
Anxiety towards COVID-19, Fear of Negative Appearance, Healthy Lifestyle, and Their Relationship with Well-Being during the Pandemic: A Cross-Cultural Study between Indonesia and Poland




Abstract
:1. Introduction
2. Instruments and Methods
2.1. Sample
2.2. Instruments
2.2.1. Outcome Variable: Well-Being during the Pandemic
2.2.2. Predictors and Mediators
Anxiety towards COVID-19
Fear of Negative Appearance
Eating Disorders
Compulsive Exercise
Sociodemographic Characteristics as Covariates
2.3. Analytical Approach
3. Results
3.1. Descriptive Analysis
3.2. Analysis of Measurement Model
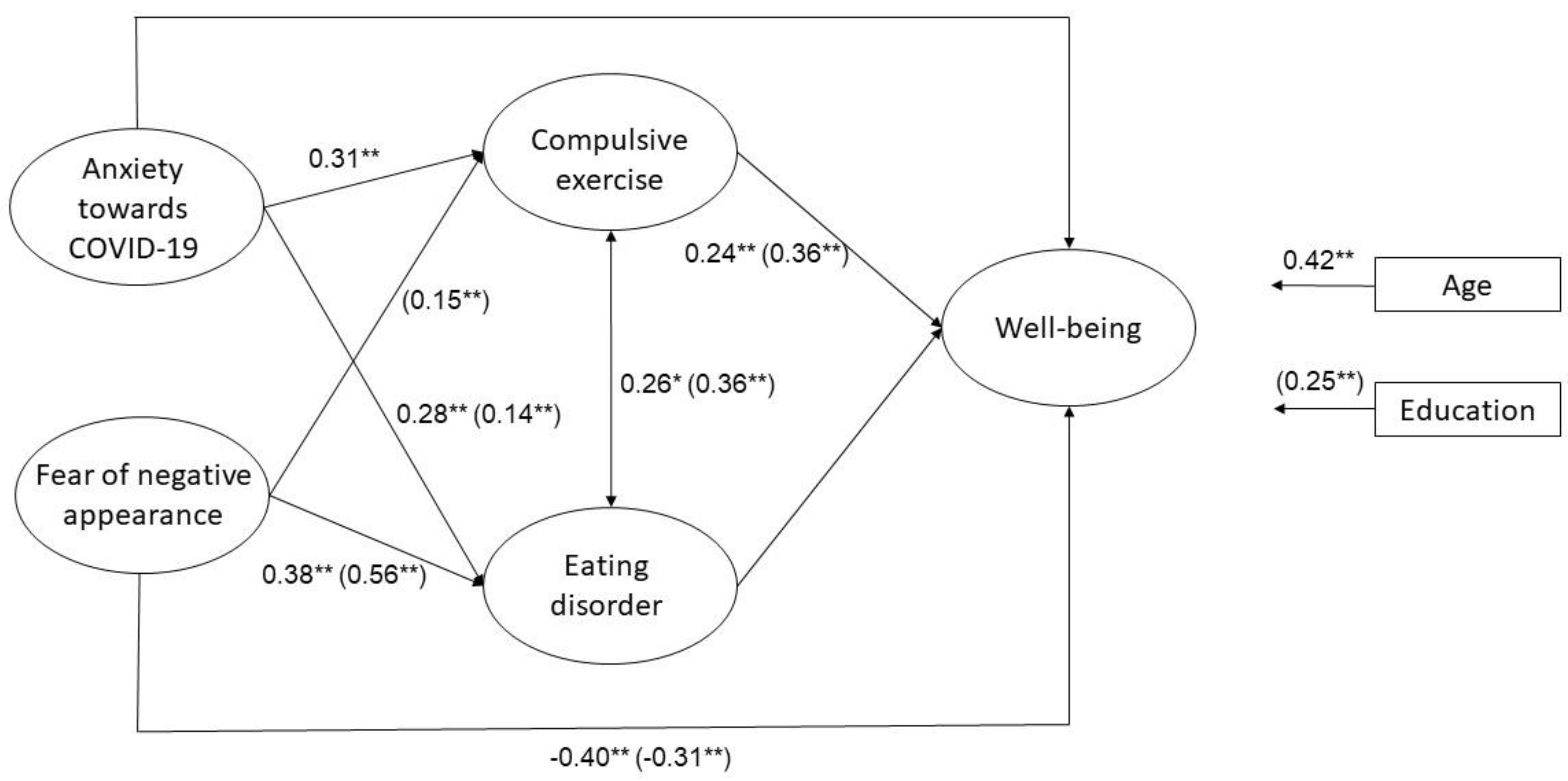
3.3. Analysis of Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Path | Indonesia | Poland | ||||
|---|---|---|---|---|---|---|
| B (SE) | p-Value | β | B (SE) | p-Value | β | |
| AC → CE | 0.48 (0.14) | 0.00 | 0.31 | 0.06 (0.09) | 0.47 | 0.03 |
| AC → ED | 1.79 (0.67) | 0.01 | 0.28 | 0.82 (0.24) | 0.00 | 0.14 |
| AC → WB | −0.04 (0.07) | 0.59 | −0.05 | −0.04 (0.04) | 0.23 | −0.05 |
| FNA → CE | −0.14 (0.08) | 0.08 | −0.15 | 0.21 (0.18) | 0.00 | 0.15 |
| FNA → ED | 1.42 (0.41) | 0.00 | 0.38 | 2.42 (0.18) | 0.00 | 0.58 |
| FNA → WB | −0.19 (0.05) | 0.00 | −0.40 | −0.19 (0.03) | 0.00 | −0.31 |
| CE → WB | 0.13 (0.05) | 0.02 | 0.24 | 0.15 (0.02) | 0.00 | 0.36 |
| ED → WB | −0.02 (0.02) | 0.15 | −0.18 | −0.01 (0.01) | 0.17 | −0.09 |
| CE ↔ ED | 2.80 (1.32) | 0.03 | 0.26 | 5.89 (0.87) | 0.00 | 0.36 |
| Age → WB | 0.05 (0.02) | 0.00 | 0.42 | 0.00 (0.00) | 0.23 | 0.05 |
| Education → WB | 0.02 (0.15) | 0.89 | 0.02 | 0.27 (0.05) | 0.00 | 0.25 |
References
- World Health Organization (WHO). Coronavirus Disease 2019; Situation Report 51; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/331475 (accessed on 30 November 2021).
- Manjunath, N.K.; Majumdar, V.; Rozzi, A.; Huiru, W.; Mishra, A.; Kimura, K.; Nagarathna, R.; Nagendra, H.R. Health Perceptions and Adopted Lifestyle Behaviors During the COVID-19 Pandemic: Cross-National Survey. JMIR Form. Res. 2021, 5, e23630. [Google Scholar] [CrossRef] [PubMed]
- White, R.G.; Van Der Boor, C. Impact of the COVID-19 pandemic and initial period of lockdown on the mental health and well-being of adults in the UK. BJPsych Open 2020, 6, E90. [Google Scholar] [CrossRef] [PubMed]
