
Changes in Prevalence and Determinants of Self-Reported Hypertension among Bangladeshi Older Adults during the COVID-19 Pandemic

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
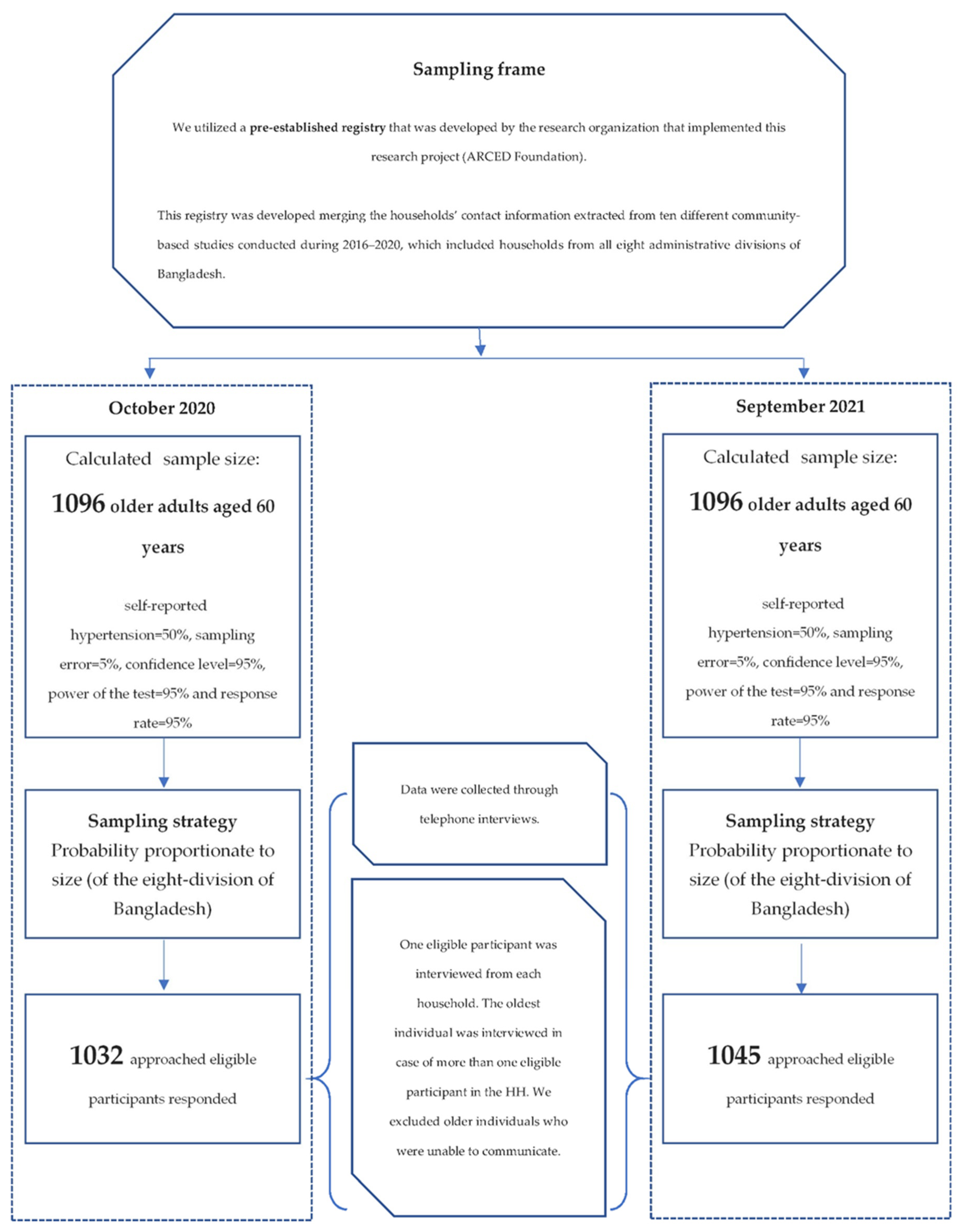
2.1. Study Design and Participants
2.2. Measures
2.2.1. Outcome Measure
2.2.2. Explanatory Variables
2.3. Data Collection Tools and Techniques
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Characteristics of the Participants
3.2. Changes in the Prevalence of Hypertension
3.3. Changes in Factors Associated with Hypertension
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 1 May 2022).
