
Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
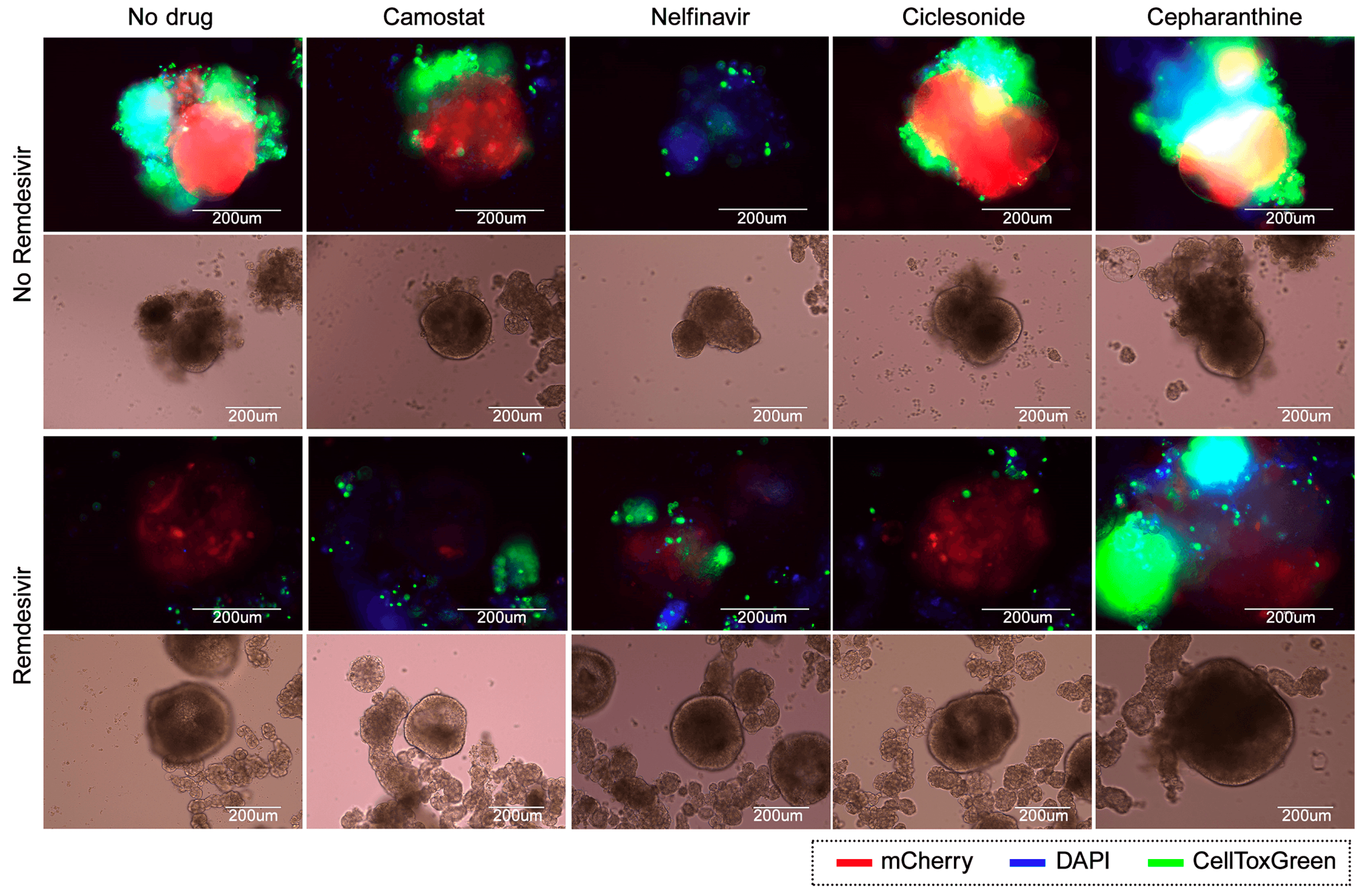
2.1. Viruses, Cell Lines, and Lung Organoids
2.2. Compound Libraries
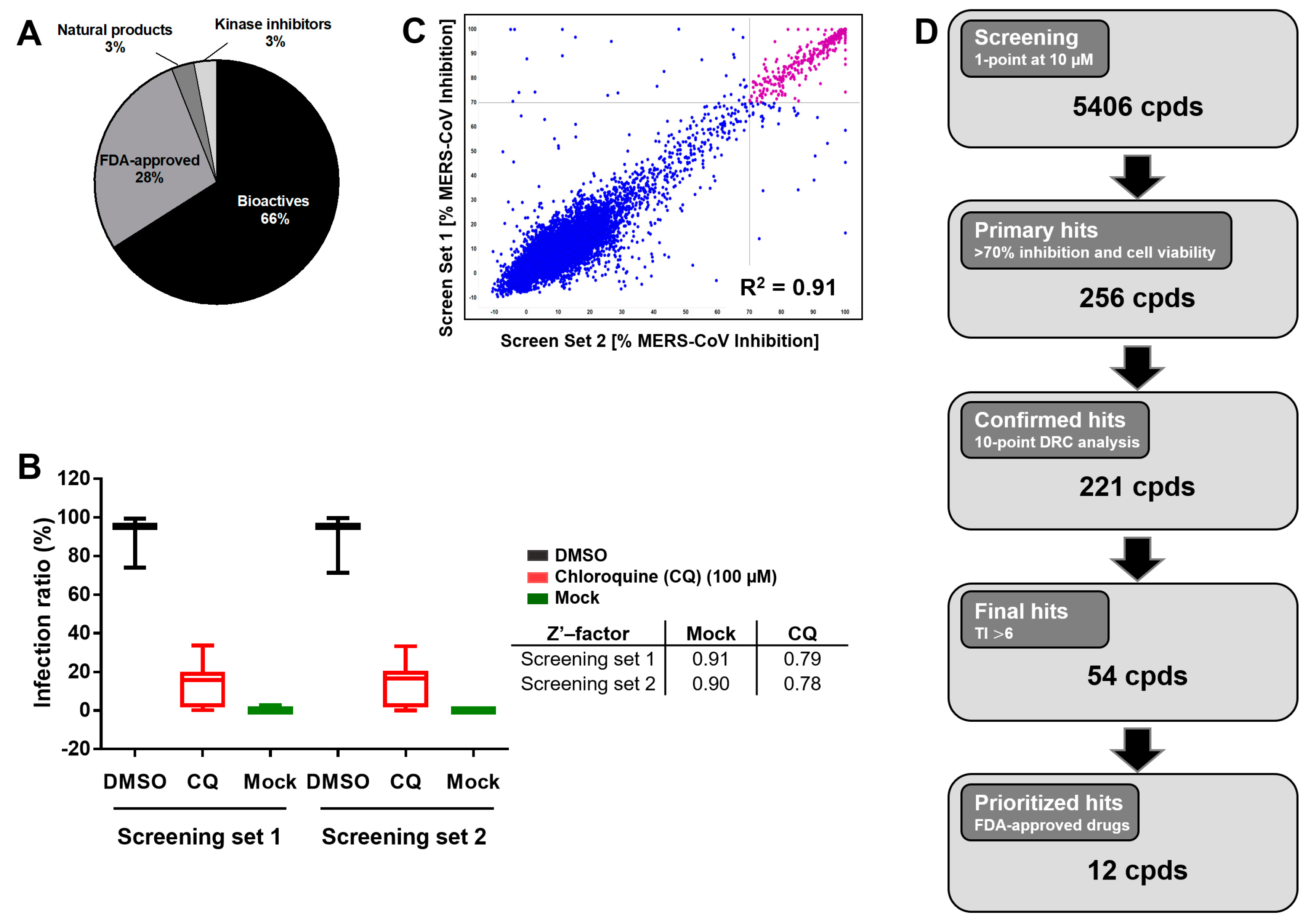
2.3. Image-Based Screening and Assay Validation
2.4. Dose–Response Curve Drug Analysis
