
The Impact of Charlson Comorbidity Index on the Functional Capacity of COVID-19 Survivors: A Prospective Cohort Study with One-Year Follow-Up

 ,
, 
 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
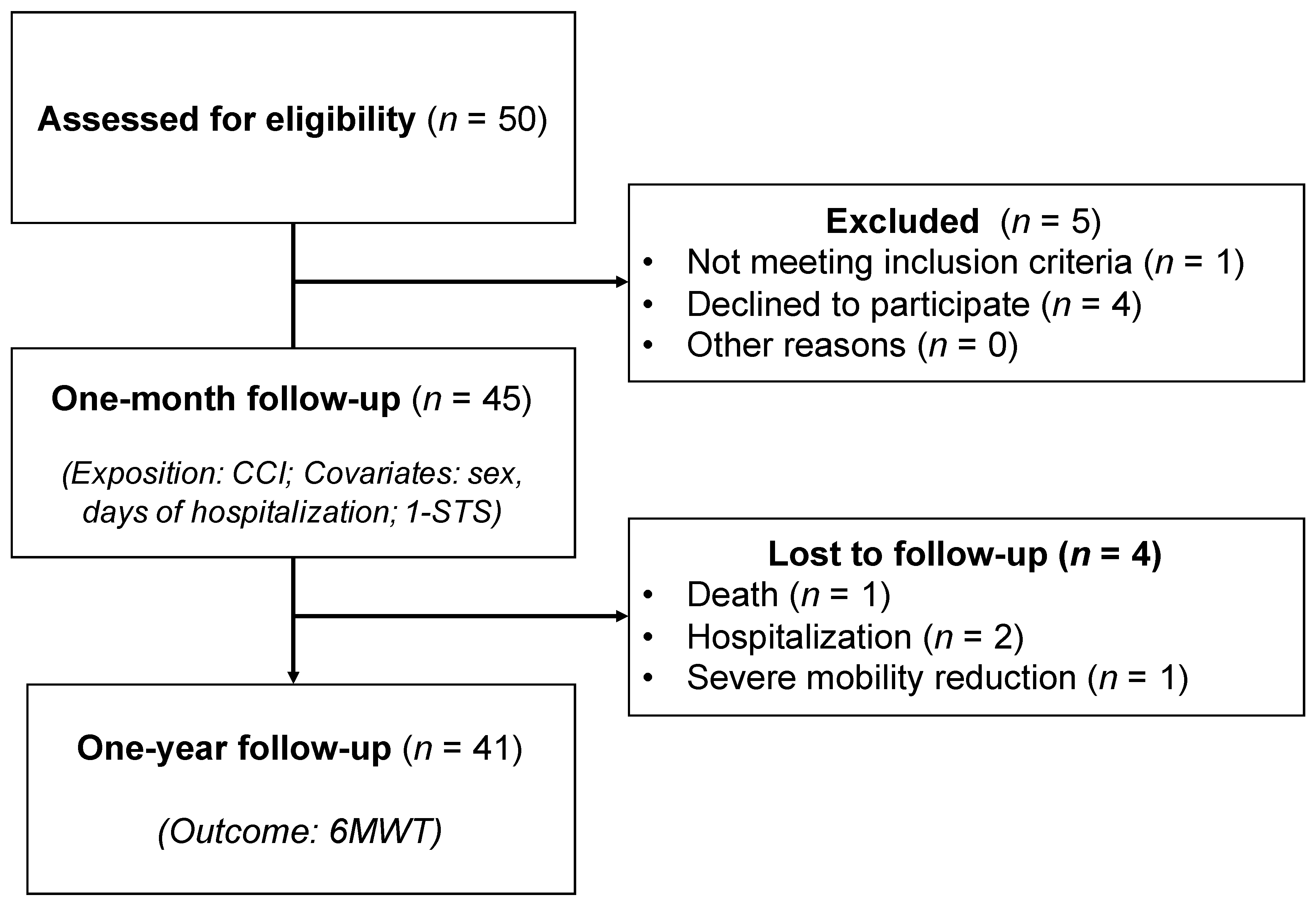
2.1. Study Setting, Design, and Participants
