salvatore, M.A.; The ItOSS-COVID-19 Working Group. SARS-CoV-2 infection among hospitalized pregnant women and impact of different viral strains on COVID-19 severity in Italy: A national prospective population-based cohort study. BJOG 2022, 129, 221–231. [Google Scholar] [CrossRef]
- Kiserud, T.A.-O.; Piaggio, G.A.-O.; Carroli, G.; Widmer, M.; Carvalho, J.A.-O.; Neerup Jensen, L.; Giordano, D.; Cecatti, J.A.-O.; Abdel Aleem, H.; Talegawkar, S.A.; et al. The World Health Organization Fetal Growth Charts: A Multinational Longitudinal Study of Ultrasound Biometric Measurements and Estimated Fetal Weight. PLoS Med. 2017, 14, e1002220. [Google Scholar]
- Boldrini, R.D.C.M.; Baisli, F.; Gaia, C.; Giannetti, A.; Rossana, M.; Romanelli, M.; Rizzuto, E. Statistic and Health Information System; Ministry of Health: Rome, Italy, 2019.
- Dyer, J. Neonatal respiratory distress syndrome: Tackling a worldwide problem. Pharm. Ther. 2019, 44, 12. [Google Scholar]
- Simpson, A.N.; Snelgrove, J.W.; Sutradhar, R.; Everett, K.; Liu, N.; Baxter, N.N. Perinatal Outcomes During the COVID-19 Pandemic in Ontario, Canada. JAMA Netw. Open 2021, 4, e2110104. [Google Scholar] [CrossRef]
- Brandt, J.S.; Hill, J.; Reddy, A.; Schuster, M.; Patrick, H.S.; Rosen, T.; Sauer, M.V.; Boyle, C.; Ananth, C.V. Epidemiology of coronavirus disease 2019 in pregnancy: Risk factors and associations with adverse maternal and neonatal outcomes. Am. J. Obstet. Gynecol. 2021, 224, 389.e1–389.e9. [Google Scholar] [CrossRef] [PubMed]
- Figueiro-Filho, E.A.; Hobson, S.R.; Farine, D.; Yudin, M.H. Highly expressed ACE-2 receptors during pregnancy: A protective factor for SARS-CoV-2 infection? Med. Hypotheses 2021, 153, 110641. [Google Scholar] [CrossRef] [PubMed]
- Richtmann, R.; Torloni, M.R.; Oyamada Otani, A.R.; Levi, J.E.; Crema Tobara, M.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvão, L.; Martins Silva, P.; Macoto Kondo, M. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Womens Health 2020, 27, e00243. [Google Scholar] [CrossRef] [PubMed]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-Trimester Miscarriage in a Pregnant Woman with SARS-CoV-2 Infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef]
- Pulinx, B.; Kieffer, D.; Michiels, I.; Petermans, S.; Strybol, D.; Delvaux, S.; Baldewijns, M.; Raymaekers, M.; Cartuyvels, R.; Maurissen, W. Vertical transmission of SARS-CoV-2 infection and preterm birth. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2441–2445. [Google Scholar] [CrossRef]
- Boldrini, R. Directorate-General of Digitalization, of Health Informative System and of Statistics; Birth Registry; Italian Ministry of Health: Rome, Italy, 2019.
- Bellos, I.; Pandita, A.; Panza, R. Maternal and perinatal outcomes in pregnant women infected by SARS-CoV-2: A meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 194–204. [Google Scholar] [CrossRef]
- Cosma, S.; Carosso, A.R.; Cusato, J.; Borella, F.; Carosso, M.; Gervasoni, F.; Stura, I.; Preti, M.; Ghisetti, V.; Di Perri, G.; et al. Preterm birth is not associated with asymptomatic/mild SARS-CoV-2 infection per se: Pre-pregnancy state is what matters. PLoS ONE 2021, 16, e0254875. [Google Scholar] [CrossRef]
- Resta, L.; Vimercati, A.; Cazzato, G.; Mazzia, G.; Cicinelli, E.; Colagrande, A.; Fanelli, M.; Scarcella, S.V.; Ceci, O.; Rossi, R. SARS-CoV-2 and Placenta: New Insights and Perspectives. Viruses 2021, 13, 723. [Google Scholar] [CrossRef]