- Singh, A.K.; Gupta, R.; Misra, A. Comorbidities in COVID-19: Outcomes in hypertensive cohort and controversies with renin angiotensin system blockers. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Grassi, G.; Borghi, C.; Ferri, C.; Muiesan, M.L.; Volpe, M.; Iaccarino, G.; SARS-RAS Investigator Group. Clinical Characteristics and Outcomes of Patients with COVID-19 Infection: The Results of the SARS-RAS Study of the Italian Society of Hypertension. High Blood Press. Cardiovasc. Prev. 2021, 28, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Mubarik, S.; Liu, X.; Eshak, E.S.; Liu, K.; Liu, Q.; Wang, F.; Shi, F.; Wen, H.; Bai, J.; Yu, C. The Association of Hypertension with the Severity of and Mortality from the COVID-19 in the Early Stage of the Epidemic in Wuhan, China: A Multicenter Retrospective Cohort Study. Front. Med. 2021, 8, 631. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Mendis, S.; Puska, P.; Norrving, B.; WHO. Global Atlas on Cardiovascular Disease Prevention and Control; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Sarki, A.M.; Nduka, C.U.; Stranges, S.; Kandala, N.-B.; Uthman, O.A. Prevalence of hypertension in low-and middle-income countries: A systematic review and meta-analysis. Medicine 2015, 94, e1959. [Google Scholar] [CrossRef]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.; Small, J.D.; Geratz, J.D.; Alexander, L.K.; Baric, R.S. An experimental model for myocarditis and congestive heart failure after rabbit coronavirus infection. J. Infect. Dis. 1992, 165, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential effects of coronaviruses on the cardiovascular system: A review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Central Statistics Office. Social Impact of COVID-19 Survey November 2020 Well-Being and Lifestyle under Level 5 Restrictions. 2020. Available online: https://www.cso.ie/en/releasesandpublications/ep/p-sic19wbl5/socialimpactofcovid-19surveynovember2020well-beingandlifestyleunderlevel5restrictions/ (accessed on 11 January 2022).
- I-PARC. Impact of COVID-19 Restrictions on Sport and Recreational Walking, Q1 2021. 2021. Available online: https://i-parc.ie/?p=2026 (accessed on 11 January 2022).
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2021, 64, 108. [Google Scholar] [CrossRef] [PubMed]
- Bari, R.; Sultana, F. Second Wave of COVID-19 in Bangladesh: An integrated and coordinated set of actions is crucial to tackle current upsurge of cases and deaths. Front. Public Health 2021, 9, 699918. [Google Scholar] [CrossRef] [PubMed]
- Daria, S.; Islam, M.R. The second wave of COVID-19 pandemic in Bangladesh: An urgent call to save lives. Asia Pac. J. Public Health 2021, 33, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Huda, M.N.; Uddin, H.; Hasan, M.K.; Malo, J.S.; Duong, M.C.; Rahman, M.A. Examining Bangladesh’s responses to COVID-19 in light of Vietnam: Lessons learned. Glob. Biosecurity 2021, 3, 1–14. [Google Scholar]
- Bangladesh Bureau of Statistics. Elderly Population in Bangladesh: Current Features and Future Perspectives; Bangladesh Bureau of Statistics, Ministry of Bangladesh, Government of Bangladesh: Dhaka, Bangladesh, 2015.
