
Individual Characteristics as Prognostic Factors of the Evolution of Hospitalized COVID-19 Romanian Patients: A Comparative Observational Study between the First and Second Waves Based on Gaussian Graphical Models and Structural Equation Modeling


 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data—Sample, Features, Compilation
2.2. Methodology—Model, Testing and Validation
3. Results
3.1. Results of the Clinical/Medical Detailed Observation and Monitoring of COVID-19 Patients from the Two Waves of Infection
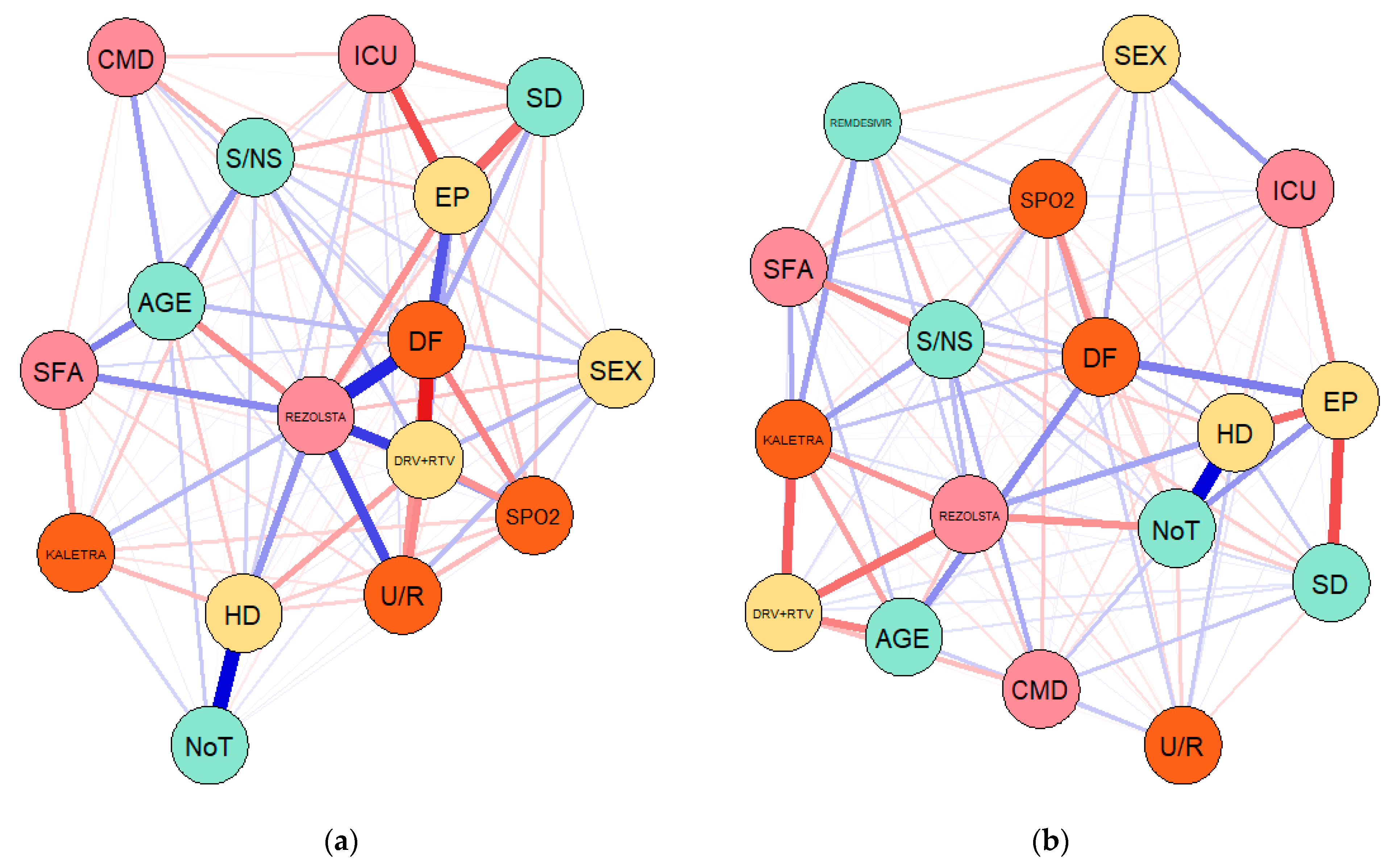
3.2. Results of the Empirical Network Analysis—Gaussian Graphical Models (GGMs)
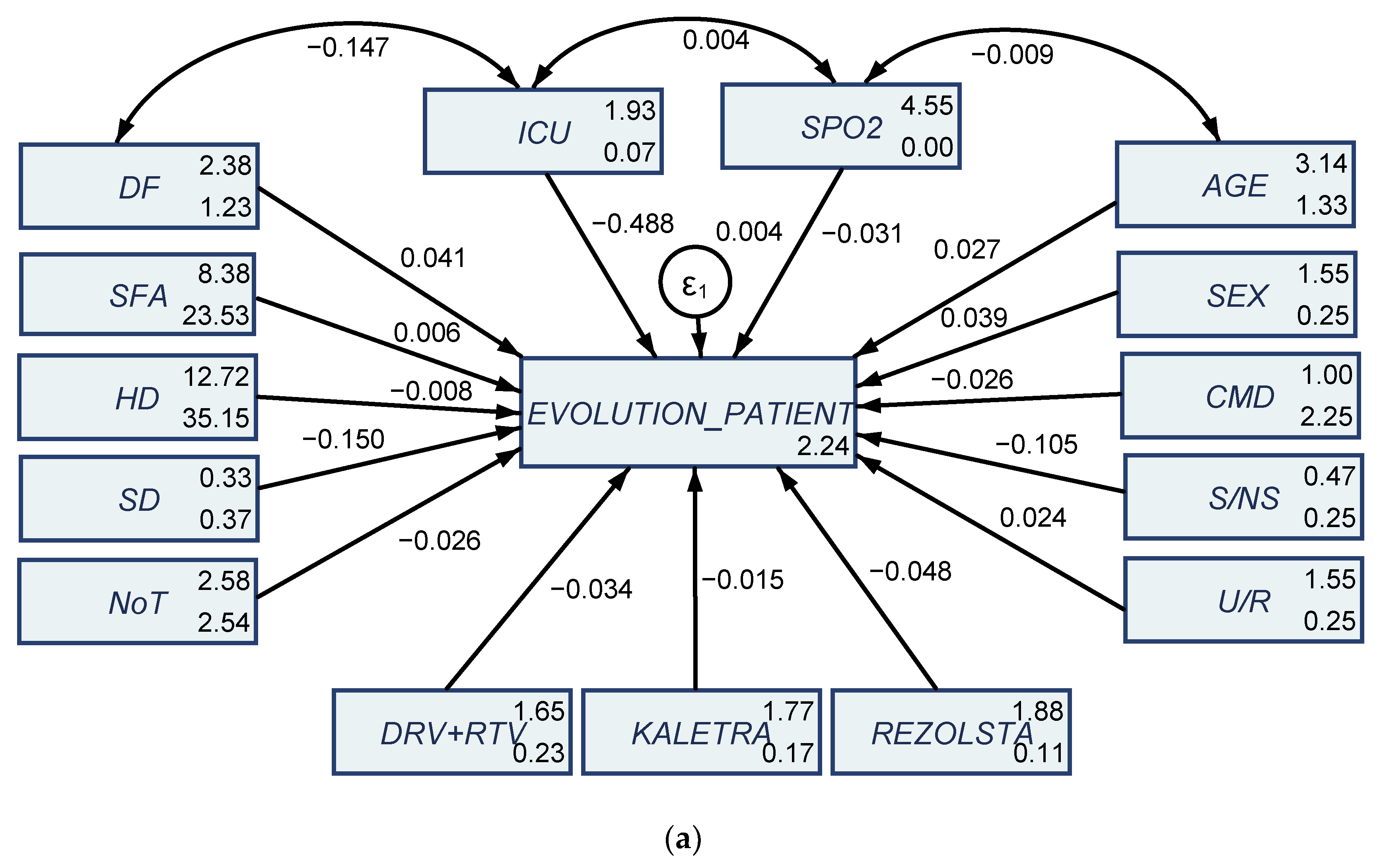
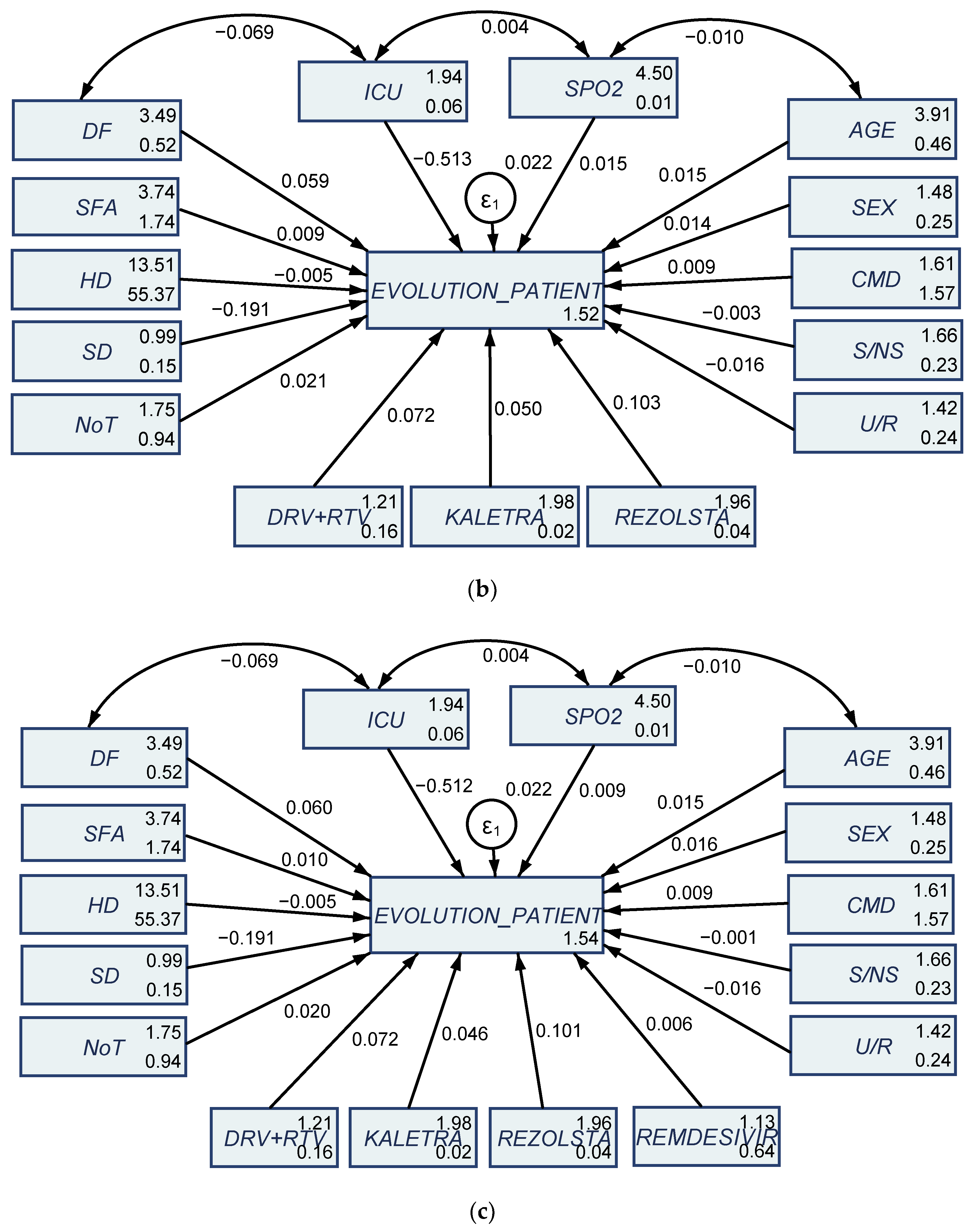
3.3. Results of Structural Equation Modeling (SEM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronym | Variable/Measure—Detailed Description |
|---|---|
| AGE | Age |
| SEX | Sex |
| U/R | Urban/rural |
| CMD | Comorbidities |
| S/NS | Smoker/non-smoker |
| HD | Hospitalization days |
| DF | Disease form (mild, moderate, severe, critical, asymptomatic) |
| SFA | Symptomatogoly at first apperareance |
| SD | Symptomatogoly at discharge |
| EP | Evolution of the patient (favourable, unfavourable/death) |
| SPO2 | Peripheral oxygen saturation |
| ICU | Intensive care unit |
| NoT | Number of tests until the patient is n negative |
| DTV + RTV | Darunavir + ritonavir |
| KALETRA | Lopinavir + ritonavir |
| REZOLSTA | Darunavir + cobicistat |
| REMDESIVIR | Remdesivir |
| (1—Figure 4a) | (2—Figure 4b) | (3—Figure 4c) | |
|---|---|---|---|
| Sample 1 145 Patients | Sample 2 130 Patients | Sample 2 cu REMDESIVIR (130) | |
| EP | |||
| SFA | 0.00584 (0.00330) | 0.00932 (0.0126) | 0.00980 (0.0127) |
| SD | −0.150 *** (0.0241) | −0.191 *** (0.0444) | −0.191 *** (0.0444) |
| HD | −0.00754 ** (0.00285) | −0.00533 (0.00309) | −0.00531 (0.00309) |
| DF | 0.0412 (0.0232) | 0.0587 * (0.0288) | 0.0598 * (0.0290) |
| AGE | 0.0271 (0.0162) | 0.0153 (0.0270) | 0.0152 (0.0270) |
| SEX | 0.0385 (0.0237) | 0.0143 (0.0326) | 0.0157 (0.0330) |
| CMD | −0.0262 * (0.0107) | 0.00889 (0.0137) | 0.00899 (0.0137) |
| S/NS | −0.105 *** (0.0294) | −0.00326 (0.0357) | −0.00132 (0.0363) |
| ICU | −0.488 *** (0.0570) | −0.513 *** (0.0807) | −0.512 *** (0.0807) |
| SPO2 | −0.0310 (0.237) | 0.0150 (0.272) | 0.00880 (0.272) |
| DRV + RTV | −0.0341 (0.0386) | 0.0717 (0.0471) | 0.0719 (0.0471) |
| KALETRA | −0.0150 (0.0312) | 0.0498 (0.119) | 0.0457 (0.120) |
| REZOLSTA | −0.0483 (0.0472) | 0.103 (0.0891) | 0.101 (0.0892) |
| NoT | −0.0263 ** (0.00948) | 0.0210 (0.0222) | 0.0203 (0.0223) |
| U/R | 0.0239 (0.0235) | −0.0162 (0.0320) | −0.0161 (0.0320) |
| REMDESIVIR | 0.00569 (0.0197) | ||
| _constant | 2.238 * (1.065) | 1.518 (1.354) | 1.540 (1.355) |
| / | |||
| mean(SFA) | 8.375 *** (0.767) | 3.735 *** (0.131) | 3.735 *** (0.131) |
| mean(SD) | 0.325 *** (0.0961) | 0.990 *** (0.0380) | 0.990 *** (0.0380) |
| mean(HD) | 12.72 *** (0.937) | 13.51 *** (0.737) | 13.51 *** (0.737) |
| mean(DF) | 2.375 *** (0.176) | 3.490 *** (0.0717) | 3.490 *** (0.0717) |
| mean(AGE) | 3.140 *** (0.182) | 3.909 *** (0.0671) | 3.909 *** (0.0671) |
| mean(SEX) | 1.550 *** (0.0787) | 1.480 *** (0.0495) | 1.480 *** (0.0495) |