2.2. Data Collection (One Month after Discharge)
2.3. Charlson Comorbidity Index (One Month after Discharge)
2.4. Follow-Up
2.5. 6-Minute Walk Test (1 Year after Discharge)
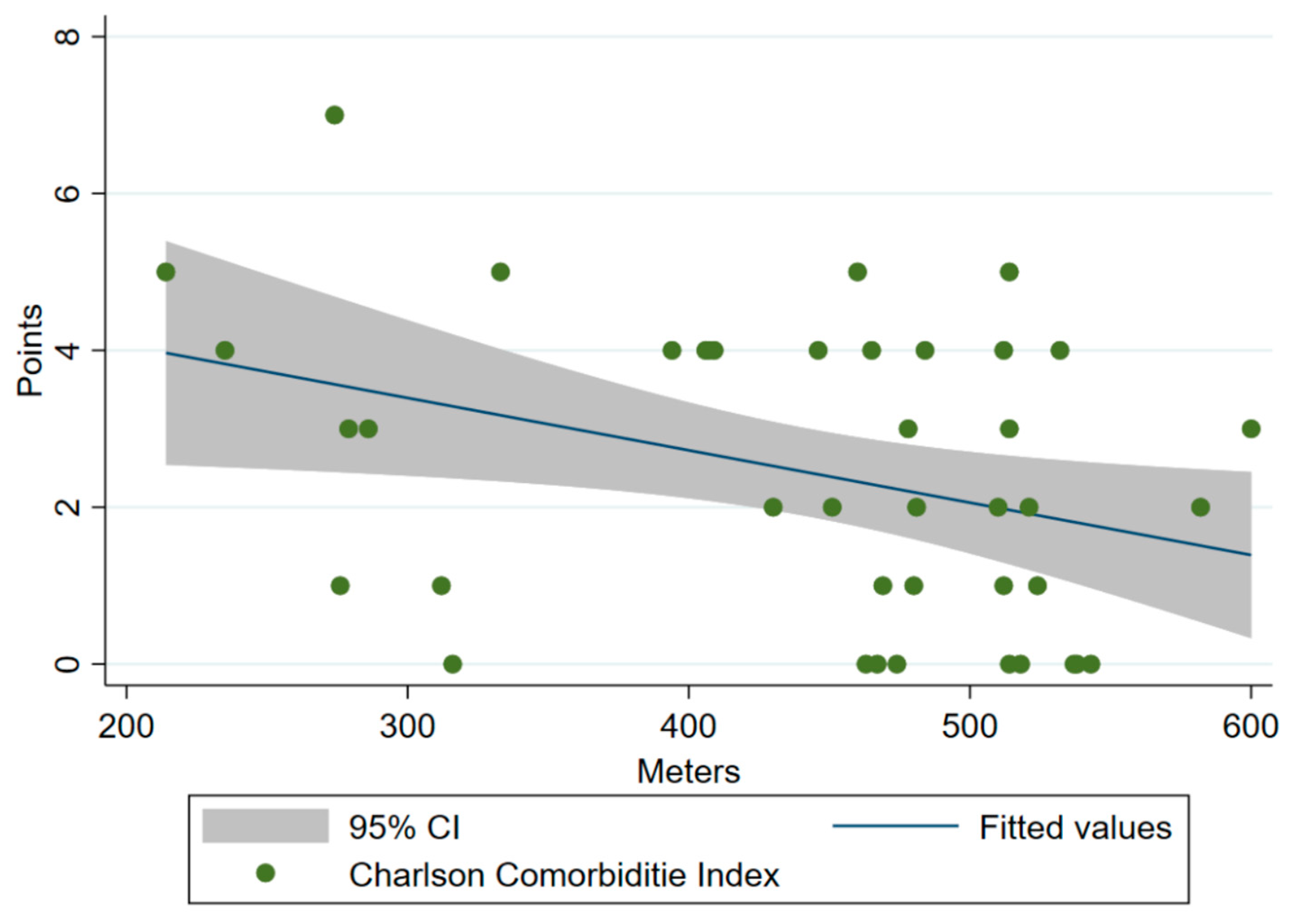
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Anon. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 11 May 2022).