- Chowdhury, M.Z.I.; Rahman, M.; Akter, T.; Akhter, T.; Ahmed, A.; Shovon, M.A.; Farhana, Z.; Chowdhury, N.; Turin, T.C. Hypertension prevalence and its trend in Bangladesh: Evidence from a systematic review and meta-analysis. Clin. Hypertens. 2020, 26, 10. [Google Scholar] [CrossRef]
- Murman, D.L. (Ed.) The Impact of Age on Cognition 2015; Thieme Medical Publishers: New York, NY, USA, 2015. [Google Scholar]
- Li, Y.; Godai, K.; Kido, M.; Komori, S.; Shima, R.; Kamide, K.; Kabayama, M. Cognitive decline and poor social relationship in older adults during COVID-19 pandemic: Can information and communications technology (ICT) use helps? BMC Geriatr. 2022, 22, 375. [Google Scholar] [CrossRef]
- Farron, M.R.; Kabeto, M.U.; Levine, D.A.; Wixom, C.R.; Langa, K.M. Blood pressure and cognitive function among older adults in India. J. Int. Med. Res. 2022, 50, 03000605211068720. [Google Scholar] [CrossRef]
- Lazo-Porras, M.; Ortiz-Soriano, V.; Moscoso-Porras, M.; Runzer-Colmenares, F.M.; Málaga, G.; Jaime Miranda, J. Cognitive impairment and hypertension in older adults living in extreme poverty: A cross-sectional study in Peru. BMC Geriatr. 2017, 17, 250. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Gilmour, S.; Akter, S.; Abe, S.K.; Saito, E.; Shibuya, K. Prevalence and control of hypertension in Bangladesh: A multilevel analysis of a nationwide population-based survey. J. Hypertens. 2015, 33, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Hanif, A.A.M.; Shamim, A.A.; Hossain, M.M.; Hasan, M.; Khan, M.S.A.; Hossaine, M.; Ullah, M.A.; Sarker, S.K.; Rahman, S.M.M.; Mitra, D.K. Gender-specific prevalence and associated factors of hypertension among elderly Bangladeshi people: Findings from a nationally representative cross-sectional survey. BMJ Open 2021, 11, e038326. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Zaman, M.M.; Islam, J.Y.; Chowdhury, J.; Ahsan, H.A.M.N.; Rahman, R.; Hassan, M.; Hossain, Z.; Alam, B.; Yasmin, R. Prevalence, treatment patterns, and risk factors of hypertension and pre-hypertension among Bangladeshi adults. J. Hum. Hypertens. 2018, 32, 334–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, J.Y.; Zaman, M.M.; Haq, S.A.; Ahmed, S.; Al-Quadir, Z. Epidemiology of hypertension among Bangladeshi adults using the 2017 ACC/AHA hypertension clinical practice guidelines and joint National Committee 7 guidelines. J. Hum. Hypertens. 2018, 32, 668–680. [Google Scholar] [CrossRef] [PubMed]
- Khanam, R.; Ahmed, S.; Rahman, S.; Al Kibria, G.M.; Syed, J.R.R.; Khan, A.M.; Moin, S.M.I.; Ram, M.; Gibson, D.G.; Pariyo, G. Prevalence and factors associated with hypertension among adults in rural Sylhet district of Bangladesh: A cross-sectional study. BMJ Open 2019, 9, e026722. [Google Scholar] [CrossRef]
- Mistry, S.K.; Harris, E.; Harris, M. Community health workers as healthcare navigators in primary care chronic disease management: A systematic review. J. Gen. Intern. Med. 2021, 36, 2755–2771. [Google Scholar] [CrossRef]