| mean(CMD) | 1 *** (0.237) | 1.608 *** (0.124) | 1.608 *** (0.124) |
| mean(S/NS) | 0.475 *** (0.0790) | 1.657 *** (0.0470) | 1.657 *** (0.0470) |
| mean(ICU) | 1.925 *** (0.0416) | 1.941 *** (0.0233) | 1.941 *** (0.0233) |
| mean(SPO2) | 4.551 *** (0.00811) | 4.501 *** (0.00777) | 4.501 *** (0.00777) |
| mean(DRV + RTV) | 1.650 *** (0.0754) | 1.206 *** (0.0400) | 1.206 *** (0.0400) |
| mean(KALETRA) | 1.775 *** (0.0660) | 1.980 *** (0.0137) | 1.980 *** (0.0137) |
| mean(REZOLSTA) | 1.875 *** (0.0523) | 1.961 *** (0.0192) | 1.961 *** (0.0192) |
| mean(NoT) | 2.575 *** (0.252) | 1.745 *** (0.0957) | 1.745 *** (0.0957) |
| mean(U/R) | 1.550 *** (0.0787) | 1.422 *** (0.0489) | 1.422 *** (0.0489) |
| var(e.EP) | 0.00412 *** (0.000922) | 0.0218 *** (0.00305) | 0.0218 *** (0.00305) |
| var(SFA) | 23.53 *** (5.262) | 1.744 *** (0.244) | 1.744 *** (0.244) |
| var(SD) | 0.369 *** (0.0826) | 0.147 *** (0.0206) | 0.147 *** (0.0206) |
| var(HD) | 35.15 *** (7.860) | 55.37 *** (7.753) | 55.37 *** (7.753) |
| var(DF) | 1.234 *** (0.276) | 0.524 *** (0.0734) | 0.524 *** (0.0734) |
| var(AGE) | 1.326 *** (0.296) | 0.459 *** (0.0643) | 0.459 *** (0.0643) |
| var(SEX) | 0.248 *** (0.0553) | 0.250 *** (0.0350) | 0.250 *** (0.0350) |
| var(CMD) | 2.250 *** (0.503) | 1.572 *** (0.220) | 1.572 *** (0.220) |
| var(S/NS) | 0.249 *** (0.0558) | 0.225 *** (0.0316) | 0.225 *** (0.0316) |
| var(ICU) | 0.0694 *** (0.0155) | 0.0554 *** (0.00775) | 0.0554 *** (0.00775) |
| var(SPO2) | 0.00263 *** (0.000588) | 0.00615 *** (0.000861) | 0.00615 *** (0.000861) |
| var(DRV + RTV) | 0.228 *** (0.0509) | 0.163 *** (0.0229) | 0.163 *** (0.0229) |
| var(KALETRA) | 0.174 *** (0.0390) | 0.0192 *** (0.00269) | 0.0192 *** (0.00269) |
| var(REZOLSTA) | 0.109 *** (0.0245) | 0.0377 *** (0.00528) | 0.0377 *** (0.00528) |
| var(NoT) | 2.544 *** (0.569) | 0.935 *** (0.131) | 0.935 *** (0.131) |
| var(U/R) | 0.248 *** (0.0553) | 0.244 *** (0.0341) | 0.244 *** (0.0341) |
| cov(SFA,SD) | 0.853 (0.485) | −0.00260 (0.0501) | −0.00260 (0.0501) |
| cov(SFA,HD) | 9.928 * (4.811) | −0.149 (0.973) | −0.149 (0.973) |
| cov(SFA,DF) | 3.409 *** (1.008) | 0.198 * (0.0967) | 0.198 * (0.0967) |
| cov(SFA,AGE) | 1.686 (0.923) | 0.202 * (0.0909) | 0.202 * (0.0909) |
| cov(SFA,SEX) | −0.0563 (0.382) | −0.0297 (0.0654) | −0.0297 (0.0654) |
| cov(SFA,CMD) | 2.550 * (1.219) | −0.0646 (0.164) | −0.0646 (0.164) |
| cov(SFA,S/NS) | 0.0469 (0.383) | −0.159 * (0.0640) | −0.159 * (0.0640) |
| cov(SFA,ICU) | −0.272 (0.207) | −0.00577 (0.0308) | −0.00577 (0.0308) |
| cov(SFA,SPO2) | 0.0193 (0.0394) | −0.00544 (0.0103) | −0.00544 (0.0103) |
| cov(SFA,DRV + RTV) | −1.044 ** (0.401) | −0.0337 (0.0530) | −0.0337 (0.0530) |
| cov(SFA,KALETRA) | −0.366 (0.325) | 0.0340 (0.0184) | 0.0340 (0.0184) |
| cov(SFA,REZOLSTA) | 0.772 ** (0.282) | −0.0104 (0.0254) | −0.0104 (0.0254) |
| cov(SFA,NoT) | 3.709 ** (1.357) | 0.0600 (0.127) | 0.0600 (0.127) |
| cov(SFA,U/R) | 0.219 (0.383) | −0.0649 (0.0649) | −0.0649 (0.0649) |
| cov(SD,HD) | 0.514 (0.575) | 0.00500 (0.282) | 0.00500 (0.282) |
| cov(SD,DF) | 0.303 ** (0.117) | −0.0638 * (0.0282) | −0.0638 * (0.0282) |
| cov(SD,AGE) | 0.239 * (0.117) | −0.00362 (0.0257) | −0.00362 (0.0257) |
| cov(SD,SEX) | 0.0712 (0.0491) | 0.00471 (0.0190) | 0.00471 (0.0190) |