- Sukhikh, G.; Petrova, U.; Prikhodko, A.; Starodubtseva, N.; Chingin, K.; Chen, H.; Bugrova, A.; Kononikhin, A.; Bourmenskaya, O.; Brzhozovskiy, A.; et al. Vertical Transmission of SARS-CoV-2 in Second Trimester Associated with Severe Neonatal Pathology. Viruses 2021, 13, 447. [Google Scholar] [CrossRef]
- Nikiforuk, A.M.; Kuchinski, K.S.; Twa, D.D.W.; Lukac, C.D.; Sbihi, H.; Basham, C.A.; Steidl, C.; Prystajecky, N.A.; Jassem, A.N.; Krajden, M.; et al. The contrasting role of nasopharyngeal angiotensin converting enzyme 2 (ACE2) transcription in SARS-CoV-2 infection: A cross-sectional study of people tested for COVID-19 in British Columbia, Canada. EBioMedicine 2021, 66, 103316. [Google Scholar] [CrossRef] [PubMed]
- Bloise, E.; Zhang, J.; Nakpu, J.; Hamada, H.; Dunk, C.E.; Li, S.; Imperio, G.E.; Nadeem, L.; Kibschull, M.; Lye, P.; et al. Expression of severe acute respiratory syndrome coronavirus 2 cell entry genes, angiotensin-converting enzyme 2 and transmembrane protease serine 2, in the placenta across gestation and at the maternal-fetal interface in pregnancies complicated by preterm birth or preeclampsia. Am. J. Obstet. Gynecol. 2021, 224, 298.e1–298.e8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| General Characteristics of COVID-19 + Pregnant Patients | N | % | |
|---|---|---|---|
| 122 | 100% | ||
| Age | <30 | 38 | 31.15% |
| 30–40 | 76 | 62.30% | |
| >40 | 7 | 5.74% | |
| Missing | 1 | 0.82% | |
| BMI | <25 normal and underweight | 20 | 16.39% |
| 25–30 overweight | 69 | 56.56% | |
| >30 obese | 25 | 20.49% | |
| Missing | 8 | 6.56% | |
| Ethnicity | Caucasian | 116 | 95.08% |
| African | 5 | 4.10% | |
| Asian | 1 | 0.82% | |
| Comorbidities | Hypertension/pre-eclampsia | 2 | 1.64% |
| Diabetes mellitus/gestational diabetes | 12 | 9.84% | |
| Others | 29 | 23.77% | |
| Healthy | 79 | 64.75% | |
| Missing | 1 | 0.82% | |
| Parity | Nulliparous | 50 | 40.98% |
| Multiparous | 72 | 59.02% | |
| G.A. at COVID-19 diagnosis | 1st trimester | 0 | 0.00% |
| 2nd trimester | 2 | 1.64% | |
| 3rd trimester | 120 | 98.36% | |
| COVID-19 symptoms | 1 none | 74 | 60.66% |
| 2A few | 24 | 19.67% | |
| 2B mild | 18 | 14.75% | |
| 3 severe, requiring ICU for COVID-19 treatment | 5 | 4.10% | |
| Missing | 1 | 0.82% | |
| Pregnancy outcome and mode of delivery | PROM | 7 | 5.74% |
| pPROM | 0 | 0.00% | |
| SVB | 66 | 54.10% | |
| OVB | 3 | 2.46% | |
| elective CS | 29 | 23.77% | |
| urgent/emergent CS | 17 | 13.93% | |
| Main Neonatal Outcomes | Total Newborns = 125 | ||
|---|---|---|---|
| Gestational age at birth | Full-term 37–42 | 107 | 85.60% |
| Late PTB 32–37 | 10 | 8.00% | |
| Early PTB 28–32 | 2 | 1.60% | |
| Extreme PTB < 28 | 1 | 0.80% | |
| Missing | 5 | 4.00% | |
| Birth weight | AGA | 97 | 77.60% |
| SGA | 8 | 6.40% | |
| LGA | 9 | 7.20% | |
| Missing | 11 | 8.80% | |
| Malformations | 3 | 2.40% | |
| RDS | 7 | 5.60% | |
| NICU admission | 13 | 10.40% | |
| COVID-19 + Neonates | 0 | 0.00% | |
| Maternal/Obstetric Risk Factors | COVID-19 SYMPTOMS | p-Value | ||||
|---|---|---|---|---|---|---|
| NO or FEW | MILD or SEVERE | |||||
| N | % | N | % | |||
| AGE | <35 yrs | 73 | 75.26 | 12 | 52.17 | 0.02 |
| ≥35 yrs | 24 | 24.74 | 11 | 47.83 | ||