- Mistry, S.K.; Ali, A.R.M.; Hossain, M.; Yadav, U.N.; Ghimire, S.; Rahman, M.; Irfan, N.M.; Huque, R. Exploring depressive symptoms and its associates among Bangladeshi older adults amid COVID-19 pandemic: Findings from a cross-sectional study. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1487–1497. [Google Scholar] [CrossRef]
- Du, M.; Yin, S.; Wang, P.; Wang, X.; Wu, J.; Xue, M.; Zheng, H.; Zhang, Y.; Liang, D.; Wang, R. Self-reported hypertension in Northern China: A cross-sectional study of a risk prediction model and age trends. BMC Health Serv. Res. 2018, 18, 475. [Google Scholar] [CrossRef]
- Abir, T.; Osuagwu, U.L.; Kalimullah, N.A.; Yazdani, D.M.N.-A.; Husain, T.; Basak, P.; Goson, P.C.; Mamun, A.A.; Permarupan, P.Y.; Milton, A.H. Psychological Impact of COVID-19 Pandemic in Bangladesh: Analysis of a Cross-Sectional Survey. Health Secur. 2021, 19, 468–478. [Google Scholar] [CrossRef]
- Mamun, M.A.; Sakib, N.; Gozal, D.; Bhuiyan, A.I.; Hossain, S.; Bodrud-Doza, M.; Al Mamun, F.; Hosen, I.; Safiq, M.B.; Abdullah, A.H. The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. J. Affect. Disord. 2021, 279, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Cheruvu, V.K.; Chiyaka, E.T. Prevalence of depressive symptoms among older adults who reported medical cost as a barrier to seeking health care: Findings from a nationally representative sample. BMC Geriatr. 2019, 19, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banna, M.H.A.; Sayeed, A.; Kundu, S.; Christopher, E.; Hasan, M.T.; Begum, M.R.; Kormoker, T.; Dola, S.T.I.; Hassan, M.M.; Chowdhury, S. The impact of the COVID-19 pandemic on the mental health of the adult population in Bangladesh: A nationwide cross-sectional study. Int. J. Environ. Health Res. 2020, 32, 850–861. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.K.; Ali, A.M.; Akther, F.; Yadav, U.N.; Harris, M.F. Exploring fear of COVID-19 and its correlates among older adults in Bangladesh. Glob. Health 2021, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.K.; Ali, A.M.; Irfan, N.M.; Yadav, U.N.; Siddique, R.F.; Peprah, P.; Reza, S.; Rahman, Z.; Casanelia, L.; O’Callaghan, C. Prevalence and correlates of depressive symptoms among Rohingya (forcibly displaced Myanmar nationals or FDMNs) older adults in Bangladesh amid the COVID-19 pandemic. Glob. Mental Health. Epidemiol. 2021, 8, e23. [Google Scholar] [CrossRef]
- Liang, K.Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Wojciechowska, W.; Januszewicz, A.; Drożdż, T.; Rojek, M.; Bączalska, J.; Terlecki, M.; Kurasz, K.; Olszanecka, A.; Smólski, M.; Prejbisz, A. Blood Pressure and Arterial Stiffness in Association with Aircraft Noise Exposure: Long-Term Observation and Potential Effect of COVID-19 Lockdown. Hypertension 2021, 79, 325–334. [Google Scholar] [CrossRef]
- Feitosa, F.G.A.M.; Feitosa, A.D.M.; Paiva, A.M.G.; Mota-Gomes, M.A.; Barroso, W.S.; Miranda, R.D.; Barbosa, E.C.D.; Brandão, A.A.; Lima-Filho, J.L.; Sposito, A.C. Impact of the COVID-19 pandemic on blood pressure control: A nationwide home blood pressure monitoring study. Hypertens. Res. 2021, 45, 364–368. [Google Scholar] [CrossRef]