| cov(SD,CMD) | 0.475 ** (0.163) | 0.00596 (0.0476) | 0.00596 (0.0476) |
| cov(SD,S/NS) | −0.00438 (0.0480) | −0.0328 (0.0183) | −0.0328 (0.0183) |
| cov(SD,ICU) | −0.0756 ** (0.0280) | 0.0288 ** (0.00938) | 0.0288 ** (0.00938) |
| cov(SD,SPO2) | −0.00739 (0.00506) | −0.000792 (0.00298) | −0.000792 (0.00298) |
| cov(SD,DRV+RTV) | −0.0862 (0.0478) | 0.00202 (0.0153) | 0.00202 (0.0153) |
| cov(SD,KALETRA) | 0.0231 (0.0403) | −0.000192 (0.00526) | −0.000192 (0.00526) |
| cov(SD,REZOLSTA) | −0.00937 (0.0318) | −0.000384 (0.00737) | −0.000384 (0.00737) |
| cov(SD,NoT) | 0.138 (0.155) | −0.101 ** (0.0380) | −0.101 ** (0.0380) |
| cov(SD,U/R) | −0.00375 (0.0478) | −0.00567 (0.0188) | −0.00567 (0.0188) |
| cov(HD,DF) | 2.278 * (1.102) | 1.750 ** (0.561) | 1.750 ** (0.561) |
| cov(HD,AGE) | −0.679 (1.085) | 0.816 (0.506) | 0.816 (0.506) |
| cov(HD,SEX) | −0.0737 (0.467) | −0.559 (0.372) | −0.559 (0.372) |
| cov(HD,CMD) | 0.600 (1.409) | 2.141 * (0.948) | 2.141 * (0.948) |
| cov(HD,S/NS) | −0.0194 (0.468) | −0.207 (0.350) | −0.207 (0.350) |
| cov(HD,ICU) | −0.246 (0.250) | −0.666 *** (0.185) | −0.666 *** (0.185) |
| cov(HD,SPO2) | 0.0680 (0.0492) | −0.370 *** (0.0684) | −0.370 *** (0.0684) |
| cov(HD,DRV + RTV) | −0.821 (0.466) | −0.360 (0.300) | −0.360 (0.300) |
| cov(HD,KALETRA) | −0.662 (0.405) | 0.0394 (0.102) | 0.0394 (0.102) |
| cov(HD,REZOLSTA) | 0.916 ** (0.342) | 0.0396 (0.143) | 0.0396 (0.143) |
| cov(HD,NoT) | 5.608 ** (1.738) | 4.316 *** (0.831) | 4.316 *** (0.831) |
| cov(HD,U/R) | 0.751 (0.481) | 0.0890 (0.364) | 0.0890 (0.364) |
| cov(DF,AGE) | 0.554 * (0.220) | 0.195 *** (0.0523) | 0.195 *** (0.0523) |
| cov(DF,SEX) | −0.00625 (0.0874) | 0.0292 (0.0359) | 0.0292 (0.0359) |
| cov(DF,CMD) | 1.125 *** (0.318) | 0.231 * (0.0928) | 0.231 * (0.0928) |
| cov(DF,S/NS) | −0.0531 (0.0881) | 0.0408 (0.0343) | 0.0408 (0.0343) |
| cov(DF,ICU) | −0.147 ** (0.0518) | −0.0692 *** (0.0182) | −0.0692 *** (0.0182) |
| cov(DF,SPO2) | −0.00688 (0.00907) | −0.0255 *** (0.00617) | −0.0255 *** (0.00617) |
| cov(DF,DRV + RTV) | −0.394 *** (0.104) | −0.0519 (0.0294) | −0.0519 (0.0294) |
| cov(DF,KALETRA) | −0.0156 (0.0734) | 0.00961 (0.00999) | 0.00961 (0.00999) |
| cov(DF,REZOLSTA) | 0.172 ** (0.0641) | 0.00942 (0.0139) | 0.00942 (0.0139) |
| cov(DF,NoT) | 0.534 (0.293) | 0.233 ** (0.0731) | 0.233 ** (0.0731) |
| cov(DF,U/R) | 0.144 (0.0903) | −0.0302 (0.0355) | −0.0302 (0.0355) |
| cov(AGE,SEX) | −0.0722 (0.0913) | 0.0154 (0.0336) | 0.0154 (0.0336) |
| cov(AGE,CMD) | 0.807 ** (0.301) | 0.230 ** (0.0872) | 0.230 ** (0.0872) |
| cov(AGE,S/NS) | 0.245 * (0.0988) | 0.00586 (0.0319) | 0.00586 (0.0319) |
| cov(AGE,ICU) | −0.0603 (0.0489) | −0.0120 (0.0158) | −0.0120 (0.0158) |
| cov(AGE,SPO2) | −0.00929 (0.00945) | −0.0105 (0.00537) | −0.0105 (0.00537) |
| cov(AGE,DRV + RTV) | −0.287 ** (0.0980) | −0.0939 ** (0.0287) | −0.0939 ** (0.0287) |
| cov(AGE,KALETRA) | −0.0858 (0.0772) | −0.000520 (0.00931) | −0.000520 (0.00931) |
| cov(AGE,REZOLSTA) | −0.0531 (0.0608) | −0.00438 (0.0130) | −0.00438 (0.0130) |
| cov(AGE,NoT) | 0.259 (0.293) | 0.108 (0.0658) | 0.108 (0.0658) |
| cov(AGE,U/R) | −0.0270 (0.0907) | 0.0514 (0.0335) | 0.0514 (0.0335) |
| cov(SEX,CMD) | 0.0250 (0.118) | −0.0371 (0.0621) | −0.0371 (0.0621) |