- Montani, D.; Savale, L.; Noel, N.; Meyrignac, O.; Colle, R.; Gasnier, M.; Corruble, E.; Beurnier, A.; Jutant, E.-M.; Pham, T.; et al. Post-acute COVID-19 syndrome. Eur. Respir. Rev. 2022, 31, 210185. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Ramirez, D.; Normand, K.; Zhaoyun, Y.; Torres-Castro, R. Long-term impact of COVID-19: A systematic review of the literature and meta-analysis. Biomedicines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paneroni, M.; Simonelli, C.; Saleri, M.; Bertacchini, L.; Venturelli, M.; Troosters, T.; Ambrosino, N.; Vitacca, M. Muscle strength and physical performance in patients without previous disabilities recovering from COVID-19 pneumonia. Am. J. Phys. Med. Rehabil. 2021, 100, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Christensen, D.M.; Strange, J.E.; Gislason, G.; Torp-Pedersen, C.; Gerds, T.; Fosbøl, E.; Phelps, M.D. Charlson comorbidity index score and risk of severe outcome and death in Danish COVID-19 patients. J. Gen. Intern. Med. 2020, 35, 2801–2803. [Google Scholar] [CrossRef]
- Varol, Y.; Hakoglu, B.; Cirak, A.K.; Polat, G.; Komurcuoglu, B.; Akkol, B.; Atasoy, C.; Bayramic, E.; Balci, G.; Ataman, S.; et al. The impact of charlson comorbidity index on mortality from SARS-CoV—2 virus infection and A novel COVID—19 mortality index: CoLACD. Int. J. Clin. Pract. 2021, 75, e13858. [Google Scholar] [CrossRef]
- Kuswardhani, R.T.; Henrina, J.; Pranata, R.; Lim, M.A.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2103–2109. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Caminati, A.; Bianchi, A.; Cassandro, R.; Mirenda, M.R.; Harari, S. Walking distance on 6-MWT is a prognostic factor in idiopathic pulmonary fibrosis. Respir. Med. 2009, 103, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Yazdanyar, A.; Aziz, M.M.; Enright, P.L.; Edmundowicz, D.; Boudreau, R.; Sutton-Tyrell, K.; Kuller, L.; Newman, A.B. Association between 6-minute walk test and all-cause mortality, coronary heart disease–specific mortality, and incident coronary heart disease. J. Aging Health 2014, 26, 583–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curci, C.; Pisano, F.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; Bergonzi, R.; De Franceschi, S.; Moro, P.; Guarnieri, R.; Ferrillo, M.; et al. Early rehabilitation in post-acute COVID-19 patients: Data from an Italian COVID-19 rehabilitation unit and proposal of a treatment protocol of a treatment protocol. Eur. J. Phys. Rehabil. Med. 2020, 56, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Cortés, R.; Rivera-Lillo, G.; Arias-Campoverde, M.; Soto-García, D.; García-Palomera, R.; Torres-Castro, R. Use of sit-to-stand test to assess the physical capacity and exertional desaturation in patients post COVID-19. Chronic Respir. Dis. 2021, 18, 1479973121999205. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Negro, F.D.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Coovadia, H.; Jewkes, R.; Barron, P.; Sanders, D.; McIntyre, D. How the COVID-19 infection tsunami revolutionized the work of respiratory physiotherapists: An experience from Northern Italy. Monaldi Arch. Chest Dis. Arch. 2020, 90. [Google Scholar] [CrossRef]
- Gabriel, S.E.; Crowson, C.S.; O’Fallon, W.M. A comparison of two comorbidity instruments in arthritis. J. Clin. Epidemiol. 1999, 52, 1137–1142. [Google Scholar] [CrossRef]