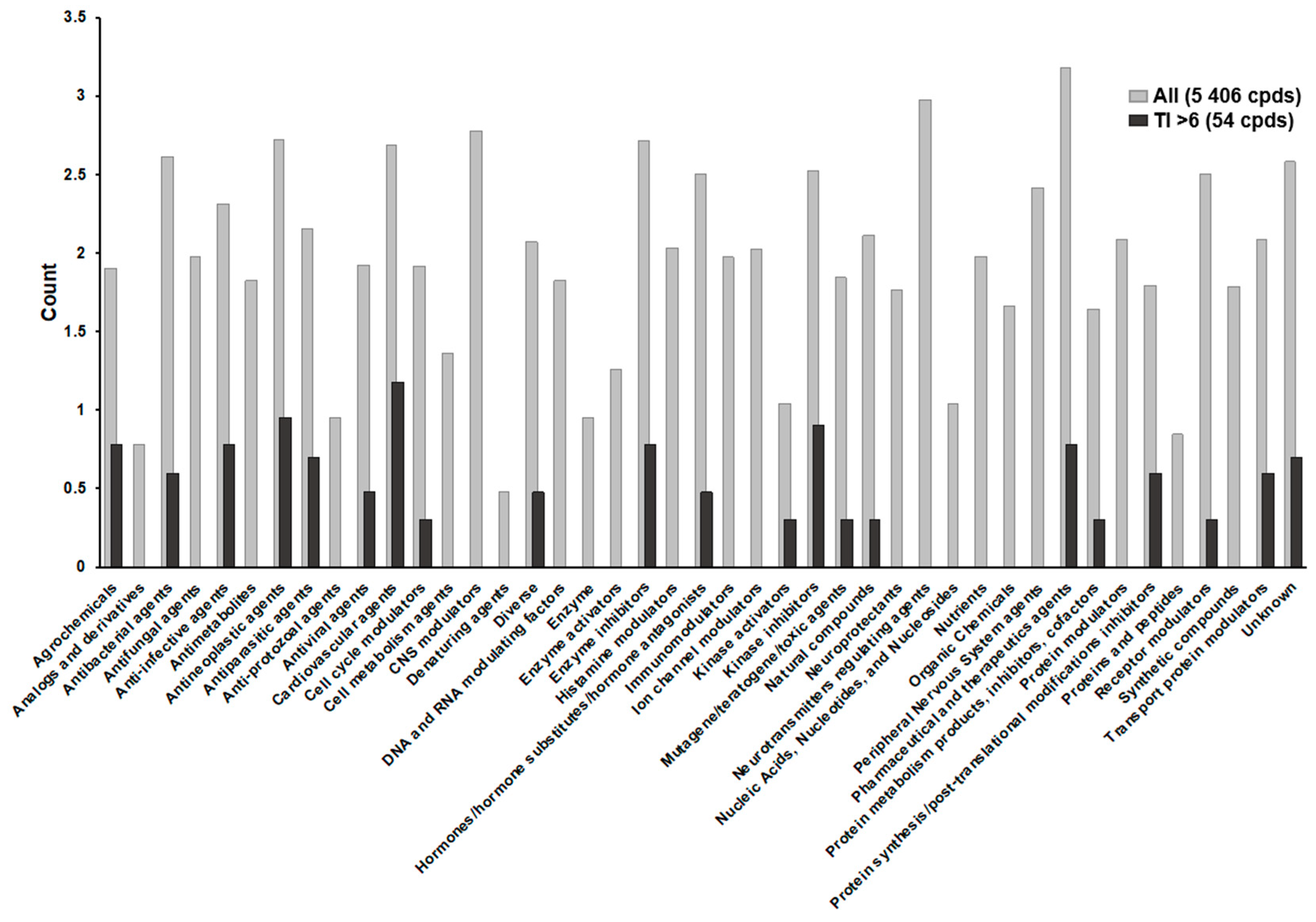
2.5. Pharmacological Action Clustering
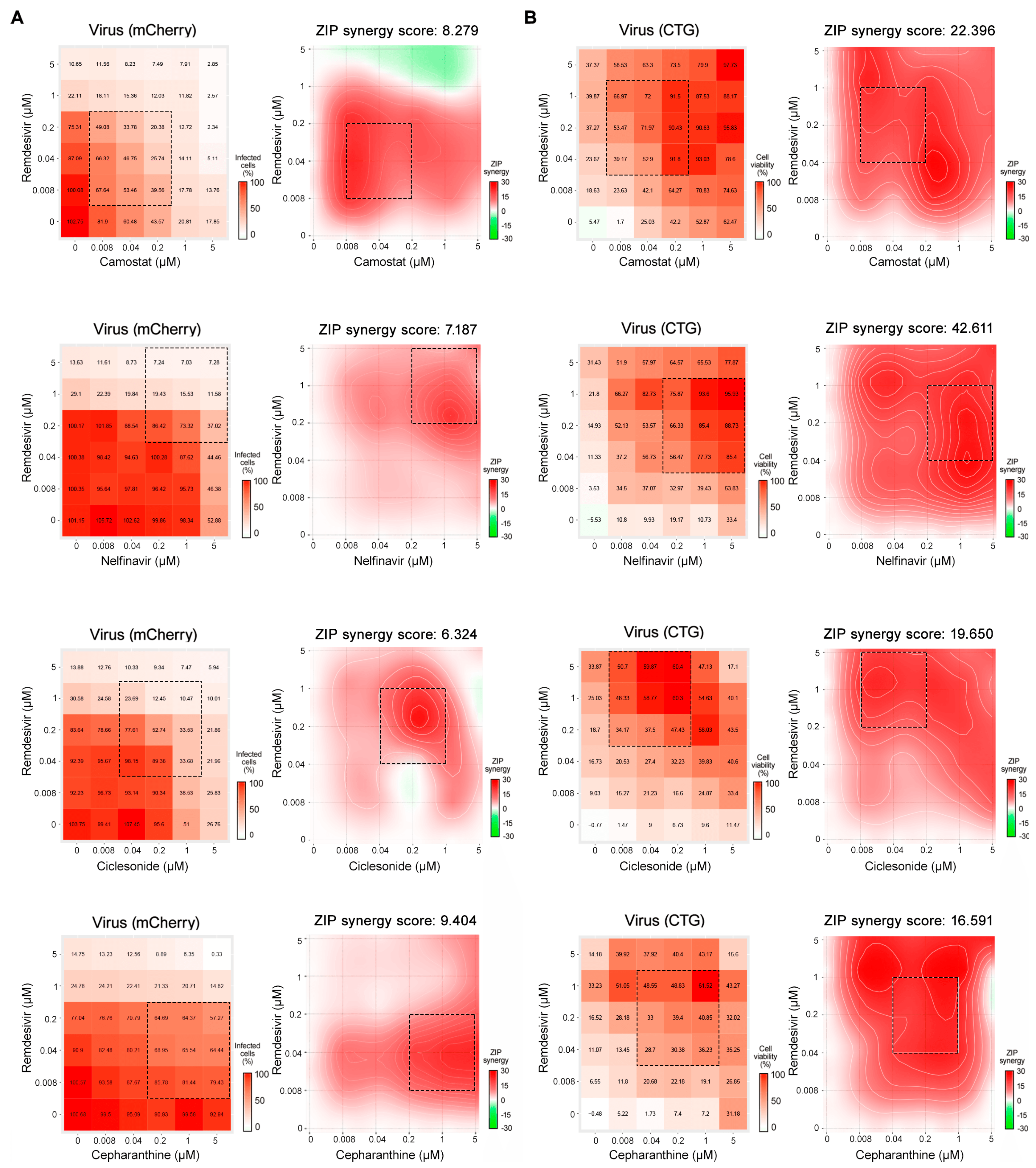
2.6. Drug Combination Studies
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Hamre, D.; Procknow, J.J. A new virus isolated from the human respiratory tract. Proc. Soc. Exp. Biol. Med. 1966, 121, 190–193. [Google Scholar] [CrossRef]
- McIntosh, K.; Dees, J.H.; Becker, W.B.; Kapikian, A.Z.; Chanock, R.M. Recovery in tracheal organ cultures of novel viruses from patients with respiratory disease. Proc. Natl. Acad. Sci. USA 1967, 57, 933–940. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Summary of Probably SARS Cases with Onset of Illness from 1 November 2002 to 31 July 2003. Available online: https://www.who.int/publications/m/item/summary-of-probable-sars-cases-with-onset-of-illness-from-1-november-2002-to-31-july-2003 (accessed on 16 November 2020).