- Girerd, N.; Meune, C.; Duarte, K.; Vercamer, V.; Lopez-Sublet, M.; Mourad, J.-J. Evidence of a Blood Pressure Reduction during the COVID-19 Pandemic and Associated Lockdown Period: Insights from e-Health Data. Telemed. e-Health 2022, 28, 266–270. [Google Scholar] [CrossRef]
- Pengo, M.F.; Albini, F.; Guglielmi, G.; Mollica, C.; Soranna, D.; Zambra, G.; Zambon, A.; Bilo, G.; Parati, G. Home blood pressure during COVID-19-related lockdown in patients with hypertension. Eur. J. Prev. Cardiol. 2022, 25, e94–e96. [Google Scholar] [CrossRef]
- Gupta, A.; Maheshwari, A.; Verma, N.; Jagadeesha, A.; Dariya, S.S.; Sharma, A.; Saxena, D.; Srivastava, A.; Patni, B.; Das, D. Impact of COVID-19 pandemic on blood pressure of healthcare professionals during lockdown—An Indian Study. J. Hypertens. 2021, 39, e203. [Google Scholar] [CrossRef]
- Islam, M.T.; Talukder, A.K.; Siddiqui, M.N.; Islam, T. Tackling the COVID-19 pandemic: The Bangladesh perspective. J. Public Health Res. 2020, 9, 1794. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.M.; Solomon, S.D. Influence of physical activity on hypertension and cardiac structure and function. Curr. Hypertens. Rep. 2015, 17, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghimire, R.; Adhikari, S. Effects of COVID-19 on non-communicable diseases and reproductive health services in a district hospital of Nepal. Arch. Pulmonol. Respir. Care 2020, 6, 065–067. [Google Scholar]
- Mistry, S.K.; Ali, A.R.M.M.; Yadav, U.N.; Ghimire, S.; Hossain, M.B.; Das Shuvo, S.; Saha, M.; Sarwar, S.; Nirob, M.M.H.; Sekaran, V.C. Older adults with non-communicable chronic conditions and their health care access amid COVID-19 pandemic in Bangladesh: Findings from a cross-sectional study. PLoS ONE 2021, 16, e0255534. [Google Scholar]
- Du, S.; Zhou, Y.; Fu, C.; Wang, Y.; Du, X.; Xie, R. Health literacy and health outcomes in hypertension: An integrative review. Int. J. Nurs. Sci. 2018, 5, 301–309. [Google Scholar] [CrossRef]
- Leng, B.; Jin, Y.; Li, G.; Chen, L.; Jin, N. Socioeconomic status and hypertension: A meta-analysis. J. Hypertens. 2015, 33, 221–229. [Google Scholar] [CrossRef]
- Pan, Y.; Cai, W.; Cheng, Q.; Dong, W.; An, T.; Yan, J. Association between anxiety and hypertension: A systematic review and meta-analysis of epidemiological studies. Neuropsychiatr. Dis. Treat. 2015, 11, 1121. [Google Scholar]
- Celik, M.; Yilmaz, Y.; Karagoz, A.; Kahyaoglu, M.; Cakmak, E.O.; Kup, A.; Celik, F.B.; Karaduman, A.; Kulahcioglu, S.; Izci, S. Anxiety disorder associated with the COVID-19 pandemic causes deterioration of blood pressure control in primary hypertensive patients. Medeni. Med. J. 2021, 36, 83. [Google Scholar]
- Feng, X.; Kelly, M.; Sarma, H. The association between educational level and multimorbidity among adults in Southeast Asia: A systematic review. PLoS ONE 2021, 16, e0261584. [Google Scholar] [CrossRef]