- Scharmer, C.; Martinez, K.; Gorrell, S.; Reilly, E.E.; Donahue, J.M.; Anderson, D.A. Eating disorder pathology and compulsive exercise during the COVID-19 public health emergency: Examining risk associated with COVID-19 anxiety and intolerance of uncertainty. Int. J. Eat. Disord. 2020, 53, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6, E125. [Google Scholar] [CrossRef] [PubMed]
- Bidzan-Bluma, I.; Bidzan, M.; Jurek, P.; Bidzan, L.; Knietzsch, J.; Stueck, M.; Bidzan, M. A Polish and German Population Study of Quality of Life, Well-Being, and Life Satisfaction in Older Adults During the COVID-19 Pandemic. Front. Psychiatry 2020, 11, 585813. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and Coronavirus disease 2019—A perfect storm. JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [Green Version]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef]
- Pikoos, T.D.; Buzwell, S.; Sharp, G.; Rossell, S.L. The Zoom Effect: Exploring the Impact of Video Calling on Appearance Dissatisfaction and Interest in Aesthetic Treatment During the COVID-19 Pandemic. Aesthetic Surg. J. 2021, 41, NP2076–NP2077. [Google Scholar] [CrossRef]
- Lundgren, J.D.; Anderson, D.A.; Thompson, J.K. Fear of negative appearance evaluation: Development and evaluation of a new construct for risk factor work in the field of eating disorders. Eat. Behav. 2004, 5, 75–84. [Google Scholar] [CrossRef]
- Rodgers, R.; Chabrol, H.; Paxton, S.J. An exploration of the tripartite influence model of body dissatisfaction and disordered eating among Australian and French college women. Body Image 2011, 8, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Niswah, I.; Rah, J.H.; Roshita, A. The Association of Body Image Perception with Dietary and Physical Activity Behaviors Among Adolescents in Indonesia. Food Nutr. Bull. 2021, 42 (Suppl. 1), S109–S121. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Story, M.; Hannan, P.J.; Perry, C.L.; Irving, L.M. Weight-related concerns and behaviors among overweight and nonoverweight adolescents: Implications for preventing weight-related disorders. Arch. Pediatr. Adolesc. Med. 2002, 156, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Shagar, P.S.; Donovan, C.L.; Boddy, J.; Tapp, C.; Harris, N. Does culture moderate the relationship between body dissatisfaction and quality of life? A comparative study of Australian and Malaysian emerging adults. Health Psychol. Open 2021, 8, 20551029211018378. [Google Scholar] [CrossRef]