- Pencina, K.M.; Bhasin, S.; Luo, M.; Baggs, G.E.; Pereira, S.L.; Davis, G.J.; E Deutz, N.; Travison, T.G. Predictor biomarkers of nonelective hospital readmission and mortality in malnourished hospitalized older adults. J. Frailty Aging 2020, 9, 226–231. [Google Scholar] [CrossRef]
- Miller, A.; Pohlig, R.T.; Wright, T.; Kim, H.E.; Reisman, D.S. Beyond Physical Capacity: Factors Associated With Real-world Walking Activity After Stroke. Arch. Phys. Med. Rehabil. 2021, 102, 1880–1887.e1. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 18, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Ozalevli, S.; Ozden, A.; Itil, O.; Akkoclu, A. Comparison of the Sit-to-Stand Test with 6 min walk test in patients with chronic obstructive pulmonary disease. Respir. Med. 2007, 101, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Strassmann, A.; Steurer-Stey, C.; Lana, K.D.; Zoller, M.; Turk, A.J.; Suter, P.; Puhan, M.A. Population-based reference values for the 1-min sit-to-stand test. Int. J. Public Health 2013, 58, 949–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osses, A.R.; Yáñez, V.J.; Barría, P.P.; Palacios, M.S.; Dreyse, D.J.; Díaz, P.O.; Lisboa, B.C. Reference values for the 6-minutes walking test in healthy subjects 20–80 years old. Revista Medica Chile 2010, 138, 1124–1130. [Google Scholar]
- Powell, H.; Lim, L.L.-Y.; Heller, R.F. Accuracy of administrative data to assess comorbidity in patients with heart disease: An Australian perspective. J. Clin. Epidemiol. 2001, 54, 687–693. [Google Scholar] [CrossRef]
- Caballero, P.E.J.; Espuela, F.L.; Cuenca, J.C.P.; Moreno, J.M.R.; Zamorano, J.D.P.; Naranjo, I.C. Charlson comorbidity index in ischemic stroke and intracerebral hemorrhage as predictor of mortality and functional outcome after 6 months. J. Stroke Cerebrovasc. Dis. 2013, 22, e214–e218. [Google Scholar] [CrossRef]
- Tessier, A.; Finch, L.; Daskalopoulou, S.S.; Mayo, N.E. Validation of the Charlson Comorbidity Index for predicting functional outcome of stroke. Arch. Phys. Med. Rehabil. 2008, 89, 1276–1283. [Google Scholar] [CrossRef]
- Groll, D.L.; Heyland, D.K.; Caeser, M.; Wright, J.G. Assessment of long-term physical function in acute respiratory distress syndrome (ARDS) patients: Comparison of the Charlson Comorbidity Index and the Functional Comorbidity Index. Am. J. Phys. Med. Rehabil. 2006, 85, 574–581. [Google Scholar] [CrossRef]
- Ozsoy, I.; Kahraman, B.O.; Acar, S.; Ozalevli, S.; Akkoclu, A.; Savci, S. Factors influencing activities of daily living in subjects with COPD. Respir. Care 2019, 64, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Núñez-Cortés, R.; Ortega-Palavecinos, M.; Soto-Carmona, C.; Torres-Gangas, P.; Concha-Rivero, M.P.; Torres-Castro, R. Social determinants of health associated with severity and mortality in patients with COVID-19. Gac. Med. Mex. 2021, 157, 263–270. [Google Scholar] [CrossRef]
- Tan, L.F.; Lim, Z.Y.; Choe, R.; Seetharaman, S.; Merchant, R.A. Screening for frailty and sarcopenia among older persons in medical outpatient clinics and its associations with healthcare burden. J. Am. Med. Dir. Assoc. 2017, 18, 583–587. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Cognitive impairment is independently associated with definitive and possible sarcopenia in hospitalized older adults: The prevalence and impact of comorbidities. Geriatr. Gerontol. Int. 2017, 17, 1048–1056. [Google Scholar] [CrossRef]