| cov(SEX,S/NS) | 0.0138 (0.0393) | −0.0214 (0.0236) | −0.0214 (0.0236) |
| cov(SEX,ICU) | −0.0338 (0.0214) | 0.0283 * (0.0120) | 0.0283 * (0.0120) |
| cov(SEX,SPO2) | −0.00161 (0.00404) | 0.00206 (0.00389) | 0.00206 (0.00389) |
| cov(SEX,DRV + RTV) | 0.0175 (0.0376) | 0.00894 (0.0200) | 0.00894 (0.0200) |
| cov(SEX,KALETRA) | −0.00125 (0.0328) | −0.0102 (0.00693) | −0.0102 (0.00693) |
| cov(SEX,REZOLSTA) | −0.00625 (0.0260) | −0.0106 (0.00966) | −0.0106 (0.00966) |
| cov(SEX,NoT) | 0.0338 (0.126) | −0.0344 (0.0480) | −0.0344 (0.0480) |
| cov(SEX,U/R) | 0.0475 (0.0398) | −0.0260 (0.0246) | −0.0260 (0.0246) |
| cov(CMD,S/NS) | 0.0250 (0.119) | 0.140 * (0.0605) | 0.140 * (0.0605) |
| cov(CMD,ICU) | −0.200 ** (0.0700) | −0.0525 (0.0297) | −0.0525 (0.0297) |
| cov(CMD,SPO2) | −0.0200 (0.0126) | −0.0252 * (0.0101) | −0.0252 * (0.0101) |
| cov(CMD,DRV + RTV) | −0.350 ** (0.126) | −0.106 * (0.0513) | −0.106 * (0.0513) |
| cov(CMD,KALETRA) | −0.0500 (0.0994) | −0.00769 (0.0172) | −0.00769 (0.0172) |
| cov(CMD,REZOLSTA) | 0.100 (0.0800) | 0.00423 (0.0241) | 0.00423 (0.0241) |
| cov(CMD,NoT) | 0.175 (0.379) | 0.380 ** (0.126) | 0.380 ** (0.126) |
| cov(CMD,U/R) | 0.0750 (0.119) | 0.0771 (0.0618) | 0.0771 (0.0618) |
| cov(S/NS,ICU) | −0.0144 (0.0209) | −0.000577 (0.0111) | −0.000577 (0.0111) |
| cov(S/NS,SPO2) | 0.00226 (0.00406) | 0.00284 (0.00370) | 0.00284 (0.00370) |
| cov(S/NS,DRV + RTV) | 0.0163 (0.0377) | −0.00779 (0.0190) | −0.00779 (0.0190) |
| cov(S/NS,KALETRA) | −0.0931 ** (0.0361) | 0.00308 (0.00652) | 0.00308 (0.00652) |
| cov(S/NS,REZOLSTA) | −0.0406 (0.0269) | 0.00615 (0.00914) | 0.00615 (0.00914) |
| cov(S/NS,NoT) | 0.00187 (0.126) | 0.0498 (0.0457) | 0.0498 (0.0457) |
| cov(S/NS,U/R) | −0.0362 (0.0397) | −0.0122 (0.0232) | −0.0122 (0.0232) |
| cov(ICU,SPO2) | 0.00387 (0.00222) | 0.00355 (0.00186) | 0.00355 (0.00186) |
| cov(ICU,DRV + RTV) | 0.0238 (0.0202) | 0.0121 (0.00950) | 0.0121 (0.00950) |
| cov(ICU,KALETRA) | 0.00813 (0.0174) | −0.00115 (0.00323) | −0.00115 (0.00323) |
| cov(ICU,REZOLSTA) | −0.00937 (0.0139) | −0.00231 (0.00453) | −0.00231 (0.00453) |
| cov(ICU,NoT) | −0.0819 (0.0677) | −0.0836 *** (0.0240) | −0.0836 *** (0.0240) |
| cov(ICU,U/R) | −0.00875 (0.0208) | −0.00461 (0.0115) | −0.00461 (0.0115) |
| cov(SPO2,DRV + RTV) | 0.00325 (0.00390) | 0.00559 (0.00319) | 0.00559 (0.00319) |
| cov(SPO2,KALETRA) | −0.00312 (0.00342) | −0.000508 (0.00108) | −0.000508 (0.00108) |
| cov(SPO2,REZOLSTA) | 0.000102 (0.00268) | −0.00132 (0.00151) | −0.00132 (0.00151) |
| cov(SPO2,NoT) | −0.00182 (0.0129) | −0.0336 *** (0.00821) | −0.0336 *** (0.00821) |
| cov(SPO2,U/R) | 0.00104 (0.00404) | 0.00347 (0.00385) | 0.00347 (0.00385) |
| cov(DRV + RTV,KALETRA) | −0.00375 (0.0315) | −0.0156 ** (0.00576) | −0.0156 ** (0.00576) |
| cov(DRV + RTV,REZOLSTA) | −0.0438 (0.0259) | −0.0311 *** (0.00836) | −0.0311 *** (0.00836) |
| cov(DRV + RTV,NoT) | −0.199 (0.124) | −0.0161 (0.0387) | −0.0161 (0.0387) |
| cov(DRV + RTV,U/R) | −0.0575 (0.0386) | −0.0280 (0.0200) | −0.0280 (0.0200) |
| cov(KALETRA,REZOLSTA) | −0.0281 (0.0223) | −0.000769 (0.00267) | −0.000769 (0.00267) |
| cov(KALETRA,NoT) | −0.146 (0.108) | 0.0146 (0.0134) | 0.0146 (0.0134) |
| cov(KALETRA,U/R) | −0.0262 (0.0331) | −0.00154 (0.00678) | −0.00154 (0.00678) |