- Tiggemann, M. Body dissatisfaction and adolescent self-esteem: Prospective findings. Body Image 2005, 2, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Andriani, D.; Novita, S.; Lipowski, M. Aktivitas Fisik, Gangguan Perilaku Makan, dan Kualitas Hidup: Benarkah Pandemi Mengubah Kesadaran Hidup Sehat? J. Muara Ilmu Sos. Hum. Dan Seni 2022. submitted. [Google Scholar]
- McClintock, J.M.; Evans, I.M. The underlying psychopathology of eating disorders and social phobia: A structural equation analysis. Eat. Behav. 2001, 2, 247–261. [Google Scholar] [CrossRef]
- Chan, C.Y.; Chiu, C.Y. Disordered eating behaviors and psychological health during the COVID-19 pandemic. Psychol. Health Med. 2022, 27, 249–256. [Google Scholar] [CrossRef]
- Badri, M.A.; Alkhaili, M.; Aldhaheri, H.; Alnahyan, H.; Yang, G.; Albahar, M.; Alrashdi, A. Understanding the Interactions of Happiness, Self-Rated Health, Mental Feelings, Habit of Eating Healthy and Sport/Activities: A Path Model for Abu Dhabi. Nutrients 2022, 14, 55. [Google Scholar] [CrossRef]
- Gerdtham, U.-G.; Johannesson, M. The relationship between happiness, health, and socio-economic factors: Results based on Swedish microdata. J. Socio-Econ. 2001, 30, 553–557. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Danielsen, M.; Bjørnelv, S.; Rø, Ø. Validation of the exercise and eating disorders questionnaire. Int. J. Eat. Disord. 2015, 48, 983–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehr, M.M.; Zamani-Alavijeh, F.; Hasanzadeh, A.; Fasihi, T. Effect of healthy lifestyle educational programs on happiness and life satisfaction in the elderly: A randomized controlled trial study. Iran. J. Ageing 2019, 13, 440–451. [Google Scholar] [CrossRef]
- Hofstede, G.; Hofstede, G.J.; Minkov, M. Cultures and Organizations: Software of the Mind, 3rd ed.; McGraw-Hill: New York, NY, USA, 2010. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Ryff, C.D. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychother. Psychosom. 2014, 83, 10–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaś, D.; Cieciuch, J. Polish adaptation of Carol Ryff’s Psychological Well-Being Scales. Rocz. Psychol. 2018, 20, 21. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Lee, S.A. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef]
- Skalski, S.; Uram, P.; Dobrakowski, P. Coronavirus Anxiety Scale—Polish Version. Available online: https://sites.google.com/cnu.edu/coronavirusanxietyproject/home (accessed on 18 May 2022).