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. MERS Situation Update. January 2019. Available online: http://www.emro.who.int/pandemic-epidemic-diseases/mers-cov/mers-situation-update-january-2019.html (accessed on 16 November 2020).
- Korea Centers for Disease Control and Prevention. Middle East Respiratory Syndrome Coronavirus Outbreak in the Republic of Korea. Osong Public Health Res. Perspect. 2015, 6, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.S.; Park, S.; Kim, Y.J.; Kang, H.J.; Kim, H.; Han, Y.W.; Lee, H.S.; Kim, D.W.; Kim, A.R.; Heo, D.R.; et al. Middle East Respiratory Syndrome in 3 Persons, South Korea, 2015. Emerg. Infect. Dis. 2015, 21, 2084–2087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.W.; Chu, C. Outbreak of Middle East Respiratory Syndrome in Korea? Osong Public Health Res. Perspect. 2015, 6, 219–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zumla, A.; Chan, J.F.; Azhar, E.I.; Hui, D.S.; Yuen, K.Y. Coronaviruses—Drug discovery and therapeutic options. Nat. Rev. Drug Discov. 2016, 15, 327–347. [Google Scholar] [CrossRef] [Green Version]
- Omrani, A.S.; Saad, M.M.; Baig, K.; Bahloul, A.; Abdul-Matin, M.; Alaidaroos, A.Y.; Almakhlafi, G.A.; Albarrak, M.M.; Memish, Z.A.; Albarrak, A.M. Ribavirin and interferon alfa-2a for severe Middle East respiratory syndrome coronavirus infection: A retrospective cohort study. Lancet Infect. Dis. 2014, 14, 1090–1095. [Google Scholar] [CrossRef] [Green Version]
- Shalhoub, S.; Farahat, F.; Al-Jiffri, A.; Simhairi, R.; Shamma, O.; Siddiqi, N.; Mushtaq, A. IFN-alpha2a or IFN-beta1a in combination with ribavirin to treat Middle East respiratory syndrome coronavirus pneumonia: A retrospective study. J. Antimicrob. Chemother. 2015, 70, 2129–2132. [Google Scholar] [CrossRef] [Green Version]
- Spanakis, N.; Tsiodras, S.; Haagmans, B.L.; Raj, V.S.; Pontikis, K.; Koutsoukou, A.; Koulouris, N.G.; Osterhaus, A.D.; Koopmans, M.P.; Tsakris, A. Virological and serological analysis of a recent Middle East respiratory syndrome coronavirus infection case on a triple combination antiviral regimen. Int. J. Antimicrob. Agents 2014, 44, 528–532. [Google Scholar] [CrossRef]
- Kim, Y.J.; Cho, Y.J.; Kim, D.W.; Yang, J.S.; Kim, H.; Park, S.; Han, Y.W.; Yun, M.R.; Lee, H.S.; Kim, A.R.; et al. Complete Genome Sequence of Middle East Respiratory Syndrome Coronavirus KOR/KNIH/002_05_2015, Isolated in South Korea. Genome Announc. 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Chang, S.Y.; Sung, M.; Park, J.H.; Bin Kim, H.; Lee, H.; Choi, J.P.; Choi, W.S.; Min, J.Y. Extensive Viable Middle East Respiratory Syndrome (MERS) Coronavirus Contamination in Air and Surrounding Environment in MERS Isolation Wards. Clin. Infect. Dis. 2016, 63, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Rihn, S.J.; Merits, A.; Bakshi, S.; Turnbull, M.L.; Wickenhagen, A.; Alexander, A.J.T.; Baillie, C.; Brennan, B.; Brown, F.; Brunker, K.; et al. A plasmid DNA-launched SARS-CoV-2 reverse genetics system and coronavirus toolkit for COVID-19 research. PLoS Biol. 2021, 19, e3001091. [Google Scholar] [CrossRef]