- Sultana, M.S.; Khan, A.H.; Hossain, S.; Islam, T.; Hasan, M.T.; Ahmed, H.U.; Khan, J.A.M. The association between financial hardship and mental health difficulties among adult wage earners during the COVID-19 pandemic in Bangladesh: Findings from a cross-sectional analysis. Front. Psychiatry 2021, 12, 635884. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Hayden, K.M.; May, N.S.; Haring, B.; Liu, Z.; Henderson, V.W.; Chen, J.; Gracely, E.J.; Wassertheil-Smoller, S.; Rapp, S.R. Association between blood pressure levels and cognitive impairment in older women: A prospective analysis of the Women’s Health Initiative Memory Study. Lancet Healthy Longev. 2022, 3, E42–E53. [Google Scholar] [CrossRef]
- Petersen, R.C. Clinical practice. Mild cognitive impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- Reitz, C.; Tang, M.-X.; Manly, J.; Mayeux, R.; Luchsinger, J.A. Hypertension and the risk of mild cognitive impairment. Arch. Neurol. 2007, 64, 1734–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagi, S.; Akaike, M.; Aihara, K.-I.; Iwase, T.; Yoshida, S.; Sumitomo-Ueda, Y.; Ikeda, Y.; Ishikawa, K.; Matsumoto, T.; Sata, M. High plasma aldosterone concentration is a novel risk factor of cognitive impairment in patients with hypertension. Hypertens. Res. 2011, 34, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.A.; Power, M.C.; Gottesman, R.F. Defining the relationship between hypertension, cognitive decline, and dementia: A review. Curr. Hypertens. Rep. 2017, 19, 24. [Google Scholar] [PubMed]
- Wysocki, M.; Luo, X.; Schmeidler, J.; Dahlman, K.; Lesser, G.T.; Grossman, H.; Haroutunian, V.; Beeri, M.S. Hypertension is associated with cognitive decline in elderly people at high risk for dementia. Am. J. Geriatr. Psychiatry 2012, 20, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Adams, A.M.; Vuckovic, M.; Graul, E.; Rashid, S.F.; Sarker, M. Supporting the role and enabling the potential of community health workers in Bangladesh’s rural maternal and newborn health programs: A qualitative study. J. Glob. Health Rep. 2020, 4, e2020029. [Google Scholar] [CrossRef]
- Mistry, S.K.; Harris-Roxas, B.; Yadav, U.N.; Shabnam, S.; Rawal, L.B.; Harris, M.F. Community health workers can provide psychosocial support to the people during COVID-19 and beyond in Low-and Middle-Income Countries. Front. Public Health 2021, 9, 666753. [Google Scholar] [CrossRef]
- Volkmer, I. Social Media and COVID-19: A Global Study of Digital Crisis Interaction among Gen Z and Millennials; WHO: Geneva, Switzerland, 2021. [Google Scholar]


{kind=link}
| Characteristics | Round 1 | Round 2 | p2 | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Overall | 1032 | 100.0 | 1045 | 100.0 | |
| Administrative division | |||||
| Barishal | 149 | 14.4 | 146 | 14.0 | 0.001 |
| Chattogram | 137 | 13.3 | 98 | 9.4 | |
| Dhaka | 210 | 20.4 | 172 | 16.5 | |
| Mymensingh | 63 | 6.1 | 69 | 6.6 | |
| Khulna | 158 | 15.3 | 198 | 19.0 | |
| Rajshahi | 103 | 10.0 | 145 | 13.9 | |
| Rangpur | 144 | 14.0 | 161 | 15.4 | |
| Sylhet | 68 | 6.6 | 56 | 5.4 | |
| Age (year) | |||||
| 60–69 | 803 | 77.8 | 790 | 75.6 | 0.385 |
| >= 70 | 229 | 22.2 | 255 | 24.4 | |
| Sex | |||||
| Male | 676 | 65.5 | 620 | 59.3 | 0.004 |
| Female | 356 | 34.5 | 425 | 40.7 | |
| Marital status | |||||
| Married | 840 | 81.4 | 799 | 76.5 | 0.006 |
| Without partner | 192 | 18.6 | 246 | 23.5 | |