- Wilczyńska, D.; Li, J.; Yang, Y.; Fan, H.; Liu, T.; Lipowski, M. Fear of COVID-19 changes the motivation for physical activity participation: Polish-Chinese comparisons. Health Psychol. Rep. 2021, 9, 138–148. [Google Scholar] [CrossRef]
- Thomas, C.M.; Keery, H.; Williams, R.; Thompson, J.K. The fear of negative appearance evaluation scale: Development and preliminary validation. Eat. Behav. 1998, 5, 75–84. [Google Scholar]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Rogoza, R.; Brytek-Matera, A.; Garner, D.M. Analysis of the EAT-26 in a non-clinical sample. Arch. Psychiatry Psychother. 2016, 18, 54–58. [Google Scholar] [CrossRef]
- Yates, A.; Shisslak, C.; Crago, M.; Allender, J. Overcommitment to sport: Is there a relationship to the eating disorders? Clin. J. Sport Med. 1994, 4, 39–46. [Google Scholar] [CrossRef]
- Steffen, J.J.; Brehm, B.J. The dimensions of obligatory exercise. Eat. Disord. 1999, 7, 219–226. [Google Scholar] [CrossRef]
- Matsunaga, M. Item parceling in structural equation modeling: A primer. Commun. Methods Meas. 2008, 2, 260–293. [Google Scholar] [CrossRef]
- Engelhard, G., Jr. Historical perspectives on invariant measurement: Guttman, Rasch, and Mokken. Measurement 2008, 6, 155–189. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 22 June 2021).
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Pearson Education: Harlow, UK, 2014. [Google Scholar]
- Johnson, M.R.D. Perceptions of Barriers to Healthy Physical Activity among Asian Communities. Sport Educ. Soc. 2000, 5, 51–70. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling. Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Tabacknick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics, 5th ed.; Pearson: New York, NY, USA, 2007; Available online: https://www.pearsonhighered.com/assets/preface/0/1/3/4/0134790545.pdf (accessed on 30 November 2021).
- Badrin, S.; Daud, N.; Ismail, S.B. Body weight perception and weight loss practices among private college students in Kelantan State, Malaysia. Korean J. Fam. Med. 2018, 39, 355–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, M.A.; Templeton, L.; Gandhi, A.; Gorzalka, B.B. Asian body image satisfaction: Ethnic and gender differences across Chinese, Indo-Asian, and European-Descent students. Eat. Disord. 2004, 12, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Atmadja, T.F.A.; Yunianto, A.E.; Yuliantini, E.; Haya, M.; Faridi, A.; Suryana, S. Gambaran sikap dan gaya hidup sehat masyarakat Indonesia selama pandemi Covid-19. AcTion Aceh Nutr. J. 2020, 5, 195. [Google Scholar] [CrossRef]
- Puciato, D.; Rozpara, M.; Borysiuk, Z. Physical activity as a determinant of quality of life in working-age people in Wrocław, Poland. Int. J. Environ. Res. Public Health 2018, 15, 623. [Google Scholar] [CrossRef] [Green Version]