- Coleman, C.M.; Frieman, M.B. Growth and Quantification of MERS-CoV Infection. Curr. Protoc. Microbiol. 2015, 37, 15E.2.1–15E.2.9. [Google Scholar] [CrossRef]
- Chen, Y.W.; Ahmed, A.; Snoeck, H.W. Generation of three-dimensional lung bud organoid and its derived branching colonies. Protocol. Exchang. 2017. [Google Scholar] [CrossRef]
- de Wilde, A.H.; Raj, V.S.; Oudshoorn, D.; Bestebroer, T.M.; van Nieuwkoop, S.; Limpens, R.; Posthuma, C.C.; van der Meer, Y.; Barcena, M.; Haagmans, B.L.; et al. MERS-coronavirus replication induces severe in vitro cytopathology and is strongly inhibited by cyclosporin A or interferon-alpha treatment. J. Gen. Virol. 2013, 94, 1749–1760. [Google Scholar] [CrossRef]
- de Wilde, A.H.; Jochmans, D.; Posthuma, C.C.; Zevenhoven-Dobbe, J.C.; van Nieuwkoop, S.; Bestebroer, T.M.; van den Hoogen, B.G.; Neyts, J.; Snijder, E.J. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob. Agents Chemother. 2014, 58, 4875–4884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MeSH Browser. Available online: https://meshb.nlm.nih.gov/ (accessed on 16 November 2020).
- SciFinder. Available online: https://scifinder.cas.org/ (accessed on 16 November 2020).
- Law, V.; Knox, C.; Djoumbou, Y.; Jewison, T.; Guo, A.C.; Liu, Y.; Maciejewski, A.; Arndt, D.; Wilson, M.; Neveu, V.; et al. DrugBank 4.0: Shedding new light on drug metabolism. Nucleic Acids Res. 2014, 42, D1091–D1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ianevski, A.; Yao, R.; Biza, S.; Zusinaite, E.; Mannik, A.; Kivi, G.; Planken, A.; Kurg, K.; Tombak, E.M.; Ustav, M., Jr.; et al. Identification and Tracking of Antiviral Drug Combinations. Viruses 2020, 12, 1178. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Gotte, M. Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency. J. Biol. Chem. 2020, 295, 6785–6797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.J.; Wei, Y.J.; Chang, H.L.; Chang, P.Y.; Tsai, C.C.; Chen, Y.H.; Hsueh, P.R. Remdesivir use in the coronavirus disease 2019 pandemic: A mini-review. J. Microbiol. Immunol. Infect. 2021, 54, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Dyall, J.; Coleman, C.M.; Hart, B.J.; Venkataraman, T.; Holbrook, M.R.; Kindrachuk, J.; Johnson, R.F.; Olinger, G.G., Jr.; Jahrling, P.B.; Laidlaw, M.; et al. Repurposing of clinically developed drugs for treatment of Middle East respiratory syndrome coronavirus infection. Antimicrob. Agents Chemother. 2014, 58, 4885–4893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prassas, I.; Diamandis, E.P. Novel therapeutic applications of cardiac glycosides. Nat. Rev. Drug Discov. 2008, 7, 926–935. [Google Scholar] [CrossRef] [PubMed]
