
Research Capacity Training on Environmental Health and Noncommunicable Diseases in the Country of Georgia: Challenges and Lessons Learned during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
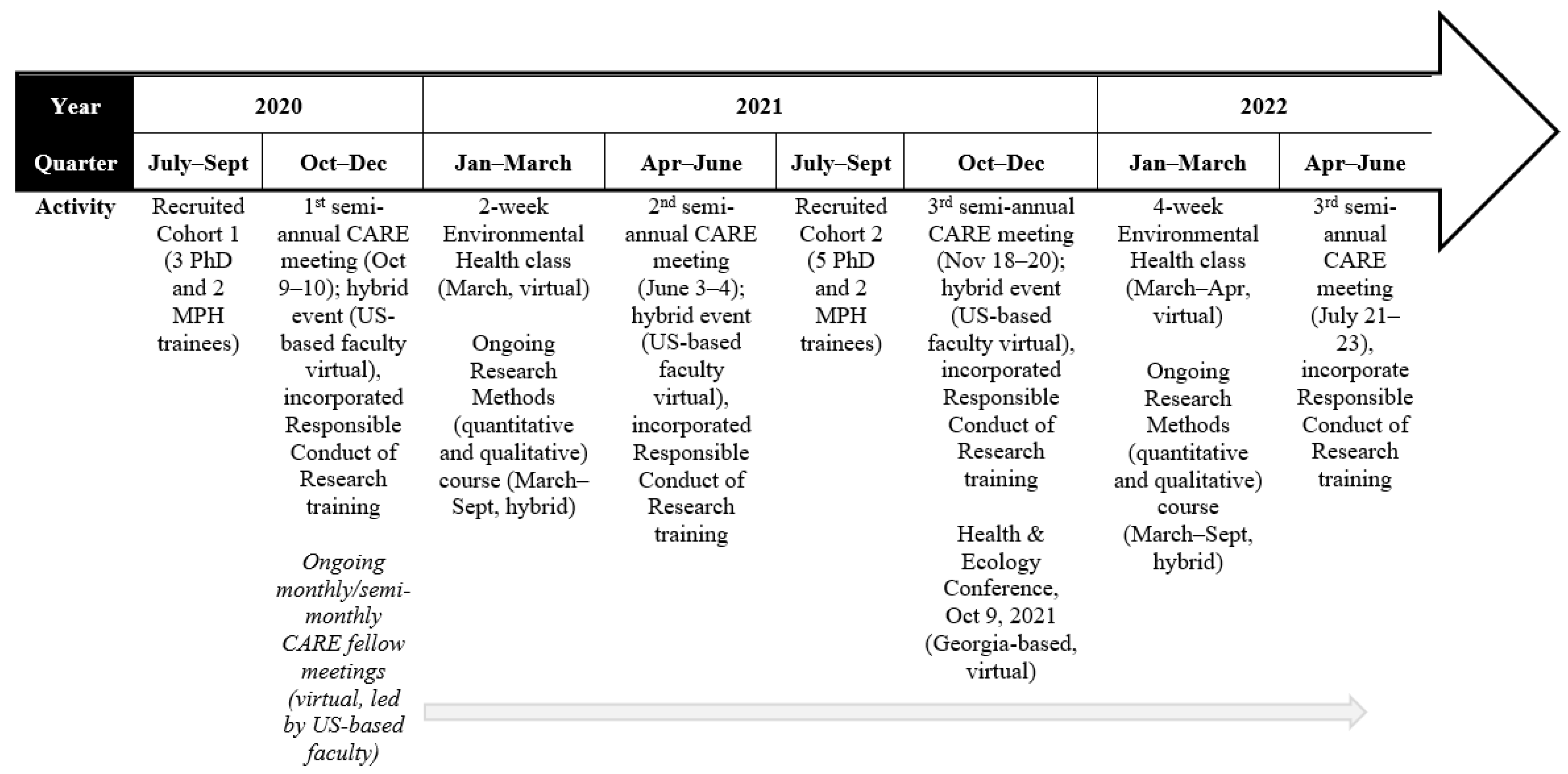
2.1. Training Program Description
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Program Benefits and Resource Utilization
3.3. Experiences with Mentor/Mentee Relationships
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fogarty International Center. Available online: https://www.fic.nih.gov/About/Pages/mission-vision.aspx (accessed on 22 May 2020).