- Bronikowska, M.; Krzysztoszek, J.; Łopatka, M.; Ludwiczak, M.; Pluta, B. Comparison of physical activity levels in youths before and during a pandemic lockdown. Int. J. Environ. Res. Public Health 2021, 18, 5139. [Google Scholar] [CrossRef]
- Łuszczki, E.; Bartosiewicz, A.; Pezdan-Śliż, I.; Kuchciak, M.; Jagielski, P.; Oleksy, Ł.; Stolarczyk, A.; Dereń, K. Children’s eating habits, physical activity, sleep, and media usage before and during COVID-19 pandemic in Poland. Nutrients 2021, 13, 2447. [Google Scholar] [CrossRef]
- Gestsdottir, S.; Svansdottir, E.; Sigurdsson, H.; Arnarsson, A.; Ommundsen, Y.; Arngrimsson, S.; Sveinsson, T.; Johannsson, E. Different factors associate with body image in adolescence than in emerging adulthood: A gender comparison in a follow-up study. Health Psychol. Rep. 2018, 6, 81–93. [Google Scholar] [CrossRef]

| Variable | Mean | SD | Min. | Max. | Effect Size (d) |
|---|---|---|---|---|---|
| Age | 23.77 (32.39) | 7.73 (11.38) | 18 (18) | 64 (74) | 0.89 |
| Education | 3.44 (4.07) | 0.80 (1.03) | 2 (1) | 6 (6) | 0.68 |
| Well-being 1 | |||||
| Acceptance | 12.60 (13.63) | 2.17 (2.13) | 7.00 (4.00) | 18.00 (18.00) | 0.48 |
| Environmental mastery | 14.13 (14.10) | 2.01 (1.92) | 9.00 (7.00) | 18.00 (18.00) | 0.01 |
| Positive relations | 11.31 (14.03) | 2.59 (2.24) | 4.00 (3.00) | 17.00 (18.00) | 1.12 |
| Purpose in life | 11.10 (13.32) | 2.26 (2.18) | 6.00 (4.00) | 17.00 (18.00) | 1.00 |
| Personal growth | 8.34 (8.93) | 1.59 (1.61) | 5.00 (6.00) | 18.00 (18.00) | 0.37 |
| Autonomy | 14.53 (14.46) | 2.08 (2.07) | 7.00 (5.00) | 18.00 (18.00) | 0.03 |
| Anxiety towards COVID-19 1 | |||||
| Indicator 1 | 2.94 (3.28) | 1.61 (1.76) | 2.00 (2.00) | 10.00 (10.00) | 0.20 |
| Indicator 2 | 2.55 (3.04) | 1.23 (1.51) | 2.00 (2.00) | 10.00 (10.00) | 0.20 |
| Indicator 3 | 1.21 (1.24) | 0.56 (0.63) | 1.00 (1.00) | 5.00 (5.00) | 0.05 |
| Fear of negative appearance 1 | |||||
| Indicator 1 | 6.64 (5.40) | 2.40 (2.13) | 2.00 (2.00) | 10.00 (10.00) | −0.55 |
| Indicator 2 | 6.01 (5.12) | 2.54 (2.24) | 2.00 (2.00) | 10.00 (10.00) | −0.37 |
| Indicator 3 | 5.94 (4.96) | 2.35 (2.34) | 2.00 (2.00) | 10.00 (10.00) | −0.42 |
| Eating disorders 1 | |||||
| Dieting | 57.63 (56.29) | 12.18 (9.98) | 20.00 (23.00) | 77.00 (78.00) | −0.12 |
| Bulimia and food preoccupation | 29.54 (31.01) | 4.54 (3.90) | 12.00 (9.00) | 36.00 (36.00) | 0.35 |
| Oral and control behavior | 30.97 (33.43) | 5.31 (5.04) | 15.00 (15.00) | 42.00 (42.00) | 0.48 |
| Compulsive exercise 1 | |||||
| Emotional element of exercise | 6.47 (7.74) | 2.15 (2.70) | 4.00 (4.00) | 14.00 (16.00) | 0.52 |
| Exercise frequency and intensity | 7.70 (9.46) | 2.32 (3.04) | 4.00 (4.00) | 15.00 (16.00) | 0.65 |