- Bertol, J.W.; Rigotto, C.; de Padua, R.M.; Kreis, W.; Barardi, C.R.; Braga, F.C.; Simoes, C.M. Antiherpes activity of glucoevatromonoside, a cardenolide isolated from a Brazilian cultivar of Digitalis lanata. Antivir. Res. 2011, 92, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, A.; Cai, H.; Forman, M.; He, R.; Shamay, M.; Arav-Boger, R. Human cytomegalovirus inhibition by cardiac glycosides: Evidence for involvement of the HERG gene. Antimicrob. Agents Chemother. 2012, 56, 4891–4899. [Google Scholar] [CrossRef] [Green Version]
- Burkard, C.; Verheije, M.H.; Haagmans, B.L.; van Kuppeveld, F.J.; Rottier, P.J.; Bosch, B.J.; de Haan, C.A. ATP1A1-mediated Src signaling inhibits coronavirus entry into host cells. J. Virol. 2015, 89, 4434–4448. [Google Scholar] [CrossRef] [Green Version]
- Jeon, S.; Ko, M.; Lee, J.; Choi, I.; Byun, S.Y.; Park, S.; Shum, D.; Kim, S. Identification of Antiviral Drug Candidates against SARS-CoV-2 from FDA-Approved Drugs. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef]
- Matsuyama, S.; Kawase, M.; Nao, N.; Shirato, K.; Ujike, M.; Kamitani, W.; Shimojima, M.; Fukushi, S. The inhaled steroid ciclesonide blocks SARS-CoV-2 RNA replication by targeting the viral replication-transcription complex in cultured cells. J. Virol. 2020, 95, e01648-20. [Google Scholar] [CrossRef]
- Epstein, M. Lercanidipine: A novel dihydropyridine calcium-channel blocker. Heart Dis. 2001, 3, 398–407. [Google Scholar] [CrossRef]
- Iwabuchi, K.; Yoshie, K.; Kurakami, Y.; Takahashi, K.; Kato, Y.; Morishima, T. Therapeutic potential of ciclesonide inhalation for COVID-19 pneumonia: Report of three cases. J. Infect. Chemother. 2020, 26, 625–632. [Google Scholar] [CrossRef]
- Yao, K.; Nagashima, K.; Miki, H. Pharmacological, pharmacokinetic, and clinical properties of benidipine hydrochloride, a novel, long-acting calcium channel blocker. J. Pharmacol. Sci. 2006, 100, 243–261. [Google Scholar] [CrossRef] [Green Version]
- Klein, G.R.; Köppel, H. Lercanidipine, a new third generation Ca-anatagonist in the treatment of hypertension. J. Clin. Basic Cardiol. 1999, 2, 169–174. [Google Scholar]
- Ozawa, Y.; Hayashi, K.; Kobori, H. New Generation Calcium Channel Blockers in Hypertensive Treatment. Curr. Hypertens. Rev. 2006, 2, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirtz, S.; Herzig, S. Molecular mechanisms of vasoselectivity of the 1,4-dihydropyridine lercanidipine. Br. J. Pharmacol. 2004, 142, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Combination | Synergy Score | Most Synergistic Area Score |
|---|---|---|
| Remdesivir–camostat | 21.3 | 25.7 |
| Remdesivir–nelfinavir | 13.9 | 19.5 |
| Remdesivir–cepharathine | 4.2 | 12.7 |
| Remdesivir–ciclesonide | −0.6 | 6.8 |
| Drug Combination | mCherry Fluorescence | CTG Assay | ||
|---|---|---|---|---|
| Synergy Score | Most Synergistic Area Score | Synergy Score | Most Synergistic Area Score | |
| Remdesivir–camostat | 8.3 | 17.3 | 22.4 | 27.7 |
| Remdesivir–nelfinavir | 7.2 | 11.1 | 42.6 | 51.8 |
| Remdesivir–cepharathine | 9.4 | 16.1 | 16.6 | 24.5 |