| cov(REZOLSTA,NoT) | 0.197 * (0.0890) | −0.0296 (0.0188) | −0.0296 (0.0188) |
| cov(REZOLSTA,U/R) | 0.0437 (0.0269) | −0.00308 (0.00950) | −0.00308 (0.00950) |
| cov(NoT,U/R) | 0.159 (0.128) | −0.0298 (0.0474) | −0.0298 (0.0474) |
| mean(REMDESIVIR) | 1.127 *** (0.0793) | ||
| var(REMDESIVIR) | 0.641 *** (0.0897) | ||
| cov(SFA,REMDESIVIR) | −0.0937 (0.105) | ||
| cov(SD,REMDESIVIR) | 0.0111 (0.0304) | ||
| cov(HD,REMDESIVIR) | −0.143 (0.590) | ||
| cov(DF,REMDESIVIR) | −0.131 * (0.0588) | ||
| cov(AGE,REMDESIVIR) | −0.0566 (0.0540) | ||
| cov(SEX,REMDESIVIR) | −0.0710 (0.0402) | ||
| cov(CMD,REMDESIVIR) | −0.0873 (0.0997) | ||
| cov(S/NS,REMDESIVIR) | −0.0543 (0.0380) | ||
| cov(ICU,REMDESIVIR) | −0.00231 (0.0186) | ||
| cov(SPO2,REMDESIVIR) | 0.00708 (0.00626) | ||
| −0.00663 (0.0321) | |||
| cov(KALETRA,REMDESIVIR) | 0.0123 (0.0111) | ||
| cov(REZOLSTA,REMDESIVIR) | 0.00500 (0.0154) | ||
| cov(NoT,REMDESIVIR) | 0.00308 (0.0766) | ||
| cov(U/R,REMDESIVIR) | 0.0149 (0.0392) | ||
| N total | 145 | 129 | 129 |
References
- Walker, P.J.; Siddell, S.G.; Lefkowitz, E.J.; Mushegian, A.R.; Dempsey, D.M.; Dutilh, E.B.; Harrach, B.; Harrison, R.L.; Hendrickson, R.C.; Junglen, S.; et al. Changes to virus taxonomy and the International Code of Virus Classification and Nomenclature ratified by the International Committee on Taxonomy of Viruses. Arch. Virol. 2019, 164, 2417–2429. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.H.; Poon, L.L.; Cheng, V.C.; Guan, Y.; Hung, I.F.; Kong, J.; Yam, L.Y.; Seto, W.H.; Yuen, K.Y.; Peiris, J.S. Detection of SARS coronavirus in patients with suspected SARS. Emerg. Infect. Dis. 2004, 10, 294–299. [Google Scholar] [CrossRef] [Green Version]
- Peiris, J.S.; Yuen, K.Y.; Osterhaus, A.D.; Stöhr, K. The severe acute respiratory syndrome. N. Engl. J. Med. 2003, 349, 2431–2441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance 2020, 25, 2000062. [CrossRef]
- Zafer, M.M.; El-Mahallawy, H.A.; Ashour, H.M. Severe COVID-19 and sepsis: Immune pathogenesis and laboratory markers. Microorganism 2021, 9, 159. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar]
- Yao, Y.; Cao, J.; Wang, O.; Shi, O.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: A case control study. J. Intensive Care 2020, 8, 49. [Google Scholar] [CrossRef]
- Bartziokas, K.; Kostikas, K. Lactate dehydrogenase, COVID-19 and mortality. Med. Clin. 2021, 156. [Google Scholar] [CrossRef]
- Asghar, M.S.; Haider Kazmi, S.J.; Khan, N.A.; Akram, M.; Hassan, M.; Rasheed, U.; Khan, S.A. Poor prognostic biochemical markers predicting fatalities caused by COVID-19: A retrospective observational study from a developing country. Cureus 2020, 12, e9575. [Google Scholar] [CrossRef]
- Sharma, A.; Eisen, J.E.; Shepard, J.O.; Bernheim, A.; Little, B.P. Case 25-2020: A 47-year-old woman with a lung mass. N. Engl. J. Med. 2020, 13, 665–674. [Google Scholar] [CrossRef]
- Altenbuchinger, M.; Weihs, A.; Quackenbush, J.; Grabe, H.J.; Zacharias, H. Gaussian and mixed graphical models as (multi)omics data analysis tools. Biochim. Biophys. Acta Gene Regul. Mech. 2020, 1863, 194418. [Google Scholar] [CrossRef] [PubMed]
- Woo Lee, J.; Moen, E.; Punshon, T.; Hoen, A.; Stewart, D.; Li, H.; Karagas, M.; Gui, J. An Integrated gaussian graphical model to evaluate the impact of expires on metabolic networks. Comput. Biol. Med. 2019, 114, 103417. [Google Scholar] [CrossRef] [PubMed]