| Exercise preoccupation | 3.38 (3.73) | 1.31 (1.43) | 2.00 (2.00) | 8.00 (8.00) | 0.26 |
| Indicator 4 | 5.19 (7.13) | 1.57 (2.36) | 3.00 (3.00) | 11.00 (11.00) | 0.97 |
| Indicator 5 | 9.01 (10.85) | 2.42 (2.51) | 5.00 (5.00) | 17.00 (20.00) | 0.75 |
| Indicator 6 | 4.54 (4.58) | 1.35 (1.30) | 2.00 (2.00) | 8.00 (8.00) | 0.03 |
| Variable | Factor Loadings |
|---|---|
| Well-being 1 | |
| Acceptance | 0.67 (0.74) |
| Environmental mastery | 0.21 (0.64) |
| Positive relations | 0.56 (0.47) |
| Purpose in life | 0.72 (0.77) |
| Personal growth | 0.63 (0.70) |
| Autonomy | 0.42 (0.61) |
| Anxiety towards COVID-19 1 | |
| Indicator 1 | 0.71 (0.74) |
| Indicator 2 | 0.91 (0.96) |
| Indicator 3 | 0.86 (0.72) |
| Fear of negative appearance 1 | |
| Indicator 1 | 0.83 (0.89) |
| Indicator 2 | 0.91 (0.95) |
| Indicator 3 | 0.89 (0.94) |
| Eating disorders 1 | |
| Dieting | 0.55 (0.76) |
| Bulimia and food preoccupation | 0.80 (0.78) |
| Oral and control behavior | 0.27 (0.48) |
| Compulsive exercise 1 | |
| Emotional element of exercise | 0.75 (0.69) |
| Exercise frequency and intensity | 0.76 (0.87) |
| Exercise preoccupation | 0.36 (0.65) |
| Indicator 4 | 0.75 (0.82) |
| Indicator 5 | 0.79 (0.80) |
| Indicator 6 | 0.29 (−0.16) |
| Path | Indonesia | Poland | ||
|---|---|---|---|---|
| Indirect Effect | Total Effect | Indirect Effect | Total Effect | |
| AC → CE → WB | 0.06 | 0.02 | 0.01 | −0.03 |
| AC → ED → WB | −0.04 | −0.08 | −0.01 | −0.05 |
| FNA → CE → WB | −2.96 | −3.15 | 0.03 ** | −0.15 ** |
| FNA → ED → WB | −0.03 | −0.22 ** | −0.03 | −0.22 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novita, S.; Andriani, D.; Erika; Lipowski, M.; Lipowska, M. Anxiety towards COVID-19, Fear of Negative Appearance, Healthy Lifestyle, and Their Relationship with Well-Being during the Pandemic: A Cross-Cultural Study between Indonesia and Poland. Int. J. Environ. Res. Public Health 2022, 19, 7525. https://doi.org/10.3390/ijerph19127525
Novita S, Andriani D, Erika, Lipowski M, Lipowska M. Anxiety towards COVID-19, Fear of Negative Appearance, Healthy Lifestyle, and Their Relationship with Well-Being during the Pandemic: A Cross-Cultural Study between Indonesia and Poland. International Journal of Environmental Research and Public Health. 2022; 19(12):7525. https://doi.org/10.3390/ijerph19127525
Chicago/Turabian StyleNovita, Shally, Dhini Andriani, Erika, Mariusz Lipowski, and Małgorzata Lipowska. 2022. "Anxiety towards COVID-19, Fear of Negative Appearance, Healthy Lifestyle, and Their Relationship with Well-Being during the Pandemic: A Cross-Cultural Study between Indonesia and Poland" International Journal of Environmental Research and Public Health 19, no. 12: 7525. https://doi.org/10.3390/ijerph19127525