| Remdesivir–ciclesonide | 6.3 | 11.6 | 19.7 | 25.8 |
| Drug Name | Trade Name | Putative Drug Target | Pharmaceutical Action | IC50 2 (μM) | SD 3 (±) | CC50 4 (μM) | TI 5 |
|---|---|---|---|---|---|---|---|
| Ouabain #,† | Strodival | Na, K-exchanging ATPase pump | Cardiotonic agent | 0.08 | 0.0066 | >25 § | >312.5 |
| Digitoxin #,† | Digitaline | Ca, Na-exchanging ATPase pump | Cardiotonic agent | 0.16 | 0.0003 | >25 § | >156.3 |
| Digoxin #,† | Lanoxin | Ca, Na-exchanging ATPase pump | Cardiotonic agent | 0.17 | 0.0084 | >25 § | >147.1 |
| Niclosamide #,† | Niclocide, others | ATP synthase | Agrochemical | 0.55 | 0.363 | >25 § | >45.5 |
| Atovaquone * | Mepron | Unknown (lipophilic) | Anti-infective agent | 0.72 | 0.0585 | >25 | >34.7 |
| Regorafenib #,† (Bay 73–4506) | Stivarga | Multiple kinases | Anti-neoplastic agent | 2.31 | 0.0834 | >25 | >10.8 |
| Lercanidipine hydrochloride * | Zanidip | Calcium channel blocker | Cardiovascular agent | 2.36 | 0.1654 | >25 | >10.6 |
| Permethrin * | Elimite, others | Na channel | Agrochemical | 3.60 | 0.7573 | >25 | >6.9 |
| Octocrylene * | None | Estrogen receptor alpha | Additive in sunscreen | 3.62 | 0.6435 | >25 | >6.9 |
| Nelfinavir mesylate #,† | Viracept | HIV-1 protease | Antiviral agent | 3.62 | 0.0177 | >25 | >6.9 |
| Ciclesonide #,† | Alvesco, others | Glucocorticoid ligand | Anti-inflammatory agent | 4.07 | 0.4907 | >25 § | >6.1 |
| Benidipine hydrochloride # | Coniel | Calcium channel blocker | Cardiovascular agent | 4.07 | 0.7234 | >25 | >6.1 |
| Inhibitor Name | Pharmaceutical Action | IC50 2 (μM) | SD 3 (±) | CC50 4 (μM) | TI 5 |
|---|---|---|---|---|---|
| Emetine dihydrochloride | Anti-neoplastic agent | 0.08 | 0.0054 | >25 | >312.5 |
| Oxyclozanide | Anti-parasitic agent | 0.07 | 0.0060 | 20.92 | 298.9 |
| Cycloheximide | Protein synthesis inhibitor | 0.16 | 0.0140 | >25 | >156.3 |
| Lanatoside C | Cardiotonic agent | 0.19 | 0.0103 | >25 | >131.6 |
| Calcimycin | Antibacterial agent | 0.20 | 0.0165 | 18.10 | 90.5 |
| Digitoxigenin | Cardiotonic agent | 0.29 | 0.0220 | >25 | >86.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, M.; Chang, S.Y.; Byun, S.Y.; Ianevski, A.; Choi, I.; Pham Hung d’Alexandry d’Orengiani, A.-L.; Ravlo, E.; Wang, W.; Bjørås, M.; Kainov, D.E.; et al. Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19. Viruses 2021, 13, 651. https://doi.org/10.3390/v13040651
Ko M, Chang SY, Byun SY, Ianevski A, Choi I, Pham Hung d’Alexandry d’Orengiani A-L, Ravlo E, Wang W, Bjørås M, Kainov DE, et al. Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19. Viruses. 2021; 13(4):651. https://doi.org/10.3390/v13040651
Chicago/Turabian StyleKo, Meehyun, So Young Chang, Soo Young Byun, Aleksandr Ianevski, Inhee Choi, Anne-Laure Pham Hung d’Alexandry d’Orengiani, Erlend Ravlo, Wei Wang, Magnar Bjørås, Denis E. Kainov, and et al. 2021. "Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19" Viruses 13, no. 4: 651. https://doi.org/10.3390/v13040651