| Formal schooling | |||||
| No formal schooling | 602 | 58.3 | 540 | 51.7 | 0.002 |
| Having formal schooling | 430 | 41.7 | 505 | 48.3 | |
| Family size | |||||
| ≤4 | 318 | 30.8 | 347 | 33.2 | 0.243 |
| >4 | 714 | 69.2 | 698 | 66.8 | |
| Family monthly income (BDT) 1 | |||||
| <5000 | 145 | 14.1 | 121 | 11.6 | <0.001 |
| 5000–10,000 | 331 | 32.1 | 469 | 44.9 | |
| >10,000 | 556 | 53.9 | 455 | 43.5 | |
| Residence | |||||
| Urban | 269 | 26.1 | 182 | 17.4 | <0.001 |
| Rural | 763 | 73.9 | 863 | 82.6 | |
| Current occupation | |||||
| Employed | 419 | 40.6 | 407 | 39.0 | 0.441 |
| Unemployed/retired | 613 | 59.4 | 638 | 61.1 | |
| Living arrangement | |||||
| Living with family | 953 | 92.3 | 992 | 94.9 | 0.016 |
| Living alone | 79 | 7.7 | 53 | 5.1 | |
| Walking distance to the nearest health centre | |||||
| <30 min | 503 | 48.7 | 581 | 55.6 | 0.002 |
| ≥30 min | 529 | 51.3 | 464 | 44.4 | |
| Problem in memory or concentration | |||||
| No problem | 782 | 75.8 | 676 | 64.7 | <0.001 |
| Low memory or concentration | 250 | 24.2 | 369 | 35.3 | |
| Receiving COVID-19-related information from health workers | |||||
| No | 936 | 90.7 | 981 | 93.9 | 0.007 |
| Yes | 96 | 9.3 | 64 | 6.1 | |
| Characteristics | Round 1 | Round 2 | p1 | ||
|---|---|---|---|---|---|
| n | %Hypertensive | n | %Hypertensive | ||
| Overall | 1032 | 43.7 | 1045 | 56.3 | 0.006 |
| Division | |||||
| Barishal | 149 | 43.3 | 146 | 56.7 | 0.213 |
| Chattogram | 137 | 43.6 | 98 | 56.4 | 0.041 |
| Dhaka | 210 | 58.3 | 172 | 41.7 | 0.444 |
| Mymensingh | 63 | 36.8 | 69 | 63.2 | 0.305 |
| Khulna | 158 | 43.2 | 198 | 56.8 | 0.825 |
| Rajshahi | 103 | 34.8 | 145 | 65.2 | 0.303 |
| Rangpur | 144 | 33.3 | 161 | 66.7 | 0.024 |
| Sylhet | 68 | 36.4 | 56 | 63.6 | 0.013 |
| Age (year) | |||||
| 60–69 | 803 | 44.8 | 790 | 55.2 | 0.036 |
| ≥70 | 229 | 41.2 | 255 | 58.8 | 0.102 |
| Sex | |||||
| Male | 676 | 48.3 | 620 | 51.7 | 0.189 |
| Female | 356 | 37.7 | 425 | 62.3 | 0.014 |
| Marital status | |||||
| Married | 840 | 46.8 | 799 | 53.3 | 0.080 |
| Without partners | 192 | 35.4 | 246 | 64.6 | 0.036 |
| Formal schooling | |||||
| No formal schooling | 602 | 35.4 | 285 | 64.6 | 0.036 |
| Having formal schooling | 430 | 42.1 | 208 | 57.9 | 0.165 |
| Family size | |||||
| ≤4 | 318 | 35.8 | 347 | 64.2 | 0.006 |
| >4 | 286 | 46.5 | 698 | 53.5 | 0.101 |
| Family monthly income (BDT) 1 | |||||
| <5000 | 145 | 45.8 | 86 | 54.2 | 0.182 |
| 5000–10,000 | 125 | 32.0 | 235 | 68.0 | 0.021 |
| >10,000 | 202 | 49.2 | 172 | 50.8 | 0.035 |
| Residence | |||||
| Urban | 269 | 53.8 | 182 | 46.2 | 0.194 |
| Rural | 763 | 40.9 | 863 | 59.2 | 0.014 |
| Current occupation | |||||
| Employed | 419 | 51.9 | 407 | 48.1 | 0.764 |
| Unemployed/retired | 613 | 40.1 | 638 | 59.9 | 0.000 |
| Living arrangement | |||||
| Living with family | 387 | 42.4 | 392 | 57.7 | 0.003 |
| Living alone | 29 | 62.1 | 24 | 37.9 | 0.782 |
| Distance from the nearest health centre | |||||
| <30 min | 503 | 36.5 | 581 | 63.5 | 0.001 |
| ≥30 min | 529 | 52.7 | 464 | 47.3 | 0.852 |
| Problem in memory or concentration | |||||
| No problem | 782 | 50.8 | 676 | 49.2 | 0.317 |