- Fogarty International Center, Fogarty at 50: Advancing Science for Global Health Since 1968. 2020. Available online: https://www.fic.nih.gov/About/50th-anniversary/Documents/fogarty-international-center-nih-at-50.pdf (accessed on 2 May 2022).
- Fogarty International Center, Global Infectious Disease Research Training—Fogarty International Center @ NIH. 2020. Available online: https://www.fic.nih.gov/Programs/Pages/infectious-disease.aspx (accessed on 22 April 2022).
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Heimburger, D.C.; Carothers, C.L.; Blevins, M.; Warner, T.L.; Vermund, S.H. Impact of Global Health Research Training on Scholarly Productivity: The Fogarty International Clinical Research Scholars and Fellows Program. Am. J. Trop. Med. Hyg. 2015, 93, 1201–1207. [Google Scholar] [CrossRef] [Green Version]
- Berg, C.; Sturua, L. The critical need for enhancing the research capacity regarding the intersection of air pollution and non-communicable diseases in Georgia. Georgian Med. News 2020, 178–182. [Google Scholar]
- World Health Organization. Burden of Disesase from the Joint Effects of Household and Ambient Air Pollution for 2016. 2018. Available online: https://cdn.who.int/media/docs/default-source/air-quality-database/aqd-2018/ap_joint_effect_bod_results_may2018.pdf (accessed on 15 May 2022).
- World Health Organization. WHO Global Ambient Air Quality Database (Update 2018). 2018. Available online: https://www.who.int/data/gho/data/themes/air-pollution/who-air-quality-database (accessed on 18 May 2022).
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. World Health Statistics Data Visualizations Dashboard: Air Pollution; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cole, D.C.; Johnson, N.L.; Mejia, R.; McCullough, H.; Turcotte-Tremblay, A.-M.; Barnoya, J.; Luco, M.S.F. Mentorings health researchers globally: Diverse experiences, programmes, challenges and responses. Glob. Public Health 2015, 11, 1093–1108. [Google Scholar] [CrossRef]
- Feldman, M.D.; Steinauer, J.E.; Khalili, M.; Huang, L.; Kahn, J.S.; Lee, K.A.; Creasman, J.; Brown, J.S. A Mentor Development Program for Clinical Translational Science Faculty Leads to Sustained, Improved Confidence in Mentoring Skills. Clin. Transl. Sci. 2012, 5, 362–367. [Google Scholar] [CrossRef]
- Gandhi, M.; Raj, T.; Fernandez, R.; Rispel, L.; Nxumalo, N.; Lescano, A.G.; Bukusi, E.A.; Mmbaga, B.T.; Heimburger, D.C.; Cohen, C.R. Mentoring the Mentors: Implementation and Evaluation of Four Fogarty-Sponsored Mentoring Training Workshops in Low-and Middle-Income Countries. Am. J. Trop. Med. Hyg. 2019, 100, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Pfund, C.; Pribbenow, C.M.; Branchaw, J.; Lauffer, S.M.; Handelsman, J. The Merits of Training Mentors. Science 2006, 311, 473–474. [Google Scholar] [CrossRef]
- Von Bartheld, C.S.; Houmanfar, R.; Candido, A. Prediction of junior faculty success in biomedical research: Comparison of metrics and effects of mentoring programs. PeerJ 2015, 3, e1262. [Google Scholar] [CrossRef]
- Wanberg, C.R.; Welsh, E.T.; Hezlett, S.A. Mentoring research: A review and dynamic process model. Res. Pers. Hum. Resour. Manag. 2004, 22, 39–124. [Google Scholar] [CrossRef]
- Cohen, J.G.; Sherman, A.E.; Kiet, T.K.; Kapp, D.S.; Osann, K.; Chen, L.-M.; O’Sullivan, P.S.; Chan, J.K. Characteristics of success in mentoring and research productivity—A case–control study of academic centers. Gynecol. Oncol. 2012, 125, 8–13. [Google Scholar] [CrossRef]
- Hou, L.; Mehta, S.D.; Christian, E.; Joyce, B.; Lesi, O.; Anorlu, R.; Akanmu, A.S.; Imade, G.; Okeke, E.; Musah, J.; et al. Impact of the COVID-19 pandemic on global health research training and education. J. Glob. Health 2020, 10, 020366. [Google Scholar] [CrossRef]
- National Institutes of Health. Mentoring Program: Annual Mentoring Evaluation Form; National Institutes of Health: Bethesda, MD, USA, 2022. Available online: https://hr.nih.gov/sites/default/files/public/documents/working-nih/mentoring/pdf/mentee-evaluation-rev.pdf (accessed on 1 May 2022).