- Istodor, A.V.; Rusu, L.-C.; Noja, G.G.; Roi, A.; Roi, C.; Bratu, E.; Moise, G.; Puiu, M.; Farcas, S.S.; Andreescu, N.I. An observational study on cephalometric characteristics and patterns associated with the Prader–Willi Syndrome: A structural equation modelling and network approach. Appl. Sci. 2021, 11, 3177. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Tavakolpour, S.; Rakhshandehroo, T.; Wei, E.X.; Rashidian, M. Lymphopenia during the COVID-19 infection: What it shows and what can be learned. Immunol. Lett. 2020, 225, 31–32. [Google Scholar] [CrossRef]
- Liu, J.; Li, H.; Luo, M.; Liu, J.; Wu, L.; Lin, X.; Li, R.; Wang, Z.; Zhong, H.; Zheng, W.; et al. Lymphopenia predicted illness severity and recovery in patients with COVID-19: A single-center, retrospective study. PLoS ONE 2020, 15, e0241659. [Google Scholar] [CrossRef]
- Cappanera, S.; Palumbo, M.; Kwan, S.H.; Priante, G.; Martella, L.A.; Saraca, L.M.; Sicari, F.; Vernelli, C.; Di Giuli, C.; Andreani, P.; et al. When does the cytokine storm begin in COVID-19 patients? A quick score to recognize it. J. Clin. Med. 2020, 10, 297. [Google Scholar]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Shah, K.; Patel, S.B.; Patel, F.S.; Osman, M.; Velagapudi, P.; Turagam, M.K.; Lakkireddy, D.; Garg, J. Elevated D-Dimer levels are associated with increased risk of mortality in coronavirus disease 2019: A systematic review and meta-analysis. Cardiol. Rev. 2020, 28, 295–302. [Google Scholar] [CrossRef]
- Chen, L.; Liu, H.G.; Liu, W.; Liu, J.; Liu, K.; Shang, J.; Deng, Y.; Wei, S. Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Chin. J. Tuberc. Respir. Med. 2020. (In Chinese) [Google Scholar] [CrossRef]
- Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; Cheng, Z.; Gao, S.; Liang, K.; et al. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan. Clin. Infect. Dis. 2020, 16, ciaa270. [Google Scholar] [CrossRef] [Green Version]
- Martha, J.W.; Wibowo, A.; Pranata, R. Prognostic value of elevated lactate dehydrogenase in patients with COVID-19: A systematic review and meta-analysis. Postgrad. Med. J. 2021. [Google Scholar] [CrossRef]
- Baranovskii, D.S.; Klabukov, I.D.; Krasilnikova, O.A.; Nikogosov, D.A.; Polekhina, N.V.; Baranovskaia, D.R.; Laberko, L.A. Prolonged prothrombin time as an early prognostic indicator of severe acute respiratory distress syndrome in patients with COVID-19 related pneumonia. Curr. Med. Res. Opin. 2021, 37, 21–25. [Google Scholar] [CrossRef]
- De Wit, E.; Feldmann, F.; Cronin, J.; Jordan, R.; Okumura, A.; Thomas, T.; Scott, D.; Cihlar, T.; Feldmann, H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc. Natl. Acad. Sci. USA 2020, 117, 6771–6776. [Google Scholar] [CrossRef] [Green Version]
- Al-Tawfiq, J.A.; Al-Homoud, A.H.; Memish, Z.A. Remdesivir as a possible therapeutic option for the COVID-19. Travel Med. Infect. Dis. 2020, 34, 101615. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with Tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.L.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in patients hospitalized with Covid-19 pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Oh, E.; Shepherd, B.; Lumley, T.; Shaw, P. Considerations for analysis of time-to-event outcomes measured with error: Bias and correction with SIMEX. Stat. Med. 2018, 37, 1276–1289. [Google Scholar] [CrossRef]