| Low memory or concentration | 250 | 32.9 | 369 | 67.1 | 0.022 |
| Receiving COVID-19-related information from health workers | |||||
| No | 936 | 38.8 | 981 | 61.2 | <0.001 |
| Yes | 96 | 67.1 | 64 | 32.9 | 0.092 |
| Characteristics | cOR 1 | 95% CI | p3 | aOR 2 | 95% CI | p4 |
|---|---|---|---|---|---|---|
| Self-reported hypertension | ||||||
| 2020 Survey | Ref | Ref | ||||
| 2021 Survey | 1.35 | 1.09–1.68 | 0.006 | 1.34 | 1.06–1.70 | 0.013 |
| Characteristics | Round 1 (n = 1032) | Round 2 (n = 1045) | ||||
|---|---|---|---|---|---|---|
| aOR 1 | 95% CI | p | aOR | 95% CI | p | |
| Age (year) | ||||||
| 60–69 | Ref | Ref | ||||
| ≥70 | 1.35 | 0.91–2.02 | 0.138 | 1.20 | 0.84–1.72 | 0.308 |
| Sex | ||||||
| Male | - | Ref | ||||
| Female | 1.15 | 0.79–1.67 | 0.479 | |||
| Marital status | ||||||
| Married | Ref | Ref | ||||
| Without partners | 1.31 | 0.83–2.07 | 0.239 | 1.34 | 0.92–1.97 | 0.131 |
| Formal schooling | ||||||
| No formal schooling | Ref | Ref | ||||
| Having formal schooling | 2.05 | 1.42–2.95 | <0.001 | 1.66 | 1.21–2.26 | 0.002 |
| Family size | ||||||
| ≤4 | Ref | Ref | ||||
| >4 | 1.41 | 0.93–2.13 | 0.105 | 1.08 | 0.77–1.50 | 0.659 |
| Family monthly income (BDT) 2 | ||||||
| <5000 | Ref | Ref | ||||
| 5000–10,000 | 0.99 | 0.55–1.80 | 0.979 | 0.75 | 0.45–1.26 | 0.281 |
| >10,000 | 1.30 | 0.74–2.29 | 0.357 | 1.32 | 0.80–2.19 | 0.279 |
| Current occupation | ||||||
| Employed | Ref | Ref | ||||
| Unemployed/retired | 1.36 | 0.93–1.99 | 0.110 | 1.70 | 1.15–2.50 | 0.007 |
| Living arrangement | ||||||
| Living with family | Ref | |||||
| Living alone | 2.07 | 1.11–3.84 | 0.022 | - | ||
| Distance from the nearest health centre | ||||||
| <30 min | - | Ref | ||||
| ≥30 min | 0.76 | 0.56–1.04 | 0.088 | |||
| Problem in memory or concentration | ||||||
| No problem | Ref | Ref | ||||
| Low memory or concentration | 1.72 | 1.17–2.53 | 0.006 | 1.91 | 1.39–2.62 | <0.001 |
| Receiving COVID-19-related information from health workers | ||||||
| No | Ref | Ref | ||||
| Yes | 6.20 | 3.80–10.12 | 0.000 | 2.40 | 1.37–4.18 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistry, S.K.; Ali, A.M.; Yadav, U.N.; Khanam, F.; Huda, M.N.; Lim, D.; Chowdhury, A.A.; Sarma, H. Changes in Prevalence and Determinants of Self-Reported Hypertension among Bangladeshi Older Adults during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13475. https://doi.org/10.3390/ijerph192013475
Mistry SK, Ali AM, Yadav UN, Khanam F, Huda MN, Lim D, Chowdhury AA, Sarma H. Changes in Prevalence and Determinants of Self-Reported Hypertension among Bangladeshi Older Adults during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(20):13475. https://doi.org/10.3390/ijerph192013475
Chicago/Turabian StyleMistry, Sabuj Kanti, ARM Mehrab Ali, Uday Narayan Yadav, Fouzia Khanam, Md. Nazmul Huda, David Lim, ABM Alauddin Chowdhury, and Haribondhu Sarma. 2022. "Changes in Prevalence and Determinants of Self-Reported Hypertension among Bangladeshi Older Adults during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 20: 13475. https://doi.org/10.3390/ijerph192013475