| BMI | <25 normal | 18 | 20.00 | 2 | 8.7 | 0.17 |
| 25–30 overweight | 55 | 61.11 | 13 | 56.52 | ||
| >30 obese | 17 | 18.89 | 8 | 34.78 | ||
| ETHNICITY | Caucasian | 93 | 94.90 | 22 | 95.65 | n.s. |
| African | 5 | 5.10 | 0 | 0.00 | ||
| Asian | 0 | 0.00 | 1 | 4.35 | ||
| COMORBIDITY | hypertension/pre-eclampsia | 1 | 1.02 | 1 | 4.35 | n.s. |
| diabetes/gestational diabetes | 8 | 8.16 | 4 | 17.39 | ||
| others | 22 | 22.45 | 7 | 30.43 | ||
| healthy | 67 | 68.4 | 11 | 47.83 | ||
| GA AT COVID-19 DIAGNOSIS | 1st trimester | 0 | 0.00 | 0 | 0.00 | n.s. |
| 2nd trimester | 2 | 2.04 | 0 | 0.00 | ||
| 3rd trimester | 90 | 97.96 | 23 | 100.00 | ||
| PARITY | nulliparous | 42 | 42.86 | 8 | 34.78 | n.s. |
| multiparous | 56 | 57.14 | 15 | 65.22 | ||
| DELIVERY MODE | OVB | 2 | 2.11 | 1 | 4.55 | 0.0001 |
| SVB | 59 | 62.11 | 9 | 40.91 | ||
| elective CS | 27 | 28.42 | 3 | 13.64 | ||
| emergent CS | 7 | 7.37 * | 9 | 40.91 * | ||
| Maternal/Obstetric Risk Factors | GESTATIONAL AGE AT BIRTH | p-Value | ||||
|---|---|---|---|---|---|---|
| FULL-TERM | PRETERM | |||||
| N | % | N | % | |||
| AGE | <35 yrs | 75 | 61.54 | 8 | 70.09 | n.s. |
| ≥35 yrs | 32 | 38.46 | 5 | 29.91 | ||
| BMI | <25 normal | 16 | 15.84 | 5 | 34.46 | 0.03 |
| 25–30 overweight | 66 | 65.35 * | 3 | 23.08 * | ||
| >30 obese | 19 | 18.81 @ | 5 | 38.46 @ | ||
| COMORBIDITY | hypertension/pre-eclampsia | 1 | 0.93 | 1 | 7.69 | 0.003 |
| diabetes/gestational diabetes | 8 | 7.48 | 3 | 23.08 | ||
| others | 22 | 2.56 # | 8 | 61.54 # | ||
| healthy | 76 | 71.03 | 1 | 7.69 | ||
| PARITY | Nulliparous | 41 | 38.32 § | 10 | 76.92 § | 0.01 |
| multiparous | 66 | 61.68 | 3 | 23.08 | ||
| GA AT COVID-19 DIAGNOSIS | 1st trimester | 0 | 0.00 | 0 | 0.00 | n.s. |
| 2nd trimester | 0 | 0.00 | 1 | 7.69 | ||
| 3rd trimester | 107 | 100.00 | 12 | 92.31 | ||
| DELIVERY MODE | OVB | 3 | 2.80 | 0 | 0.00 | 0.0005 |
| SVB | 64 | 59.81 | 5 | 38.46 | ||
| Elective CS | 29 | 27.1 a | 1 | 7.69 a | ||
| Emergent CS | 11 | 10.28 b | 7 | 53.85 b | ||
| COVID-19 SYMPTOMS | NON OR FEW | 89 | 83.96 | 7 | 53.85 | 0.01 |
| MILD OR SEVERE | 17 | 16.04 c | 6 | 46.15 c | ||
| Maternal COVID-19 Symptoms | NEONATAL RDS | p-Value | |||
|---|---|---|---|---|---|
| PRESENCE | ABSENCE | ||||
| N | % | N | % | ||
| none or few | 3 | 42.86% | 89 | 81.65% | 0.03 |
| mild or severe | 4 | 57.14% * | 20 | 18.35% * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vimercati, A.; De Nola, R.; Trerotoli, P.; Metta, M.E.; Cazzato, G.; Resta, L.; Malvasi, A.; Lepera, A.; Ricci, I.; Capozza, M.; et al. COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes—A Monocentric, Single-Cohort Study. Vaccines 2022, 10, 166. https://doi.org/10.3390/vaccines10020166
Vimercati A, De Nola R, Trerotoli P, Metta ME, Cazzato G, Resta L, Malvasi A, Lepera A, Ricci I, Capozza M, et al. COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes—A Monocentric, Single-Cohort Study. Vaccines. 2022; 10(2):166. https://doi.org/10.3390/vaccines10020166
Chicago/Turabian StyleVimercati, Antonella, Rosalba De Nola, Paolo Trerotoli, Maria Elvira Metta, Gerardo Cazzato, Leonardo Resta, Antonio Malvasi, Archiropita Lepera, Ilaria Ricci, Manuela Capozza, and et al. 2022. "COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes—A Monocentric, Single-Cohort Study" Vaccines 10, no. 2: 166. https://doi.org/10.3390/vaccines10020166