- Yukawa, M.; Gansky, S.A.; O’Sullivan, P.; Teherani, A.; Feldman, M.D. A new Mentor Evaluation Tool: Evidence of validity. PLoS ONE 2020, 15, e0234345. [Google Scholar] [CrossRef]
- Wang, C.-H.; Shannon, D.M.; Ross, M.E. Students’ characteristics, self-regulated learning, technology self-efficacy, and course outcomes in online learning. Distance Educ. 2013, 34, 302–323. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Trainees n = 12 | Faculty n = 13 |
|---|---|---|
| Participant Characteristics | ||
| Gender | ||
| Male | 3 | 6 |
| Female | 9 | 7 |
| Years in program | ||
| Since 2020 | 5 | 8 |
| Since 2021 | 7 | 5 |
| Trainee track | ||
| MPH | 4 | -- |
| PhD | 8 | -- |
| Country | ||
| Georgia | -- | 7 |
| US | -- | 6 |
| Mentor/Mentee Evaluations | ||
| Communication and relationship quality: | ||
| Solicits [mentor’s/mentee’s] thoughts and opinions when making suggestions or recommendations | 3.91 (0.30) a | 3.41 (0.78) |
| Trainee considers mentor’s advice and accepts their encouragement with respect to goals and objectives | 3.83 (0.39) a | 3.36 (0.83) |
| [Mentors/mentee] responsive to emails and other forms of communication | 3.83 (0.39) | 3.30 (0.84) |
| Satisfaction with mentor/mentee relationships | 3.83 (0.58) | 3.10 (1.00) |
| Happy with the frequency of meetings | 3.73 (0.65) a | 2.90 (0.96) |
| Find the meetings productive | 3.58 (0.67) | 3.20 (0.96) |
| Instrumental support: | ||
| Consider [mentor’s/mentee’s] perspective and respect mentee goals and objectives | 3.91 (0.30) | 3.43 (0.86) |
| Mentor connected mentee with other professionals who could “fill in the gaps” in areas where they might be less skilled | 3.63 (0.74) b | 2.93 (1.10) |
| Worked together to identify tangible steps to meet mentee goals and objectives | 3.33 (0.89) | 3.31 (0.89) |
| You and your [mentors/mentee] completed goals planned | 3.33 (0.78) | 2.97 (0.96) |
| Program Benefits and Resource Utilization | |
|---|---|
| Trainees | Faculty |
| What training, workshops, and other professional development activities you think will be beneficial to you and your professional growth? | What ideas do you have about training for this program that you think would be beneficial to trainees? |
|
|
| Experiences with Mentor/Mentee Relationship | |
| What have you learned about yourself from being a [mentee/mentor] in this program? If new, what do you hope to learn? | |
| Trainees | Faculty |
Have learned:
| Have learned:
|
| What challenges have you found or do you anticipate regarding the mentor/mentee relationship in this program specifically? | |
| Trainees | Faculty |
|
|
| What suggestions do you have for improving mentor/mentee experiences?If new, what do you hope to have as part of the mentor/mentee experience? | |
| Trainees | Faculty |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berg, C.J.; Sturua, L.; Marsit, C.J.; Baramidze, L.; Kiladze, N.; Caudle, W.M. Research Capacity Training on Environmental Health and Noncommunicable Diseases in the Country of Georgia: Challenges and Lessons Learned during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 8154. https://doi.org/10.3390/ijerph19138154
Berg CJ, Sturua L, Marsit CJ, Baramidze L, Kiladze N, Caudle WM. Research Capacity Training on Environmental Health and Noncommunicable Diseases in the Country of Georgia: Challenges and Lessons Learned during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(13):8154. https://doi.org/10.3390/ijerph19138154
Chicago/Turabian StyleBerg, Carla J., Lela Sturua, Carmen J. Marsit, Levan Baramidze, Nino Kiladze, and William Michael Caudle. 2022. "Research Capacity Training on Environmental Health and Noncommunicable Diseases in the Country of Georgia: Challenges and Lessons Learned during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 13: 8154. https://doi.org/10.3390/ijerph19138154