| No. Patients | Gender | Age (Average) | Residence (Urban/Rural) | Smokers/Non-Smokers | Days of Hospitalization (Average) | Disease Form | Deaths/ICU | |
|---|---|---|---|---|---|---|---|---|
| 1st wave | 145 | 76 men (52%); 69 women (48%) | 42 years | 55.6% urban; 44.4% rural | 48.9% smokers; 51.1% non-smokers | 12 days | 53.1%—mild; 25.51%—moderate; 7.58%—severe; 3.44%—critical; 10.37%—asymptomatic | 6 patients died (4.13%); 10 patients were treated in the ICU (6.89% of patients) |
| 2nd wave | 129 | 61 men (47%); 68 women (53%) | 58 years | 58.9% urban; 41.1% rural | 30.2% smokers; 69.7% non-smokers | 12 days | 6.97%—mild; 35.65%—moderate; 39.53%—severe; 17.08%—critical; 0.77%; asymptomatic | 24 patients died (18.60%); 13 patients were treated in the ICU (10.07% of patients) |
| N | Mean | Var | Sd | Min | Max | |
|---|---|---|---|---|---|---|
| AGE | 145 | 42 | 348.0 | 18.6 | 1 | 83 |
| HD | 145 | 12 | 31.8 | 5.6 | 2 | 29 |
| SPO2 | 139 | 95 | 21.7 | 4.6 | 70 | 112 |
| NoT | 143 | 2 | 3.0 | 1.7 | 1 | 9 |
| N total | 145 |
| N | Mean | Var | Sd | Min | Max | |
|---|---|---|---|---|---|---|
| AGE | 129 | 58 | 310.8 | 17.6 | 1 | 91 |
| HD | 129 | 12 | 53.3 | 7.3 | 2 | 57 |
| SPO2 | 129 | 89 | 52.5 | 7.2 | 50 | 99 |
| NoT | 102 | 2 | 0.9 | 0.9 | 1 | 6 |
| N total | 129 |
| Symptomatology at Onset (SFA) | 1st Wave | 2nd Wave |
|---|---|---|
| Fever | 62.06% | 66.66% |
| Headache | 37.93% | 33.33% |
| Cough | 66.89% | 79.06% |
| Anosmia and ageusia | 13.1% | 14.72% |
| Myalgias | 27.58% | 27.13% |
| Dysphonia | 4.13 % | 9.3% |
| Dysphagia | 13.7% | 8.52% |
| Shivers | 12.4% | 13.17% |
| Digestive symptoms | 16.55% | 16.27% |
| Dyspnoea | 15.17% | 51.16% |
| Symptomatology during the hospitalization | 1st wave | 2nd wave |
| Cough | 82.75% | 62.56% |
| Fever | 11.03% | 14.72% |
| Dyspnoea | 20% | 72.86% |
| Headache | 5.51% | 10.1% |
| Anosmia and ageusia | 12.4% | 7.75% |
| Myalgia | 15.17% | 5.4% |
| Dysphagia | 16.55% | 6.8% |
| Digestive symptoms | 7.58% | 4.65% |
| Asthenia (fatigue) | 16% | 62.79% |
| Symptomatology at discharge (SD) | 1st wave | 2nd wave |
| Cough | 20% | 2.3% |
| Oxygen concentrator at home | 5.5% | 26.13% |
| Asthenia (fatigue) | 8% | 18.6% |
| Comorbidities at onset (CMD) | 1st wave | 2nd wave |
| Hypertension | 26.89% | 70.54% |
| Hashimoto‘s thyroiditis | 4.82% | 5.42% |
| Type 2 diabetes | 10.34% | 27.13% |
| Heart failure | 3.44% | 37.20% |
| Obesity | 6.89% | 23.25% |
| Sepsis | 4.13% | 19.37% |
| Chronic kidney disease | 4.13% | 9.3% |
| Cerebrovascular accident | 2% | 4.6% |
| Atrial fibrillation | 1.37% | 5.4% |
| Asthma | 1.37% | 5.4% |
| Acute respiratory failure | 20% | 53.48% |
| Mixed dementia | 0% | 6.9% |
| Comorbidities developed during hospitalization | 1st wave | 2nd wave |
| Sinus tachycardia | 0% | 1.55% |
| Hepatic cytolysis syndrome | 4.82% | 34.10% |
| Inaugural diabetes | 6.2% | 38.75% |
| Acute renal failure | 6.89% | 11.62% |
| Pleurisy | 1.37% | 0% |
| Pulmonary emphysema | 1.37% | 0% |
| Pulmonary thromboembolism | 0% | 2.3% |