- Gong, G.; Wan, W.; Zhang, X.; Liu, Y.; Liu, X.; Yin, J. Correlation between the Charlson comorbidity index and skeletal muscle mass/physical performance in hospitalized older people potentially suffering from sarcopenia. BMC Geriatr. 2019, 19, 367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferté, J.-B.; Boyer, F.C.; Taiar, R.; Pineau, C.; Barbe, C.; Rapin, A. Impact of resistance training on the 6-minute walk test in individuals with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2022, 65, 101582. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.M.; Nalamalapu, S.R.; Nunna, K.; Rabiee, A.; Friedman, L.A.; Colantuoni, E.; Needham, D.M.; Dinglas, V.D. Six-minute walk distance after critical illness: A systematic review and meta-analysis. J. Intensive Care Med. 2021, 36, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Zemedikun, D.; Gray, L.J.; Khunti, K.; Davies, M.J.; Dhalwani, N.N. Patterns of Multimorbidity in Middle-Aged and Older Adults: An Analysis of the UK Biobank Data. Mayo Clin. Proc. 2018, 93, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Bandeen-Roche, K.; Seplaki, C.; Huang, J.; Buta, B.; Kalyani, R.R.; Varadhan, R.; Xue, Q.-L.; Walston, J.D.; Kasper, J.D. Frailty in older adults: A nationally representative profile in the United States. J. Gerontol. Ser. A 2015, 70, 1427–1434. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Total (n = 41) |
|---|---|
| Age (mean ± SD) | 58.8 ± 12.7 |
| Sex, male, n (%) | 20 (48.8) |
| BMI (mean ± SD) | 30.7 ± 5.2 |
| Invasive ventilation, n (%) | 12 (28.3) |
| Hospitalization days (mean ± SD) | 13.5 (4 to 55) |
| 1-STS (repetitions) | 20 (12 to 29) |
| Comorbidities, n (%) | |
| Myocardial infarction | 2 (4.9) |
| Congestive heart failure | 2 (4.9) |
| Peripheral vascular disease | 24 (58.5) |
| Cerebrovascular accident | 1 (2.4) |
| COPD | 4 (9.8) |
| Liver disease | 1 (2.4) |
| Diabetes mellitus | 14 (34.1) |
| Chronic kidney disease | 2 (4.9) |
| Cancer | 2 (4.9) |
| Charlson comorbidity index (points) | 2 (0 to 8) |
| One-year follow-up | |
| 1-STS (repetitions) | 23.5 (12 to 35) |
| 6MWT (meters) | 443.5 (214 to 600) |
| 6MWT (%predicted) | 80.5 ± 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Núñez-Cortés, R.; Malhue-Vidal, C.; Gath, F.; Valdivia-Lobos, G.; Torres-Castro, R.; Cruz-Montecinos, C.; Martinez-Arnau, F.M.; Pérez-Alenda, S.; López-Bueno, R.; Calatayud, J. The Impact of Charlson Comorbidity Index on the Functional Capacity of COVID-19 Survivors: A Prospective Cohort Study with One-Year Follow-Up. Int. J. Environ. Res. Public Health 2022, 19, 7473. https://doi.org/10.3390/ijerph19127473
Núñez-Cortés R, Malhue-Vidal C, Gath F, Valdivia-Lobos G, Torres-Castro R, Cruz-Montecinos C, Martinez-Arnau FM, Pérez-Alenda S, López-Bueno R, Calatayud J. The Impact of Charlson Comorbidity Index on the Functional Capacity of COVID-19 Survivors: A Prospective Cohort Study with One-Year Follow-Up. International Journal of Environmental Research and Public Health. 2022; 19(12):7473. https://doi.org/10.3390/ijerph19127473
Chicago/Turabian StyleNúñez-Cortés, Rodrigo, Constanza Malhue-Vidal, Florencia Gath, Gonzalo Valdivia-Lobos, Rodrigo Torres-Castro, Carlos Cruz-Montecinos, Francisco M. Martinez-Arnau, Sofía Pérez-Alenda, Rubén López-Bueno, and Joaquín Calatayud. 2022. "The Impact of Charlson Comorbidity Index on the Functional Capacity of COVID-19 Survivors: A Prospective Cohort Study with One-Year Follow-Up" International Journal of Environmental Research and Public Health 19, no. 12: 7473. https://doi.org/10.3390/ijerph19127473