| Clostridium difficile enterocolitis | 0% | 2.3% |
| Upper digestive hemorrhage | 0% | 0.77% |
| Biological Samples and Treatment from 274 Hospitalized Patients | 1st Wave | 2nd Wave |
|---|---|---|
| Leukopenia | 15.1% | 18.6% |
| Leucocytosis | 11.7% | 43.4% |
| Thrombocytopenia | 15.17% | 17.0% |
| Thrombocytosis | 24.8% | 12.4% |
| Lymphopenia | 35.1% | 92.2% |
| Hemoglobin ↓ | 13.1% | 25.5% |
| Prothrombin time ↑ | 26. 8% | 28.6% |
| Fibrinogen ↑ | 37.9% | 82.1% |
| D-Dimers ↑ | 38.6% | 64.3% |
| Ferritin ↑ | 16.5% | 81.3% |
| LDH ↑ | 46.8% | 82.1% |
| Urea↑ | 15.1% | 29.4% |
| Creatinine ↑ | 21.3% | 14.72% |
| Hyponatremia | 46.2% | 46.5% |
| Hypokalemia | 4.13% | 4.6% |
| Hyperkalemia | 15.8% | 6.75% |
| Aspartate aminotransferase (SGOT/AST) ↑ | 44.8% | 38.7% |
| Alanine aminotransferase (GPT/ALT) ↑ | 48.2% | 45.7% |
| Procalcitonin ↑ | 4.13% | 19.37% |
| Hyperglycemia | 34.4% | 82.1% |
| Lactate↑ | 19.3% | 42.6% |
| CRP↑ | 47.5% | 89.9% |
| Interleukin 6↑ | 4.13% | 75.1% |
| Troponin↑ | 2% | 2% |
| CT scan | 16%—mild form of pneumonia 6.4%—a moderate form of pneumonia 4.2%—a severe form of pneumonia | 25.58%—mild form of pneumonia 32.55%—moderate form of pneumonia 30.23%—severe form of pneumonia |
| Antiviral medication | Lopinavir/Ritonavir—25.65%, Darunavir + Cobicistat—24.58%, Darunavir + Ritonavir—41.13%, Hydroxychloroquine—28.96% | Lopinavir/Ritonavir—3.87%, Darunavir + Cobicistat—4.65%, Darunavir + Ritonavir—79.06%, Favipiravir—12.50%, Remdesivir—31% |
| Antibiotic therapy | Azithromycin—35.17% Ceftriaxone—21.37% Vancomycin—2.78% | Ceftriaxone—46.51%, Ceftriaxone + Levofloxacin—3.87%, Ceftriaxone + Moxifloxacin—4.65%, Vancomycin—1.55%, Meropenem + Vancomycin—10.07% |
| Corticotherapy | 31% | 77.51% |
| Anticoagulant | 21.37% | 94.57% |
| Immunomodulatory medication | 0% | Anakinra—4.65% Tocilizumab—15.50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mocanu, A.; Noja, G.G.; Istodor, A.V.; Moise, G.; Leretter, M.; Rusu, L.-C.; Marza, A.M.; Mederle, A.O. Individual Characteristics as Prognostic Factors of the Evolution of Hospitalized COVID-19 Romanian Patients: A Comparative Observational Study between the First and Second Waves Based on Gaussian Graphical Models and Structural Equation Modeling. J. Clin. Med. 2021, 10, 1958. https://doi.org/10.3390/jcm10091958
Mocanu A, Noja GG, Istodor AV, Moise G, Leretter M, Rusu L-C, Marza AM, Mederle AO. Individual Characteristics as Prognostic Factors of the Evolution of Hospitalized COVID-19 Romanian Patients: A Comparative Observational Study between the First and Second Waves Based on Gaussian Graphical Models and Structural Equation Modeling. Journal of Clinical Medicine. 2021; 10(9):1958. https://doi.org/10.3390/jcm10091958
Chicago/Turabian StyleMocanu, Alexandra, Gratiela Georgiana Noja, Alin Viorel Istodor, Georgiana Moise, Marius Leretter, Laura-Cristina Rusu, Adina Maria Marza, and Alexandru Ovidiu Mederle. 2021. "Individual Characteristics as Prognostic Factors of the Evolution of Hospitalized COVID-19 Romanian Patients: A Comparative Observational Study between the First and Second Waves Based on Gaussian Graphical Models and Structural Equation Modeling" Journal of Clinical Medicine 10, no. 9: 1958. https://doi.org/10.3390/jcm10091958